Formoterol izihaler
Ukraine
Table of Contents
INSTRUCTIONS FOR MEDICAL USE OF THE MEDICINAL PRODUCT FORMOTEROL EASYHALER (FORMOTEROL EASYHALER)
Composition:
Active substance: formoterol;
1 dose emitted from the mouthpiece contains 12 mcg of formoterol fumarate dihydrate;
Excipient: lactose monohydrate.
Pharmaceutical form. Powder for inhalation.
Main physicochemical properties: white or off-white powder.
Pharmacotherapeutic group.
Selective β2-adrenoreceptor agonists. ATC code R03AC13.
Pharmacological Properties.
Pharmacodynamics.
Mechanism of action. Formoterol is a selective β2-adrenoceptor agonist. In patients with reversible airway obstruction, it produces bronchodilation. This effect develops rapidly (within 1–3 minutes) and remains significantly pronounced for up to 12 hours after inhalation.
Pharmacokinetics.
Absorption. As with other inhaled medications, approximately 80% of the formoterol delivered via the "Easyhaler" inhaler is likely to be swallowed and subsequently absorbed from the gastrointestinal tract. Therefore, pharmacokinetic data obtained from oral dosage forms are largely applicable to the inhaled powder. After inhalation of therapeutic doses, formoterol is not detectable in plasma using currently available analytical methods.
Absorption is rapid and extensive: following doses exceeding therapeutic levels (120 mcg), peak plasma concentrations are observed within 5 minutes after inhalation. When administered orally, a radiolabeled 80-mcg dose results in absorption of at least 65%, and oral doses up to 300 mcg are associated with rapid absorption, achieving peak concentrations of unchanged formoterol fumarate within 0.5–1 hour. In patients with chronic obstructive pulmonary disease (COPD) treated for 12 weeks with formoterol fumarate at doses of 12 or 24 mcg twice daily, plasma concentrations of formoterol ranged between 11.5–25.7 pmol/L and 23.3–50.3 pmol/L, respectively, measured 10 minutes, 2 hours, and 6 hours after inhalation.
Formoterol pharmacokinetics are linear over the dose range of 20 to 300 mcg. With repeated oral administration at doses of 40–160 mcg/day, no significant drug accumulation occurs. Maximum excretion rates after administration of 12–96 mcg are reached within 1–2 hours following inhalation.
After 12 weeks of treatment with 12 mcg or 24 mcg of formoterol powder twice daily, urinary excretion of unchanged formoterol increases by 63–73% in adults and by 18–84% in children, indicating moderate and self-limiting accumulation of formoterol in plasma following repeated dosing.
Measurement of total urinary excretion of formoterol and/or its (R,R)- and (S,S)-enantiomers after inhalation of dry powder (12–96 mcg) or aerosol formulations (12–96 mcg) demonstrated that absorption increases linearly with increasing dose.
Distribution. Plasma protein binding of formoterol ranges from 61–64%, primarily to albumin (34%). No saturation of binding sites occurs within the concentration range achieved with therapeutic doses.
Metabolism. Formoterol is primarily eliminated via metabolism. The main metabolic pathway is glucuronidation; another pathway is O-demethylation followed by glucuronidation. The transformation process is catalyzed by several CYP450 isoenzymes (2D6, 2C19, 2C9, and 2A6), resulting in a low potential for metabolic drug interactions. The pharmacokinetics of formoterol after single and repeated administration are similar, indicating no autoinduction or inhibition of its metabolism.
Elimination. Elimination of formoterol from systemic circulation is multiphasic. The apparent elimination half-life depends on the time interval considered. Based on plasma concentration data collected within 6, 8, or 12 hours after oral administration, the elimination half-life is approximately 2–3 hours. Based on urinary excretion rates measured between 3 and 16 hours after inhalation, the elimination half-life is calculated to be about 5 hours.
After inhalation, the plasma kinetics of formoterol and urinary excretion rates in healthy volunteers show biphasic elimination, with terminal half-lives of (R,R)- and (S,S)-enantiomers being 13.9 and 12.3 hours, respectively. Approximately 6.4–8% of the administered dose is excreted in urine as unchanged formoterol, with (R,R)- and (S,S)-enantiomers accounting for 40% and 60% of the unchanged drug, respectively.
Following a single oral dose of tritium-labeled formoterol, 59–62% of the dose is excreted in urine and 32–34% in feces. Renal clearance of formoterol is 150 mL/min.
