Twinrix vaccine for prevention of hepatitis a (inactivated) and b (adsorbed)
Ukraine
Table of Contents
INSTRUCTION FOR MEDICAL USE OF THE MEDICINAL PRODUCT TWINRIX
Vaccine for prevention of hepatitis A (inactivated) and hepatitis B (adsorbed)
Composition:
Active substances: 1 dose (1 ml) contains:
Hepatitis A virus (inactivated)1,2 720 ELISA units
Hepatitis B virus surface antigen3,4 20 μg
1 produced on human diploid MRC-5 cells
2 adsorbed on aluminum hydroxide hydrate, 0.05 mg Al3+
3 produced in yeast cell culture Saccharomyces cerevisiae using recombinant DNA technology
4 adsorbed on aluminum phosphate, 0.4 mg Al3+
Excipients: aluminum hydroxide, aluminum phosphate, sodium chloride, and water for injections.
Amino acids for injection, formaldehyde, neomycin sulfate, and polysorbate-20 are present in trace amounts as residuals from the manufacturing process.
Pharmaceutical form. Injection suspension.
Main physicochemical properties: a mixture of purified inactivated hepatitis A virus (HAV) and purified hepatitis B virus surface antigen (HBsAg), separately adsorbed onto aluminum hydroxide and aluminum phosphate. The hepatitis A virus is obtained using a human diploid cell culture (MRC5). HBsAg is produced by genetic engineering in a yeast cell culture.
Pharmacotherapeutic group. Viral vaccines. Combined vaccine for prevention of hepatitis. ATC code J07BC20.
Immunological and biological properties.
Pharmacodynamics
The TWINRIX vaccine induces immunity against hepatitis A and B viruses by stimulating the production of specific antibodies anti-HAV and anti-HBs.
- Children aged 1 to 15 years
In clinical studies involving individuals aged 1 to 15 years, seroconversion for anti-HAV was 99.1% one month after administration of the first dose and 100% six months after administration of the second dose (at month 7). Seroconversion for anti-HBs was 74.2% one month after administration of the first dose and 100% six months after administration of the second dose (at month 7). The seroprotection rate for anti-HBs (titers ≥ 0.01 mIU/mL) at these time points was 37.4% and 98.2%, respectively.
In a comparative clinical study involving adolescents aged 12–15 years inclusive, 142 patients received TWINRIX according to a 2-dose vaccination schedule, while 147 patients received a standard 3-dose vaccination schedule (0, 1, 6 months) using a combined hepatitis A and B vaccine containing 360 ELISA units of formalin-inactivated hepatitis A virus and 10 μg of recombinant HBsAg in a 0.5 ml dose. Among the 289 patients evaluated for immunogenicity, seroprotection rates against hepatitis B were significantly higher at months 2 and 6 with the 3-dose schedule compared to the 2-dose TWINRIX schedule. However, by month 7 after administration of TWINRIX according to the 2-dose schedule (i.e., after completion of the vaccination course), the immune response was comparable.
Immune response after primary vaccination according to the 0–12 month schedule
In a clinical study involving 120 adolescents aged 12–15 years, administration of the second vaccine dose at month 12 resulted in seropositivity rates at month 13 of 99.0% for anti-HAV and 99.0% for anti-HBs, with seroprotection rates of 97.0%.
Duration of immune response
The duration of immune response was evaluated in children up to 15 years of age following primary vaccination with TWINRIX. Data are presented in the table below.
| Year after first dose administration |
Age at primary vaccination |
Vaccination schedule (months) |
Anti-HAV antibodies |
Anti-HBs antibodies |
| Seroconversion (%) |
Seropositivity (%) |
|||
| 6 |
12-15 years |
0, 6 |
100 |
84.8 |
| 0, 12 |
100 |
92.9 |
||
| 10 |
1-11 years |
0, 6 |
100 |
77.3 |
| 15 |
12-15 years |
0, 6 |
100 |
81.1 |
After 15 years following primary vaccination with TWINRIX according to a 2-dose schedule in patients aged 12 to 15 years at the time of primary vaccination, the immune response to both antigens was shown to be comparable to that after a 3-dose schedule of a combined vaccine containing 360 EL.U. of inactivated HAV and 10 µg of surface antigen HBsAg per 0.5 mL dose.
