Gonal-f®
UkraineTable of Contents
INSTRUCTIONS FOR MEDICAL USE OF THE MEDICINAL PRODUCT GONAL-fâ (GONAL-fâ)
Composition:
Active substance: follitropin alfa;
1 vial of powder contains 75 IU of follitropin alfa (recombinant human follicle-stimulating hormone – r-hFSH), equivalent to 5.5 mcg;
Excipients: sucrose, sodium hydrogen phosphate dihydrate, sodium dihydrogen phosphate monohydrate, methionine, polysorbate 20, concentrated phosphoric acid, sodium hydroxide;
Solvent: 1 pre-filled syringe with solvent contains 1 ml of water for injections.
Pharmaceutical form. Powder and solvent for solution for injection.
Main physicochemical properties: the preparation is a white lyophilisate in the form of a pellet; solvent – clear, colorless liquid. The pH of the diluted preparation solution ranges from 6.5 to 7.5.
Pharmacotherapeutic group. Gonadotrophins. ATC code G03GA05.
Pharmacological Properties
Pharmacodynamics
GONAL-f® is a preparation of follicle-stimulating hormone (FSH) produced by recombinant DNA technology using Chinese hamster ovary cells. In women, the primary effect of parenteral administration of FSH is the development of mature Graafian follicles.
In clinical studies, patients with severe deficiency of FSH and luteinizing hormone (LH) were defined by a serum level of endogenous LH < 1.2 IU/L; however, it should be noted that LH levels measured in different laboratories may vary.
In comparative clinical studies, during assisted reproductive technologies (ART) and ovulation induction, GONAL-f® demonstrated superior efficacy compared to urinary FSH, as evidenced by a lower total dose and shorter treatment duration required to achieve follicular maturation. In ART cycles, the use of lower doses of GONAL-f® over a shorter treatment period resulted in a higher number of oocytes and embryos cleaved on day 2 after fertilization compared to urinary FSH. In ovulation induction, treatment with GONAL-f® led to a lower rate of cycle cancellation due to therapeutic inefficacy compared to urinary FSH.
Results of study GF 8407—a randomized, parallel-group design study comparing the efficacy and safety of GONAL-f® and urinary FSH in ART
| GONAL-f® |
Urinary FSH |
|
| Number of oocytes retrieved |
11.0 ± 5.9 |
8.8 ± 4.8 |
| Duration of stimulation (days) |
11.7 ± 1.9 |
14.5 ± 3.3 |
| Total required FSH dose (number of 75 IU FSH vials) |
27.6 ± 10.2 |
40.7 ± 13.6 |
| Dose increase required (%) |
56.2 |
85.3 |
For all the listed criteria, the difference between the two groups was statistically significant (p < 0.05).
Concomitant administration of GONAL-f® and human chorionic gonadotropin (hCG) for at least 4 months induces spermatogenesis in men with FSH deficiency.
Pharmacokinetics.
After intravenous administration, follitropin alfa distributes into the extracellular fluid with an initial half-life of approximately 2 hours and is eliminated with a terminal half-life of about 1 day. The volume of distribution at steady state and total clearance are 10 L and 0.6 L/hour, respectively. One-eighth of the dose of follitropin alfa is excreted in urine.
After subcutaneous administration, the absolute bioavailability of follitropin alfa is approximately 70%. Repeated administration results in a threefold increase in its accumulation, reaching a steady state within 3–4 days. It has been demonstrated that in women with suppressed endogenous gonadotropin secretion, follitropin alfa effectively stimulates follicular development and steroidogenesis, despite low LH levels below the limit of quantification.
Clinical characteristics.
Indications.
Treatment of adult women
- Anovulation (including polycystic ovary syndrome) in women who have been unresponsive to clomiphene citrate treatment.
- Stimulation of multiple follicular development in patients undergoing superovulation as part of assisted reproductive technologies (ART), such as in vitro fertilization (IVF), gamete intrafallopian transfer (GIFT), and zygote intrafallopian transfer (ZIFT).
- Stimulation of follicular development in women with severe deficiency of luteinizing hormone (LH) and follicle-stimulating hormone (FSH) (in combination with an LH-containing preparation).
