Novomix® 30 flexpen®
Ukraine
Table of Contents
I N S T R U C T I O N for medical use of the medicinal product NOVOMIX® 30 FLEXPEN® (NOVOMIX® 30 FLEXPEN®)
Composition:
active substance: 1 ml of injectable suspension contains 100 IU/ml insulin aspart (rDNA) (30% soluble insulin aspart and 70% insulin aspart crystallized with protamine);
1 pen-injector contains 3 ml, equivalent to 300 IU;
1 unit (IU) equals 6 nmol or 0.035 mg of salt-free anhydrous insulin aspart;
excipients: glycerol; phenol; m-cresol; zinc chloride; sodium chloride; disodium hydrogen phosphate dihydrate; protamine sulfate; sodium hydroxide; hydrochloric acid diluted; water for injections.
Pharmaceutical form. Injectable suspension.
Main physicochemical properties: white homogeneous suspension without aggregates or particles. Upon standing, separation into a white sediment and a colorless supernatant liquid occurs.
Pharmacotherapeutic group. Antidiabetic agents. Insulins and analogues for injection,
combinations of short-acting insulins with intermediate- or long-acting insulins.
ATC code A10AD05.
Pharmacological Properties.
Pharmacodynamics.
NovoMix® 30 FlexPen® is a biphasic suspension of soluble insulin aspart (an analogue of short-acting insulin) and protamine-crystallized insulin aspart (an analogue of intermediate-acting insulin). The suspension contains 30% short-acting and 70% intermediate-acting insulin aspart in a 30/70 ratio. When administered in equimolar doses, insulin aspart is equipotent to human insulin.
Mechanism of action.
The glucose-lowering effect of insulin results from enhanced tissue uptake of glucose following insulin binding to receptors on muscle and fat cells, along with simultaneous inhibition of glucose release from the liver.
NovoMix® 30 FlexPen® begins to act within 10–20 minutes after subcutaneous injection. Maximum effect develops within 1–4 hours after administration. Duration of action lasts up to 24 hours.
In a 3-month clinical study comparing administration of NovoMix® 30 FlexPen® versus biphasic human insulin 30 before breakfast and dinner in patients with type 1 and type 2 diabetes, NovoMix® 30 FlexPen® resulted in significantly lower blood glucose levels after both meals (breakfast and dinner) compared to biphasic human insulin 30.
In a meta-analysis including 9 clinical trials in patients with type 1 and type 2 diabetes, NovoMix® 30 FlexPen® administered before breakfast and dinner resulted in significantly better postprandial glucose control compared to biphasic human insulin 30 (based on mean post-meal glucose excursions after breakfast, lunch, and dinner).
Despite higher fasting glucose levels observed in patients treated with NovoMix® 30 FlexPen®, the level of glycated hemoglobin (HbA1c), a marker of overall glycemic control, was similar.
In a clinical study of patients with type 2 diabetes (341 patients), randomized to receive either NovoMix® 30 FlexPen® alone, NovoMix® 30 FlexPen® in combination with metformin, or metformin plus a sulfonylurea, the primary efficacy endpoint HbA1c after 16 weeks of treatment did not differ between patients receiving NovoMix® 30 FlexPen® with metformin and those receiving metformin with a sulfonylurea. In this study, 57% of patients had baseline HbA1c >9%; in these patients, treatment with NovoMix® 30 FlexPen® in combination with metformin resulted in a greater reduction in HbA1c compared to metformin plus sulfonylurea.
In a study of patients with type 2 diabetes in whom glycemic control with oral antidiabetic agents alone was ineffective, patients were treated with twice-daily NovoMix® 30 FlexPen® (117 patients) or once-daily insulin glargine (116 patients). After 28 weeks of treatment with dose titration, HbA1c decreased by 2.8% (mean baseline HbA1c was 9.7%). With NovoMix® 30 FlexPen® treatment, 66% of patients achieved HbA1c <7% and 42% achieved HbA1c <6.5%. Fasting plasma glucose decreased by approximately 7 mmol/L (from 14.0 mmol/L before treatment to 7.1 mmol/L).
