Zoladex
Ukraine
Table of Contents
INSTRUCTIONS FOR MEDICAL USE OF THE MEDICINAL PRODUCT ZOLADEX (ZOLADEX®)
Composition:
Active substance: 1 prolonged-release subcutaneous implant capsule contains goserelin acetate equivalent to 10.8 mg goserelin base;
Excipients: copolymer of lactide and glycolide.
Pharmaceutical form. Prolonged-release subcutaneous implant capsule.
Main physicochemical properties: solid cylindrical polymer pieces of white to cream color, free or practically free from visible particles.
Pharmacotherapeutic group. Gonadotropin-releasing hormone analogs.
ATC code L02A E03.
Pharmacological Properties.
Pharmacodynamics.
Zoladex (D-Ser (But)6Azgly10LH-RH) is a synthetic analogue of the natural luteinizing hormone – releasing hormone (LH-RH). With continuous administration, Zoladex 10.8 mg suppresses pituitary secretion of luteinizing hormone, resulting in decreased serum concentrations of testosterone in men and estradiol in women. Initially, like other LH-RH agonists, Zoladex 10.8 mg may cause a transient increase in serum testosterone concentrations in men and estradiol in women.
In men, testosterone concentrations decrease to castrate levels by approximately day 21 after administration of the first implant and remain suppressed with continued administration every 12 weeks. Data indicate that, in exceptional circumstances when the next dose is not administered at 3 months, testosterone concentrations remain at castrate levels for up to 16 weeks in most patients.
In comparative clinical trials of metastatic prostate cancer, Zoladex demonstrated survival outcomes similar to those of surgical castration.
In a combined analysis of two randomized controlled trials comparing monotherapy with bicalutamide 150 mg versus castration (primarily using Zoladex), no significant difference in overall survival was observed between patients with prostate cancer receiving bicalutamide and those undergoing castration (relative risk = 1.05 [confidence interval (CI) 0.81 to 1.36]). However, statistical equivalence between the two treatment approaches cannot be established.
In comparative studies, Zoladex improved relapse-free survival and overall survival when used as adjuvant therapy prior to radiotherapy in patients with high-risk localized prostate cancer (T1–T2 with PSA [prostate-specific antigen] ≥10 ng/mL or Gleason score of 7) or locally advanced (T3–T4) prostate cancer. The optimal duration of adjuvant therapy has not been established; however, a comparative trial demonstrated that adjuvant treatment with Zoladex for 3 years significantly improved survival compared to radiotherapy alone. Neoadjuvant use of Zoladex prior to radiotherapy improved relapse-free survival in patients with high-risk localized or locally advanced prostate cancer.
Following prostatectomy in patients with extracapsular extension of prostate tumor, adjuvant therapy with Zoladex may improve disease-free survival, although significant survival benefit is not observed if patients did not have lymph node involvement at surgery. Patients with locally advanced disease confirmed histopathologically and additional risk factors such as PSA ≥10 ng/mL or Gleason score of 7 prior to adjuvant therapy with Zoladex should undergo careful evaluation. There is no evidence of improved clinical outcomes with neoadjuvant use of Zoladex following radical prostatectomy.
In women, serum estradiol concentrations decrease within 4 weeks after administration of the first implant and remain suppressed throughout the treatment period. In patients whose estradiol levels are already suppressed due to prior use of LH-RH analogues, switching to Zoladex 10.8 mg maintains suppressed estradiol concentrations. Suppression of estradiol leads to a therapeutic response in patients with endometriosis or uterine fibroids and results in amenorrhea in most patients.
At the beginning of Zoladex treatment, some women may experience vaginal bleeding of variable duration and intensity. Such bleeding is likely a response to estrogen withdrawal and usually resolves spontaneously.
During treatment with LH-RH analogues, natural menopause may occur in some women; in rare cases, menstruation does not resume after treatment discontinuation.
Pharmacokinetics.
