Midazolam calcex
Ukraine
Table of Contents
INSTRUCTIONS FOR MEDICAL USE OF THE MEDICINAL PRODUCT MIDAZOLAM KALCEKS (MIDAZOLAM KALCEKS)
Composition:
Active substance: midazolam;
1 ml of solution contains 5 mg of midazolam;
Excipients: hydrochloric acid, sodium chloride, sodium hydroxide, water for injections.
Pharmaceutical form. Injection solution.
Main physicochemical properties: clear, colorless solution.
Pharmacotherapeutic group.
Hypnotics and sedatives, benzodiazepine derivatives. ATC code N05CD08.
Pharmacological Properties.
Pharmacodynamics.
Midazolam is a derivative of the imidazobenzodiazepine group. The free base is a lipophilic substance with low water solubility.
The basic nitrogen at position 2 of the imidazobenzodiazepine ring allows midazolam to form water-soluble salts with acids, resulting in a stable and well-tolerated solution for injection or infusion.
The pharmacological action of midazolam is characterized by short duration due to rapid metabolic transformation within a short time period. Midazolam has potent sedative and hypnotic effects. In addition, it possesses anxiolytic, anticonvulsant, and muscle-relaxant properties. After intramuscular or intravenous administration, transient anterograde amnesia occurs (the patient does not recall events occurring during the peak effect of the active substance).
Pharmacokinetics.
Absorption after intramuscular injection
Midazolam is rapidly and completely absorbed from muscle tissue. Maximum plasma concentration (Cmax) is achieved within 30 minutes. Absolute bioavailability after intramuscular administration exceeds 90%.
Absorption after rectal administration
Midazolam is rapidly absorbed after rectal administration. Cmax is reached within approximately 30 minutes. Absolute bioavailability is approximately 50%.
Distribution
After intravenous administration of midazolam, one or two distinct distribution phases appear on the plasma concentration–time curve (AUC). The volume of distribution at steady state ranges from 0.7 to 1.2 L/kg. Midazolam is 96–98% bound to plasma proteins, primarily albumin. Midazolam slowly and in small amounts enters cerebrospinal fluid. It has been established that midazolam slowly penetrates the placental barrier and enters the fetal circulation. Midazolam has been detected in human breast milk in small quantities.
Biotransformation
Midazolam is almost entirely eliminated via biotransformation. It has been estimated that the fraction of the dose metabolized by the liver ranges from 30% to 60%. Midazolam is hydroxylated by the CYP3A4 isoenzyme of cytochrome P450. The main metabolite in plasma and urine is alpha-hydroxymidazolam. The plasma concentration of alpha-hydroxymidazolam is about 12% of the parent compound. Alpha-hydroxymidazolam is pharmacologically active but contributes minimally (approximately 10%) to the effects of intravenously administered midazolam.
Elimination
In healthy volunteers, the elimination half-life of midazolam ranges from 1.5 to 2.5 hours.
Plasma clearance ranges from 300 to 500 mL/min. Midazolam is primarily excreted by the kidneys (60–80% of the administered dose), mainly as alpha-hydroxymidazolam conjugated with glucuronide. Less than 1% of the dose is excreted unchanged in urine. The elimination half-life of alpha-hydroxymidazolam is less than 1 hour. The elimination kinetics of midazolam administered as a continuous intravenous infusion do not differ from those observed after bolus injection.
Special patient groups
Elderly patients
In adults aged 60 years and older, the elimination half-life may be prolonged up to fourfold.
Paediatric population
While the absorption rate of rectally administered midazolam is similar in children and adults, bioavailability in children is reduced (5–18%). Compared to adults, the elimination half-life after intravenous and rectal administration is shorter (1–1.5 hours) in children aged 3 to 10 years. This difference corresponds to increased metabolic clearance in children.
Neonates
In neonates, the elimination half-life averages 6–12 hours, likely due to hepatic immaturity and reduced clearance (see section "Special Warnings and Precautions for Use").
Patients with increased body weight
The mean elimination half-life in patients with increased body weight is higher than in those with normal body weight (5.9 vs. 2.3 hours). This is associated with an approximately 50% increase in volume of distribution adjusted for total body weight. Clearance does not significantly differ between patients with normal and increased body weight.
Patients with hepatic impairment
The elimination half-life may be prolonged and clearance reduced in patients with cirrhosis compared to healthy volunteers (see section "Special Warnings and Precautions for Use").
Patients with renal impairment
The elimination half-life in patients with chronic renal impairment is similar to that in healthy volunteers.
Critically ill patients
The elimination half-life of midazolam may be prolonged up to sixfold in critically ill patients.
Patients with cardiac insufficiency
The elimination half-life in patients with congestive heart failure is longer than in healthy volunteers (see section "Special Warnings and Precautions for Use").
Indications.
Midazolam is a short-acting hypnotic agent with the following indications:
- Adults:
- Sedation with preservation of consciousness prior to or during diagnostic or therapeutic procedures, with or without local anaesthesia;
- Anaesthesia (premedication before induction of anaesthesia, induction of anaesthesia, as a sedative component in the maintenance of anaesthesia);
- Sedation in intensive care units.
