Zomacton
UkraineTable of Contents
INSTRUCTION FOR MEDICAL USE OF THE MEDICINAL PRODUCT ZOMACTON (Zomacton)
Composition:
Active substance: somatropin;
1 vial contains 4 mg of somatropin;
Excipients:
1 vial of powder contains mannitol (E 421);
1 ampoule of solvent contains sodium chloride, benzyl alcohol (9 mg/mL), water for injections.
Pharmaceutical form. Powder for solution for injection.
Main physicochemical properties: white or almost white lyophilized powder;
solvent – clear, colorless solution.
Pharmacotherapeutic group. Somatropin and somatropin agonists.
ATC code H01A C01.
Pharmacological properties.
Pharmacodynamics.
Somatropin is identical to human pituitary growth hormone in amino acid sequence, chain length (191 amino acids), and pharmacokinetic profile. It can be assumed that Somatropin (Zomacton) produces the same pharmacological effects as endogenous growth hormone.
Growth hormone promotes generalized proportional skeletal growth in humans.
After administration of exogenous Zomacton in children with confirmed pituitary growth hormone deficiency, linear growth is observed. The increased body length recorded after Zomacton administration was due to its effect on the epiphyseal plates of long bones. In children with insufficient production of pituitary growth hormone, Zomacton increases the growth rate and elevates IGF-1 (insulin-like growth factor/somatomedin-C) concentration, similar to pituitary growth hormone therapy. Increased blood levels of alkaline phosphatase have also been observed.
In response to growth hormone administration, analogous to the increase in overall body growth and mass, a proportional increase in the size of other tissues occurs. These changes include: increased connective tissue, skin, and its derivatives; increased skeletal muscle mass with an increase in size and number of cells; thymus enlargement; liver enlargement with enhanced cell proliferation; slight enlargement of gonads (sex glands), adrenal glands, and thyroid gland. There have been no reports of disproportionate skin and flat bone growth or accelerated sexual maturation associated with growth hormone replacement therapy.
Growth hormone enhances nitrogen retention and stimulates amino acid transport into tissues. Both processes promote protein synthesis. Growth hormone inhibits carbohydrate metabolism and fat formation. In high doses or in the absence of insulin, growth hormone acts as a diabetogenic agent, producing effects typically observed during fasting (impaired carbohydrate tolerance, inhibition of lipogenesis, fat mobilization, and ketosis).
After treatment with growth hormone, increased concentrations of sodium, potassium, and phosphorus are observed.
Increased renal excretion of calcium is compensated by enhanced intestinal absorption of calcium. Serum calcium concentration in patients receiving Zomacton does not significantly differ from that in patients receiving pituitary growth hormone. Elevated serum inorganic phosphate concentration has been observed in patients receiving either Zomacton or pituitary growth hormone. The increased concentration of these salts indicates their higher demand during tissue synthesis.
Pharmacokinetics.
Zomacton was administered subcutaneously at a dose of 0.1 mg somatropin/kg body weight to 8 healthy volunteers. The maximum plasma concentration of somatropin, measured 6 hours after administration, was approximately 64 ng/mL.
Clinical characteristics.
Indications.
Zomacton is indicated for:
- Long-term treatment of children with pituitary growth failure due to inadequate production and/or secretion of growth hormone, and for long-term treatment of growth failure associated with Turner syndrome, confirmed by chromosomal analysis.
Contraindications.
Hypersensitivity to somatropin or to any of the other components of the medicinal product.
Zomacton should not be administered to children whose epiphyses are already closed.
Somatropin should not be used in patients with evidence of active neoplastic disease. Antineoplastic therapy must be completed prior to initiation of growth hormone therapy, and signs of intracranial neoplastic growth must be absent. If signs of tumor growth occur, treatment should be discontinued.
Proliferative or preproliferative diabetic retinopathy.
Zomacton should not be administered to patients in critical conditions, including complications following open cardiac surgery, abdominal surgery, multiple trauma, acute respiratory failure, and other similar conditions.
Somatropin treatment in children with chronic kidney disease should be discontinued following kidney transplantation.
Zomacton should not be administered to premature infants and neonates, as the solvent contains benzyl alcohol.
Interaction with other medicinal products and other forms of interaction.
Glucocorticoid therapy may inhibit the growth-promoting effects of Zomacton. Patients with concomitant adrenocorticotropic hormone (ACTH) deficiency should receive carefully adjusted glucocorticoid replacement doses. High doses of androgens, estrogens, and anabolic steroids may accelerate skeletal maturation and thereby reduce final height gain.