In the group of patients who received TWINRIX according to the 2-dose vaccination schedule, a booster dose of hepatitis B vaccine was administered to a limited number of patients (n = 8) whose anti-HBs antibody concentrations had decreased to <10 mIU/mL, and all of them showed an anamnestic response.
- Individuals aged 16 years and older
In individuals aged 16 years and older, administration of three doses of TWINRIX induced immune protection against hepatitis A and B within 2–4 weeks. Clinical studies showed that one month after the first dose, anti-HAV antibodies were detected in approximately 94% of recipients, and one month after the third dose (i.e., at month 7), in 100% of vaccinated individuals. Anti-HBs antibodies appeared in 70% of individuals after the first dose and in 99% after the third dose.
In adults vaccinated according to the 0, 7, 21-day schedule plus a fourth dose at month 12, seroprotection rates against anti-HBV were 82% and 85% one and five weeks after the third dose, respectively. One month after the fourth dose, all vaccinated individuals developed a protective level of seroprotection against anti-HBV. One and five weeks after the third dose, seroconversion for anti-HAV was 100% and 99.5%, respectively, reaching 100% one month after the fourth dose in all vaccinated individuals.
In a clinical study conducted in adults over 40 years of age, seropositivity rates for anti-HAV antibodies and seroprotection rates against hepatitis B after vaccination with TWINRIX according to the 0, 1, 6-month schedule were similar to those observed with separately administered monovalent hepatitis A and B vaccines.
Seroprotection rates against hepatitis B at 7 and 48 months after the first dose of TWINRIX were 92% and 57%, respectively, compared to 80% and 40% after administration of a monovalent hepatitis B vaccine (GlaxoSmithKline) containing 20 µg of antigen, and 71% and 31%, respectively, after another licensed monovalent hepatitis B vaccine containing 10 µg of antigen. In all groups, anti-HBs antibody concentrations decreased with increasing age and body weight. Antibody concentrations were lower in men compared to women.
Seropositivity rates for anti-HAV antibodies at 7 and 48 months after the first dose of TWINRIX were 97% (in both groups at 7 and 48 months), compared to 99% and 94% after administration of a monovalent hepatitis A vaccine (GlaxoSmithKline) and 99% and 96%, respectively, after another licensed monovalent hepatitis A vaccine.
To assess immune memory, 48 months after the first dose of TWINRIX in the primary vaccination series, patients received an additional dose of the same vaccine. One month after this dose, anti-HBV antibody concentrations were ≥10 mIU/mL in 95% of patients.
In two long-term studies involving adult patients aged 17 to 43 years and patients aged 18 to 25 years, respectively, 20 years after primary immunization with TWINRIX, anti-HAV seropositivity rates reached 100% and 96%, respectively, and anti-HBs seroprotection rates were 94% and 92%, respectively.
Concomitant administration of vaccines
When the first dose of TWINRIX was administered concomitantly with a booster dose of a combined vaccine for the prevention of diphtheria, tetanus, pertussis (acellular component), poliomyelitis (inactivated), and Haemophilus influenzae type b infections (DTPa-IPV/Hib), or with the first dose of a combined measles, mumps, and rubella vaccine during the second year of life, the immune response to all antigens was satisfactory.
Pharmacokinetics
Assessment of pharmacokinetic properties is not required for vaccines.
Clinical characteristics
Indications.
TWINRIX is indicated for vaccination of individuals not previously vaccinated (from 1 year of age and older), adolescents and adults for prevention of hepatitis A and B.
Contraindications.