- Children:
- Sedation with preservation of consciousness prior to or during diagnostic or therapeutic procedures, with or without local anaesthesia;
- Anaesthesia (premedication before induction of anaesthesia);
- Sedation in intensive care units.
Contraindications.
Hypersensitivity to midazolam, benzodiazepines, or any excipient of the medicinal product.
Sedation with preservation of consciousness in patients with severe or acute respiratory insufficiency.
Interaction with other medicinal products and other forms of interaction.
Pharmacokinetic interactions
Midazolam is metabolized by CYP3A4. Inhibitors and inducers of CYP3A may potentially increase or decrease midazolam plasma concentrations, respectively, thereby affecting its clinical effects, necessitating appropriate dose adjustments.
Pharmacokinetic interactions with CYP3A inhibitors or inducers are more pronounced with oral administration compared to intravenous administration of midazolam, particularly because CYP3A4 is also present in the upper gastrointestinal tract. This is due to the fact that after oral administration, both systemic clearance and bioavailability are altered, whereas after parenteral administration, only systemic clearance is affected. After a single intravenous dose of midazolam, the change in maximum clinical effect due to CYP3A4 inhibition is minimal, although the duration of effect may be prolonged. However, after prolonged administration of midazolam, both the magnitude and duration of effect may be increased with CYP3A4 inhibition.
There are no available studies on the effect of CYP3A4 modulation on midazolam pharmacokinetics after rectal or intramuscular administration. These interactions are expected to be less pronounced after rectal than after oral administration, as the gastrointestinal tract is not involved, whereas after intramuscular administration, the effects of CYP3A4 modulation should not significantly differ from those observed with intravenous administration.
Therefore, careful monitoring of clinical effects and vital signs is recommended during midazolam administration, considering that the clinical effect of midazolam may be stronger and longer-lasting when co-administered with a CYP3A4 inhibitor, even if administered only once. In particular, administration of high doses or prolonged infusions of midazolam to patients receiving strong CYP3A4 inhibitors (e.g., during intensive therapy) may result in prolonged sedation, delayed emergence from anaesthesia, and respiratory depression, requiring dose adjustment.
With CYP3A4 induction, it should be noted that the induction process takes several days to reach maximum effect and several days to subside. Unlike treatment with an inducer over several days, short-term treatment leads to less pronounced interactions with midazolam. However, significant induction cannot be ruled out even after short-term treatment with strong inducers. Midazolam is known not to alter the pharmacokinetics of other medicinal products.
Medicinal products that inhibit CYP3A
Azole antifungal agents
- Ketoconazole increases the plasma concentration of intravenously administered midazolam by 5-fold, while the terminal elimination half-life is prolonged approximately 3-fold. If parenteral midazolam is administered concomitantly with a strong CYP3A inhibitor such as ketoconazole, it should be done in an intensive care unit or similar setting to ensure close clinical monitoring and appropriate management in case of respiratory depression and/or prolonged sedation. Stepwise dose titration or dose adjustment should be considered, especially when more than one intravenous dose of midazolam is administered. This recommendation may also apply to other azole antifungal agents (see below), as increased sedative effects of intravenously administered midazolam have been reported, albeit to a lesser extent.
- Voriconazole increases the plasma concentration of intravenously administered midazolam by 3-fold, while the elimination half-life is also prolonged approximately 3-fold.
- Fluconazole and itraconazole increase the plasma concentration of intravenously administered midazolam by 2–3-fold, associated with a prolongation of the terminal elimination half-life by 2.4-fold for itraconazole and 1.5-fold for fluconazole.
- Posaconazole increases the plasma concentration of intravenously administered midazolam by approximately 2-fold.
It should be noted that the effect after oral administration of midazolam would be significantly greater than with the above-mentioned agents, especially with ketoconazole, itraconazole, and voriconazole.
Midazolam in ampoules is not intended for oral administration.
Macrolide antibiotics
- Erythromycin increases the plasma concentration of intravenously administered midazolam by approximately 1.6–2-fold, associated with a prolongation of the terminal elimination half-life by 1.5–1.8-fold.
- Clarithromycin increases the plasma concentration of midazolam by up to 2.5-fold, and the terminal elimination half-life is prolonged by 1.5–2-fold.
Additional information regarding oral midazolam
- Roxithromycin: Although there are no data on the effect of roxithromycin on intravenously administered midazolam, a weak effect on the terminal elimination half-life of oral midazolam tablets (approximately 30% prolongation) suggests a possible minor effect of roxithromycin on intravenously administered midazolam.
HIV protease inhibitors
- Saquinavir and other HIV protease inhibitors: concomitant use with protease inhibitors may cause a significant increase in midazolam concentration. Co-administration of ritonavir-boosted lopinavir increases the plasma concentration of intravenously administered midazolam by 5.4-fold, associated with a similar prolongation of the terminal elimination half-life. If parenteral midazolam is administered together with HIV protease inhibitors, treatment parameters should follow those described in the above section for azole antifungals, ketoconazole.
