Leiprorelin-vista
Ukraine
Table of Contents
INSTRUCTIONS FOR MEDICAL USE OF THE MEDICINAL PRODUCT LEUPRORELIN-VISTA LEUPRORELIN-VISTA
Composition:
Active substance: leuprolide acetate;
1 implant contains leuprolide acetate 11.25 mg, equivalent to 10.72 mg of leuprolide;
Excipients: poly-D,L-lactide, poly(lactide-co-glycolide).
Pharmaceutical form. Implant.
Main physicochemical properties: the implant is visible in the implant holder. Dimensions: length approximately 17.8 mm, width approximately 1.5 mm.
Functionality: after activation of the applicator syringe, an intact cylindrical rod of white to almost white color emerges from the needle.
Pharmacotherapeutic group. Gonadotropin-releasing hormone analogues.
ATC code L02A E02.
Pharmacological properties.
Pharmacodynamics.
The active substance of the medicinal product, leuprorelin acetate, is a synthetic analogue of the natural hypothalamic gonadotropin-releasing hormone (GnRH), which regulates the secretion of gonadotropic hormones—luteinizing hormone (LH) and follicle-stimulating hormone (FSH)—by the anterior pituitary gland. These hormones stimulate steroid synthesis in the gonads.
Unlike endogenous GnRH, which is secreted by the hypothalamus in a pulsatile manner, leuprorelin acetate (also known as a GnRH agonist) provides continuous blockade of GnRH receptors in the pituitary gland throughout the treatment period, resulting in desensitization of the pituitary to initial transient stimulation (downregulation). As a consequence of this negative feedback inhibition of gonadotropin secretion by the pituitary, testosterone levels decrease, thereby reducing the stimulation of prostate cancer tissue growth. Under normal conditions, this tissue is stimulated by dihydrotestosterone, which is produced in response to decreased testosterone levels in prostate cells.
Continuous administration of leuprorelin acetate leads to a reduction in both the number and sensitivity (so-called downregulation) of pituitary receptors, resulting in decreased levels of LH, FSH, and DHT. This, in turn, reduces testosterone levels to the castrate range. Animal studies have demonstrated an antiandrogenic effect and inhibition of prostate carcinoma growth.
According to experimental and clinical studies, a three-month course of leuprorelin acetate treatment following initial stimulation results in reduced gonadotropin secretion. In men, subcutaneous administration of leuprorelin acetate initially causes an increase in LH and FSH levels, accompanied by a transient rise in testosterone and dihydrotestosterone levels. This may lead to a temporary worsening of the clinical condition within the first 3 weeks of treatment, observed in isolated cases; therefore, in men with prostate cancer, concomitant antiandrogen therapy may be considered at the beginning of treatment. Prolonged administration of leuprorelin acetate, on the contrary, leads to a reduction in LH and FSH levels. Androgen levels in men decrease to values comparable to those observed after surgical removal of both testes. These changes typically occur within 2–3 weeks after initiation of therapy and are maintained throughout the subsequent treatment period. When considering leuprorelin acetate as a treatment option, it is necessary to evaluate the hormonal sensitivity of prostate cancer tissue and the potential therapeutic benefits of orchidectomy. If required, orchidectomy may be replaced by 3-monthly administration of leuprorelin acetate. According to available data, continuous administration of leuprorelin acetate can maintain castrate testosterone levels for over 5 years.
Clinical efficacy.
Clinical studies in patients with metastatic, castration-resistant prostate cancer have demonstrated benefits from adding agents such as androgen synthesis inhibitors (e.g., abiraterone acetate), antiandrogens (e.g., enzalutamide), taxanes (e.g., docetaxel or cabazitaxel), or radiopharmaceuticals (e.g., radium-223) to hypothalamic gonadotropin-releasing hormone therapy, such as leuprorelin acetate.
Pharmacokinetics.
After implant injection, leuprorelin acetate (the active substance) is continuously released from the lactic acid polymer matrix over a period of up to 3 months. Over time, the polymer is absorbed similarly to surgical suture material.
Distribution and elimination.
The volume of distribution of leuprorelin in men is 36 L, and total clearance is 139.6 mL/min. Repeated administration leads to sustained reduction of testosterone levels to castrate levels (sterility), except for the transient increase in testosterone levels that may occur after the first injection.