TWINRIX must not be administered to individuals with known hypersensitivity to any component of the vaccine or to neomycin, or to individuals who have shown signs of hypersensitivity after previous administration of TWINRIX or monovalent vaccines for prevention of hepatitis A and B. As with other vaccines, administration of TWINRIX should be postponed in individuals with acute illnesses accompanied by fever.
Interaction with other medicinal products and other types of interactions.
The effect of concomitant administration of TWINRIX and specific immunoglobulins against hepatitis A or B viruses is unknown. However, when monovalent vaccines for prevention of hepatitis A and B were co-administered with specific immunoglobulins, no impact on seroconversion was observed, although this may lead to the appearance of antibodies at somewhat reduced titers.
When TWINRIX was administered simultaneously but as a separate injection during the second year of life together with a combined vaccine for prevention of diphtheria, tetanus, pertussis (acellular component), poliomyelitis (inactivated) and Haemophilus influenzae type b (DTPa-IPV/Hib) and/or with a combined vaccine for prevention of measles, mumps and rubella, the immune response to all antigens was satisfactory (see section "Pharmacodynamics").
Although concomitant administration of TWINRIX with other vaccines has not been specifically studied, no interaction is expected when different syringes are used and injections are administered into different body sites.
Since concomitant use of TWINRIX with vaccines other than those mentioned above has not been studied, it is recommended not to administer TWINRIX simultaneously with other vaccines unless absolutely necessary.
Vaccines administered simultaneously should always be injected into different sites, preferably into different limbs.
An adequate immune response following vaccination may not be achieved in patients receiving immunosuppressive therapy or in patients with immune system deficiencies.
Special precautions for use.
Syncope (fainting) may occur during or shortly after any injectable vaccination, as a psychogenic reaction to needle injection. This may be accompanied by several neurological symptoms such as visual disturbances, paraesthesia, and tonic-clonic limb movements during recovery. It is important to ensure conditions that prevent potential injury to the patient in case of loss of consciousness.
It is possible that at the time of vaccination, the patient is already infected with hepatitis A or B virus. In such cases, it is unknown whether administration of TWINRIX vaccine can prevent the development of hepatitis A or B. The vaccine does not prevent infections caused by hepatitis C and E viruses, or by other pathogens affecting the liver. TWINRIX vaccine is not recommended for post-exposure prophylaxis (e.g., after a needle-stick injury with a contaminated needle).
The efficacy of the vaccine in immunocompromised individuals has not been evaluated. In patients undergoing haemodialysis and in individuals with impaired immune systems, protective antibody titres against hepatitis A and B viruses may not develop after primary immunization. Therefore, these patients may require additional vaccine doses.
Obesity (defined as BMI ≥ 30 kg/m²) has been observed to reduce immune response to hepatitis A vaccines. Several factors have been identified as reducing immune response to hepatitis B vaccines, including: advanced age, male sex, obesity, smoking, route of administration, and certain underlying chronic diseases. A decision should be made regarding serological testing of individuals who may be at risk of not achieving seroprotection after a complete course of TWINRIX vaccination in adults. Additional doses may be necessary for individuals who show no or suboptimal immune response to the vaccination series.
As with other injectable vaccines, appropriate measures should be readily available to manage very rare cases of anaphylactic shock. Therefore, patients should be observed for at least 30 minutes after vaccination.
Since intradermal administration and intramuscular injection into the gluteal muscle do not elicit an adequate immune response, these routes of administration must not be used. In exceptional cases, TWINRIX vaccine may be administered subcutaneously to patients with thrombocytopenia or coagulation disorders, as intramuscular injection in such individuals may lead to bleeding (see section "Administration and dosage").
TWINRIX must never be administered intravenously.
TWINRIX vaccine must not be mixed with other vaccines in the same syringe.
This medicinal product contains less than 1 mmol (23 mg) of sodium per dose, i.e., essentially "sodium-free".
As with any vaccine, an adequate immune response may not be achieved in all vaccinated individuals.
Traceability
To improve traceability of biological medicinal products, healthcare professionals should clearly and legibly record the trade name and batch number of the administered biological medicinal product in the appropriate medical documentation related to vaccination.