Since somatropin may induce insulin resistance in patients with diabetes mellitus, insulin dosage should be adjusted in patients receiving Zomacton.
Data from drug interaction studies in adult patients with growth hormone deficiency indicate that administration of somatropin may significantly increase the clearance of substances metabolized by the cytochrome P450 3A4 system (such as sex hormones, corticosteroids, anticonvulsants, and cyclosporine), leading to reduced blood concentrations of these substances. The clinical significance of this interaction is unknown.
Special precautions for use.
The maximum recommended daily dose should not be exceeded (see section "Dosage and administration").
Zomacton should not be administered to premature infants and newborns because one of the excipients is benzyl alcohol, which may cause toxic and anaphylactoid reactions in infants and children under 3 years of age.
Zomacton is not indicated for long-term therapy in children with genetically confirmed Prader-Willi syndrome and growth failure unless accompanied by a diagnosis of growth hormone deficiency. Cases of sleep apnea and sudden death have been reported in pediatric patients with Prader-Willi syndrome receiving growth hormone therapy, particularly in those with one or more of the following risk factors: severe obesity, history of upper airway obstruction, sleep apnea, or undiagnosed respiratory infection.
Isolated cases of benign intracranial hypertension have been reported. In the event of severe or recurrent headache, visual disturbances, nausea, and/or vomiting, fundoscopic examination should be performed to detect papilledema. If papilledema is confirmed, evaluation for benign intracranial hypertension should be conducted, and if this diagnosis is confirmed, somatropin therapy should be discontinued. Currently, there is insufficient evidence to guide clinical decisions regarding patients with resolved intracranial hypertension. If resuming growth hormone therapy, symptoms of intracranial hypertension should be closely monitored.
Leukemia has been observed in some patients with growth hormone deficiency receiving somatropin, as well as in untreated patients. However, there is no evidence of increased incidence of leukemia in patients with growth hormone deficiency in the absence of predisposing factors.
As with all other somatropin-containing products, a small percentage of patients may develop antibodies to somatropin. The binding capacity of these antibodies is low and does not affect growth velocity. In any patient who does not respond to therapy, testing for the presence of antibodies should be considered.
Growth hormone increases extrathyroidal conversion of T4 to T3, which may unmask underlying hypothyroidism. Therefore, thyroid function should be evaluated in all patients. In patients with hypothyroidism, careful monitoring of standard replacement therapy is required during somatropin treatment.
Patients should be evaluated for impaired glucose tolerance, as growth hormone may induce insulin resistance. Insulin dosage may need to be adjusted in diabetic patients after initiation of somatropin therapy. Patients with diabetes mellitus or impaired glucose tolerance should be closely monitored during somatropin therapy. Zomacton should also be used with caution in patients with a known family history of diabetes.
If preproliferative retinal changes develop during somatropin treatment, or if proliferative diabetic retinopathy is present, replacement therapy with somatropin should be discontinued. However, the presence of stable background diabetic retinopathy does not contraindicate somatropin replacement therapy.
In patients with growth hormone deficiency due to intracranial lesions, monitoring of the primary condition, including progression or regression, is recommended. An increased risk of secondary neoplasms has been reported in patients who had childhood cancer and received somatropin therapy after the initial tumor. Intracranial tumors, particularly meningiomas, in patients who received cranial irradiation for treatment of the initial tumor, are the most frequently reported secondary neoplasms.
If progression or recurrence of the lesion occurs, Zomacton therapy should be discontinued. Particular attention should be paid to symptoms of recurrence in patients with a history of malignancy.
In any child experiencing rapid growth, progression of scoliosis is possible. Signs of scoliosis should be monitored during somatropin therapy.
Epiphyseal slip of the femoral head may occur in patients with endocrine disorders. Physicians should examine patients treated with Zomacton who develop limping or pain in the hip or knee.
The effect of growth hormone therapy on recovery has been studied in two placebo-controlled trials involving 522 critically ill adult patients with complications following open-heart surgery, abdominal surgery, multiple accidental traumas, or acute respiratory failure.
Mortality was higher (42% vs. 19%) in patients treated with growth hormone (doses of 5.3 to 8 mg per day) compared to those receiving placebo. Given this information, growth hormone therapy should not be administered to such patients. Due to the lack of safety data on growth hormone therapy in critically ill patients, the benefits of treatment in this setting should be weighed against potential risks.
