Kafnea
UkraineTable of Contents
INSTRUCTIONS FOR MEDICAL USE OF THE MEDICINAL PRODUCT Cafnea (Cafnea®)
Composition:
Active substance: caffeine citrate;
1 vial (2 ml) contains 40 mg of caffeine citrate, equivalent to 20 mg of caffeine base;
Excipients: citric acid monohydrate; sodium citrate; water for injections.
Pharmaceutical form. Injection solution.
Main physicochemical properties: colorless solution, free from any visible particles.
Pharmacotherapeutic group. Psychostimulants. Psychostimulants, drugs used in attention deficit hyperactivity disorder (ADHD), and nootropic agents. Xanthine derivatives.
ATC code N06B C01.
Pharmacological Properties
Pharmacodynamics
Caffeine is a respiratory stimulant of central action. It significantly increases respiratory rate (breaths/minute) in premature infants and also significantly reduces the number of brief and prolonged apnea episodes. Evidence suggests that caffeine exerts a direct effect on the myocardium. In premature infants undergoing mechanical ventilation (MV), caffeine has been shown to reduce airway resistance and increase lung compliance, resulting in a concomitant reduction in oxygen requirements.
The following pharmacodynamic effects of caffeine have been observed in premature infants with apnea:
- Caffeine increases heart rate;
- Caffeine increases respiratory rate in some studies, but not in all;
- Mean arterial pressure, TcPO2 (transcutaneous partial pressure of oxygen), and TcPCO2 (transcutaneous partial pressure of carbon dioxide) remain unchanged;
- Blood flow in the celiac artery and superior mesenteric artery, LVO (left ventricular output), and PCO2 (partial pressure of carbon dioxide) do not change significantly;
- Caffeine increases cerebral blood flow in some studies, but not in all.
Pharmacokinetics
Absorption
After intravenous administration of a loading dose of 20 mg/kg of caffeine citrate, the mean peak plasma caffeine concentration is 12 mg/L. Following intravenous infusion of a single 10 mg/kg dose of caffeine citrate, mean ± SD (standard deviation) serum caffeine concentration was 14.5 ± 1.4 µg/mL at 10 minutes, 11.3 ± 0.1 µg/mL at 24 hours, and 6.1 µg/mL at 72 hours. After administration of a loading dose of 10 mg/kg caffeine citrate followed by oral maintenance doses of 5 mg/kg/day or 10 mg/kg/day, serum concentrations reached steady state after approximately 5 days, with higher concentrations observed with the 10 mg/kg/day maintenance dose (see figure below). Following maintenance doses of caffeine citrate 5 mg/kg, plasma caffeine levels range between 5 and 15 mg/L.
Distribution
Caffeine rapidly distributes throughout the body in infants, with a volume of distribution (V) of 0.8–0.9 L/kg.
Metabolism
In premature infants, caffeine is poorly metabolized. The main metabolites of caffeine are paraxanthine (primary metabolite), theobromine, and theophylline. Interconversion between caffeine and theophylline has been observed in premature infants, and it is expected that approximately 3–8% of administered caffeine is converted to theophylline.
Caffeine is metabolized in the liver by cytochrome P450 enzymes, primarily CYP1A2. This enzyme catalyzes N1-, N3-, and N7-demethylation of caffeine. In addition, CYP2E1 also catalyzes N1- and N7-demethylation, while CYP3A catalyzes 8-hydroxylation. The N3- and N7-demethylation metabolic pathways are immature until approximately 4 months after birth, which explains the prolonged elimination half-life and low clearance in infants under 4 months of age.
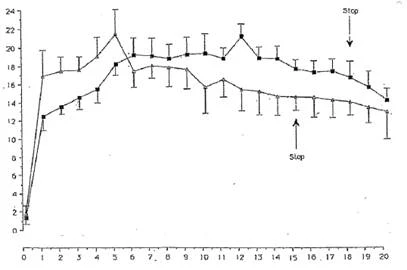
µg/mL
Days of life.
Figure. Mean ± SD serum caffeine concentrations after administration of caffeine citrate 10/5 (loading/maintenance dose) mg/kg [■] in 13 premature neonates and caffeine citrate 10/2.5 (loading/maintenance dose) mg/kg [Δ] in 10 premature neonates.