Patients with renal/hepatic impairment.
In patients with impaired renal or hepatic function, leuprorelin parameters were found to be at similar levels as in patients with normal kidney and liver function. In some patients with chronic renal failure, serum levels of leuprorelin were higher. However, this observation is unlikely to have clinical significance.
Bioavailability.
Relative bioavailability on day 84 is 84.6%, calculated by comparison with the AUC of 1 mg intravenous leuprorelin acetate injection.
Clinical characteristics.
Indications.
Determination of hormonal sensitivity of prostate cancer to assess the need for hormone suppression/hormonal ablative interventions.
Treatment of hormone-dependent advanced prostate cancer and treatment of high-risk localized prostate cancer and locally-advanced prostate cancer in combination with radiation therapy.
Contraindications.
- Hypersensitivity to leuprorelin acetate, other gonadotropin-releasing hormone (GnRH) agonists, or to any of the excipients of the medicinal product.
- Patients who have previously undergone orchidectomy (like other GnRH agonists, does not cause further reduction in serum testosterone levels after surgical castration).
- Hormone-independent tumors.
- Contraindicated in women and children.
Special precautions.
Use only if the pre-filled syringe-applier package is undamaged. Use immediately after opening the package.
Interaction with other medicinal products and other types of interactions.
Interaction with other medicinal products is unknown.
Since antiandrogen therapy may prolong the QT interval, concomitant use of Leuprorelin-Vista with medicinal products that prolong the QT interval or may cause torsade de pointes, such as class IA antiarrhythmics (e.g., quinidine, disopyramide) or class III antiarrhythmics (e.g., amiodarone, sotalol, dofetilide, ibutilide), methadone, moxifloxacin, neuroleptics and others, should be carefully evaluated (see section "Special instructions for use").
Special precautions for use.
Patients with arterial hypertension require careful monitoring. Idiopathic intracranial hypertension.
Idiopathic intracranial hypertension (pseudotumor cerebri) has been reported in patients receiving leuprorelin. Patients should be advised about the signs and symptoms of idiopathic intracranial hypertension, including severe, intermittent headache, visual disturbances, and tinnitus. If idiopathic intracranial hypertension occurs, discontinuation of leuprorelin should be considered.
There is an increased risk of depression (which may be severe), and symptoms of emotional lability such as crying, irritability, impatience, anger, and aggression in patients receiving gonadotropin-releasing hormone (GnRH) antagonists. Patients should be informed about this risk and provided with appropriate medical support if such symptoms occur.
During the post-marketing period, seizures have been reported in patients receiving leuprorelin acetate; these events were reported in adults with or without a history of epilepsy, seizure disorders, or risk factors for seizures. At the beginning of treatment, a transient increase in serum testosterone levels frequently occurs, which may be accompanied by a temporary worsening of certain clinical symptoms (onset or exacerbation of bone pain, urinary obstruction with associated complications, spinal cord compression, leg weakness, lymphedema). With continued therapy, these complications usually resolve spontaneously. Allergic and anaphylactic reactions, including both local reactions at the injection site and systemic reactions, may occur. At the initial stage of treatment, to reduce the severity of possible complications (initial testosterone surge and clinical symptom exacerbation), the concomitant use of appropriate antiandrogens may be considered.
Therapeutic efficacy should be regularly monitored by clinical examinations (digital rectal examination of the prostate, ultrasound, bone scintigraphy, computed tomography) and by measuring serum levels of phosphatase and/or prostate-specific antigen (PSA) and testosterone.
Hypogonadism resulting from long-term treatment with GnRH analogs and/or orchiectomy may lead to osteoporosis with an increased risk of fractures. Osteoporosis development is more pronounced after orchiectomy (with elevated cortisol levels) than after administration of GnRH analogs.
In patients at high risk, additional bisphosphonate therapy may prevent bone demineralization.
Patients with metastases to the brain or spinal cord, neurological disorders, or urinary tract obstruction require very careful monitoring, especially during the first few weeks of treatment. In isolated cases, spinal cord compression and renal insufficiency have been observed in such patients.
