Fortex
Ukraine
Table of Contents
INSTRUCTIONS for MEDICAL USE of the medicinal product FORTIX (FORTIX)
Composition:
Active substance: formoterol;
1 capsule contains formoterol fumarate dihydrate equivalent to 12 mcg of formoterol fumarate;
Excipients: partially micronized lactose monohydrate, micronized lactose monohydrate;
Capsule shell: gelatin.
Pharmaceutical form. Powder for inhalation, hard capsules.
Main physicochemical properties: white powder in transparent colorless hard gelatin capsules of size "3".
Pharmacotherapeutic group. Medicinal products used in obstructive respiratory diseases. Selective β2-adrenoreceptor agonists. ATC code R03AC13.
Pharmacological properties.
Pharmacodynamics.
Formoterol fumarate is a selective β2-adrenergic agonist. In patients with reversible airway obstruction, it produces a rapid bronchodilating effect (within 1–3 minutes), which lasts significantly for up to 12 hours after inhalation. At therapeutic doses, the effect on the cardiovascular system is minimal and occurs only in isolated cases.
Formoterol inhibits the release of histamines and leukotrienes from passively sensitized human lungs. Formoterol effectively prevents bronchospasm induced by physical exertion or methacholine. Since the bronchodilating effect of the drug is pronounced for 12 hours after inhalation, maintenance therapy with formoterol administered twice daily allows, in most cases, adequate control of bronchospasm in chronic lung diseases both during the day and at night.
In studies evaluating the use of formoterol for the treatment of conditions associated with chronic obstructive pulmonary disease (COPD), improvements in disease symptoms, lung function, and quality of life were observed. Formoterol acted on reversible airway obstruction.
Severe exacerbations of bronchial asthma
Results from placebo-controlled clinical trials of formoterol treatment for at least 4 weeks showed a higher incidence of severe exacerbations of bronchial asthma in patients receiving formoterol compared to those in the placebo group, particularly in children aged 5–12 years.
Pharmacokinetics.
The therapeutic dose of formoterol ranges from 12 to 24 mcg twice daily. Data on the pharmacokinetic properties of formoterol were obtained from studies in healthy volunteers after inhalation of doses exceeding the therapeutic range, and in COPD patients after inhalation of therapeutic doses. The amount of unchanged formoterol excreted in urine is used as an indirect measure of total systemic exposure and correlates with data on plasma elimination. Elimination half-lives calculated for urine and plasma are similar.
Absorption.
After administration of a formoterol dose exceeding the therapeutic level (single dose of 120 mcg), maximum plasma concentration (Cmax) of 266 pmol/L was observed 5 minutes after inhalation. In COPD patients receiving formoterol at doses of 12 or 24 mcg twice daily for 12 weeks, plasma concentrations measured 10 minutes, 2 hours, and 6 hours after inhalation ranged between 11.5–25.7 pmol/L and 23.3–50.3 pmol/L, respectively.
Assessment of total excretion of formoterol and/or its (R,R)- and (S,S)-enantiomers showed that systemic exposure to formoterol increased proportionally with the administered dose (12–96 mcg).
After repeated inhalation of 12 or 24 mcg of formoterol fumarate twice daily for 12 weeks, urinary excretion of unchanged formoterol increased by 63% to 73% (last dose compared to first dose) in patients with bronchial asthma, by 19% to 38% in adult COPD patients, and by 18–84% in children. These data indicate limited accumulation of formoterol in plasma after repeated dosing. No relative preferential accumulation of one enantiomer over the other was observed after repeated administration.
As with other inhaled medications, a significant portion of the formoterol dose from the inhaler is expected to be swallowed and subsequently absorbed from the gastrointestinal tract. After oral administration of 80 micrograms of tritium-labeled formoterol fumarate to two healthy volunteers, at least 65% of the administered dose was absorbed.
Distribution.
Plasma protein binding of formoterol ranges between 61–64% (primarily to albumin — 34%). At concentrations achieved after therapeutic doses, binding sites are not saturated.
Metabolism.
The main metabolic pathway of formoterol is direct glucuronidation. Another pathway is O-demethylation followed by glucuronidation. Other metabolic processes include conjugation of formoterol with sulfate and deformylation, followed by sulfate conjugation. O-demethylation and glucuronidation are catalyzed by multiple isoenzymes (UGT1A1, 1A3, 1A6, 1A7, 1A8, 1A9, 1A10, 2B7, 2B15 and CYP2D6, 2C19, 2A6, respectively), indicating a low likelihood of drug interactions due to inhibition of specific isoenzymes involved in formoterol metabolism. Formoterol, at therapeutic concentrations, does not inhibit cytochrome P450 isoenzymes.