Additional information regarding oral midazolam
Based on data from other CYP3A4 inhibitors, plasma concentrations of midazolam are expected to be significantly higher with oral midazolam. Therefore, protease inhibitors should not be administered concomitantly with oral midazolam.
Calcium channel blockers
- Diltiazem: administration of a single dose of diltiazem increases the plasma concentration of intravenously administered midazolam by approximately 25% and prolongs the terminal elimination half-life by 43%.
Additional information regarding oral midazolam
- Verapamil/diltiazem increases the plasma concentration of oral midazolam by 3 and 4 times, respectively. The terminal elimination half-life of midazolam is prolonged by 41% and 49%, respectively.
Other medicinal products/phytopreparations.
- Atorvastatin increases the plasma concentration of intravenously administered midazolam by 1.4-fold compared to the control group.
Additional information regarding oral midazolam
- Nefazodone increases the plasma concentration of oral midazolam by 4.6-fold and the terminal elimination half-life by 1.6-fold.
- Aprepitant increases midazolam plasma concentration in a dose-dependent manner (3.3-fold at a dose of 80 mg/day) and prolongs the terminal elimination half-life by 2-fold.
Medicinal products that induce CYP3A
- Rifampicin reduces the plasma concentration of intravenously administered midazolam by 60% after administration of 600 mg/day rifampicin for 7 days. The terminal elimination half-life is shortened by approximately 50–60%.
Additional information regarding oral midazolam
- Rifampicin reduces the plasma concentration of orally administered midazolam by 96% in healthy volunteers, and its psychomotor effects are almost completely lost.
- Carbamazepine/phenytoin: repeated dosing of carbamazepine or phenytoin reduces the plasma concentration of orally administered midazolam by up to 90%, and the terminal elimination half-life is shortened by 60%.
- Efavirenz: a 5-fold increase in the ratio of alpha-hydroxymidazolam (produced via CYP3A4) to midazolam confirms its inducing effect on CYP3A4.
Phytopreparations and food products
St. John’s wort reduces midazolam plasma concentration by approximately 20–40%, associated with a shortening of the terminal elimination half-life by approximately 15–17%. Depending on the specific St. John’s wort extract, the CYP3A4 induction effect may vary.
Pharmacodynamic interactions
Concomitant use of midazolam with other sedatives/hypnotics and central nervous system (CNS) depressants (including alcohol) may lead to enhanced sedation and respiratory depression. These include opioid derivatives (used as analgesics, antitussives, or for substitution therapy), antipsychotics, other benzodiazepines used as anxiolytics or hypnotics, phenobarbital, propofol, ketamine, etomidate, antidepressants with sedative effects, H1-antihistamines, and centrally acting antihypertensives.
Alcohol may significantly enhance the sedative effect of midazolam. Consumption of alcohol is contraindicated during midazolam treatment (see section "Special Warnings and Precautions for Use").
Midazolam reduces the minimum alveolar concentration (MAC) of inhalational anaesthetics.
Special precautions for use.
Midazolam should be administered only by experienced physicians in fully equipped settings for monitoring and supporting respiratory and cardiovascular functions, or by personnel specifically trained to recognize and manage adverse reactions, including resuscitation. In rare cases, serious cardiopulmonary adverse reactions have been reported, including respiratory depression, apnea, respiratory arrest, and/or cardiac arrest. Such life-threatening complications occur more frequently when the injection is administered very rapidly or when a high dose is given (see section "Adverse reactions").
Special caution is required when administering sedation with preserved consciousness to patients with impaired respiratory function.
Infants under 6 months of age are particularly susceptible to airway obstruction and hypoventilation; therefore, it is essential to titrate the dose in small increments to achieve the desired clinical effect and to carefully monitor respiratory rate and oxygen saturation. After midazolam administration as premedication, the patient must remain under close supervision, as individual sensitivity may vary and symptoms of overdose may occur.
Special caution is required when prescribing midazolam to patients at high risk:
- elderly patients aged 60 years and older;
- chronically ill or debilitated patients, for example:
- patients with chronic respiratory insufficiency;
- patients with chronic renal insufficiency, hepatic or cardiac dysfunction;
- pediatric patients, especially those with cardiovascular instability.
Lower doses should be used in patients at high risk (see section "Dosage and administration"), and continuous monitoring for early signs of changes in vital functions is required.
As with any centrally acting CNS depressant and/or muscle relaxant agent, particular caution is required when administering midazolam to patients with myasthenia gravis.
Tolerance
Some loss of effectiveness has been reported with prolonged use of midazolam for sedation in intensive care units.
Dependence
When midazolam is used for prolonged sedation in intensive care, the possibility of physical dependence should be considered. The risk of dependence increases with higher doses and longer duration of treatment; it is also higher in patients with a history of alcohol and/or drug abuse (see section "Adverse reactions").
Withdrawal syndrome
Physical dependence may develop following prolonged treatment with midazolam in intensive care units. Therefore, abrupt discontinuation of treatment may lead to withdrawal syndrome. Symptoms may include headache, muscle pain, anxiety, tension, restlessness, confusion, irritability, rebound insomnia, mood changes, hallucinations, and seizures. Since the risk of withdrawal symptoms after abrupt discontinuation is higher, gradual dose reduction is recommended.