In a meta-analysis of patients with type 2 diabetes, the risk of nocturnal hypoglycemia and severe hypoglycemia was lower with NovoMix® 30 FlexPen® compared to biphasic human insulin 30. However, the risk of daytime hypoglycemic episodes was higher in patients receiving NovoMix® 30 FlexPen®.
Children and adolescents. In a 16-week study involving 167 patients aged 10–18 years, the efficacy of postprandial glycemic control was compared between NovoMix® 30 FlexPen® administered at meals and biphasic human insulin 30 administered at meals with bedtime NPH insulin injections. Throughout the study period, HbA1c concentrations remained stable in both groups, and no differences in the frequency of hypoglycemic episodes were observed between NovoMix® 30 FlexPen® and biphasic human insulin 30.
In a small double-blind crossover study (12 weeks per treatment period) involving 54 children aged 6–12 years, the number of hypoglycemic episodes and postprandial glucose levels were statistically significantly lower with NovoMix® 30 compared to biphasic human insulin 30. However, at the end of treatment, HbA1c levels were significantly lower in the group receiving biphasic human insulin 30 than in the group receiving NovoMix® 30 FlexPen®.
Elderly patients. The pharmacodynamics of NovoMix® 30 FlexPen® have not been studied in elderly patients. However, a randomized, double-blind crossover study comparing the pharmacokinetics and pharmacodynamics of insulin aspart and soluble human insulin was conducted in 19 patients with type 2 diabetes aged 65–83 years (mean age 70 years). The relative differences in pharmacodynamic parameters (GIRmax, AUCGIR, 0–120 min) after administration of insulin aspart or human insulin in these patients were similar to those observed in healthy subjects or younger patients with diabetes.
Pharmacokinetics.
In insulin aspart, the amino acid proline at position B28 of the insulin molecule is replaced by aspartic acid, which reduces its tendency to form hexamers compared to soluble human insulin preparations. In the soluble phase of NovoMix® 30 FlexPen®, insulin aspart constitutes 30% of total insulin: it is absorbed into the bloodstream more rapidly from the subcutaneous tissue than soluble insulin in biphasic human insulin.
The remaining 70% is in the crystalline protamine-insulin aspart form, which has a prolonged absorption profile similar to that of human NPH insulin.
After administration of NovoMix® 30 FlexPen®, maximum insulin concentration in serum is 50% higher and the time to peak concentration is twice as short compared to biphasic human insulin 30. In healthy volunteers, after subcutaneous administration of NovoMix® 30 FlexPen® at a dose of 0.20 IU/kg body weight, maximum serum insulin aspart concentration was reached within 60 minutes and amounted to 140 ± 32 pmol/L. The elimination half-life (t½) of NovoMix® 30 FlexPen®, reflecting the absorption rate of the protamine-bound fraction, was approximately 8–9 hours. Serum insulin levels returned to baseline within 15–18 hours after subcutaneous injection. In patients with type 2 diabetes, maximum concentration was reached within 95 minutes and remained above baseline for at least 14 hours.
Elderly patients. The pharmacokinetics of NovoMix® 30 FlexPen® have not been studied in elderly patients. However, relative differences in pharmacokinetic parameters after administration of insulin aspart or human insulin in elderly and older adult patients with type 2 diabetes (65–83 years, mean age 70 years) were similar to those in healthy subjects or younger patients with diabetes. In elderly patients, absorption rate was reduced, as indicated by a longer time to maximum serum insulin concentration (tmax: 82 minutes, interquartile range 60–120 minutes). However, Cmax values were similar to those in younger patients with type 2 diabetes and slightly lower than in patients with type 1 diabetes.
Renal and hepatic impairment.
The pharmacokinetics of NovoMix® 30 FlexPen® have not been studied in patients with renal or hepatic impairment.
Children and adolescents. The pharmacokinetics of NovoMix® 30 FlexPen® in children and adolescents have not been studied. However, in children (6–12 years) and adolescents (13–17 years) with type 1 diabetes, the pharmacokinetics and pharmacodynamics of soluble insulin aspart have been investigated. It was rapidly absorbed in both age groups, with tmax values similar to those in adults. However, Cmax values varied significantly between age groups, indicating the importance of individual insulin aspart dose adjustment.