Use during pregnancy or breastfeeding.
The effects of TWINRIX vaccine on embryofetal, perinatal, and postnatal development and survival were evaluated in animal studies (rats). These studies provided no evidence of direct or indirect harmful effects on fertility, pregnancy, embryonal development, parturition, or postnatal development.
The effects of TWINRIX vaccine on embryofetal, perinatal, and postnatal development and survival of the child have not been studied in clinical trials.
Data from a limited number of pregnancies in vaccinated women do not indicate any adverse effect of TWINRIX vaccine on pregnancy or fetal/infant health outcomes. Although a negative impact of the recombinant hepatitis B surface antigen is not expected on pregnancy or the fetus, vaccination is recommended to be postponed until after delivery unless there is an urgent need to protect the pregnant woman from hepatitis B infection.
Administration of TWINRIX vaccine during pregnancy should only be considered if the expected benefit outweighs the potential risks to the fetus.
It is unknown whether TWINRIX vaccine is excreted in human breast milk. Excretion of TWINRIX vaccine in milk in animals has not been studied. The decision on whether to continue or discontinue breastfeeding or to continue or discontinue vaccination with TWINRIX should be made after considering the benefits of breastfeeding for the child and the benefits of vaccination for the mother.
Ability to influence the ability to drive and use machines
The effect of the vaccine on the ability to drive or operate machinery is unlikely.
Administration and Dosage
The recommended dose for children (from 1 year of age), adolescents, and adults is 1.0 mL.
Primary vaccination schedule:
- Children aged 1 to 15 years: The standard primary vaccination course with TWINRIX vaccine consists of two doses, the first administered on a chosen day and the second given between 6 and 12 months after the first dose.
- Adults and adolescents aged 16 years and older: The standard primary vaccination course with TWINRIX vaccine consists of three doses. The first dose is administered on a chosen day, the second one month later, and the third six months after the first dose.
In exceptional cases, adults who are planning to travel within one month or slightly later and who are unable to complete the primary vaccination course according to the 0, 1, 6 month schedule may be vaccinated according to the 0, 7, 21 day schedule. When using this schedule, administration of a fourth vaccine dose is recommended 12 months after the first dose.
The recommended vaccination schedules must be strictly followed. Once the primary vaccination course has been initiated, it must be completed using the same vaccine.
Booster Vaccination
If a decision is made to administer a booster dose against hepatitis A and/or hepatitis B, either monovalent or combination vaccines may be used.
- Long-term follow-up data from vaccination of children aged 1 to 15 years with TWINRIX vaccine have shown that specific antibodies persist for up to 15 years after completion of vaccination (see section "Immunological and Biological Properties").
- Long-term follow-up data from vaccination of adults with TWINRIX vaccine according to the 0, 1, 6 month schedule have shown that specific antibodies persist for up to 20 years after completion of vaccination (see section "Immunological and Biological Properties").
Anti-HAV and anti-HBs titers following primary vaccination with the combined vaccine are within the range typical for monovalent vaccines. Therefore, general recommendations for booster immunization may be based on experience with monovalent vaccines.
Hepatitis B
The need for a booster dose of hepatitis B vaccine in healthy individuals who have completed the full primary vaccination course has not been established. However, some official immunization programs include booster doses. In such cases, these recommendations must be strictly followed.
For certain high-risk groups for hepatitis B virus infection (e.g., hemodialysis patients, immunodeficient states, etc.), continuous monitoring of specific antibody levels is necessary to ensure they do not fall below 10 mIU/mL.
Hepatitis A
Currently, the need for a booster dose in immunocompetent individuals who have responded immunologically to hepatitis A vaccine has not been established, as protection may be maintained through immunological memory even in the absence of detectable antibodies. Recommendations for administering a booster dose are based on the premise that antibodies are required for protection.