Amnesia
Midazolam causes anterograde amnesia (an effect that is sometimes highly desirable, particularly before and during surgical and diagnostic procedures), the duration of which is directly related to the administered dose. Prolonged amnesia may pose problems in outpatient settings when patients are scheduled for discharge after a procedure. After parenteral administration of midazolam, patients may be discharged from hospital or transferred to an outpatient clinic only if accompanied by a responsible adult.
Paradoxical reactions
Paradoxical reactions have been observed with midazolam use, such as excitement, involuntary movements (including tonic/clonic seizures and muscle tremor), hyperactivity, hostility, rage attacks, aggression, paroxysmal agitation, and risk of violence. Such reactions may occur with high doses and/or rapid administration of the drug. These reactions are more common in children and elderly patients.
Altered elimination of midazolam
Changes in midazolam elimination may be caused by compounds that inhibit or induce the CYP3A4 isoenzyme; therefore, the midazolam dose may need to be adjusted accordingly (see section "Interaction with other medicinal products and other forms of interaction").
The elimination time of midazolam may also be prolonged in patients with hepatic dysfunction and low cardiac output, as well as in neonates (see section "Pharmacokinetics").
Preterm infants and neonates
Due to the increased risk of apnea, caution is required when administering sedation to preterm and ex-preterm infants. Close monitoring of respiratory rate and oxygen saturation is essential. Rapid intravenous injection should be avoided in neonates. Neonates have immature organs and/or reduced organ function, making them more sensitive to pronounced and/or prolonged respiratory effects of midazolam. Adverse hemodynamic reactions have been reported in infants with cardiovascular instability; therefore, rapid intravenous administration should be avoided in such patients.
Pediatric patients under 6 months of age
For these patients, midazolam is indicated for sedation only in intensive care units. Infants under 6 months of age are particularly susceptible to airway obstruction and hypoventilation. Therefore, dose titration in small increments to achieve clinical effect and careful monitoring of respiratory rate and oxygen saturation are required (see also the subsection "Preterm infants and neonates" above).
Concomitant use of alcohol/CNS depressants
Concomitant use of midazolam with alcohol and/or other CNS depressants should be avoided. Concurrent use may enhance the clinical effect of midazolam, leading to pronounced sedation or clinically significant respiratory depression (see section "Interaction with other medicinal products and other forms of interaction").
History of alcohol or drug abuse
Midazolam and other benzodiazepines should be avoided in patients with a history of alcohol or drug abuse.
Discharge criteria
After midazolam administration, patients may be discharged from hospital or transferred to an outpatient clinic only upon physician recommendation and in the presence of a responsible accompanying person. The patient should not be left unattended after discharge.
Use during pregnancy or breastfeeding.
Pregnancy.
There are insufficient data to assess the safety of midazolam during pregnancy.
Animal studies do not indicate a teratogenic effect, but fetotoxicity has been observed with other benzodiazepines. There are no data on the use of midazolam during the first two trimesters of pregnancy.
It has been reported that administration of high doses of midazolam during the third trimester, during labor, or as an induction agent for anesthesia in cesarean section may cause adverse effects in the mother or fetus (inhalation risk for the mother, fetal arrhythmia, hypotonia, impaired sucking reflex, hypothermia, and respiratory depression in newborns).
Furthermore, infants born to mothers who received benzodiazepines regularly during the late stages of pregnancy may develop physical dependence, with a potential risk of withdrawal symptoms in the postnatal period.
Therefore, midazolam should not be administered during pregnancy unless clearly necessary. Its use during cesarean section should preferably be avoided.
The risk to the newborn should be considered if midazolam is used for any surgical procedure close to term.
Breastfeeding.
Midazolam is excreted in small amounts in breast milk. Breastfeeding mothers are advised not to breastfeed for 24 hours after midazolam administration.
Ability to affect reaction speed when driving or operating machinery.
Sedation, amnesia, impaired attention, and impaired muscle function may negatively affect the ability to drive or operate machinery. Before administering midazolam, patients should be warned to refrain from driving or operating machinery until the drug's effects have completely subsided. The physician should determine when these activities may be safely resumed. It is recommended that a responsible person accompany the patient home after discharge.
Dosage and Administration
Administered intramuscularly, intravenously, or rectally.
Instructions for dilution of the medicinal product prior to administration are provided below under "Directions for Use".
Standard Dosage
Midazolam is a potent sedative agent requiring slow administration and individual dose titration. Dose titration is strongly recommended to achieve a safe level of sedation according to clinical needs, physical condition, age, and concomitant therapy. Midazolam should be administered with caution in patients aged 60 years and older, debilitated patients, patients with chronic illness, and pediatric patients; risk factors for each patient should be individually assessed. Standard dosages are provided in the table below. Additional information is provided in the text following the table.