Non-clinical safety data.
Non-clinical data from traditional safety pharmacology studies (repeated-dose toxicity, genotoxicity, and toxic effects on reproductive function and fetal development) revealed no specific hazard for humans associated with the use of NovoMix® 30 FlexPen®.
In vitro tests, including binding to insulin and IGF-1 receptors and effects on cell growth, showed insulin aspart to behave similarly to human insulin. Studies also demonstrated that dissociation from the insulin receptor for insulin aspart is equivalent to that of human insulin.
Clinical characteristics.
Indications.
NovoMix® 30 FlexPen® is indicated for the treatment of diabetes mellitus in adults, adolescents, and children aged 10 years and older.
Contraindications.
Hypersensitivity to the active substance or to any of the excipients (see section "Composition").
Interaction with other medicinal products and other forms of interaction.
It is known that a number of medicinal products affect glucose metabolism, which should be taken into account when determining the insulin dose.
Medicinal products that may decrease insulin requirements
Oral hypoglycemic agents (OHAs), GLP-1 receptor agonists, monoamine oxidase inhibitors,
β-blockers, angiotensin-converting enzyme inhibitors, salicylates, anabolic steroids, and sulfonamides.
Medicinal products that may increase insulin requirements
Oral contraceptives, thiazides, glucocorticoids, thyroid hormones, sympathomimetics, growth hormone, and danazol.
β-blockers may mask the symptoms of hypoglycemia and delay recovery from hypoglycemia.
Octreotide/lanreotide may either increase or decrease insulin requirements.
Alcohol may potentiate or weaken the blood glucose-lowering effect of insulin.
Special precautions.
Before traveling across time zones, patients should consult their doctor, as this changes the schedule of insulin injections and meal times.
Hyperglycemia (high blood sugar).
Inadequate dosing or discontinuation of treatment (especially in type 1 diabetes) may lead to hyperglycemia and diabetic ketoacidosis. The first symptoms of hyperglycemia usually develop gradually over several hours or days. They include thirst, frequent urination, nausea, vomiting, drowsiness, skin redness and dryness, dry mouth, loss of appetite, and acetone odor on the breath.
In type 1 diabetes, untreated hyperglycemia leads to diabetic ketoacidosis, which is potentially life-threatening.
Hypoglycemia (low blood sugar).
Skipping meals or unexpected physical exertion may lead to hypoglycemia.
Hypoglycemia may occur if the insulin dose is too high relative to insulin requirements.
Do not administer the medication in case of hypoglycemia or suspected hypoglycemia.
After stabilization of blood glucose levels, the need for insulin dose adjustment should be considered.
Compared to biphasic human insulin 30, administration of NovoMix® 30 FlexPen® may result in a more pronounced hypoglycemic effect, which may last up to 6 hours after injection. This may necessitate dose adjustments of insulin and/or changes in meal patterns.
Patients whose blood glucose control has significantly improved due to intensive insulin therapy may experience changes in the usual warning symptoms of hypoglycemia; they should be informed about this in advance.
Usual warning symptoms may disappear in patients with long-standing diabetes.
Tighter blood glucose control may increase the frequency of hypoglycemic episodes; therefore, special monitoring is required during therapy intensification, as specified in the section "Dosage and administration".
Since NovoMix® 30 FlexPen® should be administered immediately before meals, the rapid onset of its action should be taken into account when treating patients with concomitant diseases or taking medications that delay gastrointestinal absorption of food.
Concomitant diseases, especially infections and fever, generally increase insulin requirements. Kidney or liver disease, or disorders of the adrenal glands, pituitary gland, or thyroid gland may necessitate insulin dose adjustments.
When patients are switched to another type of insulin, symptoms of hypoglycemia may change or become less pronounced compared to those experienced with the previous insulin.
Switching from other insulin products.