Use of the medicinal product Leuprorelin-Vista may result in positive doping test outcomes.
Metabolic changes:
Epidemiological data indicate that metabolic changes (e.g., hepatic steatosis) may occur during androgen deprivation therapy. Impaired glucose tolerance has been observed in some patients receiving GnRH analogs. Diabetic patients require monitoring during treatment with this medicinal product.
Antiandrogen therapy may prolong the QT interval.
In patients with a history of QT interval prolongation (or relevant risk factors), and in patients receiving concomitant medicinal products that may prolong the QT interval (see section "Interaction with other medicinal products and other forms of interaction"), physicians should assess the benefit-risk ratio, including the risk of torsade de pointes, before initiating treatment.
Use during pregnancy or breastfeeding.
The medicinal product Leuprorelin-Vista is not intended for use in women and is contraindicated during pregnancy and breastfeeding.
Ability to influence reaction speed when driving or operating machinery.
Due to the occurrence of fatigue, sometimes severe, in some patients—particularly at the initial stage of treatment, which may be related to the underlying tumor disease—the medicinal product, even when used correctly, may impair reaction speed and negatively affect the ability to drive a vehicle or operate complex machinery. Alcohol may enhance this adverse effect. The potential occurrence of adverse reactions affecting the nervous system and visual organs should also be considered.
Method of Administration and Dosage.
The recommended dose is 1 implant every 3 months. If no temporary improvement or positive dynamics are observed, continuation of treatment is not recommended.
In exceptional cases, administration of the medicinal product may be delayed for up to 4 weeks; the therapeutic effect is not reduced in most patients.
The medicinal product must be administered by a physician experienced in anticancer therapy. The implant is injected subcutaneously in the abdominal area, avoiding accidental intra-arterial administration.
Instructions for Use:
Read these instructions carefully, as the syringe supplied with this medicinal product may differ from those previously used by the patient.
- Disinfect the injection site on the anterior abdominal wall below the umbilical line.
- Remove the applicator from the sterile pouch. Check that the implant is in the correct position within the applicator. Remove the safety clip.
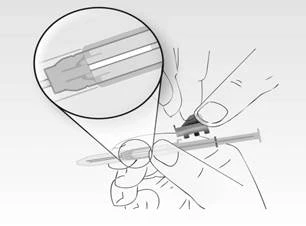
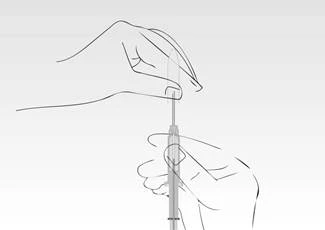
- Hold the applicator by the syringe cylinder and remove the protective cap.
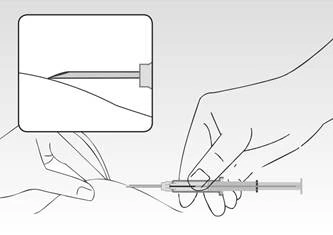
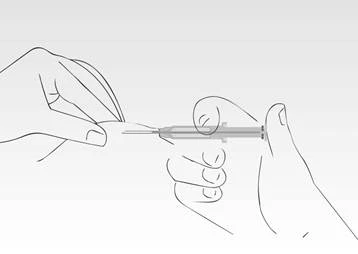
- Press the patient’s skin, holding the syringe cylinder, and insert the needle at an angle (almost parallel to the skin), with the needle opening facing upward.
Insert the needle into the subcutaneous tissue (not into muscle or the abdominal cavity) of the anterior abdominal wall below the umbilical line until the syringe cylinder touches the patient’s skin.
The syringe cylinder must remain in contact with the skin throughout the entire administration process!
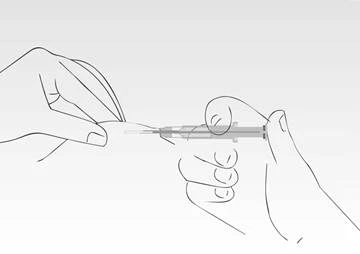
- Press the syringe plunger. The implant is transported to the needle tip. Do not pull the syringe back. During administration, the syringe cylinder must remain in contact with the patient’s skin.