In adult asthmatics, after multiple doses of 12 and 24 mcg, approximately 10% and 15–18% of the dose, respectively, is excreted in urine as unchanged and conjugated formoterol. In children, after multiple doses of 12 and 24 mcg, approximately 6% and 6.5–9% of the dose, respectively, is excreted in urine as unchanged and conjugated formoterol. In healthy volunteers, (R,R)- and (S,S)-enantiomers account for approximately 40% and 60%, respectively, of the unchanged drug excreted in urine in adults. No relative accumulation of one enantiomer over the other was observed after repeated dosing.
Clinical characteristics.
Indications.
Treatment of bronchial asthma in patients who are using inhaled corticosteroids or require treatment with long-acting β2-agonists.
For reduction of obstructive respiratory symptoms in patients with chronic obstructive pulmonary disease (COPD) who require treatment with long-acting β2-agonists.
Contraindications.
Hypersensitivity to formoterol fumarate or lactose monohydrate (contains a small amount of milk proteins). Hypersensitivity to other β2-adrenergic stimulants.
Tachyarrhythmia, third-degree atrioventricular block, idiopathic subvalvular aortic stenosis, hypertrophic obstructive cardiomyopathy, thyrotoxicosis.
Suspected or confirmed prolongation of the QT interval (QTc > 0.44 s).
Interaction with other medicinal products and other types of interactions.
Specific studies on the interaction of the medicinal product Formoterol Izihaler have not been conducted.
There is a theoretical risk that concomitant treatment with other medicinal products known to prolong the QTc interval may result in pharmacodynamic interaction with formoterol and increase the risk of ventricular arrhythmia. Examples of such medicinal products include certain antihistamines (e.g., terfenadine, astemizole, mizolastine), certain antiarrhythmic agents (e.g., quinidine, disopyramide, procainamide, erythromycin), and tricyclic antidepressants. Use of levodopa, levothyroxine, oxytocin, as well as alcohol consumption, may potentiate the cardiac side effects of β2-agonists.
Concomitant use with macrolides requires caution, as their effects on the cardiovascular system may be potentiated.
Concomitant use of other sympathomimetic agents, such as other β2-agonists or ephedrine, may enhance both desired and undesirable effects of Formoterol Izihaler. Therefore, dose titration may be required.
Concomitant treatment with xanthine derivatives, corticosteroids, or diuretics such as thiazides and loop diuretics may potentiate the potential hypokalemic adverse effect of β2-agonists.
Hypokalemia may increase susceptibility to cardiac arrhythmias in patients treated with cardiac glycosides—digitalis preparations.
The risk of developing arrhythmias is increased during anesthesia with halogenated hydrocarbon agents.
Formoterol may interact with monoamine oxidase inhibitors (MAOIs); therefore, it should not be administered to patients receiving MAOIs or within 14 days after discontinuation of such therapy.
Concomitant use of formoterol and corticosteroids may enhance the hyperglycemic effect observed with these medicinal products.
The bronchodilator effect of formoterol may be enhanced by anticholinergic agents.
β-adrenoblockers may attenuate and antagonize the effect of Formoterol Izihaler. Therefore, Formoterol Izihaler should not be used concomitantly with β-adrenoblockers (including ophthalmic drops), unless their use is essential.
Special precautions for use.
The dose of formoterol should be individually adjusted according to the patient's needs, using the lowest possible dose that provides therapeutic effect. The maximum recommended dose must not be exceeded (see "Dosage and administration").
Before prescribing formoterol, the patient's condition should be assessed to determine whether adequate anti-inflammatory treatment is being received. When symptoms of bronchial asthma are under control, the dose of formoterol should be gradually reduced. During dose reduction, the patient's condition should be regularly monitored.
Although formoterol may be added to the treatment regimen when inhaled corticosteroids do not provide sufficient control of bronchial asthma symptoms, formoterol therapy should not be initiated during severe asthma exacerbations or significant or acute worsening of asthma.
At the beginning of formoterol treatment, there is a risk of adverse effects related to bronchial asthma, as well as worsening of its course. If bronchial asthma symptoms remain uncontrolled or if the patient's condition deteriorates after formoterol inhalation, the patient should consult a physician regarding the appropriateness of continuing treatment.