Excretion.
In patients with bronchial asthma or COPD treated for 12 weeks with 12 or 24 mcg of formoterol fumarate twice daily, approximately 10% and 7% of the dose, respectively, was excreted unchanged in urine. In children with bronchial asthma, about 6% of the administered dose of unchanged formoterol was detected in urine after repeated administration of 12 and 24 mcg doses. The (R,R) and (S,S) enantiomers accounted for 40% and 60%, respectively, of unchanged formoterol in urine after single doses (12–120 mcg) in healthy volunteers and after single and repeated doses in patients with bronchial asthma.
The active substance and its metabolites are completely eliminated from the body; approximately ⅔ of the orally administered dose is excreted in urine and ⅓ in feces. Renal clearance of formoterol is 150 mL/min.
In healthy volunteers, the elimination half-life of formoterol in plasma after inhalation of a single 120 mcg dose of formoterol fumarate is 10 hours. In contrast, elimination half-lives of the (R,R) and (S,S) enantiomers, calculated based on urinary excretion data, are 13.9 and 12.3 hours, respectively.
Pharmacokinetic properties of formoterol in elderly patients and in patients with hepatic or renal impairment have not been studied.
Clinical characteristics.
Indications.
The medicinal product FORTICS is indicated for the treatment of bronchial asthma (including nocturnal attacks of bronchial asthma and symptoms of bronchospasm induced by physical exertion) in patients who are receiving treatment with inhaled corticosteroids and who require additional administration of long-acting β2-agonists.
The medicinal product FORTICS is indicated for relief of reversible airway obstruction in patients with chronic obstructive pulmonary disease (COPD) who require long-term bronchodilator therapy.
Contraindications.
Hypersensitivity to formoterol, to any other components of the drug or to other β2-adrenergic stimulants.
Tachyarrhythmia, third-degree atrioventricular block, idiopathic subvalvular aortic stenosis, hypertrophic obstructive cardiomyopathy, thyrotoxicosis.
Patients with suspected or known QT interval prolongation (QTc > 0.44 s).
Interaction with other medicinal products and other types of interactions.
Concomitant use of formoterol and medicinal products such as quinidine, disopyramide, procainamide, phenothiazines, antihistamines (e.g., terfenadine, astemizole, mizolastine), tricyclic antidepressants, monoamine oxidase inhibitors (MAOIs), macrolides, or drugs that prolong the QT interval requires caution, as their effects on the cardiovascular system may be potentiated (e.g., drugs that increase the QT interval increase the risk of ventricular arrhythmias).
Concomitant use of other sympathomimetic agents or ephedrine may enhance the adverse effects of formoterol and may require dose titration.
Concomitant use of xanthine derivatives, steroids, or diuretics may potentiate the potential hypokalemic effect of β2-adrenergic stimulants. Hypokalemia increases susceptibility to cardiac arrhythmias (e.g., in patients receiving cardiac glycosides).
In patients receiving anesthesia with halogenated hydrocarbons, there is a risk of cardiac rhythm disturbances.
Anticholinergic agents, corticosteroids, and xanthine derivatives may enhance the bronchodilator effect of formoterol.
β-adrenergic blockers may attenuate or completely counteract the effect of formoterol; therefore, β-blockers (including ophthalmic drops) should not be administered concomitantly with formoterol unless no alternative exists.
Formoterol may interact with monoamine oxidase inhibitors (MAOIs); therefore, patients receiving these drugs should not use formoterol during treatment and for 14 days after discontinuation of MAOI therapy.
In addition, L-dopa, L-thyroxine, oxytocin, and alcohol may impair cardiovascular tolerance to β2-sympathomimetics.
Special precautions for use.
Formoterol should not be used (its effect is not sufficient) as a first-line drug for the treatment of bronchial asthma.
The dose of formoterol should be individually adjusted according to the patient's needs. The lowest effective dose providing therapeutic effect should be used. The maximum recommended dose should not be exceeded (see "Dosage and administration").
Death associated with bronchial asthma.
Formoterol fumarate dihydrate belongs to the class of long-acting β2-adrenergic receptor agonists. In clinical trials with salmeterol, another long-acting β2-agonist, a higher incidence of asthma-related deaths was observed in the active treatment group (13/13,176) compared to the placebo group (3/13,179). Adequate studies have not been conducted to determine whether the frequency of asthma-related deaths increases with formoterol-containing medicinal products.