Treatment of adult men
- Stimulation of spermatogenesis in men with congenital or acquired hypogonadotropic hypogonadism, in conjunction with human chorionic gonadotropin (hCG) therapy.
Contraindications.
- Hypersensitivity to the active substance or to any of the excipients;
- tumors of the hypothalamus or pituitary gland;
- ovarian enlargement or cysts not related to polycystic ovary syndrome;
- gynecological bleeding of unknown etiology;
- carcinomas of the ovaries, uterus, or breasts.
The product must not be used if an effective response to treatment cannot be achieved, for example in the presence of:
- primary ovarian insufficiency;
- genital tract abnormalities incompatible with pregnancy;
- fibroid tumors of the uterus incompatible with pregnancy;
- primary testicular insufficiency.
Interaction with other medicinal products and other forms of interaction.
Concomitant use of GONAL-f® with other agents used to stimulate ovulation (e.g., hCG, clomiphene citrate) may enhance follicular response, whereas co-administration with gonadotropin-releasing hormone (GnRH) agonists or antagonists inducing pituitary desensitization may lead to an increased dosage requirement of GONAL-f® to achieve adequate ovarian response. No other clinically significant drug interactions during GONAL-f® therapy have been reported.
Special precautions for use.
Since GONAL-fâ exhibits significant gonadotropic activity, which may cause mild to severe adverse reactions, the drug should be prescribed only by physicians who are well experienced in infertility and its treatment.
Therapy with gonadotropins requires a significant time commitment from physicians and other healthcare professionals, as well as appropriate equipment for monitoring treatment. Safe and effective use of GONAL-fâ in women requires regular monitoring of ovarian response by ultrasound, preferably combined with simultaneous measurement of serum estradiol levels. Patient response to FSH administration is highly individual, with some patients responding poorly to FSH and others over-responding. For treatment of both women and men, the lowest effective dose of the drug should be used according to the treatment objective.
Patients with porphyria
GONAL-fâ should be administered to patients with porphyria or a family history of porphyria under strict medical supervision. Treatment should be discontinued at the first signs of disease onset or worsening.
Elderly patients and patients with renal or hepatic impairment
The safety and efficacy of GONAL-fâ in elderly patients, as well as in patients with renal or hepatic impairment, have not been established.
GONAL-fâ contains less than 1 mmol of sodium (23 mg) per dose, i.e., it is practically sodium-free.
Treatment of women
Prior to initiating treatment, infertile couples should undergo evaluation to identify existing or potential contraindications to pregnancy. In particular, patients should be screened for hypothyroidism, adrenal insufficiency, hyperprolactinemia, and appropriate specific treatment should be initiated if necessary.
During ovarian stimulation for the treatment of anovulatory infertility or assisted reproductive technologies (ART), ovarian enlargement or ovarian hyperstimulation may occur. Adherence to the recommended dosage and administration regimen of GONAL-fâ, along with careful monitoring of therapy, minimizes the frequency of such events. Accurate interpretation of follicular development and maturation requires an experienced specialist.
Clinical studies have shown increased ovarian sensitivity to GONAL-fâ when administered concomitantly with lutropin alfa. If an increase in FSH dose is considered necessary, it should preferably be adjusted every 7–14 days by increments of 37.5–75 IU. There has been no direct comparison between GONAL-fâ/LH and human menopausal gonadotropin (hMG). However, comparison with published data suggests that the ovulation rate achieved with GONAL-fâ/LH is similar to that obtained with hMG.
Ovarian hyperstimulation syndrome (OHSS)
An expected outcome of controlled ovarian stimulation is some degree of ovarian enlargement. This phenomenon, which is most common in women with polycystic ovary syndrome (PCOS), usually resolves spontaneously without treatment.
In contrast to uncomplicated ovarian enlargement, OHSS is a syndrome that may progress in severity. It is characterized by marked ovarian enlargement, high serum levels of sex steroids, and increased vascular permeability, which may lead to fluid accumulation in the abdominal, pleural, and rarely pericardial cavities.