Formoterol should not be used concomitantly with other long-acting β2-adrenergic agonists. During treatment of bronchial asthma, formoterol should be used only as an adjunctive medication, administered together with inhaled corticosteroids, in patients whose bronchial asthma is not adequately controlled by inhaled corticosteroids alone or in patients whose disease exacerbations warrant initiation of treatment with inhaled corticosteroids and a long-acting β2-adrenergic agonist.
For children aged 6 to 12 years, a combination product containing inhaled corticosteroids and a long-acting β2-adrenergic agonist is recommended, except in cases where separate administration of inhaled corticosteroids and a long-acting β2-adrenergic agonist is required.
Patients not receiving anti-inflammatory treatment should begin such therapy simultaneously with the initiation of formoterol. Patients should be advised to continue anti-inflammatory therapy after starting formoterol, even if improvement in condition is observed. Persistent symptoms or the need to increase the formoterol dose to control symptoms usually indicate worsening of the underlying disease and the need to reassess the treatment regimen.
If bronchial asthma symptoms improve, consideration may be given to gradually reducing the formoterol dose. It is important to regularly monitor patients during dose reduction. The lowest effective dose of formoterol should be used.
Fatalities have been reported with excessive use of medications containing β-adrenergic stimulants, although the exact cause of death is unknown. In several cases, death was due to cardiac arrest. Patients should be informed of the importance of strictly adhering to dosage recommendations and the inadmissibility of exceeding the maximum dose.
Formoterol Isihaler is not intended (and is insufficient) for use as primary therapy for bronchial asthma.
Patients with bronchial asthma requiring treatment with long-acting β2-agonists should also receive optimal maintenance anti-inflammatory therapy with corticosteroids. Patients should be advised to continue their anti-inflammatory therapy after starting Formoterol Isihaler, even if symptom intensity decreases. If symptoms persist or if treatment with β2-agonists needs to be intensified, this indicates worsening of the underlying disease and necessitates re-evaluation of maintenance therapy.
Although Formoterol Isihaler may be used as add-on therapy when inhaled corticosteroids do not provide adequate control of bronchial asthma symptoms, treatment with Formoterol Isihaler should not be initiated during severe exacerbations of bronchial asthma or significant or acute worsening or complications of asthma. Serious asthma-related adverse events and exacerbations may occur during treatment with Formoterol Isihaler. Patients should be informed of the need to continue treatment and to consult a physician if bronchial asthma symptoms are not controlled or worsen after starting Formoterol Isihaler. Once bronchial asthma symptoms are controlled, consideration should be given to gradually reducing the dose of Formoterol Isihaler. It is important to regularly monitor patients during dose reduction. The lowest effective dose of Formoterol Isihaler should be used.
Special caution and careful monitoring, particularly regarding maximum doses, are required in patients with the following conditions:
severe hypertension, severe heart failure, ischemic heart disease, cardiac arrhythmia, especially third-degree atrioventricular block, idiopathic subvalvular aortic stenosis, hypertrophic obstructive cardiomyopathy, thyrotoxicosis, pheochromocytoma, known or potential QTc interval prolongation (QTc > 0.44 s), concomitant use of medications affecting the QTc interval. Formoterol itself may cause QTc interval prolongation.
Caution is advised when theophylline and formoterol are used concomitantly in patients with heart disease.
Due to the hyperglycemic effect of β2-stimulants, additional monitoring of blood glucose concentration is recommended for diabetic patients at the beginning of treatment.
Life-threatening hypokalemia may develop during treatment with β2-agonists. Particular caution is recommended during severe exacerbations of bronchial asthma, as the associated risk increases under hypoxic conditions. The hypokalemic effect may be potentiated by concomitant treatment with other medications such as xanthine derivatives, steroids, and diuretics. In such cases, serum potassium levels should be monitored.
As with other forms of inhaled therapy, there is a risk of paradoxical bronchospasm. In such cases, wheezing and shortness of breath increase immediately after dosing; to relieve these symptoms, a rapid-acting inhaled bronchodilator must be used immediately. Inhalation of Formoterol Isihaler powder should be discontinued immediately, the patient evaluated, and alternative therapy prescribed if necessary.
Patients with rare hereditary conditions of galactose intolerance, lactase deficiency (Lapp syndrome), or glucose-galactose malabsorption should be aware that each dose of Formoterol Isihaler contains approximately 8 mg of lactose. This amount of lactose usually does not cause problems in individuals with lactose intolerance.
Use during pregnancy or breastfeeding.