Switching a patient to another type or brand of insulin should be done under strict medical supervision. Changes in concentration, type (manufacturer), kind, origin of insulin (human insulin or human insulin analog), and/or method of production (recombinant DNA technology or animal-sourced insulin) may require a change in insulin dosage. Patients switched to NovoMix® 30 FlexPen® from another insulin may require an increased number of daily injections or changes in dosage compared to their previous insulin regimen.
Dose adjustments may be necessary both at initiation of the new product and during the first weeks or months of treatment.
Injection site reactions.
With any insulin therapy, injection site reactions may occur, including pain, redness, urticaria, inflammation, swelling, bruising, and itching.
Regular rotation of injection sites within one area may reduce or prevent these reactions. Reactions usually resolve within a few days or weeks. Rarely, injection site reactions may require discontinuation of NovoMix® 30 FlexPen®.
Skin and subcutaneous tissue disorders.
Patients should be instructed on the necessity of regularly rotating injection sites to reduce the risk of lipodystrophy and cutaneous amyloidosis. Injecting insulin into areas with such reactions may potentially delay insulin absorption and impair glycemic control. Cases of hypoglycemia after sudden switching from such affected injection sites to unaffected ones have been reported. It is recommended to monitor blood glucose levels after changing injection sites from affected to unaffected areas and to adjust antidiabetic medication doses accordingly.
Combination of pioglitazone with NovoMix® 30 FlexPen®
Cases of congestive heart failure have been reported when pioglitazone is used in combination with insulin, particularly in patients with risk factors. This should be considered when prescribing combination therapy with pioglitazone and insulin. Patients receiving these drugs concomitantly should be monitored for signs of congestive heart failure, weight gain, and edema. If cardiac function worsens, pioglitazone therapy should be discontinued.
Avoiding medication errors.
Patients should be instructed to always check the label on the insulin product before each injection to avoid confusing NovoMix® 30 FlexPen® with other insulin products.
Insulin antibodies.
Administration of insulin may lead to the formation of insulin antibodies. Very rarely, the presence of such antibodies may require insulin dose adjustments to prevent hyperglycemia or hypoglycemia.
NovoMix® 30 FlexPen® contains less than 1 mmol of sodium (23 mg); therefore, the medicinal product can be considered essentially sodium-free.
Use during pregnancy or breastfeeding.
Clinical experience with the use of NovoMix® 30 FlexPen® during pregnancy is limited.
No clinical studies with NovoMix® 30 FlexPen® in pregnant women have been conducted. However, two randomized clinical trials (involving 157 and 14 pregnant women receiving insulin aspart under a basal-bolus treatment regimen) showed no adverse effects of insulin aspart on pregnancy, the fetus, or the newborn compared to soluble human insulin.
Enhanced monitoring of insulin-treated diabetic pregnant women is recommended throughout pregnancy and in case of suspected pregnancy. Insulin requirements usually decrease during the first trimester and significantly increase during the second and third trimesters. After delivery, insulin requirements rapidly return to pre-pregnancy levels.
There are no restrictions on insulin treatment of diabetes during breastfeeding, as maternal treatment does not pose any risk to the infant. However, dose adjustments of NovoMix® 30 FlexPen® may be necessary.
Fertility.
Reproductive toxicity studies in animals using human insulin showed no adverse effects on fertility.
Ability to affect reaction speed when driving or operating machinery.
A patient's reaction and ability to concentrate may be impaired during hypoglycemia, which may pose a risk in situations where such abilities are critical (e.g., driving a vehicle or operating machinery).
Patients should be advised to take preventive measures against hypoglycemia before driving or operating machinery.
This is especially important for patients with impaired or absent hypoglycemia warning symptoms or those who experience frequent hypoglycemic episodes. In such cases, the appropriateness of driving or operating machinery should be carefully considered.
Dosage and administration.
The dosage of NovoMix® 30 FlexPen® is individual and must be determined by a physician according to the patient's needs.
To achieve optimal glycemic control, regular monitoring of blood glucose levels and insulin dose adjustments are recommended.
NovoMix® 30 FlexPen® may be prescribed to patients with type 2 diabetes mellitus both as monotherapy and in combination with oral antidiabetic drugs (OADs) and/or GLP-1 receptor agonists.