In severe cases, OHSS may present with symptoms such as abdominal pain and distension, significant ovarian enlargement, weight gain, dyspnea, oliguria, and gastrointestinal symptoms including nausea, vomiting, and diarrhea. Clinical examination may reveal hypovolemia, hemoconcentration, electrolyte imbalance, ascites, hemoperitoneum, pleural effusions, hydrothorax, and acute respiratory distress syndrome. Rarely, severe OHSS may be complicated by ovarian torsion and thromboembolic events such as pulmonary embolism, ischemic stroke, and myocardial infarction.
Independent risk factors for OHSS include polycystic ovary syndrome, high absolute or rapidly rising serum estradiol levels (e.g., >900 pg/mL or >3300 pmol/L in anovulation; >3000 pg/mL or >11000 pmol/L in ART), and a large number of developing follicles (e.g., >3 follicles ≥14 mm in diameter in anovulation; ≥20 follicles ≥12 mm in diameter in ART).
Adherence to the recommended dosage and administration regimen of GONAL-fâ may minimize the risk of ovarian hyperstimulation. Monitoring of stimulation cycles by ultrasound and serum estradiol measurement is recommended for early identification of relevant risk factors.
It is known that hCG plays a key role in initiating OHSS and that this syndrome may become more severe and prolonged if pregnancy occurs. Therefore, in the presence of signs of ovarian hyperstimulation, such as serum estradiol levels >5500 pg/mL or >20200 pmol/L and development of more than 40 follicles in total, administration of hCG should be cancelled, and patients should be advised to abstain from sexual intercourse or use barrier contraception for at least 4 days. OHSS may progress rapidly (within 24 hours) and become a serious medical complication within a few days. It most commonly occurs after discontinuation of hormonal treatment and peaks approximately 7–10 days after treatment ends. Therefore, patients should remain under medical supervision for at least 2 weeks following hCG administration.
In ART, the incidence of hyperstimulation may be reduced by aspiration of all follicles prior to ovulation.
Mild or moderate forms of OHSS usually resolve spontaneously. If severe OHSS occurs, gonadotropin treatment should be discontinued if still ongoing, the patient should be hospitalized, and appropriate OHSS therapy initiated.
Multiples pregnancy
Multiple pregnancy, especially of higher order, carries an increased risk of adverse obstetric and perinatal outcomes.
The rate of multiple pregnancies is higher with ovulation induction than with natural conception. Most multiple conceptions are twins. To minimize the risk of multiple pregnancy, careful monitoring of ovarian response is recommended.
In ART procedures, the risk of multiple pregnancy is primarily related to the number of embryos transferred, embryo quality, and patient age.
Patients should be informed about the potential risk of multiple pregnancy before starting treatment.
Pregnancy loss
In women undergoing follicular stimulation for ovulation induction or ART, the rate of pregnancy loss due to miscarriage or spontaneous abortion is higher than with natural conception.
Ectopic pregnancy
Women with a history of tubal disease are at risk of ectopic pregnancy, regardless of whether conception occurs spontaneously or following infertility treatment. The incidence of ectopic pregnancy after ART has been reported to be higher than in the general population.
Reproductive system neoplasms
There have been reports of both benign and malignant neoplasms of the ovaries and other female reproductive organs in women who have received various fertility drugs. It has not yet been established whether gonadotropin treatment increases the baseline risk of such tumors in infertile women.
Congenital malformations
The incidence of congenital malformations after ART may be slightly higher than after spontaneous conception. This is believed to be due to differences in parental characteristics (e.g., maternal age, sperm quality) and multiple pregnancies.
Thromboembolic events
In women with established risk factors for thromboembolic events, such as personal or family history, or those with existing or recent thromboembolic disorders, gonadotropin treatment may further increase the risk of exacerbation or occurrence of such events. In such women, the benefits of gonadotropin use should be weighed against the risk of such events. However, it should be noted that pregnancy itself and OHSS both increase the risk of thromboembolic complications.
Treatment of men
Elevated endogenous FSH levels in patients indicate primary testicular insufficiency. Such patients are unresponsive to treatment with GONAL-fâ/LH preparations. GONAL-fâ should not be used if an effective treatment response cannot be achieved.
Semen analysis is recommended 4–6 months after initiation of treatment to assess treatment response.
Use during pregnancy or breastfeeding.