Administration of Zoladex 10.8 mg every 12 weeks provides stable exposure to goserelin without clinically significant drug accumulation. Zoladex has minimal protein binding; its serum half-life is 2 to 4 hours in patients with normal renal function. In patients with impaired renal function, the elimination half-life is prolonged. However, when the drug is administered as 10.8 mg implants every 12 weeks, this change does not lead to drug accumulation, and dose adjustment is not required in such patients. No significant changes in pharmacokinetics are observed in patients with hepatic insufficiency.
Clinical characteristics.
Indications.
Prostate cancer. Treatment of prostate cancer where hormonal influence is possible.
Endometriosis. Treatment of endometriosis, including relief of symptoms such as pain, and reduction in the size and number of endometrial lesions.
Uterine fibroids. Treatment of fibroids, including reduction of lesions, improvement of hematological status, and relief of symptoms such as pain. As an adjunct to surgical intervention to facilitate surgical technique and reduce blood loss during surgery.
Breast cancer in premenopausal women.
Contraindications.
Hypersensitivity to goserelin acetate or to any of the excipients.
Pregnancy or breastfeeding period.
Pediatric age.
Interaction with other medicinal products and other forms of interaction.
Since androgen deprivation therapy may lead to QT interval prolongation, concomitant use of Zoladex with medicinal products capable of prolonging the QT interval, or agents that may cause torsades de pointes ventricular tachycardia, such as class IA antiarrhythmics (e.g., quinidine, disopyramide) or class III (e.g., amiodarone, sotalol, dofetilide, ibutilide), methadone, moxifloxacin, antipsychotic agents, etc., should be carefully evaluated (see section "Special precautions").
Special precautions for use.
Injection site reactions have been reported with the use of Zoladex, including pain, hematoma, bleeding, and vascular injury. Patients should be monitored for signs or symptoms of abdominal bleeding. In very rare cases, administration errors have led to vascular injury and hemorrhagic shock requiring blood transfusion and surgical intervention. Particular caution is required when administering Zoladex to patients with low body mass index (BMI) and to patients receiving full anticoagulant therapy (see section "Method of administration and dosage").
There are no data on removal or dissolution of the implant.
There is a high risk of depression (which may be severe) in patients receiving gonadotropin-releasing hormone (GnRH) agonists such as goserelin. Patients should be informed of this risk, and appropriate treatment should be initiated if symptoms occur.
Cases of bleeding around the injection site leading to hemorrhagic shock have been reported. The following safety measures should be considered when using Zoladex:
- Administer injections in areas with lower likelihood of vascular injury.
- Carefully consider the potential use of Zoladex in patients with bleeding tendencies (e.g., those receiving anticoagulants).
Androgen deprivation therapy may prolong the QT interval.
Before prescribing Zoladex to patients with a history of QT prolongation or risk factors for QT prolongation, and to patients receiving concomitant medications that may cause QT prolongation (see section "Interaction with other medicinal products and other forms of interaction"), the benefit-risk ratio should be assessed, including the potential risk of torsades de pointes.
Men
Zoladex 10.8 mg should be used with caution in men at risk of developing urinary tract obstruction or spinal cord compression, and such patients should be closely monitored during the first month of therapy. In cases of existing or developing spinal cord compression or renal failure due to urinary tract obstruction, standard treatment for these complications should be initiated.
It is unlikely that patients with non-hormone-dependent prostate cancer will benefit from this treatment. This resistance to treatment may result from a lack of response to castration or hormonal therapy.
Testosterone measurement is recommended before initiating therapy to allow assessment of therapeutic benefit.
At the initial stages of therapy with GnRH analogs, consideration should be given to the use of antiandrogens (e.g., cyproterone acetate 300 mg daily for three days before and three weeks after starting Zoladex therapy), as reports suggest this may prevent potential consequences of the initial rise in serum testosterone levels.
Use of GnRH agonists may lead to decreased bone mineral density. Preliminary data suggest that the use of bisphosphonates in men, in addition to GnRH agonists, may reduce bone mineral loss. Particular caution is advised in patients with additional risk factors for osteoporosis (such as chronic alcohol abuse, smoking, long-term anticonvulsant or corticosteroid therapy, or family history of osteoporosis).