Initiating treatment.
Patients starting insulin therapy for the first time: for patients with type 2 diabetes, the recommended initial dose of NovoMix® 30 FlexPen® is 6 IU before breakfast and 6 IU before dinner. However, treatment may also be initiated with a dose of 12 IU before dinner.
When administering NovoMix® 30 FlexPen® once daily, if the dose reaches 30 IU, it is recommended to split the dose into two equal injections before breakfast and before dinner. If recurrent episodes of hypoglycemia occur during the day while using NovoMix® 30 FlexPen® twice daily, the morning dose may be divided into doses before breakfast and lunch (administration three times daily).
Switching from other insulin products.
When switching patients from biphasic human insulins to NovoMix® 30 FlexPen®, treatment should be initiated at the same doses and according to the same regimen. Subsequent dose titration should be performed according to individual patient requirements (see dose adjustment table below).
As with all insulin therapies, careful monitoring of blood glucose levels is recommended during the transition period and throughout the first weeks after switching (see section "Special Instructions", subsection "Switching from other insulin products").
Intensifying therapy.
Transition from once-daily to twice-daily administration of NovoMix® 30 FlexPen® is possible.
When administering once daily, transition to two daily injections is generally recommended once the dose reaches 30 IU, splitting the dose equally before breakfast and dinner (50:50).
When transitioning from twice-daily to three-times-daily administration: the morning dose may be divided into doses before breakfast and lunch (administration three times daily).
Dose adjustment.
- When adjusting the dose of NovoMix® 30 FlexPen®, reference should be made to the lowest fasting blood glucose values recorded over the previous three days.
- Always adjust the dose administered before meals based on previous blood glucose measurements.
- Dose adjustments may be made once weekly until the target HbA1c level is achieved.
- If episodes of hypoglycemia occurred during this period, the insulin dose should not be increased.
- Dose adjustments may be necessary for patients during periods of increased physical activity, changes in usual diet, or during concomitant illness.
When adjusting doses, it is recommended to follow the guidance provided in the table below.
| Blood glucose levels before meals |
Dose adjustment of NovoMix® 30 FlexPen® |
|
| < 4.4 mmol/L |
< 80 mg/dL |
|
| 4.4–6.1 mmol/L |
80–110 mg/dL |
0 |
| 6.2–7.8 mmol/L |
111–140 mg/dL |
+ 2 IU |
| 7.9–10 mmol/L |
141–180 mg/dL |
+ 4 IU |
| > 10 mmol/L |
> 180 mg/dL |
+ 6 IU |
In patients with type 1 diabetes mellitus, the individual daily insulin requirement ranges from 0.5 to 1.0 IU/kg/day. NovoMix® 30 FlexPen® can fully or partially meet this requirement.
For patients with type 2 diabetes mellitus who are using NovoMix® 30 FlexPen® and have HbA1c less than 8%, a 20% dose reduction is recommended when adding GLP-1 receptor agonists, in order to reduce the risk of hypoglycemia. For patients with HbA1c greater than 8%, consideration should be given to reducing the dose. Thereafter, the dose should be individually adjusted.
Special populations.
As with other insulin products, increased glucose monitoring and individual adjustment of insulin aspart dosage are recommended for patients in special populations.
Elderly patients (≥ 65 years).
NovoMix® 30 FlexPen® can be used in elderly patients; however, experience with its use in combination with OADs in patients aged 75 years and older is limited.
Renal and hepatic impairment.
Impaired renal or hepatic function may reduce the patient's insulin requirements.
Children.
NovoMix® 30 FlexPen® can be used in adolescents and children aged 10 years and older when treatment with biphasic insulins is preferred. Clinical trial data on the use of the product in children aged 6–9 years are limited (see section "Pharmacodynamics").
Studies in children under 6 years of age have not been conducted.
Method of administration.
NovoMix® 30 FlexPen® is intended exclusively for subcutaneous administration.
NovoMix® 30 FlexPen® must never be administered intravenously, as this may lead to severe hypoglycemia. Intramuscular administration should also be avoided. NovoMix® 30 FlexPen® must not be used in infusion pumps.