Elimination
More than 85% of caffeine is excreted unchanged in urine. In premature infants (gestational age 28 to 32 weeks), 85–97% of caffeine is excreted unchanged. The terminal half-life of caffeine decreases from birth and reaches adult-like values at approximately 60 weeks postnatal age. The half-life of caffeine in premature neonates is significantly longer than in term neonates. The mean terminal half-life in neonates ranges from 65 to 102 hours. In premature infants, caffeine elimination is slow, with a half-life of 80 to 120 hours. After discontinuation of treatment, serum caffeine concentrations are likely to remain elevated due to the prolonged elimination half-life of the drug (see figure above).
Special Patient Populations
Neonates of Asian origin tolerated an intravenous loading dose of 20 mg/kg caffeine citrate followed by intravenous maintenance doses of 5 mg/kg/day of caffeine citrate well. Use of higher maintenance doses was associated with increased incidence of hyperglycemia and tachycardia.
In other studies, no effect of sex or race on the volume of distribution of caffeine was established. Hepatic impairment, as defined by serum creatinine or urea levels, does not affect the volume of distribution.
Clinical Studies
Efficacy Studies
In a randomized, double-blind, placebo-controlled study conducted by Erenberg et al., the efficacy and safety of caffeine citrate for the treatment of apnea in premature neonates were evaluated. A total of 87 premature infants with a gestational age of 28 to 32 weeks were enrolled. Infants randomized to the caffeine group received an intravenous loading dose of 20 mg/kg caffeine citrate, followed by a daily maintenance dose of 5 mg/kg caffeine citrate administered either intravenously as an injection solution or orally as an oral solution for 10 days.
The primary endpoint was a reduction of at least 50% in the frequency of apnea episodes compared to baseline and resolution of apnea. Caffeine citrate was significantly more effective than placebo in achieving at least a 50% reduction in apnea frequency within 6 days (p < 0.05). The percentage of patients achieving at least a 50% reduction in apnea episodes was 68.9% in the active treatment group compared to 43.2% in the placebo group (p = 0.02). Caffeine citrate was also significantly more effective in resolving apnea within 5 days (p < 0.05). The percentage of patients in whom apnea episodes were resolved was 24.4% in the active treatment group compared to 0% in the placebo group (p = 0.005).
Safety Studies
A long-term safety study conducted by Schmidt et al. was a large-scale international trial involving 2006 randomized premature infants with birth weights between 500 and 1250 g, comparing caffeine to placebo to assess both short- and long-term safety of caffeine in the treatment or prevention of apnea in premature infants or to facilitate extubation. Infants in the treatment group received an intravenous loading dose of 20 mg/kg caffeine citrate, followed by a daily maintenance dose of 5 mg/kg administered either intravenously as an injection solution or orally as an oral solution. If apnea persisted, the daily maintenance dose could be increased up to a maximum of 10 mg/kg. The maintenance dose was adjusted weekly based on changes in body weight.
Table 1
Primary and secondary outcomes from the clinical study by Schmidt et al.
| Primary outcome (at corrected age 10–21 months) |
P-value |
Other outcomes (at corrected age 10–21 months) |
P-value |
Secondary short-term outcomes (until first discharge home) |
P-value |
| Composite |
Retinopathy of prematurity |
Death |
0.75 |
||
| Death or disability |
0.008 |
All stages |
0.06 |
Bronchopulmonary dysplasia |
< 0.001 |
| Components |
Severe retinopathy |
0.01 |
Retinopathy of prematurity |
0.09 |
|
| Death by 18 months |
0.87 |
Cerebral palsy |
0.2 |
Brain injury |
0.44 |
| Cerebral palsy |
0.009 |
Seizures |
0.85 |
Necrotizing enterocolitis |
0.63 |
| Cognitive developmental delay |
0.04 |
Growth percentile |
0.88 |
Pharmacologic treatment only for patent ductus arteriosus |
< 0.001 |
| Severe hearing loss |
0.41 |
Body weight percentile |
0.66 |
Surgical treatment of patent ductus arteriosus |
< 0.001 |
| Bilateral blindness |
0.58 |
Head circumference |
0.12 |
Safety data from preclinical studies.