If a decision is made to administer a booster dose for prevention of hepatitis A and B, the TWINRIX vaccine may be used. For booster immunization of individuals previously vaccinated with TWINRIX, monovalent hepatitis A and hepatitis B vaccines may also be used.
TWINRIX vaccine is intended for intramuscular injection into the deltoid muscle of the upper limb in adults and older children. For children under three years of age, the vaccine should be administered into the anterolateral aspect of the thigh.
Since intradermal administration and intramuscular injection into the gluteal muscle do not elicit an adequate immune response, these routes of administration must not be used.
In exceptional cases, TWINRIX vaccine may be administered subcutaneously to patients with thrombocytopenia or coagulation disorders. However, this route of administration may result in a reduced immune response. (See section "Special Warnings and Precautions for Use").
When conducting immunization in Ukraine, current orders of the Ministry of Health of Ukraine regarding preventive vaccinations must be followed.
Instructions for Vaccine Use
A white sediment with a clear, colorless supernatant may be observed after storage.
The vaccine must be resuspended before use. After resuspension, the vaccine should become a homogeneous, cloudy, white suspension.
Steps for resuspending the vaccine to obtain a homogeneous, slightly cloudy, white suspension:
- Hold the syringe vertically in a closed hand.
- Shake the syringe by inverting it upside down and back.
- Repeat this step vigorously for at least 15 seconds.
- Examine the vaccine again:
a) If the vaccine appears as a homogeneous, cloudy, white suspension, it is ready for use (the vaccine must not be clear);
b) If the vaccine does not yet appear as a homogeneous, cloudy, white suspension, shake the syringe by inverting it upside down and back for at least another 15 seconds, then recheck.
The vaccine should be inspected visually for any foreign particulate matter and/or unusual appearance prior to administration. If such conditions are observed, the vaccine must not be used.
Any unused product or waste material must be disposed of in accordance with local requirements.
Technique for using the prefilled syringe:

Hold the syringe by the barrel, not by the plunger.
Unscrew the syringe cap by turning it counterclockwise.
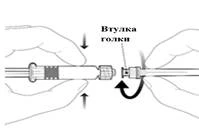
To attach the needle, connect the needle hub to the Luer-Lock adapter and turn one-quarter turn clockwise until the needle is securely attached.
Do not pull the plunger out of the syringe barrel. If this occurs, do not administer the vaccine.
Children
The TWINRIX vaccine is indicated for vaccination of unvaccinated children aged 1 year and older (see sections "Indications", "Administration and Dosage").
The safety and efficacy of TWINRIX vaccine in children under 1 year of age have not been established. No data are available.
Overdose
Post-marketing surveillance data include reports of overdose following administration of TWINRIX vaccine. Adverse events observed in cases of overdose were similar to those occurring after standard vaccination.
Adverse reactions.
Clinical trial data.
Adults and adolescents aged 16 years and older
The safety profile described below is based on data from clinical trials involving more than 6000 individuals who received the standard 0, 1, 6 month vaccination schedule (n = 5683) or an accelerated schedule of 0, 7, 21 days (n = 320). The most frequently reported local adverse reactions after administration of the vaccine according to the standard 0, 1, 6 month schedule were pain and redness, with frequencies per dose of 37.6% and 17.0%, respectively. In two clinical trials using the 0, 7, 21 day schedule, the overall reporting rates for systemic and local symptoms were comparable to those defined below. After the fourth dose administered at month 12, the frequency of systemic and local adverse reactions was consistent with the frequency observed after vaccination on the 0, 7, 21 day schedule.
In a comparative study, the frequency of adverse events following administration of TWINRIX was found to be no different from that observed with monovalent vaccines.