NovoMix® 30 FlexPen® is usually administered by subcutaneous injection into the thigh or abdominal wall. If convenient, it may also be administered into the buttocks or the deltoid region of the upper arm.
Injection sites should be rotated, even within the same body area, to reduce the risk of lipodystrophy and cutaneous amyloidosis.
As with other insulin products, the duration of action may vary depending on dose, injection site, blood flow, temperature, and the patient's level of physical activity.
Since the onset of action of NovoMix® 30 FlexPen® is faster than that of biphasic human insulin 30, it should be administered immediately before a meal. If necessary, NovoMix® 30 FlexPen® may also be administered shortly after a meal.
Instructions for use of NovoMix® 30 FlexPen®.
Before using the FlexPen® device, read these instructions carefully.
Failure to follow these instructions may result in administering too little or too much insulin, which could lead to a sudden increase or decrease in blood glucose levels.
FlexPen® is a pre-filled insulin pen with a dose selector allowing doses from 1 to 60 units of insulin in 1-unit increments. NovoMix® 30 FlexPen® is used with NovoFine® or NovoTwist® needles up to 8 mm in length. Always keep a spare pen available in case your NovoMix® 30 FlexPen® is damaged or lost.

Pen care.
▶ Handle the FlexPen® device with care. If it has been dropped, damaged, or deformed, insulin leakage may occur. This could lead to incorrect dosing, resulting in high or low blood sugar levels.
▶ The surface of the FlexPen® device may be cleaned by wiping it with cotton moistened with ethyl alcohol. Do not immerse the pen in alcohol, wash it, or lubricate it. This may damage the pen mechanism.
▶ Do not refill the FlexPen® device.
| Resuspending insulin. Check the label for the name and color to ensure that the pen contains the correct type of insulin. This is especially important if you are using more than one type of insulin. Another type of insulin may sharply increase or decrease your blood sugar level. |
|
| Using a new insulin pen Fig. A. Before use, the insulin should be at room temperature. This facilitates resuspension. Remove the cap from the insulin pen. |
|
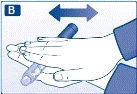
| Fig. B. Before the first injection with a new pen, the insulin must be resuspended: Roll the NovoMix® 30 FlexPen® between your palms 10 times, making sure that the cartridge remains in a horizontal position. |
|
| Fig. C. After this, invert the cartridge up and down at least 10 times between the two positions so that the glass ball inside moves from one end of the cartridge to the other. Repeat these steps until the liquid inside becomes uniformly white and cloudy. Performing the next injection Invert the pen up and down between the two positions at least 10 times until the liquid becomes uniformly white and cloudy. Before each injection, ensure that the insulin has been resuspended. This may reduce the risk of sudden increase or decrease in blood sugar levels. After resuspension, immediately proceed with the following steps to perform the injection: |
|
|
|
|
| Attaching the needle. |
|
| Fig. D. Take a new needle and remove the paper label from it. Screw the needle tightly onto the NovoMix® 30 FlexPen®. |
|
| Fig. E. Remove the outer large needle cap. Do not discard it. |
|
| Fig. F. Remove the inner needle cap and discard it. Never attempt to re-cover a removed inner needle cap, as you may injure yourself with the needle. |
|
|
|
|
| Checking insulin flow. When using the pen, a small amount of air may accumulate in the cartridge. To prevent injecting air and to ensure delivery of the required insulin dose, follow these steps: |
|
| Fig. G. Set the dose selector to 2 units. |
|
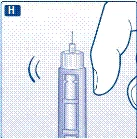
| Fig. H. Hold the NovoMix® 30 FlexPen® vertically with the needle pointing upward. Gently tap the cartridge several times with your finger to bring air bubbles to the top of the cartridge. |
|
| Fig. I. While holding the pen vertically with the needle pointing upward, press the injection button. The dose selector will return to zero. A drop of insulin should appear at the needle tip. If it does not, replace the needle and repeat this procedure no more than 6 times. If a drop of insulin still does not appear, this indicates that the pen is defective and a new pen should be used. |
|
|
|
|