Patients with established depression and those with hypertension require close monitoring.
There is a high risk of hypotension (which may be serious) in patients treated with GnRH agonists such as goserelin. Patients should be informed of this risk and managed appropriately if symptoms occur.
In a pharmacoepidemiological study of GnRH agonists used for the treatment of prostate cancer, cases of myocardial infarction and heart failure were observed. The risk increases when the drug is used in combination with antiandrogen agents.
Reduced glucose tolerance has been observed in men receiving GnRH agonists. This may manifest as diabetes or loss of glycemic control in individuals with pre-existing diabetes. Therefore, monitoring of blood glucose levels is required.
Women
In premenopausal women with breast cancer, the hormonal receptor status of the tumor should be determined before initiating treatment with Zoladex 10.8 mg. If the disease is receptor-negative, Zoladex 10.8 mg prolonged-release subcutaneous implants should not be used.
A transient increase in serum estradiol levels may occur in women after initiation of GnRH agonist therapy.
Reduction in bone mineral density
The use of GnRH agonists may lead to a decrease in bone mineral density of approximately 1% per month during the first 6 months of treatment. Each 10% reduction in bone mineral density increases the risk of fractures by 2–3 times.
Available data indicate that bone density is restored in most women after discontinuation of the drug.
In patients receiving Zoladex for endometriosis, additional hormone replacement therapy (HRT) has been shown to reduce the decline in bone mineral density and the severity of vasomotor symptoms. However, there is no experience with HRT in women receiving Zoladex 10.8 mg.
There are no specific data on the use of the drug in patients with established osteoporosis or risk factors for its development (such as chronic alcohol abuse, smoking, long-term therapy with drugs that reduce bone mineral density, e.g., anticonvulsants or corticosteroids, family history of osteoporosis, eating disorders such as anorexia nervosa). Since bone mineral loss in such patients may be more hazardous, the use of Zoladex should be carefully considered on a case-by-case basis, and treatment should be initiated only after a thorough evaluation indicating that benefits outweigh the risks. Additional measures to prevent bone mineral loss should be implemented.
Reduction in bone mineral density during breast cancer treatment in women
The use of GnRH agonists may cause a reduction in bone mineral density. After 2 years of treatment for early-stage breast cancer, the mean loss in bone mineral density was 6.2% at the femoral neck and 11.5% at the lumbar spine. This loss has been shown to be partially reversible during one year of observation after treatment discontinuation, with recovery of 3.4% and 6.4% at the femoral neck and lumbar spine, respectively, although this recovery is based on very limited data. Available data for most women suggest that bone tissue loss is reversed after treatment cessation.
Preliminary data suggest that the use of goserelin in combination with tamoxifen in breast cancer patients may reduce bone demineralization.
Withdrawal bleeding
At the beginning of Zoladex therapy, some women may experience vaginal bleeding of varying duration and intensity. This usually occurs during the first month of treatment, is likely a response to estrogen withdrawal, and typically resolves spontaneously. If bleeding persists, the cause should be investigated.
The time to return of menstruation after discontinuation of Zoladex 10.8 mg may be prolonged in some cases (mean duration of secondary amenorrhea after stopping Zoladex 10.8 mg is 7–8 months). If rapid return of menstruation is desired, Zoladex 3.6 mg is recommended.
Zoladex use may increase cervical resistance; therefore, caution should be exercised during cervical dilation.
There are no clinical data on the effect of Zoladex use for benign gynecological conditions beyond 6 months.
Women of reproductive age should use non-hormonal contraception during Zoladex therapy and until menstruation resumes after treatment completion.
Patients with established depression and those with arterial hypertension require close monitoring.
Zoladex use may lead to a positive result in anti-doping tests.
There is a high risk of hypotension (which may be serious) in patients treated with GnRH agonists such as goserelin. Patients should be informed of this risk and managed appropriately if symptoms occur.