| Indication |
Adults <60 years |
Adults ≥60 years / debilitated or chronically ill patients |
Children |
| Conscious sedation |
IV Initial dose: 2–2.5 mg Titration step: 1 mg Total dose: 3.5–7.5 mg |
IV Initial dose: 0.5–1 mg Titration step: 0.5–1 mg Total dose: <3.5 mg |
IV in children aged 6 months to 5 years Initial dose: 0.05–0.1 mg/kg Total dose: <6 mg IV in children aged 6 to 12 years Initial dose: 0.025–0.05 mg/kg Total dose: <10 mg Rectal in children >6 months 0.3–0.5 mg/kg IM in children aged 1 to 15 years 0.05–0.15 mg/kg |
| Premedication before anesthesia induction |
IV 1–2 mg repeated IM 0.07–0.1 mg/kg |
IV Initial dose: 0.5 mg Slow dose escalation by titration if needed IM 0.025–0.05 mg/kg |
Rectal in children >6 months 0.3–0.5 mg/kg IM in children aged 1 to 15 years 0.08–0.2 mg/kg |
| Anesthesia induction |
IV 0.15–0.2 mg/kg (0.3–0.35 mg/kg without premedication) |
IV 0.05–0.15 mg/kg (0.15–0.3 mg/kg without premedication) |
|
| Sedative component in anesthesia maintenance |
IV Intermittent doses 0.03–0.1 mg/kg or continuous infusion 0.03–0.1 mg/kg/hour |
IV Lower doses than recommended for adults <60 years |
|
| Sedation in intensive care unit (ICU) |
IV Loading dose: 0.03–0.3 mg/kg with increments of 1–2.5 mg Maintenance dose: 0.03–0.2 mg/kg/hour |
IV in neonates <32 weeks gestational age 0.03 mg/kg/hour IV in neonates >32 weeks gestational age and infants up to 6 months 0.06 mg/kg/hour IV in children >6 months Loading dose: 0.05–0.2 mg/kg Maintenance dose: 0.06–0.12 mg/kg/hour |
|
Dosing for sedation with preservation of consciousness
For sedation required during diagnostic and surgical procedures, midazolam is administered intravenously. The appropriate dose should be individually titrated. The drug must not be administered rapidly or as a bolus injection, but only by gradual dose titration. The onset of sedative effect may vary individually depending on the patient's physical condition and the dosing regimen used (e.g., rate of administration, dose size). Additional doses may be administered as needed according to individual requirements. The effect begins approximately 2 minutes after injection. Maximum effect is achieved within approximately 5–10 minutes.
Adults
Midazolam should be administered intravenously slowly at a rate of approximately 1 mg/30 seconds. For adults under 60 years of age, an initial dose of 2 to 2.5 mg is administered 5–10 minutes before the start of the procedure. This initial dose may be followed by additional doses of 1 mg as needed. The average total dose ranges from 3.5 to 7.5 mg. Administration of a total dose exceeding 5 mg is generally unnecessary.
The initial dose for patients aged 60 years and older, debilitated patients, or patients with chronic diseases is 0.5–1 mg, administered 5–10 minutes before the start of the procedure. Subsequent additional doses of 0.5–1 mg of midazolam may be administered as needed. For these patients, a longer time may be required to achieve maximum effect; therefore, additional doses of midazolam should be titrated very slowly and cautiously. Administration of a total dose exceeding 3.5 mg is generally unnecessary.
Pediatric population
Intravenous administration: midazolam doses are slowly titrated to achieve the desired clinical effect. The initial dose should be administered over 2–3 minutes. An additional 2–5 minutes should elapse before starting the procedure or repeating the dose to fully assess the sedative effect. If deeper sedation is required, additional small doses should be administered until the desired level of sedation is achieved. Infants and children under 5 years of age may require significantly higher doses (mg/kg) compared to older children and adolescents.
- Children under 6 months of age: these children are particularly susceptible to airway obstruction and hypoventilation; therefore, conscious sedation is not recommended for this age group.
- Children aged 6 months to 5 years: the initial dose is 0.05 to 0.1 mg/kg. Doses up to 0.6 mg/kg may be required to achieve the desired effect, but the total dose must not exceed 6 mg. Higher doses may cause prolonged sedative effects and risk of hypoventilation.
- Children aged 6 to 12 years: the initial dose is 0.025 to 0.05 mg/kg. A total dose of up to 0.4 mg/kg (maximum dose – 10 mg) may be required. Higher doses may cause prolonged sedative effects and risk of hypoventiation.
- Children aged 12 to 16 years: use the recommended adult doses.
Rectal administration: the total dose of midazolam is generally 0.3 to 0.5 mg/kg. The solution contained in the ampoule is administered rectally using a plastic applicator attached to a syringe. If the volume to be administered is too small, water may be added to achieve a total volume of 10 ml. The entire dose should be administered immediately. Avoid repeated rectal administration. Rectal administration is not recommended for children under 6 months of age due to limited data in this age group.
Intramuscular administration: doses range from 0.05 to 0.15 mg/kg. A total dose exceeding 10.0 mg is generally not required. Intramuscular administration is possible only in exceptional cases. Rectal administration should be preferred, as intramuscular injection is painful.
For children weighing less than 15 kg, midazolam solutions with a concentration higher than 1 mg/ml are not recommended. Higher concentrations should be diluted to 1 mg/ml.
