Salbutamol-inteli
Ukraine
Table of Contents
INSTRUCTIONS FOR MEDICAL USE OF THE MEDICINAL PRODUCT SАLBUTAMOL-INTELI (SALBUTAMOL-INTELI)
Composition:
Active substance: salbutamol;
One dose contains salbutamol (as sulfate) 100 mcg;
Excipients: oleic acid, anhydrous ethanol, 1,1,1,2-tetrafluoroethane (HFA-134a).
Pharmaceutical form. Pressurized inhalation, suspension.
Main physico-chemical characteristics: white pressurized metered-dose aerosol suspension for 200 doses (10 ml).
Pharmacotherapeutic group. Drugs for treatment of obstructive airway diseases. Selective β2-adrenoreceptor agonists. ATC code R03AC02.
Pharmacological properties.
Pharmacodynamics.
Salbutamol is a selective β2-adrenergic receptor agonist. At therapeutic doses, it acts on β2-adrenergic receptors of bronchial smooth muscle, providing rapid (within 5 minutes) and short-acting (4–6 hours) bronchodilation in patients with reversible airway obstruction.
Pharmacokinetics.
After inhaled administration, 10 to 20% of the administered dose reaches the lower respiratory tract. The remainder remains in the inhalation device or in the oropharynx, from where it is swallowed. Part of the dose reaching the airways is absorbed into lung tissue and enters systemic circulation but is not metabolized in the lungs.
After entering systemic circulation, the drug is metabolized in the liver and is primarily excreted by the kidneys, both unchanged and as a phenolsulfate metabolite.
The portion of the dose swallowed from the oropharynx is absorbed from the gastrointestinal tract, undergoes first-pass metabolism in the liver to the phenolsulfate compound, and is then excreted by the kidneys. Most of the drug is eliminated from the body within 72 hours. Plasma protein binding is 10%.
Clinical characteristics.
Indications.
Short-term (4 to 6 hours) bronchodilation with rapid onset (within approximately 5 minutes) in airway obstruction.
Relief of asthma attacks in diseases associated with reversible airway obstruction, such as bronchial asthma.
Prevention of bronchospasm attacks caused by allergens or physical exertion.
As part of combination therapy in patients with bronchial asthma.
Contraindications.
Hypersensitivity to any component of the medicinal product. Salbutamol dosage forms not intended for intravenous administration must not be used to suppress uncomplicated preterm labor or threatened abortion.
Interaction with other medicinal products and other forms of interaction.
Salbutamol must not be used concomitantly with non-selective β-blockers, such as propranolol (including ophthalmic preparations containing β-blockers).
Concomitant use of salbutamol with monoamine oxidase inhibitors (MAO inhibitors) is not contraindicated.
Special precautions for use.
To ensure optimal delivery of the medicinal product to the patient's lungs, the patient's inhalation technique should be checked. Patients should be informed that they may experience a different taste compared to that when using a previous inhaler.
Sudden and progressive worsening of bronchial asthma is a life-threatening condition requiring initiation or increase of corticosteroid therapy. Patients at risk are recommended to perform daily peak expiratory flow monitoring.
Asthma treatment is generally carried out according to a stepwise approach, which requires continuous clinical monitoring with pulmonary function tests.
Bronchodilators should not be the sole treatment method for patients with severe or unstable asthma. Severe asthma requires constant medical supervision, as such patients are at high risk of severe asthma attack. In such cases, the physician should consider the possibility of using the maximum recommended dose of inhaled or systemic corticosteroids.
Patients receiving regular anti-inflammatory therapy (e.g., inhaled corticosteroids) should be advised to continue taking anti-inflammatory medications even when symptoms subside and they do not require salbutamol.
An increased frequency of using short-acting bronchodilators, particularly beta-2 agonists, to relieve symptoms indicates worsening asthma control, and patients should be warned to seek medical help as soon as possible. In such cases, the patient's treatment plan should be reassessed.
Excessive use of short-acting beta-agonists may mask the progression of the underlying disease and contribute to worsening asthma control, increasing the risk of severe asthma exacerbations and mortality.
Patients using salbutamol more than twice a week "as needed," excluding prophylactic use before physical exertion, should undergo re-evaluation (e.g., daytime symptoms, nocturnal awakenings, and activity limitations due to asthma) for appropriate adjustment of therapy, as these patients belong to the risk group for excessive salbutamol use.