Instructions for use of the pouch
Use only if the pouch containing the pre-filled syringe-applicator is undamaged. Use immediately after opening the pouch.
Use during pregnancy or breastfeeding
Zoladex should not be used during pregnancy or breastfeeding, as there is a theoretical risk of miscarriage or fetal abnormalities if GnRH agonists are administered during pregnancy. A careful evaluation should be performed in women of childbearing potential to exclude pregnancy.
Non-hormonal contraception should be used during treatment until menstruation resumes.
Fertility
In women, GnRH analogs such as Zoladex 3.6 mg and Zoladex 10.8 mg suppress LH and FSH. As a result, libido may be affected (see section "Side effects"), and ovulation and menstruation may cease, leading to a negative but reversible effect on female fertility. Natural menopause may occur during GnRH analog therapy. Rarely, menstruation does not return after treatment cessation in some women. Animal studies in rats indicate that the effect on female fertility is reversible.
In men: GnRH analogs such as Zoladex 3.6 mg and Zoladex 10.8 mg suppress LH and FSH. As a result, erectile dysfunction and effects on libido (see section "Side effects") may occur, and spermatogenesis may be affected. Although data on male fertility are limited, based on the reversibility of fertility effects in rats and the reversibility of histopathological changes in the reproductive system of dogs after one year of Zoladex treatment, the effect in men is expected to be reversible.
Ability to influence reaction speed while driving or operating machinery
Zoladex has no effect or a negligible effect on the ability to drive or operate machinery.
Method of Administration and Dosage
Zoladex should be administered with caution into the anterior abdominal wall due to the proximity of the inferior epigastric artery and its branches.
Particular caution is required when administering Zoladex to patients with low BMI or those receiving anticoagulant therapy (see section "Special Precautions").
Local anesthesia may be used, although it is generally not required in most cases.
Adult men (including elderly patients)
1 capsule (10.8 mg) of Zoladex should be administered subcutaneously into the anterior abdominal wall every 12 weeks.
Adult women (including elderly patients)
1 capsule (10.8 mg) of Zoladex should be administered subcutaneously into the anterior abdominal wall every 12 weeks.
Endometriosis and uterine fibroids: treatment should be limited to 6 months, as clinical data on longer treatment durations are lacking.
Repeated treatment courses are not recommended due to the risk of mineral loss and decreased bone mineral density.
In women treated with goserelin for endometriosis, additional hormone replacement therapy (daily administration of estrogen and progestogen) has been shown to reduce bone mineral density loss and alleviate vasomotor symptoms.
Experience with hormone replacement therapy in women receiving Zoladex 10.8 mg is lacking.
Dosage adjustment is not required in patients with renal or hepatic impairment, or in elderly patients.
Instructions for Administration
Use according to the recommendations of the prescribing physician.
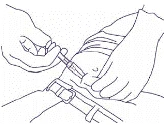
Ensure that the injection is administered subcutaneously, following the technique described in the administration instructions. Do not inject the drug into blood vessels, muscle, or the peritoneal cavity.
If surgical removal of the Zoladex capsule is required, its location can be identified using ultrasound imaging.
Instructions for Use
Use only if the pre-filled syringe applicator pouch is undamaged. Use immediately after opening the pouch.
Dispose of the syringe using special sharps containers.
The following information is intended exclusively for healthcare professionals:
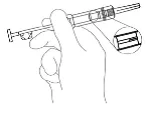
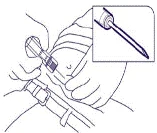
Zoladex is administered by subcutaneous injection. The instructions below should be read carefully before administration.
NOTE. Exercise caution when administering Zoladex into the anterior abdominal wall due to the proximity of the inferior epigastric artery and its branches; very thin patients may be at increased risk of vascular injury.
NOTE. The Zoladex syringe cannot be used for aspiration. If the needle enters a large blood vessel, blood will be immediately visible in the syringe chamber. If a vessel is punctured, withdraw the needle, immediately control the bleeding caused by the puncture, and monitor the patient for signs or symptoms of abdominal hemorrhage. Once hemodynamic stability is confirmed, another Zoladex implant may be administered using a new syringe at a different injection site. Exercise particular caution when administering the drug to patients with low BMI and/or those receiving full-dose anticoagulant therapy.