Genotoxicity
Mutagenicity studies in bacteria and mammals in vitro, as well as clastogenicity studies in vitro and in vivo, generally did not demonstrate mutagenicity or clastogenicity of caffeine. Positive results observed in some studies were associated with extremely high concentrations, lethal doses, or non-validated methods. Therefore, the drug Cafnea is considered not to pose a genotoxic risk to patients.
Carcinogenicity
In a limited number of animal studies, caffeine did not demonstrate carcinogenic or oncogenic potential. In two-year carcinogenicity studies conducted in rats, caffeine (administered in pure form) did not increase tumor incidence when administered at oral doses up to 102 mg/kg/day in males and 170 mg/kg/day in females. Systemic exposure in animals at these doses was estimated to be 2−6 times higher than that in neonates receiving the recommended maintenance dose of 5 mg/kg/day of caffeine citrate.
Clinical characteristics.
Indications.
Short-term treatment of apnea in premature infants with a gestational age from 28 to 33 weeks.
Contraindications.
Hypersensitivity to the active substance or to any of the excipients.
Interaction with other medicinal products and other forms of interaction.
There is limited data on drug interactions with caffeine in premature neonates. However, CYP1A2 is the main enzyme responsible for caffeine metabolism; therefore, caffeine has the potential to interact with drugs that are substrates for this enzyme or that inhibit it or reduce its amount. Studies in adult patients have shown that concomitant administration of mexiletine, cimetidine, fluvoxamine, oral idrocilamide, oral methoxsalen, 5-methoxypsoralen, enoxacin, thiabendazole, artemisinin, fluconazole, terbinafine, and verapamil may reduce caffeine clearance. Concomitant administration of phenytoin may increase caffeine clearance. Caffeine reduces the effects of benzodiazepines. Caffeine increases levels of both endogenous and orally administered melatonin, as well as clozapine. Caffeine may cause reduced bioavailability of fluvoxamine.
When co-administered with antibacterial agents such as ciprofloxacin, enoxacin, pipemidic acid, lomefloxacin, norfloxacin, and ofloxacin, increased half-life and decreased clearance of caffeine have been reported.
Other methylxanthines (theophylline, aminophylline) should not be administered concomitantly.
Special precautions for use
Before starting treatment, other causes of apnea (e.g., central nervous system disorders, primary lung disease, anemia, sepsis, metabolic disturbances, cardiovascular disorders, or obstructive apnea) should be excluded or appropriately treated prior to initiating caffeine citrate therapy.
Caffeine is a central nervous system (CNS) stimulant, and seizures have been reported in cases of caffeine overdose. Caffeine citrate injection (brand name: Cafnea) should be used with caution in infants with epilepsy.
Clinical studies have shown that necrotizing enterocolitis may develop in neonates during treatment. Patients should be closely monitored for the development of necrotizing enterocolitis.
Cardiovascular system effects
Cafnea should be used with caution in infants with cardiovascular disorders, as caffeine has been shown to increase heart rate, left ventricular output, and stroke volume.
Renal and hepatic function impairment
Cafnea should be used with caution in infants with impaired renal or hepatic function. In such cases, serum caffeine concentrations should be monitored and dosage adjusted accordingly to avoid potential toxicity.
Gastroesophageal reflux disease (GERD)
Cafnea may relax the lower esophageal sphincter and increase gastric acid secretion, leading to an increased frequency of gastroesophageal reflux episodes in neonates.
Use during pregnancy or breastfeeding
Effects on reproductive function
Animal study data are limited but indicate no adverse effects on subsequent reproductive function following caffeine administration in neonates.
Use during pregnancy
Not applicable.
Use during breastfeeding
Women breastfeeding neonates receiving caffeine citrate therapy should avoid consuming food, beverages, or medicinal products containing caffeine. If women consume caffeine-containing beverages, this should be taken into account when determining the dosage of the medicinal product for the neonate.
Ability to affect reaction speed when driving or operating machinery
Administered in a hospital setting.
Administration and Dosage
The medicinal product Cafnea, solution for injection, is intended for use in specialized neonatal units. The medication is intended for single use in one patient only. Any unused portion should be discarded.
Prior to administration, ensure that no other methylxanthine (e.g., theophylline or aminophylline) is being administered.
Baseline serum caffeine levels should be determined if the mother consumed caffeine-containing beverages during pregnancy, as caffeine readily crosses the placenta.