There are no indications for the use of GONAL-fâ during pregnancy. Data from a limited number of cases of drug use during pregnancy (fewer than 300 cases) suggest no congenital malformations or fetal or neonatal toxicity associated with follitropin alfa, although clinical data are insufficient to exclude a teratogenic effect of GONAL-fâ.
GONAL-fâ is not indicated for use during breastfeeding.
Effect on the ability to drive and use machines.
GONAL-fâ is expected to have no effect or a negligible effect on the ability of patients to drive or operate machinery.
Administration and Dosage
Treatment with GONAL-fâ should be initiated under the supervision of a physician experienced in the management of infertility.
Daily doses, administration schedule, and monitoring procedures during treatment with GONAL-f® should not differ from those used with urinary FSH preparations. Comparative clinical studies have shown that, compared to urinary FSH, a lower total dose of GONAL-f® is required over a shorter treatment period, allowing not only optimization of therapy but also minimizing the risk of ovarian hyperstimulation.
It is recommended to follow the proposed initial doses of the drug as outlined below.
Bioequivalence has been demonstrated for equivalent doses of the single-dose and multi-dose formulations of GONAL-f®.
Women with anovulation, including polycystic ovary syndrome
GONAL-fâ is administered as a course of daily injections. In patients with regular menstruation, treatment should begin within the first 7 days of the menstrual cycle.
The usual treatment regimen starts with daily administration of 75–150 IU FSH. If necessary, the dose may be increased by 37.5 IU (preferably) or 75 IU at intervals of 7 or (preferably) 14 days to achieve adequate, but not excessive, ovarian response. Treatment should be individualized based on the patient’s response, assessed by ultrasound evaluation of follicular size and/or serum estrogen levels. The maximum daily dose of FSH generally does not exceed 225 IU. If the patient does not respond adequately within 4 weeks, the treatment cycle should be discontinued, the patient should undergo further evaluation, and treatment should be restarted in the next cycle with a higher initial dose than in the previous cycle.
When optimal response is achieved, 250 mcg of recombinant LH (r-LH) or 5000–10000 IU of hCG should be administered as a single injection 24–48 hours after the last GONAL-f® injection. The patient is advised to have intercourse on the day of hCG administration and the following day. Alternatively, intrauterine insemination may be performed.
If excessive response occurs, treatment must be discontinued and hCG administration should be canceled (see section "Special Warnings and Precautions"). In the subsequent treatment cycle, therapy should be initiated with a lower FSH dose than that used in the previous cycle.
Stimulation of multiple follicular development in women undergoing controlled ovarian hyperstimulation in assisted reproductive technology (ART) or in vitro fertilization (IVF)
The usual regimen for controlled ovarian hyperstimulation involves daily administration of 150–225 IU of GONAL-f® starting on day 2 or 3 of the cycle. Treatment continues until adequate follicular development is achieved, as assessed by serum estrogen levels and/or ultrasound monitoring. The dose should be adjusted according to the patient’s response, but generally should not exceed 450 IU daily. Adequate follicular development is typically achieved by approximately day 10 of treatment (range: 5–20 days).
To induce final follicular maturation, a single injection of 250 mcg r-LH or 5000–10000 IU hCG should be administered 24–48 hours after the last GONAL-f® injection.
To suppress the premature surge of endogenous LH and control basal LH levels, pituitary suppression with gonadotropin-releasing hormone (GnRH) agonists or antagonists is usually employed. In a standard treatment protocol, GONAL-f® administration is initiated approximately 2 weeks after starting the agonist, and both agents are administered concurrently until adequate follicular development is achieved. For example, after 2 weeks of agonist treatment, daily administration of 150–225 IU GONAL-f® is initiated and continued for the first 7 days, with subsequent dose adjustments based on ovarian response.
Overall IVF experience indicates that the success rate generally remains stable during the first four treatment attempts and then gradually declines.
Women with anovulation due to severe deficiency of LH and FSH secretion
In women with severe deficiency of LH and FSH secretion (hypogonadotropic hypogonadism; endogenous LH serum level < 1.2 IU/L), the goal of combined therapy with GONAL-f® and lutropin alfa is the development of a single mature Graafian follicle, from which an oocyte will be released following hCG administration. GONAL-fâ is administered as a course of daily injections concomitantly with lutropin alfa. Since such patients typically present with amenorrhea and low endogenous estrogen secretion, treatment may be initiated at any time.