Despite the rarity of such events, pancreatitis should be considered as a possible adverse effect in patients receiving somatropin therapy, especially in children presenting with abdominal pain.
Zomacton contains sodium, but less than 1 mmol (23 mg) of sodium per dose, thus being practically sodium-free.
Use during pregnancy or breastfeeding.
Data on the effects of Zomacton are lacking.
Data on the use of somatropin in animals during pregnancy are lacking.
Zomacton is not recommended for use in pregnant women or women of childbearing potential who are not using contraception.
Clinical studies with somatropin-containing products have not been conducted in breastfeeding women. It is unknown whether somatropin is excreted in human milk.
Ability to affect driving and operating machinery.
Zomacton does not affect the ability to drive or operate machinery.
Method of Administration and Dosage
Treatment with ZOMACTON should be carried out under the supervision of a qualified physician experienced in the management of patients with growth hormone deficiency.
The dose and administration schedule of ZOMACTON should be individually adjusted for each patient.
The usual duration of treatment lasts several years and depends on the therapeutic response achieved.
Subcutaneous administration of growth hormone may lead to atrophy or hypertrophy of subcutaneous tissue at the injection site. Therefore, injection sites should be rotated.
Growth hormone deficiency.
The recommended weekly dose is usually 0.17–0.23 mg/kg body weight (equivalent to 4.9 mg/m²–6.9 mg/m² body surface area) administered as 6–7 subcutaneous injections per week (corresponding to a daily dose of 0.02–0.03 mg/kg body weight, or 0.7–1 mg/m² body surface area). The total weekly dose should not exceed 0.27 mg/kg, or 8 mg/m² body surface area (corresponding to a daily dose of up to 0.04 mg/kg).
Turner syndrome.
The recommended weekly dose is usually 0.33 mg/kg body weight (approximately 9.86 mg/m² body surface area), divided into 6–7 subcutaneous injections (corresponding to a daily dose of 0.05 mg/kg body weight, or 1.40–1.63 mg/m² body surface area).
Reconstitution.
Depending on the volume of diluent used, two different concentrations of the preparation can be prepared (the concentration is determined by the physician).
- When using the ZOMAJET 2 Vision needle-free injector or a conventional syringe, 1.3 mL of diluent should be used to prepare a solution with a concentration of 3.3 mg/mL.
- When using only a conventional syringe, 3.2 mL of diluent should be used to prepare a solution with a concentration of 1.3 mg/mL.
The powder must be reconstituted only with the diluent provided.
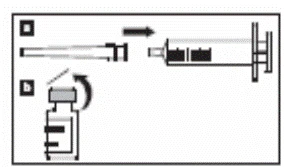
Fig. 1, a. Attach the needle to the graduated syringe.
b. Remove the plastic cap from the vial.
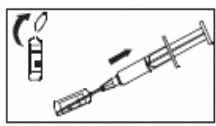
Fig. 2. Snap off the ampoule neck containing the diluent, remove the plastic cap from the needle, and ensure that the syringe plunger is fully withdrawn before inserting the needle into the ampoule.
Slowly draw the required volume of diluent into the syringe. Depending on the volume of diluent used, two concentrations of the preparation can be prepared (the concentration is determined by the physician).
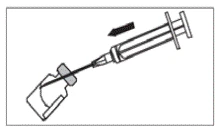
Fig. 3. To prevent foaming, the diluent should be added down the side of the vial.
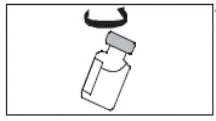
Fig. 4. Gently rotate the vial until the powder is completely dissolved and a clear, colorless solution is obtained.
Shaking or vigorous mixing should be avoided. If the solution remains cloudy or contains particles, the vial and its contents should be discarded. If cloudiness persists after cooling, allow the solution to warm to room temperature. If cloudiness persists or discoloration appears, the vial and its contents must be discarded.
After reconstitution, the clear, colorless solution should be administered subcutaneously using a syringe or the needle-free injector ZOMAJET 2 Vision. Instructions for the use of the ZOMAJET 2 Vision needle-free injector are provided in the leaflet accompanying the device.
Children. ZOMACTON is administered to children (see section "Method of Administration and Dosage"). ZOMACTON should not be administered to premature infants or newborns, as the diluent contains benzyl alcohol.
Overdose.
The recommended dose of ZOMACTON should not be exceeded.
Although there are no reported cases of ZOMACTON overdose, acute overdose may cause initial hypoglycemia followed by hyperglycemia.