The dosage expressed in terms of pure caffeine is half the dose of caffeine citrate (e.g., 20 mg of caffeine citrate is equivalent to 10 mg of caffeine).
Loading dose: 20 mg/kg of caffeine citrate administered intravenously via syringe pump over 30 minutes.
Maintenance dose: 5 mg/kg of caffeine citrate once daily until apnea resolves or until treatment is no longer considered necessary. If apnea persists, the maintenance dose may be increased up to a maximum of 10 mg/kg of caffeine citrate once daily. The maintenance dose should be adjusted weekly according to changes in body weight. If signs of caffeine toxicity occur—such as tachycardia, tachypnea (rapid breathing), hyperexcitability syndrome, tremor, unexplained seizures, or vomiting—the dose of caffeine citrate should be reduced or treatment discontinued. The dose of caffeine citrate should also be reduced or treatment stopped for other clinical reasons.
The maintenance dose should be administered intravenously over 10 minutes. Initiation of the maintenance dose should occur 24 hours after the loading dose.
Caffeine withdrawal syndrome: Symptoms of withdrawal syndrome after short-term treatment (less than three weeks) have not been reported.
Children
The medication is used in preterm neonates with a gestational age of 28 to 33 weeks.
Overdose
Symptoms
When doses exceeding the usual dose by three times were administered, no significant adverse effects were observed other than an increased incidence of hyperexcitability syndrome and decreased body weight, which normalized after discontinuation of treatment. Higher doses may cause fever, irritability, poor feeding, somnolence, tachypnea, hyperexcitability syndrome, fine limb tremor, arterial hypertension, opisthotonus, tonic-clonic movements, purposeless (uncontrolled) jaw and lip movements, vomiting, hyperglycemia, increased blood urea nitrogen, elevated total leukocyte count, seizures, neurological complications, tachycardia, respiratory distress syndrome, heart failure, abdominal distension, and acidosis.
Treatment
In case of caffeine overdose, treatment is primarily symptomatic and supportive. It has been observed that plasma caffeine levels decrease following exchange transfusion. Seizure management may include intravenous administration of diazepam or barbiturates such as sodium pentobarbital.
Adverse reactions.
Necrotizing enterocolitis is a common occurrence in premature infants, and therefore, regardless of whether the newborn is receiving caffeine, monitoring for the development of necrotizing enterocolitis is necessary.
Table 2
Percentage of adverse events most frequently reported during the Erenberg et al. study.
| Adverse event |
Treatment group |
|
| Caffeine citrate |
Placebo |
|
| Injection site reaction |
8.7 |
12.8 |
| Perinatal disorder (residual aspirates, feeding intolerance) |
8.7 |
5.1 |
| Constipation |
17.4 |
20.5 |
| Gastrointestinal disorders (gastroesophageal reflux, bowel loop dilation) |
4.3 |
7.7 |
| Anemia |
6.5 |
17.9 |
| Hypotremia |
0 |
5.1 |
| Rash |
8.7 |
7.7 |
The following effects were reported in uncontrolled studies:
Central nervous system stimulation: Irritability, excitation, hyperreflexia syndrome.
Cardiovascular disorders: Tachycardia, increased left ventricular ejection, and increased stroke volume.
Gastrointestinal disorders: Increased aspiration of gastric contents, gastrointestinal intolerance.
Changes in serum glucose levels: Hypoglycemia and hyperglycemia.
Renal disorders: Increased diuresis, increased creatinine clearance, and increased excretion of sodium and calcium.
Adverse effects observed in controlled clinical studies by Schmidt et al. included tachycardia, tachypnea (rapid breathing), hyperreflexia syndrome, tremor, seizures of unknown etiology, and vomiting. Caffeine temporarily reduced body weight gain.
Shelf life.
3 years.
Storage conditions.
Store in a place inaccessible to children, at a temperature not exceeding 30 °C.
Incompatibility.
Compatibility studies have not been performed, as the drug is not reconstituted or diluted prior to administration.
Packaging.
2 ml in a vial; 10 vials in a cardboard box.
Prescription status.
Prescription only.
Manufacturer.
Febra Pty Ltd.
Manufacturer's address and location of activity.
19 Orion Road, Lane Cove, New South Wales 2066, Australia.