If a previously effective inhaled dose of salbutamol fails to relieve symptoms for at least 3 hours, the patient should be advised to consult a physician. Dose or frequency increases should only be made by a physician.
To enhance treatment efficacy, patients should be trained in correct inhaler use, and the inhaler should initially be used under medical supervision.
Severe asthma exacerbation should be treated in the usual manner.
Salbutamol should be prescribed with caution in patients with thyrotoxicosis, heart failure, arterial hypertension, aneurysm, impaired glucose tolerance, diabetes mellitus, pheochromocytoma, and when used concomitantly with cardiac glycosides.
Use with caution in patients with myocardial ischemia, tachycardia, hypertrophic obstructive cardiomyopathy, glaucoma, and cardiac arrhythmias.
The use of β2-adrenergic receptor agonists may cause potentially dangerous hypokalemia, especially after parenteral or aerosol administration. Particular caution is required in severe acute asthma, as this effect may be intensified by concomitant use of xanthine derivatives, corticosteroids, diuretics, and hypoxia. In such cases, regular monitoring of serum potassium levels is recommended.
Adverse cardiovascular effects may occur with sympathomimetic agents, including salbutamol. Post-marketing surveillance and published literature have reported cases of myocardial ischemia during salbutamol therapy. Patients with severe cardiac conditions (such as ischemic heart disease, arrhythmia, or severe heart failure) should be warned to seek immediate medical attention if chest pain or other symptoms of cardiac exacerbation occur. Particular attention should be paid to identifying the causes of symptoms such as dyspnea and chest pain, as they may originate from either respiratory or cardiac disorders.
Salbutamol should be used with caution in patients receiving high doses of other sympathomimetic agents. Like other beta-adrenergic agonists, salbutamol may cause reversible metabolic changes, such as increased blood glucose levels. Compensation for these changes in diabetic patients is not always possible, and there have been isolated reports of ketoacidosis in such patients. Concomitant use of corticosteroids may exacerbate this condition.
As with other inhaled medications, paradoxical bronchospasm with immediate worsening of dyspnea after administration may occur. In such cases, alternative formulations or other fast-acting inhaled bronchodilators should be prescribed immediately. Salbutamol should be discontinued promptly, the patient's condition assessed, and, if necessary, another fast-acting bronchodilator prescribed for regular use.
Use during pregnancy or breastfeeding.
Large, well-controlled clinical studies on the use of salbutamol in pregnant women have not been conducted. Animal studies indicate reproductive toxicity of salbutamol. The safety of salbutamol use during pregnancy has not been established. There have been isolated reports of various congenital malformations in intrauterine development, including cleft palate, limb defects, and cardiac abnormalities. Some women received multiple other medications during pregnancy. Like other medicinal products, salbutamol should be prescribed during pregnancy only if the expected benefit outweighs the potential risk to the fetus.
Salbutamol is likely excreted in breast milk; therefore, it should be prescribed to breastfeeding women with caution. It is unknown whether salbutamol in breast milk has harmful effects on the newborn infant. Therefore, its use in breastfeeding women should be limited to cases where the benefit to the mother outweighs the potential risk to the infant.
Ability to affect reaction speed when driving or operating machinery.
There are no data on the effect of salbutamol on driving or operating machinery. However, if nervous system side effects (e.g., tremor) occur, driving or operating machinery should be avoided.
Method of Administration and Dosage
Salbutamol-Intel is an aerosol intended only for inhalation via the mouth. For patients who have difficulty coordinating breathing with the use of an inhaler, the additional use of a spacer – a device facilitating inhalation of inhaled medications – is recommended.
Adults (including elderly patients)
To relieve acute asthma symptoms, including acute bronchospasm, a minimum initial dose of 1 inhalation (100 mcg) may be used. If necessary, the dose can be increased to 200 mcg (2 inhalations).
For prophylaxis prior to physical exertion or anticipated exposure to allergens, 200 mcg (2 inhalations) should be administered 10–15 minutes before the expected exposure to allergens or physical activity. The total daily dose of salbutamol must not exceed 800 mcg (8 inhalations).
For long-term maintenance therapy, 200 mcg (2 inhalations) four times daily is recommended.
Children aged 4 to 12 years
To relieve acute bronchospasm, administer 1 inhalation (100 mcg). If necessary, the dose can be increased to 200 mcg (2 inhalations).