Dosing for premedication
Administration of midazolam immediately before a procedure produces a sedative effect (hypnotic or anesthetic effect and reduced level of consciousness) and preoperative amnesia. Midazolam may also be administered in combination with anticholinergic agents. In such cases, midazolam is administered intravenously or intramuscularly (deep into the muscle mass, 20–60 minutes before anesthesia induction), while in children rectal administration is preferred (see below). After premedication, the patient must be under continuous close monitoring, as individual sensitivity to the drug varies and symptoms of overdose may occur.
Adults
The recommended dose for preoperative sedation and amnesia in patients classified as ASA physical status I and II, as well as in patients under 60 years of age, is 1 to 2 mg intravenously (the dose may be repeated if necessary) or 0.07 to 0.1 mg/kg intramuscularly. For patients aged 60 years and older, debilitated patients, or chronically ill patients, the dose should be reduced and adjusted according to the individual case. The recommended initial intravenous dose is 0.5 mg, which may be increased gradually by titration if necessary. The recommended initial dose for intramuscular administration is 0.025 to 0.05 mg/kg. When opioids are co-administered, the dose of midazolam should be reduced. The usual dose ranges from 2 to 3 mg.
Pediatric population
Neonates and children under 6 months of age
This medicinal product is not recommended for children under 6 months of age due to limited data in this age group.
Children aged 6 months and older
Rectal administration: the total dose of midazolam (usually in the range of 0.3 to 0.5 mg/kg) should be administered 15–30 minutes before anesthesia induction. The solution contained in the ampoule is administered rectally using a plastic applicator attached to a syringe. If the volume to be administered is too small, water may be added to achieve a total volume of 10 ml.
Intramuscular administration: intramuscular administration is painful; therefore, this route should be used only in exceptional cases. Rectal administration should be preferred. The range of effective and safe doses for intramuscular administration is 0.08 to 0.2 mg/kg. Children aged 1 to 15 years require proportionally higher doses per kg of body weight compared to adults.
For children weighing less than 15 kg, midazolam solutions with a concentration higher than 1 mg/ml are not recommended. Higher concentration solutions should be diluted to 1 mg/ml.
Anesthesia induction
Adults
When midazolam is used prior to or in combination with other anesthetic agents for anesthesia induction, individual patient responses may vary. The dose should be increased by titration until the desired effect is achieved. The dose should be titrated according to the patient's age and clinical status. When midazolam is used before or in combination with other intravenous or inhalational agents used for anesthesia induction, the initial doses of all these agents should be significantly reduced, sometimes to 25% of the usual initial dose.
The desired level of anesthesia is achieved by gradual dose escalation. For intravenous anesthesia induction, midazolam is administered slowly in divided doses. Each dose portion (not exceeding 5 mg) should be administered over 20–30 seconds with 2-minute intervals between doses.
- For adults under 60 years of age who have received premedication, a dose of 0.15 to 0.2 mg/kg intravenously is usually administered.
- For adults under 60 years of age without premedication, higher doses may be used (0.3–0.35 mg/kg intravenously). If necessary, additional doses of approximately 25% of the patient's initial dose may be administered to complete induction. Induction may also be achieved using inhalational anesthetics. In refractory cases, a total dose of up to 0.6 mg/kg may be used for induction, but such higher doses may cause prolonged recovery after anesthesia.
- For adults aged 60 years and older who have received premedication, debilitated patients, or patients with chronic diseases, the dosage should be significantly reduced, e.g., to 0.05–0.15 mg/kg intravenously, administered over 20–30 seconds, with an onset of action of 2 minutes.
- For adults aged 60 years and older without premedication, higher doses of midazolam are usually required for induction. The recommended initial dose is 0.15 to 0.3 mg/kg. For debilitated patients or patients with serious systemic disease without premedication, a smaller amount of midazolam should usually be administered for induction. An initial dose of 0.15 to 0.25 mg/kg is generally sufficient.
As a sedative component in combined anesthesia
Adults
Midazolam may be administered as a sedative component in combined anesthesia either by repeated small intravenous doses (in the range of 0.03 to 0.1 mg/kg) or by continuous intravenous infusion of midazolam (in the range of 0.03 to 0.1 mg/kg/hour), usually in combination with analgesics. The dose and dosing intervals vary depending on the individual patient response.
For adults aged 60 years and older, debilitated patients, or chronically ill patients, lower doses are required for maintenance.
Sedation in intensive care unit
The desired level of sedation is achieved by stepwise titration of midazolam dose, followed by continuous infusion or intermittent bolus administration. Midazolam is administered according to clinical needs, patient condition, age, and concomitant medications (see section "Interaction with other medicinal products and other forms of interaction").
Adults
Intravenous loading dose: 0.03 to 0.3 mg/kg, administered slowly with increments. Each dose of 1 to 2.5 mg should be administered over 20–30 seconds with 2-minute intervals between doses. For patients with hypovolemia, vasoconstriction, or hypothermia, the loading dose should be reduced or omitted. If midazolam is administered simultaneously with potent analgesics, the analgesics should be administered first. This ensures safe titration of the sedative effect of midazolam, thus avoiding the influence of analgesic sedation.