Frequency of adverse reactions according to reporting rates:
Very common: ≥ 1/10,
Common: ≥ 1/100 to < 1/10,
Uncommon: ≥ 1/1000 to < 1/100,
Rare: ≥ 1/10000 to < 1/1000,
Very rare: < 1/10000.
| Organs and systems |
Frequency |
Adverse reactions |
| Clinical trials |
||
| Infections and infestations |
Uncommon |
upper respiratory tract infections |
| Blood and lymphatic system |
Rare |
lymphadenopathy |
| Metabolism and nutrition disorders |
Rare |
decreased appetite |
| Nervous system |
Very common |
headache |
| Uncommon |
dizziness |
|
| Rare |
hypoesthesia, paraesthesia |
|
| Vascular system |
Rare |
hypotension |
| Gastrointestinal tract |
Common |
gastrointestinal symptoms, diarrhea, nausea |
| Uncommon |
vomiting |
|
| Skin and subcutaneous tissue |
Rare |
rash, pruritus |
| Very rare |
urticaria |
|
| Musculoskeletal and connective tissue |
Uncommon |
myalgia |
| Rare |
arthralgia |
|
| General disorders and administration site conditions |
Very common |
pain and redness at injection site, fatigue |
| Common |
swelling at injection site, injection site reaction (such as hematoma, pruritus, bruising), malaise |
|
| Uncommon |
fever (≥ 37.5 °C) |
|
| Rare |
influenza-like symptoms, chills |
|
| Post-marketing data |
||
| The adverse reactions listed below have been reported during post-marketing use of TWINRIX vaccine as well as monovalent vaccines for prevention of hepatitis A or B manufactured by GlaxoSmithKline. |
||
| Infections and infestations |
Meningitis |
|
| Blood and lymphatic system |
Thrombocytopenia, thrombocytopenic purpura |
|
| Immune system |
Anaphylaxis, allergic reactions including anaphylactoid reactions and serum sickness-like reactions |
|
| Nervous system |
Encephalitis, encephalopathy, neuritis, neuropathy, paralysis, convulsions |
|
| Vascular disorders |
Vasculitis |
|
| Skin and subcutaneous tissue |
Angioneurotic edema, lichen planus, erythema multiforme |
|
| Musculos游戏副本-м’язова система та сполучна тканина |
Arthritis, muscle weakness |
|
| General disorders and injection site reactions |
Pain at injection site at time of vaccination |
|
| During widespread use of monovalent hepatitis A and/or hepatitis B vaccines, the following adverse reactions have additionally been reported and considered temporally associated with vaccination |
||
| Nervous system |
Multiple sclerosis, myelitis, facial paralysis, polyneuritis such as Guillain-Barré syndrome (with ascending paralysis), optic neuritis |
|
| General disorders and injection site reactions |
Pricking and burning sensations |
|
| Investigations |
Abnormal liver function test results |
|
Children aged 1 to 15 years
In clinical studies, 2029 doses of the TWINRIX vaccine were administered to 1027 individuals aged 1 to 15 years inclusive.
In two comparative studies involving subjects aged 1 to 15 years inclusive, the incidence of local and general symptoms following the 2-dose vaccination schedule of TWINRIX was similar to that observed with the 3-dose vaccination schedule using a vaccine containing 360 ELISA units of HAV and 10 µg of HBsAg.
The most frequently reported adverse reactions following administration of the TWINRIX vaccine are pain and fatigue, occurring at approximately a frequency of 50% and 30% per administered dose, respectively.
The following adverse reactions were reported during clinical trials with the TWINRIX vaccine:
| Organs and systems |
Frequency |
Adverse reactions |
| Clinical trials |
||
| Metabolism and nutrition disorders |
Very common |
decreased appetite |
| Psychiatric disorders |
Very common |
irritability |
| Nervous system |
Very common |
headache |
| Common |
drowsiness |
|
| Gastrointestinal system |
Common |
gastrointestinal symptoms |
| General disorders and administration site conditions |
Very common |
pain and redness at injection site, fatigue |
| Common |
swelling at injection site, fever |
|
| Additional adverse reactions reported during clinical trials with combined vaccines for prevention of hepatitis A or B manufactured by GlaxoSmithKline (using 3-, 4-dose schedules). |
||
| Infections and infestations |
Uncommon |
upper respiratory tract infections |
| Blood and lymphatic system |
Rare |
lymphadenopathy |
| Nervous system |
Uncommon |
dizziness |
| Rare |
paraesthesia |
|
| Vascular system |
Rare |
hypotension |
| Gastrointestinal system |
Common |
diarrhea, nausea |
| Uncommon |
vomiting |
|
| Skin and subcutaneous tissue |
Rare |
rash, pruritus |
| Very rare |
urticaria |
|
| Musculoskeletal and connective tissue system |
Uncommon |
myalgia |
| Rare |
arthralgia |
|
| General disorders and administration site conditions |
Common |
malaise, injection site reaction |
| Rare |
influenza-like symptoms, chills |
|
Post-marketing data
Since the adverse reactions listed below are spontaneously reported, it is not possible to determine their frequency.