Anti-inflammatory treatment.
Before prescribing formoterol, the patient's condition should be assessed to determine whether adequate anti-inflammatory treatment is being received. When asthma symptoms are under control, the formoterol dose should be gradually reduced. The patient's condition should be regularly monitored during dose reduction.
Although formoterol may be added to the treatment regimen when inhaled corticosteroids do not provide sufficient control of asthma symptoms, formoterol therapy should not be initiated during severe asthma exacerbations or in cases of significant or acute worsening of asthma.
At the beginning of formoterol treatment, there may be a risk of adverse effects related to bronchial asthma, including worsening of its course. If asthma symptoms remain uncontrolled or if the patient's condition deteriorates after formoterol inhalation, the patient should consult a physician regarding the appropriateness of continuing treatment.
Formoterol should not be used concomitantly with other long-acting β2-adrenergic stimulants. In the treatment of patients with bronchial asthma, formoterol should be used only as an add-on therapy in combination with inhaled corticosteroids: for patients whose asthma is not adequately controlled by inhaled corticosteroids alone, or for patients in whom disease exacerbation warrants initiating treatment with inhaled corticosteroids and a long-acting β2-adrenergic stimulant.
Formoterol is not indicated for use in children under 6 years of age due to insufficient experience with its use in this age group.
For children aged 6 to 12 years, a combination product containing inhaled corticosteroids and a long-acting β2-adrenergic stimulant is recommended, except in cases where separate administration of inhaled corticosteroids and a long-acting β2-adrenergic stimulant is required.
If patients are not receiving anti-inflammatory treatment, it should be initiated simultaneously with the start of formoterol therapy. Patients should be advised to continue anti-inflammatory therapy after starting formoterol, even if their condition improves. Persistent symptoms or the need to increase the formoterol dose to control symptoms usually indicate worsening of the underlying disease and the need to reassess treatment.
If bronchial asthma symptoms improve, a gradual reduction in the formoterol dose may be considered. It is important to regularly monitor patients during dose reduction. The lowest effective dose of formoterol should be used.
Fatalities have been reported following overdose of medications containing β-adrenergic stimulants, although the exact cause of death is unknown. In several cases, death was due to cardiac arrest. Patients should be informed about the importance of strictly adhering to dosage recommendations and the inadmissibility of exceeding the maximum dose.
Exacerbations of bronchial asthma.
Clinical trials using formoterol indicate a higher frequency of severe exacerbations of bronchial asthma in patients receiving formoterol compared to those receiving placebo, particularly in children aged 6 to 12 years. These studies do not allow precise determination of the difference in the number of asthma exacerbation events between the study groups.
If symptoms persist or the number of formoterol doses required to control disease symptoms increases, this usually indicates worsening of the underlying condition and the need for a physician to reassess the basic therapy for bronchial asthma.
Initiation of formoterol treatment or dose escalation should not be undertaken during severe asthma exacerbations or if symptoms significantly worsen or asthma progresses to a more severe form.
In case of an asthma attack, a short-acting β2-adrenergic stimulant should be used. Patients should be instructed to seek immediate medical help in case of sudden asthma exacerbation.
Frequent use of the drug (i.e., prophylactic treatment, e.g., with corticosteroids and long-acting β2-adrenergic stimulants) several times a week to prevent exercise-induced bronchospasm, despite ongoing maintenance therapy, may indicate inadequate control of bronchial asthma and may be a reason to reassess treatment and evaluate patient adherence to physician recommendations.
Concomitant diseases.
Formoterol should be used with particular caution and under physician supervision, especially regarding adherence to the recommended dose, in the following conditions: ischemic heart disease; myocardial infarction; severe heart failure or severe uncompensated heart failure; severe arterial hypertension; aortic aneurysm; pheochromocytoma.
Formoterol may prolong the QTc interval. The medicinal product should be used cautiously in patients taking drugs that affect the QTc interval.
Due to the hyperglycemic effect inherent to β2-adrenergic stimulants, additional monitoring of blood glucose levels is recommended for patients with diabetes mellitus.
Caution should be exercised when administering theophylline and formoterol concomitantly in patients with pre-existing heart disease.
Hypokalemia.