The recommended regimen begins with daily administration of 75 IU lutropin alfa together with 75–150 IU FSH. Treatment should be individualized based on the patient’s response, assessed by serum estrogen levels and ultrasound evaluation of follicular size.
If an increase in FSH dose is required, it should be adjusted by increments of 37.5–75 IU at intervals of 7–14 days. In a single cycle, stimulation duration may be extended up to 5 weeks.
When optimal response is achieved, 250 mcg r-LH or 5000–10000 IU hCG should be administered as a single injection 24–48 hours after the last injection of GONAL-f® and lutropin alfa. The patient is advised to have intercourse on the day of hCG administration and the following day. Alternatively, intrauterine insemination may be performed.
During treatment, luteal phase support should be considered, as the absence of substances with luteotropic activity (LH/hCG) after ovulation may lead to premature luteal phase deficiency.
If excessive ovarian response occurs, treatment must be discontinued and hCG administration should be canceled. In the subsequent treatment cycle, therapy should be initiated with a lower FSH dose than that used in the previous cycle.
Men with hypogonadotropic hypogonadism
GONAL-fâ is administered at a dose of 150 IU three times weekly, in combination with hCG, for at least 4 months. If no response is observed after this period, combined treatment may be continued. Clinical experience indicates that, if necessary, treatment may be continued for at least 18 months to achieve spermatogenesis.
If you are self-administering GONAL-fâ, please carefully read and follow the instructions below.
GONAL-fâ is intended for subcutaneous injection. Self-injection of GONAL-f® should only be performed by patients who have been properly trained and who have access to expert advice if needed. The first injection of GONAL-f® must be administered under the direct supervision of a healthcare professional. Subsequent injections should be given at the same time each day, rotating injection sites. Do not use the solution if it is cloudy or contains particles.
Immediately before administration, the powder should be reconstituted with the solvent provided in the package. To avoid injecting large volumes, no more than the contents of 3 vials of the drug should be dissolved in 1 mL of solvent.
- Wash your hands. It is important that your hands and all materials you will use are as clean as possible.
- Prepare all necessary materials. Place on a clean surface one vial of the drug, one pre-filled syringe with solvent, one needle for reconstitution, one fine needle for subcutaneous injection, two alcohol swabs, and a sharps container for used glass and needles.
- Prepare the injection solution. Remove the protective caps from the drug vial and the pre-filled syringe with solvent.
|
|
Attach the needle for solution preparation to the pre-filled syringe with solvent and slowly inject the entire solvent into the vial with powder. Gently mix the contents of the vial with circular movements, without removing the syringe needle. Do not shake the vial. |

|
|
After dissolving the powder (which usually occurs immediately), check the clarity of the resulting solution and the absence of any particles in it. Turn the vial upside down and slowly draw the solution back into the syringe. |
(If you have been prescribed to administer the contents of several GONAL-fâ vials, repeatedly draw the solution into the syringe and re-inject it into the next vials of powder until you have dissolved the contents of the prescribed number of vials of powder. If, in addition to GONAL-fâ, you have also been prescribed luteinizing hormone alpha, you may also mix these two medications, which is an alternative to administering each medication separately. In this case, after dissolving the luteinizing hormone alpha powder, draw the solution back into the syringe and re-inject it into the vial containing GONAL-fâ powder. After dissolving, draw the solution back into the syringe. Check the solution for particles as described above and do not use the solution if it is not clear. The contents of up to three vials of powder can be dissolved in 1 ml of solvent.)
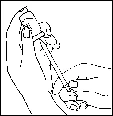
- Replace the needle with a fine needle suitable for subcutaneous injections and remove any air bubbles from the syringe.
|
|
If you see air bubbles in the syringe, gently tap the syringe while holding it with the needle pointing upwards until all the air collects in the upper part. Press the plunger of the syringe until all air bubbles are expelled. |

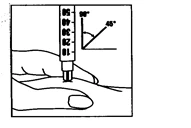
- Immediately after this, administer the injection: Your doctor or nurse has already advised you where to inject (for example, in the abdomen or front of the thigh).
|
|
Wipe the area selected for injection with an alcohol swab. Firmly pinch the skin and insert the needle at a 45–90° angle. Inject under the skin as you have been trained. Do not inject directly into a vein. Inject all of the solution by gently pushing the plunger. Immediately remove the needle and wipe the skin with a circular motion using an alcohol swab. |
- Dispose of all used materials: Immediately after completing the injection, place all needles and empty glass containers into a sharps container. Unused solution should also be disposed of.