The following adverse reactions have been observed during post-marketing surveillance of vaccination with TWINRIX vaccine.
| Organs and systems |
Adverse reactions |
| Immune system |
allergic reactions, including anaphylactic and anaphylactoid reactions |
| Nervous system |
syncope or vasovagal reactions to injection, localized hypoaesthesia |
| During widespread use of both combined hepatitis A and hepatitis B vaccines and monovalent hepatitis A and/or hepatitis B vaccines manufactured by GlaxoSmithKline, the following additional adverse reactions have been reported |
|
| Infections and infestations |
Meningitis |
| Blood and lymphatic system |
Thrombocytopenia, thrombocytopenic purpura |
| Immune system |
Allergic reactions, including serum sickness-like reactions, angioneurotic edema |
| Nervous system |
Multiplex sclerosis, encephalitis, encephalopathies, polyneuritis such as Guillain-Barré syndrome (with ascending paralysis), myelitis, convulsions, paralysis, neuritis, optic neuritis, neuropathies |
| Vascular disorders |
Vasculitis |
| Hepatobiliary system |
Abnormal liver function tests |
| Skin and subcutaneous tissue |
Lichen planus, erythema multiforme |
| Musculoskeletal and connective tissue system |
Arthritis, muscle weakness |
| General disorders and administration site reactions |
Pain, burning and warmth at injection site at the time of vaccine administration |
Reporting of suspected adverse reactions
Reporting of adverse reactions after medicinal product registration is important. It allows ongoing monitoring of the benefit/risk balance of the medicinal product. Medical and pharmaceutical professionals, as well as patients or their legal representatives, should report all cases of suspected adverse reactions and lack of effectiveness of the medicinal product via the Automated Information System for Pharmacovigilance at the following link: https://aisf.dec.gov.ua.
Shelf life.
36 months. The expiry date of the vaccine is indicated on the label and packaging.
Storage conditions.
The vaccine must be stored at a temperature of 2 to 8 °C in a place protected from light. Store out of reach of children.
Do not freeze. If the vaccine has been frozen, it must be destroyed.
Incompatibilities.
Due to the lack of compatibility studies, this medicinal product must not be mixed with other medicinal products.
Packaging.
Suspension for injection, 1 dose (1 mL/dose) in a pre-filled syringe No. 1, supplied with a needle.
The cap and the plunger of the pre-filled syringe are made of synthetic rubber.
Prescription status. Prescription only.
Manufacturer. GlaxoSmithKline Biologicals S.A., Belgium.
Manufacturer's address and location of operations.
Rue de l’Institut, 89, 1330 Rixensart, Belgium.
Marketing authorization holder and/or its representative.
LLC "GlaxoSmithKline Pharmaceuticals Ukraine".
Address of the marketing authorization holder and/or its representative.
1-V Pavla Tychyny Avenue, Kyiv, 02152, Tel: (044) 585-51-85, Fax: (044) 585-51-92.
All suspected adverse reactions and lack of effectiveness of the medicinal product can be reported to LLC "GlaxoSmithKline Pharmaceuticals Ukraine" via 24/7 hotline (044) 585-51-85 or by email at [email protected].