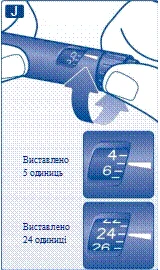
| Setting the dose. Ensure that the dose selector is set to "0". |
|
| Fig. J. Set the required dose for injection. The set dose can be adjusted upward or downward by rotating the dose selector in the appropriate direction until the required dose aligns with the dose indicator. While turning the selector, be careful not to press the injection button accidentally, as this may cause insulin leakage. A dose cannot be set that exceeds the number of units remaining in the cartridge. |
|
|
|
|
| Injecting insulin. Insert the needle under the skin. Follow the injection technique taught by your doctor or nurse. |
|
| Fig. K. Inject the dose by pressing the injection button fully until "0" aligns with the dose indicator. During injection, press only the injection button. Rotating the dose selector will not deliver insulin. |
|
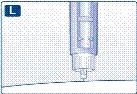
| Fig. L. Keep the injection button fully pressed and keep the needle under the skin for at least 6 seconds. This ensures delivery of the full dose. Remove the needle from the skin and release the injection button. Always ensure that the dose indicator returns to "0" after injection. If the dose indicator stops before returning to "0", the full dose was not delivered, which may affect blood sugar levels. |
|
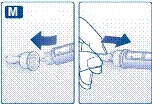
| Fig. M. Cover the needle with the large outer cap without touching it. When the needle is fully covered by the large outer cap, gently press the cap on and then unscrew the needle. Dispose of the needle safely and replace the cap on the insulin pen. |
|
|
|
|
| Additional important information
|
|

 Make sure that at least 12 units of insulin remain in the cartridge to allow proper resuspension. If less than 12 units remain, use a new NovoMix® 30 FlexPen®. The 12-unit mark is indicated on the insulin remaining scale (see the large illustration at the beginning of the NovoMix® 30 FlexPen® instructions for use).
Make sure that at least 12 units of insulin remain in the cartridge to allow proper resuspension. If less than 12 units remain, use a new NovoMix® 30 FlexPen®. The 12-unit mark is indicated on the insulin remaining scale (see the large illustration at the beginning of the NovoMix® 30 FlexPen® instructions for use). 





Children.
NovoMix® 30 FlexPen® may be used in adolescents and children aged 10 years and older when a preference exists for treatment with biphasic insulins. Clinical data on the use of the medicinal product in children aged 6–9 years are limited (see section "Pharmacodynamics").
Studies in children under 6 years of age have not been conducted.
Overdose.
Although a specific definition of insulin overdose has not been established, hypoglycaemia may develop in a stepwise manner following administration of doses higher than the patient's requirements.
- Mild hypoglycaemia can be treated by oral administration of glucose or sugary products. Therefore, diabetic patients are advised to always carry sugar-containing foods with them.
- In cases of severe hypoglycaemia, when the patient is unconscious, individuals who have received appropriate training should administer glucagon subcutaneously or intramuscularly (0.5 to 1.0 mg), or a healthcare professional should administer intravenous glucose. Intravenous glucose must be administered if the patient does not respond to glucagon within 10–15 minutes.
After the patient regains consciousness, carbohydrates should be administered orally to prevent recurrence.
Adverse Reactions
Adverse reactions observed in patients receiving NovoMix® 30 FlexPen® are mostly manifestations of the pharmacological action of insulin. The frequency of hypoglycemia varies among different patient groups, dosing regimens, and levels of glycemic control, as described below.
At the beginning of insulin therapy, transient refractive disturbances, edema, and injection site reactions (pain, redness, urticaria, inflammation, bruising, swelling, and itching at the injection site) may occur; these reactions are usually transient. Rapid improvement in glucose control may lead to a reversible condition of acute painful neuropathy.
Rapid improvement in glycemic control due to intensified insulin therapy may be accompanied by a temporary worsening of diabetic retinopathy, whereas long-term, well-established glycemic control reduces the risk of progression of diabetic retinopathy.