Intravenous maintenance dose: 0.03 to 0.2 mg/kg/hour. For patients with hypovolemia, vasoconstriction, or hypothermia, the maintenance dose should be reduced. The level of sedation should be assessed regularly. Prolonged sedation may lead to the development of tolerance, which may require dose escalation.
Pediatric population
Neonates and children under 6 months of age
Midazolam is administered as a continuous intravenous infusion. The initial infusion rate for neonates with gestational age less than 32 weeks is 0.03 mg/kg/hour (0.5 µg/kg/min), and for neonates with gestational age over 32 weeks and children under 6 months of age – 0.06 mg/kg/hour (1 µg/kg/min).
Intravenous loading doses are not recommended for preterm neonates, full-term neonates, and children under 6 months of age; a higher infusion rate during the first hours of administration is preferable to achieve therapeutic concentrations. The infusion rate should be frequently and carefully reviewed to select the lowest effective dose and prevent drug accumulation (especially during the first 24 hours). Careful monitoring of respiratory rate and oxygen saturation is required.
Children aged 6 months and older
For children on mechanical ventilation and intubated patients, a loading dose of 0.05 to 0.2 mg/kg should be administered slowly intravenously over at least 2–3 minutes to achieve the desired clinical effect.
Midazolam should not be administered as a rapid intravenous injection. After administration of the loading dose, midazolam should be administered as a continuous infusion at a rate of 0.06 to 0.12 mg/kg/hour (1 to 2 µg/kg/min). If necessary, the infusion rate may be increased or decreased (usually by 25% of the initial or subsequent infusion rate), or additional doses of midazolam may be administered intravenously to maintain or enhance the desired effect.
If midazolam infusion is initiated in hemodynamically unstable patients, the usual loading dose should be titrated in small increments, and the patient should be monitored for hemodynamic changes (e.g., hypotension). These patients are more sensitive to the respiratory depressant effects of midazolam; therefore, careful monitoring of respiratory rate and oxygen saturation is required.
For preterm neonates, neonates, and children with body weight below 15 kg, midazolam solutions with a concentration higher than 1 mg/ml are not recommended. Higher concentration solutions should be diluted to 1 mg/ml.
Patients with renal impairment
In patients with renal impairment (creatinine clearance <10 ml/min), the pharmacokinetics of unbound midazolam after single intravenous administration are similar to those in healthy volunteers. However, after prolonged infusion in intensive care unit (ICU) patients, the mean duration of sedative effect was significantly prolonged in the population with renal insufficiency, primarily due to accumulation of alpha-hydroxymidazolam glucuronide. There are no specific data for patients with severe renal impairment (creatinine clearance below 30 ml/min) receiving midazolam for anesthesia induction.
Patients with hepatic impairment
In patients with hepatic impairment, clearance of intravenously administered midazolam is reduced, resulting in prolonged terminal half-life. This may lead to a more pronounced and prolonged clinical effect. Lower doses of midazolam may be required, and careful monitoring of vital signs should be ensured (see section "Special precautions for use").
Instructions for use
Compatible with the following infusion solutions: 0.9% sodium chloride solution, 5% glucose solution, 10% glucose solution, Ringer's solution, Hartmann's solution.
For intravenous infusion, the contents of Midazolam Kalceks ampoules may be diluted with one of the above-mentioned solutions in a ratio of 15 mg midazolam per 100–1000 ml of infusion solution.
For single use only; any unused portion of the solution should be discarded.
The solution should be inspected visually before administration. Only clear solutions without visible particles should be used.
How to open the ampoule:
- Turn the ampoule so that the colored dot faces you. Gently tap the top of the ampoule with your finger to ensure the solution is in the lower part of the ampoule (Fig. 1).
- Open the ampoule with both hands: hold the lower part of the ampoule with one hand and press the top part of the ampoule with the other hand in the direction away from the colored dot (Fig. 2).
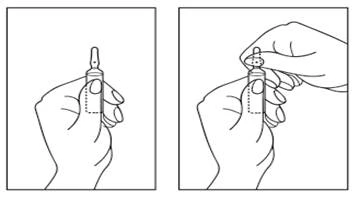
Fig. 1. Fig. 2.
Children.
The use of the drug in children is described in detail in the section "Method of administration and dosage." The drug is not recommended for sedation in children under 6 months of age, as this age group of patients is highly sensitive to hypoventilation and airway obstruction.
Overdose.
Symptoms.
Like other benzodiazepines, midazolam usually causes drowsiness, ataxia, dysarthria, and nystagmus. Overdose with midazolam alone is rarely life-threatening but may lead to areflexia, apnea, hypotension, cardiorespiratory depression, and, in rare cases, coma. Coma usually lasts several hours but may be prolonged and cyclic, especially in elderly patients. The respiratory depressant effect of benzodiazepines is more pronounced in patients with respiratory diseases. Benzodiazepines enhance the effects of other CNS depressants, including alcohol.
Treatment.
Vital signs of the patient should be monitored, and supportive therapy should be initiated according to the patient's clinical status. In particular, symptomatic treatment may be required to support cardiorespiratory function and CNS activity.