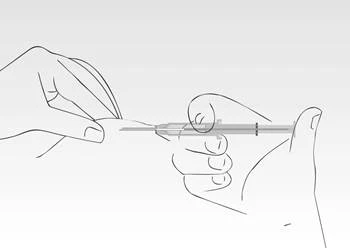
- When the plunger stops, the needle retraction is automatically unlocked.
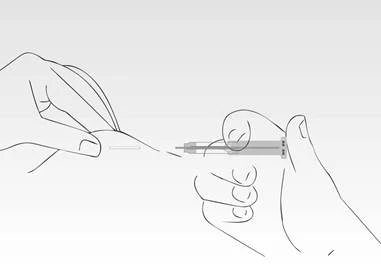
- The needle retracts from the tissue into the syringe cylinder. The syringe cylinder must remain in contact with the patient’s skin. Typically, forward movement of the plunger and needle retraction occur in one smooth motion.
- The implant administration is complete. The needle has been fully retracted into the syringe cylinder. The mandrin protects against injury from the needle tip.
Typically, within 3 months it can be determined whether prostate carcinoma is androgen-sensitive. The main diagnostic parameter is the analysis of prostate-specific antigen (PSA) concentration, which usually exceeds 10 ng/mL in active tumor progression. However, PSA levels, as well as testosterone levels in general, should be measured before and after administration of the medicinal product over a 3-month period. Test results are considered positive if, within 3 months, testosterone concentration reaches castrate levels (< 0.5 ng/mL) and PSA values decrease. An early reduction in PSA (approximately 80% from baseline) may be considered a positive indicator of long-term response to androgen deprivation. In such cases, hormonal suppression therapy is indicated.
Test results are considered negative if PSA levels remain unchanged or increase alongside a decrease in testosterone. In such cases, continuation of hormonal suppression therapy is not appropriate.
However, if a clinical response is observed in the patient (e.g., reduction in pain, decreased urinary discomfort, and return of the prostate to normal size), inconclusive negative results should be taken into account. In such rare cases, leuprorelin administration should be continued for the next 3 months, and PSA levels should be monitored. Additionally, the patient’s clinical symptoms should be carefully followed.
Treatment of prostate cancer with gonadotropin-releasing hormone (GnRH) analogs may be continued even after the development of castration resistance, provided appropriate guidelines are followed.
Treatment of advanced hormone-dependent prostate cancer is typically long-term.
Clinical data have shown that 3 years of androgen deprivation therapy (ADT), administered concurrently with and after radiation therapy, is superior to a 6-month course of ADT in locally advanced, hormone-dependent prostate cancer. A 2–3-year course of androgen deprivation therapy is recommended for patients (T3–T4) receiving radiation therapy.
Typically, treatment of advanced hormone-dependent prostate carcinomas with this medicinal product requires long-term therapy.
The therapeutic effect of treatment should be regularly monitored through clinical examinations (digital rectal examination of the prostate, ultrasound imaging, bone scans, computed tomography) and assessment of phosphatase or PSA and serum testosterone levels (especially if signs of tumor progression occur despite adequate therapy).
Children.
Not to be used for the treatment of children.
Overdose.
Symptoms. No symptoms of intoxication have been reported to date.
Treatment. In case of overdose, symptomatic treatment should be administered; supportive therapy should be provided as needed.
Adverse reactions.
At the beginning of treatment, a transient increase in serum testosterone concentration is usually observed, primarily due to the specific pharmacological action of leuprorelin. This may temporarily worsen certain disease symptoms (development or exacerbation of bone pain, urinary tract obstruction and its consequences, spinal cord compression, leg muscle weakness, lymphatic edema). This symptom exacerbation usually regresses spontaneously, without the need to discontinue leuprorelin. Due to suppression of certain sex hormones, undesirable adverse reactions may develop.
The adverse reactions of leuprorelin listed below are based on clinical trial experience and post-marketing data. Adverse reactions are grouped by MedDRA system organ classes. According to frequency classification, adverse reactions are categorized as follows: very common (≥ 1/10), common (≥ 1/100 to < 1/10), uncommon (≥ 1/1000 to < 1/100), rare (≥ 1/10,000 to < 1/1000), very rare (< 1/10,000), frequency not known (available data do not allow estimation of frequency).