Children.
GONAL-fâ is not used for the treatment of children.
Overdose.
Symptoms of GONAL-fâ overdose are unknown; however, the possibility of developing ovarian hyperstimulation syndrome, as described in the section «Special precautions», cannot be excluded.
Adverse Reactions
The most commonly reported adverse reactions associated with the use of the medicinal product are headache, ovarian cysts, and local injection site reactions (e.g., pain, erythema, hematoma, swelling, and/or irritation at the injection site).
Mild to moderate ovarian hyperstimulation syndrome (OHSS), which is also frequently reported, is an inherent risk of the stimulation procedure; however, severe OHSS is uncommon.
Very rarely, thromboembolic complications may occur.
The following classification is used to define the frequency of adverse reactions: very common (≥ 1/10); common (≥ 1/100 to < 1/10); uncommon (≥ 1/1,000 to < 1/100); rare (≥ 1/10,000 to < 1/1,000); very rare (< 1/10,000).
Treatment of Women
Immune system disorders
Rare: hypersensitivity reactions ranging from mild to severe, including anaphylactic reactions and shock.
Nervous system disorders
Very common: headache.
Vascular disorders
Rare: thromboembolism (with or without OHSS).
Respiratory, thoracic and mediastinal disorders
Rare: exacerbation or worsening of asthma.
Gastrointestinal disorders
Common: abdominal pain, sensation of abdominal distension and discomfort, nausea, vomiting, diarrhea.
Reproductive and breast disorders
Very common: ovarian cysts;
Common: mild to moderate OHSS (including associated symptoms);
Uncommon: severe OHSS (including associated symptoms) (see section "Special precautions");
Rare: complications of severe OHSS.
General disorders and administration site conditions
Very common: injection site reactions (e.g., pain, erythema, hematoma, swelling, and/or irritation at the injection site).
Treatment of Men
Immune system disorders
Rare: hypersensitivity reactions ranging from mild to severe, including anaphylactic reactions and shock.
Respiratory, thoracic and mediastinal disorders
Rare: exacerbation or worsening of asthma.
Skin and subcutaneous tissue disorders
Common: acne.
Reproductive and breast disorders
Common: gynecomastia, varicocele.
General disorders and administration site conditions
Very common: injection site reactions (e.g., pain, erythema, hematoma, swelling, and/or irritation at the injection site).
Other
Common: weight gain.
Reporting suspected adverse reactions after medicinal product authorization is important. It allows continued monitoring of the benefit-risk balance of the medicinal product. Healthcare professionals and patients are encouraged to report any suspected adverse reactions and lack of efficacy via the Automated Pharmacovigilance Information System at the following link: https://aisf.dec.gov.ua.
Shelf life. 3 years.
Do not use after the expiry date stated on the packaging.
For immediate and single use after first opening and reconstitution.
Storage conditions.
Store at a temperature not exceeding 25°C.
Store in the original packaging to protect from light.
Keep out of the reach of children.
Packaging.
- Powder for solution for injection in vial No. 1 in a set with solvent (1 ml of water for injections) in a pre-filled syringe No. 1, reconstitution needle No. 1, administration needle No. 1 in a blister pack; 1 blister pack in a cardboard box.
- Powder for solution for injection in vials No. 5 in a set with solvent (1 ml of water for injections) in pre-filled syringes No. 5, reconstitution needles No. 5, administration needles No. 5 in a blister pack; 2 blister packs in a cardboard box.
Prescription status. Prescription only.
Manufacturer.
Merck Serono S.A., Aubonne branch / Merck Serono S.A., Succursale d’Aubonne;
Merck Serono S.p.A.
Manufacturer's location and address of its business premises.
Zone Industrielle de l'Ouriettaz, 1170 Aubonne, Switzerland;
Via delle Magnolie 15 (locality frazione Zona Industriale), 70026 Modugno (Bari), Italy.