In case of oral ingestion, further absorption should be prevented by appropriate methods, such as administration of activated charcoal within 1–2 hours after overdose. If activated charcoal is used, airway protection is mandatory for patients exhibiting drowsiness. Gastric lavage may be considered in cases of mixed overdose but is not a routine measure.
In cases of severe CNS depression, flumazenil, a benzodiazepine antagonist, should be considered. This should be performed only under strict monitoring conditions. Flumazenil has a short half-life (approximately one hour); therefore, patients who have received flumazenil should be monitored after its effects wear off. Flumazenil should be used with particular caution in patients receiving concomitant medications that lower the seizure threshold (e.g., tricyclic antidepressants). For more detailed information on the proper use of flumazenil, refer to the summary of product characteristics.
Adverse Reactions
Very common (≥1/10), common (≥1/100, <1/10), uncommon (≥1/1,000, <1/100), rare (≥1/10,000, <1/1,000), very rare (<1/10,000), frequency not known (cannot be estimated from available data).
Immune system disorders: frequency not known – hypersensitivity, angioedema, anaphylactic shock.
Psychiatric disorders: frequency not known – confusion, euphoric mood, hallucinations, agitation*, hostility*, rage*, aggression*, excitement*, drug dependence and withdrawal syndrome, abuse.
Nervous system disorders: frequency not known – involuntary movements (including tonic/clonic movements and muscle tremor)*, hyperactivity*, sedation (prolonged and postoperative), reduced alertness, drowsiness, headache, dizziness, ataxia, anterograde amnesia**, duration of which is directly related to the administered dose, seizures due to withdrawal syndrome. Seizures have been reported in preterm infants and newborns.
Cardiac disorders: frequency not known – cardiac arrest, bradycardia, Cushing’s syndrome****.
Vascular disorders: frequency not known – arterial hypotension, vasodilation, thrombophlebitis, thrombosis.
Respiratory system disorders: frequency not known – respiratory depression, apnea, respiratory arrest, dyspnea, laryngospasm, hiccup.
Gastrointestinal disorders: frequency not known – nausea, vomiting, constipation, dry mouth.
Skin and subcutaneous tissue disorders: frequency not known – skin rashes, urticaria, pruritus.
General disorders and administration site conditions: frequency not known – fatigue, injection site erythema, injection site pain.
Injury, poisoning and procedural complications: frequency not known – falls, fractures***.
Social circumstances: frequency not known – threat of violence*.
*Paradoxical reactions of this type have been reported in children and elderly patients (see section "Special precautions").
**Anterograde amnesia may persist until the end of the procedure; prolonged amnesia has been observed in several isolated cases (see section "Special precautions").
***The risk of falls and fractures is higher in patients receiving concomitant sedative medications (including alcoholic beverages) and in elderly patients.
**** Especially after parenteral administration.
Dependence. Midazolam may lead to physical dependence even when used at therapeutic doses. Discontinuation of treatment (particularly abrupt) after prolonged intravenous administration may cause withdrawal symptoms, including withdrawal seizures (see section "Special precautions"). Cases of drug abuse have been reported. Severe cardiopulmonary adverse reactions have occurred. Life-threatening complications have been observed more frequently in adults aged 60 years and older and in patients with pre-existing respiratory insufficiency or cardiac dysfunction, particularly with rapid or high-dose administration (see section "Special precautions").
Shelf life. 4 years.
Do not use after the expiry date stated on the packaging.
Shelf life after dilution.
Chemical and physical stability in use has been demonstrated for 24 hours at 25 °C and for 3 days at 2–8 °C when diluted with the following infusion solutions: 0.9% sodium chloride solution, 5% and 10% glucose solution, Ringer’s solution, and Hartmann’s solution.
From a microbiological standpoint, the solution should be used immediately. If not used immediately, storage duration and conditions prior to use are the responsibility of the user and should generally not exceed 24 hours at 2–8 °C, unless dilution was performed under well-controlled and validated aseptic conditions.
Storage conditions.
No special storage requirements.
Store in the original packaging to protect from light. Do not freeze.
Keep out of reach of children.
Incompatibilities.
Midazolam Kalceks, solution for injection/infusion, can be diluted in 6% glucose solution Macrodex. Midazolam Kalceks must not be mixed with alkaline injection solutions. Midazolam precipitates in solutions containing sodium bicarbonate.
This medicinal product must not be mixed with other medicinal products except those specified above (see "Instructions for use").
Packaging.
1 ml or 3 ml of solution in a colorless glass ampoule of hydrolytic class I with scoring rings and a break point.
5 ampoules in a blister pack (cavity tray) made of polyvinyl chloride film.
1 or 2 blister packs (cavity trays) in a cardboard box with a first-opening control in the form of a self-adhesive sticker on each opening part of the box.
Prescription status.
Prescription only.
Manufacturer.
Manufacturer responsible for batch release:
JSC "Kalceks", Latvia.
Manufacturer's address and place of business.
71E Krustpils Street, Riga, LV-1057, Latvia.
Marketing Authorisation Holder.
JSC "Kalceks", Latvia.
Address of the Marketing Authorisation Holder.
71E Krustpils Street, Riga, LV-1057, Latvia.