β2-adrenergic stimulant therapy may lead to potentially serious hypokalemia. Since this drug effect may be enhanced by hypoxia and concomitant therapy, particular caution is required in patients with severe bronchial asthma. In such cases, regular monitoring of serum potassium levels is recommended.
Paradoxical bronchospasm.
As with other inhaled therapies, the possibility of paradoxical bronchospasm should be considered during formoterol use. In such cases, the drug should be discontinued immediately and alternative treatment initiated.
The medicinal product contains lactose; therefore, it should not be used in patients with rare hereditary forms of galactose intolerance, Lapp lactase deficiency, or glucose-galactose malabsorption syndrome.
Incorrect use.
Some patients have mistakenly swallowed formoterol capsules instead of using them via an inhalation device. Most such incidents were not associated with adverse reactions. Healthcare professionals should discuss the correct use of the medicinal product with patients. If a patient prescribed formoterol does not experience improvement in breathing, the healthcare professional should inquire about how the patient is using formoterol.
Use during pregnancy or breastfeeding.
The safety of formoterol use during pregnancy or breastfeeding has not been established.
Animal studies have shown that formoterol causes embryotoxic effects and reduces early postnatal survival and birth weight.
It should not be used during pregnancy except when no safer alternative is available. Like other β2-adrenergic stimulants, formoterol may delay labor due to its relaxing effect on uterine smooth muscle.
It is unknown whether formoterol is excreted in breast milk. Women should discontinue breastfeeding during treatment.
Fertility
Data on the effect of formoterol on human fertility are lacking. In studies in male and female rats, no fertility impairments were observed.
Ability to affect reaction speed when driving or operating machinery.
If dizziness, tremor, or seizures occur during treatment, patients should not drive or operate complex machinery.
Administration and Dosage.
Formoterol is intended for inhalation use in adults, including elderly patients, and children aged 6 years and older.
The medicinal product FORTEX should only be prescribed in combination with an inhaled corticosteroid.
Adults (including elderly patients and children aged 12 years and older).
Bronchial asthma.
Regular maintenance therapy: 1 capsule of powder for inhalation (equivalent to 12 mcg of formoterol fumarate dihydrate) twice daily. In more severe cases, 2 capsules of powder for inhalation twice daily may be used. This dosing regimen provides symptomatic relief during both day and night. The maximum recommended daily dose for maintenance therapy is 48 mcg. If additional doses are required more frequently than 2 days per week, the treatment regimen should be reviewed, as this may indicate worsening of the underlying disease.
FORTEX should not be used to relieve acute symptoms of bronchial asthma attacks. In case of acute attack, a short-acting β2-agonist should be used.
Chronic obstructive pulmonary disease (COPD).
Regular maintenance therapy: 1 capsule of powder for inhalation (equivalent to 12 mcg of formoterol fumarate dihydrate) twice daily.
Children aged 6 to 12 years.
Bronchial asthma.
The medicinal product FORTEX should only be prescribed in combination with inhaled corticosteroids.
Regular maintenance dose: 1 capsule of powder for inhalation (12 mcg) twice daily.
The maximum recommended daily dose is 24 mcg.
When inhaled corticosteroid and long-acting β2-agonist therapy is indicated in children aged 6–12 years, a combination product is recommended, except in cases where separate administration of inhaled corticosteroid and long-acting β2-agonist is considered more appropriate.
FORTEX should not be used to relieve acute symptoms of bronchial asthma attacks. In case of acute attack, a short-acting β2-agonist should be administered.
Renal and hepatic impairment
There are no theoretical reasons to assume that dose adjustment of formoterol is required in patients with renal or hepatic impairment; however, clinical data on use in these populations are lacking.
Elderly patients (aged over 65 years)
The pharmacokinetics of formoterol have not been studied in elderly populations. Available results from clinical trials involving elderly patients do not indicate the need for doses different from those recommended for other adults.
Warning: Do not use more than 4 doses (48 mcg) per day (risk of cardiac arrest).
Administration method
A physician or other healthcare professional should explain to the patient how to use the inhaler.
Capsules should be removed from the blister pack only immediately before use.
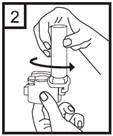
- Remove the protective cap.

- To open the inhaler, firmly hold the base and rotate the mouthpiece in the direction of the arrow.
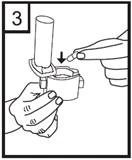
- Place the capsule into the chamber at the base of the inhaler. It is important to remove the capsule from the blister pack only immediately before use.