Based on clinical trial data, the adverse reactions listed below are classified by frequency and by system organ class according to MedDRA. Reactions are categorized by frequency as very common (≥ 1/10); common (≥ 1/100, < 1/10); uncommon (≥ 1/1000, < 1/100); rare (≥ 1/10000, < 1/1000); very rare (< 1/10000); and frequency not known (cannot be estimated from available data).
Immune system disorders
Urticaria, rash, erythema – uncommon.
Anaphylactic reactions* – very rare.
Metabolism and nutrition disorders
Hypoglycemia* – very common.
Nervous system disorders
Peripheral neuropathies (painful neuropathies) – uncommon.
Eye disorders
Refractive disturbances – uncommon.
Diabetic retinopathy – uncommon.
Skin and subcutaneous tissue disorders
Lipodystrophy* – uncommon. Frequency not known – skin amyloidosis*†.
General disorders and administration site conditions
Injection site reactions – uncommon.
Edema – uncommon.
*See section "Description of selected adverse reactions".
†See information from post-marketing surveillance.
Description of selected adverse reactions
Anaphylactic reactions.
Symptoms of generalized hypersensitivity reactions (including generalized skin rash, pruritus, sweating, gastrointestinal disturbances, angioedema, dyspnea, tachycardia, and decreased blood pressure) are very rare but may be potentially life-threatening.
Hypoglycemia.
Hypoglycemia is the most common adverse event and may occur when the insulin dose significantly exceeds the patient's insulin requirement. Severe hypoglycemia may lead to loss of consciousness and/or seizures, resulting in temporary or permanent impairment of brain function and even death. Symptoms of hypoglycemia usually appear suddenly and may include cold sweat, pallor, cold and clammy skin, fatigue, nervousness or tremor, anxiety, unusual tiredness or weakness, confusion, difficulty concentrating, drowsiness, excessive hunger, visual disturbances, headache, nausea, and tachycardia.
In clinical trials, the frequency of hypoglycemia varied depending on the patient population, dosing regimen, and level of glycemic control.
In clinical studies, the frequency of severe hypoglycemic episodes in patients receiving insulin aspart was the same as in patients receiving human insulin.
Skin and subcutaneous tissue disorders
Lipodystrophy (including lipohypertrophy, lipoatrophy) and skin amyloidosis may develop at injection sites and may delay insulin absorption from the injection site. Regular rotation of injection sites within a given area may reduce or prevent the development of these reactions.
Children
Based on post-marketing surveillance and clinical studies, adverse reactions in children do not differ in frequency, type, or severity from those in the general population.
Other special patient groups
Based on post-marketing surveillance and clinical studies, adverse reactions in elderly patients and in patients with renal or hepatic impairment do not differ in frequency, type, or severity from those in the general population.
Reporting suspected adverse reactions
After marketing authorization, it is important to report suspected adverse reactions. This allows continued monitoring of the benefit-risk balance of the medicinal product. Healthcare professionals are encouraged to report suspected adverse reactions to the local pharmacovigilance authorities.
Shelf life. 2 years.
Storage conditions.
The NovoMix® 30 FlexPen® pen in use should not be stored in the refrigerator. The pen in use or carried as a spare should be stored for no more than 4 weeks at a temperature not exceeding 30 °C.
The NovoMix® 30 FlexPen® pen not in use should be stored in the original packaging at 2–8 °C (in the refrigerator).
Do not freeze.
To protect from light, store the pen with the cap on.
Keep out of reach and sight of children.
Never use insulin after the expiry date stated on the packaging.
Packaging.
The pre-filled multi-dose disposable pen contains a 3 ml cartridge made of glass (type 1), sealed at one end with a plunger made of bromobutyl rubber and at the other end with a stopper made of bromobutyl/polysoprene rubber. The cartridge is contained in a multi-dose disposable pen made of plastic. Packs of 5 or 1 pen in a cardboard box.
Prescription status. Prescription only.
Manufacturer.
A/T Novo Nordisk.
Novo Nordisk Production SAS.
Manufacturer's address.
Novo Allé, Bagsværd, 2880, Denmark.
45, avenue d'Orléans, 28000, Chartres, France.