NOTE. The needle does not retract.
NOTE. Surgical removal of the implant is rarely needed, but if required, its location can be identified using ultrasound scanning. |
Fig. 1 |
|
Fig. 2 |
|
|
Fig. 3 |
|
|
Fig. 4 |
|
|
Fig. 5 |


Children.
Zoladex is not indicated for use in children, as the safety and efficacy of use in this patient group have not been established.
Overdose.
There is insufficient data on overdose in humans. Administration of Zoladex earlier than scheduled or in higher than prescribed doses has not been associated with clinically significant adverse effects. Results from animal studies do not indicate any effects other than the therapeutic ones on sex hormone concentrations and genital organs following administration of higher doses of Zoladex 10.8 mg. In case of overdose, symptomatic treatment should be provided.
Adverse reactions.
The frequency of adverse reactions was calculated based on data from clinical trials of Zoladex and post-marketing reports. The most commonly reported adverse reactions were hot flushes, increased sweating, and injection site reactions.
The following classification was used to define the frequency: very common (≥ 1/10), common (≥ 1/100 to < 1/10), uncommon (≥ 1/1000 to < 1/100), rare (≥ 1/10000 to < 1/1000), very rare (< 1/10000), frequency not known (cannot be estimated from the available data).
Table. Adverse reactions to Zoladex 10.8 mg by organ system classes according to MedDRA.
| System organ class |
Frequency |
Men |
Women |
| Benign, malignant and unspecified neoplasms (including cysts and polyps) |
Very rare |
Pituitary tumors |
Pituitary tumors |
| Frequency not known |
|
Uterine fibroid degeneration |
|
| Immune system disorders |
Uncommon |
Drug hypersensitivity reactions |
Drug hypersensitivity reactions |
| Rare |
Anaphylactic reactions |
Anaphylactic reactions |
|
| Endocrine system disorders |
Very rare |
Pituitary haemorrhage |
Pituitary haemorrhage |
| Metabolism and nutrition disorders |
Common |
Impaired glucose tolerancea |
|
| Psychiatric disorders |
Very common |
Decreased libidob |
Decreased libidob |
| Common |
Mood changes, depression |
Mood changes, depression |
|
| Very rare |
Psychiatric disorders |
Psychiatric disorders |
|
| Nervous system disorders |
Common |
Paraesthesia |
Paraesthesia |
| Spinal cord compression |
|
||
| |
Headache |
||
| Cardiac disorders |
Common |
Heart failuref, myocardial infarctionf |
|
| Frequency not known |
QT interval prolongation (see sections "Special warnings and precautions for use" and "Interaction with other medicinal products and other forms of interaction") |
|
|
| Vascular disorders |
Very common |
Hot flushesb |
Hot flushesb |
| Common |
Arterial pressure disturbancesc |
Arterial pressure disturbancesc |
|
| Skin and subcutaneous tissue disorders |
Very common |
Hyperhidrosisb |
Hyperhidrosisb, acnei |
| Common |
Rashd |
Rashd, hair lossh |
|
| Frequency not known |
Alopeciag |
Rashd, hair lossh |
|
| Musculoskeletal and connective tissue disorders |
Common |
Bone paine |
|
| Uncommon |
Arthralgia |
Arthralgia |
|
| Renal and urinary disorders |
Uncommon |
Ureteral obstruction |
|
| Reproductive system and breast disorders |
Very common |
Erectile dysfunction |
|
| |
Vulvovaginal dryness |
||
| |
Breast enlargement |
||
| Common |
Gynaecomastia |
|
|
| Uncommon |
Breast tenderness |
|
|
| Rare |
|
Ovarian cysts |
|
| Frequency not known |
|
Withdrawal bleeding |
|
| General disorders and administration site conditions |
Very common |
|
Injection site reactions |
| Common |
Injection site reactions |
Injection site reactions |
|
| |
Tumour flare, painful tumour |
||
| Investigations |
Common |
Decreased bone mineral density (see section "Special warnings and precautions for use"), increased body weight |
Decreased bone mineral density, increased body weight |
a Decreased glucose tolerance was observed in men receiving GnRH agonists. This may manifest as diabetes mellitus or loss of glycemic control in patients with pre-existing diabetes.