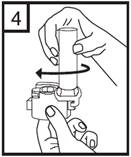
- Rotate the mouthpiece back to the closed position.
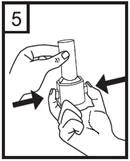
- Press the red buttons while holding the inhaler vertically. Release the buttons.
- Breathe out fully.

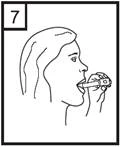
- Place the mouthpiece in the mouth and tilt the head slightly backward. Close lips tightly around the mouthpiece and inhale quickly and continuously as deeply as possible.
- Hold breath as long as possible without discomfort, simultaneously removing the inhaler from the mouth. Then exhale. Open the inhaler to check whether any powder remains in the capsule. If powder remains, repeat steps 6–8.
- After use, remove the empty capsule, close the mouthpiece, and cover the inhaler with the cap.
To remove residual powder, clean the mouthpiece and capsule chamber with a dry cloth. A soft brush may also be used for cleaning.
Children.
Formoterol should not be used in children under 6 years of age due to insufficient clinical experience in this patient group.
Overdose.
Symptoms: formoterol overdose may cause effects typical of excessive action of other β2-adrenergic agonists, such as nausea, vomiting, headache, tremor, drowsiness, palpitations, tachycardia, dizziness, ventricular arrhythmias, metabolic acidosis, hypokalemia, hyperglycemia, QT interval prolongation on electrocardiogram, arterial hypertension.
Treatment: supportive and symptomatic therapy is indicated. Hospitalization is required in severe cases.
β-adrenoblockers may be considered, but only with extreme caution, as their use may provoke bronchospasm.
In cases of severe intoxication, serum electrolyte concentrations (e.g., potassium) and acid-base balance should be monitored.
Adverse reactions.
Severe exacerbation of bronchial asthma.
The frequency of the adverse reactions listed below is defined as follows: very common (≥1/10), common (≥1/100, <1/10), uncommon (≥1/1000, <1/100), rare (≥1/10,000, <1/1000), and very rare (<1/10,000).
| Immune system disorders |
Very rare: hypersensitivity (including arterial hypotension, angioedema) Rare: hypersensitivity reactions, including bronchospasm, urticaria, swelling, pruritus, exanthema, rash** |
| Metabolism and nutrition disorders |
Rare: hypokalemia Very rare: hyperkalemia, hyperglycemia |
| Central nervous system disorders |
Common: headache, tremor Uncommon: dizziness Very rare: taste disturbances |
| Psychiatric disorders |
Uncommon: excitement, anxiety, nervousness, insomnia, restlessness |
| Cardiovascular system disorders |
Common: palpitations Uncommon: tachycardia Rare: arrhythmia, e.g. atrial fibrillation, supraventricular tachycardia, extrasystoles Very rare: angina pectoris, prolonged QT interval on electrocardiogram, peripheral edema, blood pressure changes |
| Respiratory and thoracic disorders |
Uncommon: paradoxical bronchospasm, pharyngeal irritation, allergic reactions, acute worsening of bronchial asthma* Frequency unknown: cough** |
| Gastrointestinal disorders |
Uncommon: dry mouth Very rare: nausea |
| Musculoskeletal system disorders |
Uncommon: myalgia, muscle cramps |
| Other |
Frequency unknown: eye mucosa irritation, eyelid edema, increased blood pressure (including arterial hypertension)** |
* The percentage of patients experiencing serious exacerbations of bronchial asthma was higher in the group receiving formoterol than in the placebo group, with the greatest difference observed in children aged 5–12 years.
** These adverse reactions were reported by patients treated with a formoterol-containing medicinal product during the post-marketing period.
As with all other types of inhaled therapy, paradoxical bronchospasm may occur very rarely. Treatment with β2-agonists may lead to increased blood levels of insulin, free fatty acids, glycerol, and ketone bodies. The excipient lactose contains a small amount of milk proteins, which may cause allergic reactions.
Shelf life.
2 years.
Storage conditions.
Store at a temperature not exceeding 25 °C.
Keep in the original packaging.
Keep out of reach of children.
Packaging.
10 capsules per blister; 6 blisters per cardboard box, supplied with an inhaler.
Prescription category.
Prescription only.
Manufacturer: Laboratorios Noscua, S.A.
Manufacturer's address and place of business.
Ctra. Miralcampo, No. 7, Polígono Industrial Miralcampo, 19200 Azuqueca de Henares, Guadalajara, Spain.