Children aged 12 years and older should receive adult doses.
For prophylaxis, 100 mcg (1 inhalation) should be administered 10–15 minutes before physical exertion or anticipated allergen exposure; if necessary, the dose can be increased to 200 mcg (2 inhalations).
For long-term maintenance therapy, 200 mcg (2 inhalations) four times daily is recommended.
The total daily dose of salbutamol must not exceed 800 mcg (8 inhalations).
Increased need for β2-agonists may indicate worsening of asthma control. Under such circumstances, the patient’s treatment regimen should be reviewed and the need for initiating glucocorticosteroid therapy should be considered.
Instructions for Proper Use
Before using the aerosol, check the expiration date of the medication. If the inhaler is new or has not been used for several days, it should be shaken well and one dose should be released into the air to ensure proper functioning.
|
|
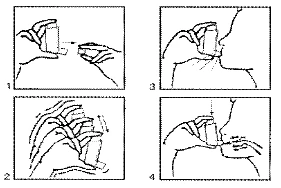
- After inhaling, hold your breath to allow maximum penetration of the medication.
- If necessary, continue for several seconds and repeat the procedure again (steps 3, 4, 5, and 6).
- Close with the cap after use.
The plastic adapter must be cleaned regularly. To clean, remove the metal container and wash the adapter with warm (not hot) soapy water.
Rinse thoroughly, dry the adapter completely, and reassemble the device. After reassembly, close with the cap.
Children.
The medication is contraindicated in children under 4 years of age.
Overdose.
The most common signs and symptoms of salbutamol overdose are transient pharmacologically induced beta-agonist effects, such as tachycardia, tremor, hyperactivity, and metabolic disturbances, including hypokalemia (see sections "Special precautions for use" and "Adverse reactions").
Salbutamol overdose may lead to hypokalemia; therefore, serum potassium levels should be monitored. Cases of lactic acidosis have been reported following high therapeutic doses or overdose of short-acting beta2-agonists. Thus, serum lactate levels should be checked, and metabolic acidosis should be monitored accordingly, especially in the presence of persistent or increasing respiratory rate despite improvement in bronchospasm symptoms such as stridorous breathing.
Treatment. Treatment is symptomatic. Cardioselective beta-blockers are generally preferred. Beta-blocker medications should be prescribed with caution in patients with a history of bronchospasm.
Side effects.
The adverse reactions listed below are classified by organs and systems and by frequency of occurrence: very common (≥ 1/10), common (≥ 1/100 and < 1/10), uncommon (≥ 1/1,000 and < 1/100), rare (≥ 1/10,000 and < 1/1,000), very rare (<1/10,000), including isolated cases, frequency not known.
Immune system disorders
Very rare: hypersensitivity reactions, including angioedema, urticaria, bronchospasm, hypotension, and collapse.
Metabolism and nutrition disorders
Rare: hypokalemia. Potentially, the use of β2-agonists may cause pronounced hypokalemia, increased serum lactate levels/lactic acidosis.
Nervous system disorders
Common: tremor, headache.
Very rare: hyperactivity.
Cardiac disorders
Common: tachycardia.
Uncommon: palpitations.
Very rare: cardiac arrhythmia (including atrial fibrillation, supraventricular tachycardia, and extrasystoles).
Frequency not known: myocardial ischemia (see section "Special precautions").
Vascular disorders
Rare: peripheral vasodilation.
Respiratory, thoracic and mediastinal disorders
Very rare: paradoxical bronchospasm.
Gastrointestinal disorders
Uncommon: irritation of the mucous membranes of the mouth and pharynx.
Musculoskeletal and connective tissue disorders
Uncommon: muscle cramps.
Shelf life.
3 years.
Storage conditions.
Store at a temperature not exceeding 30 °C.
Keep out of reach and sight of children.
Pressurized container – do not pierce. Do not throw into fire, even if empty.
Protect from direct sunlight. Do not store near sources of heat.
Do not freeze.
Packaging.
Aluminum canister containing 200 doses (10 ml) of 100 mcg salbutamol per dose, with a plastic adapter and cap, in a cardboard box.
Prescription category.
Prescription only.
Manufacturer.
Laboratorio Aldo-Union, S.L.
Manufacturer's address and place of business.
Baronesa de Maldà, 73, 08950 Esplugues de Llobregat, Barcelona, Spain.