b These pharmacological effects rarely require discontinuation of therapy. Hyperhidrosis and hot flushes may persist after stopping Zoladex.
c Hypo- or hypertension has been occasionally reported in patients receiving Zoladex. Changes are usually temporary and resolve either with continued therapy or after discontinuation of Zoladex. Rarely, such changes required medical intervention, including discontinuation of Zoladex.
d Usually mild, often decreases without the need to discontinue treatment.
e Initially, patients with prostate cancer may experience a temporary worsening of bone pain; in such cases symptomatic treatment may be prescribed.
f Observed in pharmacoepidemiological studies of GnRH agonists used for the treatment of prostate cancer. The risk clearly increases when used in combination with antiandrogen agents.
g Particularly loss of body hair is an expected effect of reduced androgen levels.
h Hair loss on the head has been observed in women, including young women, treated for benign gynecological conditions. This phenomenon is usually mild, but occasionally may be severe.
i In most cases, acne occurred within one month after initiation of treatment.
Possible side effects with goserelin use include: hepatic dysfunction and development of jaundice with elevated levels of ALT (alanine aminotransferase), AST (aspartate aminotransferase), GGT (gamma-glutamyl transferase); increased LDH (lactate dehydrogenase), alkaline phosphatase, and triglycerides; epistaxis, vaginal bleeding, urticaria, pruritus.
Also observed during drug use: urinary system – dysuria, increased blood urea nitrogen, elevated creatinine, proteinuria; blood – anemia, leukopenia, thrombocytopenia.
During goserelin administration, injection site reactions (bleeding, hematoma, abscess, induration, pain) may occur, as well as bleeding around the injection site leading to hemorrhagic shock.
Post-marketing experience
Rarely, abnormal blood test results, cases of hepatic dysfunction, pulmonary artery embolism, and interstitial pneumonia have been observed during Zoladex use.
In women receiving therapy for endometriosis and/or fibroids, hypercalcemia has been rarely reported. In case of symptoms suggestive of hypercalcemia (e.g., thirst), investigations should be performed to rule it out.
Additionally, the following adverse reactions have been observed in women receiving the drug for benign gynecological conditions:
acne, changes in body hair, dry skin, weight gain, increased serum cholesterol, ovarian hyperstimulation syndrome (when used in combination with gonadotropins), vaginitis, vaginal discharge, nervousness, sleep disturbances, fatigue, peripheral edema, myalgia, calf muscle spasms, nausea, vomiting, diarrhea, constipation, abdominal complaints, voice changes.
At the beginning of treatment, signs and symptoms of the disease may temporarily worsen – in such cases symptomatic treatment may be prescribed.
Rarely, during treatment with GnRH analogues in women, menopause may occur and menstruation may not resume after completion of therapy. It is unknown whether this is due to the effect of Zoladex or the underlying gynecological conditions.
Reporting of suspected adverse reactions
Reporting of suspected adverse reactions after medicine registration is important. It allows continued monitoring of the benefit-risk balance of the medicine. Healthcare professionals should report any suspected adverse reactions.
Shelf life.
3 years.
Storage conditions.
Store at a temperature not exceeding 25 °C. Keep out of reach of children.
Packaging.
1 capsule in a pre-filled syringe-applicator with a safety mechanism; 1 syringe in a pouch with a moisture-absorbing capsule and attached flag-label; 1 pouch in a cardboard box.
Prescription status.
Prescription only.
Manufacturer.
AstraZeneca UK Limited.
Manufacturer's address and place of business.
Silk Road Business Park, Macclesfield, SK10 2NA, United Kingdom.