Immune system disorders
Uncommon: systemic allergic reactions (fever, pruritus, eosinophilia, skin rashes). Very rare: anaphylaxis.
Frequency not known: severe skin adverse reactions (SSAR), Stevens-Johnson syndrome (SJS), toxic epidermal necrolysis (TEN), erythema multiforme, and toxic skin rashes.
Metabolism and nutrition disorders
Common: increased appetite, decreased appetite.
Rare: metabolic changes in patients with diabetes mellitus (decreased or increased blood glucose levels).
Psychiatric disorders
Common: depression, sleep disturbances, mood swings.
Nervous system disorders
Common: headache, paresthesia.
Rare: dizziness, transient dysgeusia.
Rare: as with other drugs in this class, very rare cases of pituitary apoplexy have been reported after initial administration of leuprorelin acetate in patients with pituitary adenoma.
Frequency not known: convulsions, idiopathic intracranial hypertension (pseudotumor cerebri), see section "Special precautions".
Cardiac disorders
Frequency not known: QT interval prolongation (see sections "Interaction with other medicinal products and other forms of interaction" and "Special precautions").
Very common: hot flushes.
Rare: changes in blood pressure (arterial hypertension or arterial hypotension).
Gastrointestinal disorders
Common: nausea/vomiting.
Uncommon: diarrhea.
Skin and subcutaneous tissue disorders
Uncommon: dryness of the skin and/or mucous membranes, night sweats.
Rare: alopecia.
Musculoskeletal and connective tissue disorders
Very common: arthralgia.
Common: joint and/or back pain, muscle weakness.
Frequency not known: bone demineralization (see section "Special precautions").
Renal and reproductive system disorders
Very common: decreased libido and sexual potency, reduction in testicular size.
Common: nocturia, dysuria, pollakiuria, gynecomastia.
Uncommon: dysuria, testicular pain.
Respiratory system disorders
Frequency not known: interstitial lung disease.
General disorders and administration site conditions
Very common: increased sweating, injection site reactions such as erythema, pain, swelling, pruritus, which usually resolve with continued treatment.
Common: fatigue, peripheral edema.
Investigations
Very common: increased body weight.
Common: weight loss, elevated lactate dehydrogenase (LDH), transaminases, γ-GT, and alkaline phosphatase, which may reflect the underlying disease.
Special notes:
Response to therapy with the medicinal product Leuprorelin-Vista should be monitored by measuring serum testosterone concentration 28 days after each injection and before each subsequent administration of Leuprorelin-Vista, as well as based on other laboratory tests such as acid phosphatase and PSA. For example, testosterone levels show an initial surge at the beginning of therapy, which then decreases within 2 weeks. Within 2–4 weeks, testosterone concentration reaches a level similar to that observed after bilateral orchidectomy and remains at this level throughout the treatment period. An increase in acid phosphatase levels may be observed at the initial stage of treatment and is transient. Acid phosphatase usually returns to normal or near-normal levels within a few weeks. Abscesses at the injection site are rare. In one report of an injection site abscess, absorption of leuprorelin from the depot was reduced. Therefore, in such cases, testosterone level determination is recommended.
Reporting suspected adverse reactions
Reporting of adverse reactions after medicinal product registration is of great importance. It allows continuous monitoring of the benefit-risk balance of the medicinal product. Healthcare professionals, pharmacists, patients, and their legal representatives should report all suspected adverse reactions and lack of efficacy via the Automated Pharmacovigilance Information System at the following link: https://aisf.dec.gov.ua
Shelf life. 4 years.
Storage conditions.
Store in the original packaging at a temperature not exceeding 30 °C. Keep out of reach of children.
Packaging.
One implant in a syringe-applicator (the syringe-applicator consists of a polymer body with an implant holder, needle, and plunger).
One syringe in a pouch together with a desiccant capsule. One pouch in a cardboard box.
Prescription category. Prescription only.
Marketing authorization holder.
Mistral Capital Management Limited
Manufacturer.
AMW GmbH
Manufacturer's address and location of operations.
Birkerfeld 11, Lochham, Warngau, Bavaria, 83627, Germany / Birkerfeld 11, Lochham, Warngau, Bavaria, 83627, Germany