The effects of prolonged, repeated administration of ZOMACTON at doses exceeding the recommended levels have not been studied. However, such use may lead to symptoms similar to those observed in excessive human growth hormone production (e.g., acromegaly).
Adverse Reactions
Subcutaneous administration of growth hormone may lead to atrophy or proliferation of subcutaneous adipose tissue at the injection site. In individual cases, patients may experience pain or itching rash at the injection site.
Adverse reactions are categorized by frequency as follows: very common (≥ 1/10), common (≥ 1/100 to < 1/10), uncommon (≥ 1/1000 to < 1/100), rare (≥ 1/10000 to < 1/1000), very rare (< 1/10000).
Blood and lymphatic system disorders: uncommon – anemia.
Cardiac disorders: uncommon – tachycardia, hypertension (in adults); rare – hypertension (in children).
Ear and labyrinth disorders: uncommon – dizziness.
Endocrine disorders: common – hypothyroidism.
Eye disorders: uncommon – optic disc edema, diplopia.
Gastrointestinal disorders: uncommon – vomiting, abdominal pain, flatulence, nausea; rare – diarrhea.
General disorders and administration site conditions: very common – edema (in adults), peripheral edema (in adults); common – edema (in children), peripheral edema (in children), injection site reactions, asthenia; uncommon – weakness, atrophy at injection site, hemorrhage at injection site, nodule formation at injection site, hypertrophy.
Immune system disorders: common – antibody formation.
Investigations: rare – renal function abnormalities.
Metabolism and nutrition disorders: very common – mild hyperglycemia (in adults); common – impaired glucose tolerance (in children); uncommon – hypoglycemia, hyperphosphatemia; rare – type 2 diabetes mellitus.
Musculoskeletal and connective tissue disorders: very common – arthralgia (in adults), myalgia (in adults); common – arthralgia (in children), myalgia (in children), limb stiffness (in adults); uncommon – muscle atrophy, bone pain, carpal tunnel syndrome, limb stiffness (in children).
Benign, malignant and unspecified neoplasms (including cysts and polyps): uncommon – malignant neoplasms, neoplasms; very rare – leukemia (in children).
Nervous system disorders: very common – headache (in adults), paresthesia (in adults); common – headache, hypertonia, insomnia (in adults); uncommon – somnolence, nystagmus; rare – neuropathy, increased intracranial pressure, insomnia (in children), paresthesia (in children).
Psychiatric disorders: uncommon – personality disorders.
Renal and urinary disorders: uncommon – urinary incontinence, hematuria, polyuria, increased frequency of urination/pollakiuria, urine abnormality.
Reproductive system and breast disorders: uncommon – genital discharge, gynecomastia (in adults); very rare – gynecomastia (in children).
Skin and subcutaneous tissue disorders: uncommon – lipodystrophy, skin atrophy, exfoliative dermatitis, urticaria, hirsutism, skin hypertrophy.
Pancreatitis has been reported during post-marketing use of growth hormone therapy (frequency unknown).
Somatropin leads to antibody formation in 1% of cases. The binding capacity of these antibodies is low and has no clinical significance.
Very rarely, leukemia has been observed in children with growth hormone deficiency treated with somatropin, but the incidence is extremely low.
In children treated with growth hormone, cases of slipped capital femoral epiphysis and Legg–Calvé–Perthes disease have been reported. Slipped capital femoral epiphysis occurs more frequently in patients with endocrine disorders, and Legg–Calvé–Perthes disease is more common in children with short stature. However, it is unknown whether these conditions occur more frequently with somatropin treatment. These diagnoses should be considered in the presence of discomfort or pain in the hip and/or knee.
Other adverse reactions may be considered characteristic of somatropin, including hyperglycemia due to reduced insulin sensitivity, decreased levels of free thyroxine, and possible development of benign intracranial hypertension.
Hypersensitivity reactions cannot be ruled out.
Shelf life. 3 years.
Storage conditions. Store in a refrigerator at 2–8 °C in the original packaging. Keep out of reach of children.
The reconstituted preparation may be stored in an upright position in the refrigerator at 2–8 °C for up to 14 days.
Incompatibilities.
Due to lack of compatibility data, this medicinal product should not be mixed with other medicinal products.
Packaging.
1 vial of powder with 1 ampoule of 3.5 ml diluent in a cardboard package.
Prescription status. Prescription only.
Manufacturer.
Ferring GmbH, Germany.
Manufacturer's address and place of business.
Wittland 11, 24109 Kiel, Germany.