Pregnancy
There are insufficient data on the use of formoterol in pregnant women. In animal studies, formoterol caused death of implanted embryos and reduced survival in the early postnatal period, as well as decreased birth weight. These effects were observed at significantly higher systemic exposure than that achieved with clinical use of formoterol. Formoterol treatment may be considered only if necessary for control of bronchial asthma and if no other safe alternative exists, taking into account that the expected benefit to the mother outweighs the risk to the fetus. The potential risk to humans is unknown.
Like other β2-adrenergic stimulants, formoterol may delay labor due to its relaxing effect on uterine smooth muscle.
Breastfeeding
It is unknown whether formoterol passes into breast milk. If treatment is necessary, a decision should be made whether to discontinue breastfeeding.
Ability to affect reaction speed when driving vehicles or operating machinery.
If dizziness, tremor, or seizures occur during treatment, driving vehicles or operating complex machinery should be avoided.
Method of Administration and Dosage
Route of administration – by inhalation.
Adults (including elderly patients) and children aged 12 years and older
Bronchial Asthma
Regular maintenance therapy: 1 inhalation (12 mcg) twice daily. In severe disease, this dosage regimen may be increased to 2 inhalations (24 mcg) twice daily.
Maximum daily dose is 4 inhalations (48 mcg) per day.
Chronic Obstructive Pulmonary Disease (COPD)
Regular maintenance therapy: 1 inhalation (12 mcg) twice daily.
Maximum daily dose is 2 inhalations (1 inhalation twice daily).
Children aged 6–12 years
Bronchial Asthma
Regular maintenance therapy: 1 inhalation (12 mcg) twice daily. Maximum daily dose is 24 mcg.
Renal or Hepatic Impairment
There are no data on the use of Formoterol Iciheiler in patients with impaired liver or kidney function. Since formoterol is primarily eliminated via hepatic metabolism, increased drug effects can be expected in patients with severe hepatic cirrhosis.
The duration of action of formoterol is approximately 12 hours. Treatment should always be initiated with the lowest effective dose.
Inhaled β2-agonists are required for maintenance bronchodilator therapy. In addition, short-acting β2-agonists are recommended for use during acute asthma attacks.
Long-acting β2-agonists may be added to the treatment regimen in patients whose symptoms of bronchial asthma are not adequately controlled with high doses of inhaled corticosteroids. Patients must be warned not to discontinue or alter their corticosteroid therapy when starting treatment with formoterol.
If symptoms persist or worsen, or if the recommended dose of Formoterol Iciheiler fails to control symptoms (provide effective relief), this often indicates worsening of the underlying disease.
When switching a patient to Formoterol Iciheiler from other inhalers, the treatment regimen should be individually tailored, taking into account previous therapy, dosing regimen, and method of administration.
Recommendations for Use
The "Iciheiler" is a flow-triggered inhaler, meaning the patient inhales through the mouthpiece, and the medication is delivered into the airways along with the inhaled air.





Important points to emphasize to the patient:
- Read the instructions for use carefully.
- If the package contains a protective container for the inhaler, after opening the laminated pouch, it is recommended to store the inhaler in the protective container to protect it from impact and ensure reliable device performance.
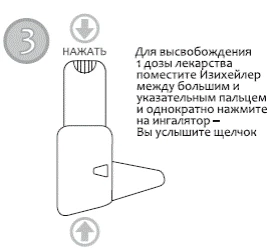
- Shake the device and activate it before each inhalation.
- Inhale through the mouthpiece sufficiently actively and deeply to ensure optimal delivery of the medication to the lungs.
- Do not exhale through the mouthpiece, as this will reduce the delivered dose. If this occurs, the patient should tap the inhaler gently on a hard surface or the palm of the hand to remove powder from the mouthpiece, then repeat the inhalation procedure.
- Do not activate the device more than once without inhaling the powder. If this occurs, the patient should tap the inhaler gently on a hard surface or the palm of the hand to remove powder from the mouthpiece, then repeat the inhalation procedure.
- Always replace the dust cap and close the protective container lid (if included in the package) after using the inhaler to prevent accidental dispersion of powder (which could lead to either overdose or insufficient medication delivery during the next use).
- Clean the mouthpiece regularly with a dry cloth. Do not use water for cleaning, as the powder is hygroscopic.
- Replace the Formoterol Iciheiler inhaler when the counter displays zero, even if some powder remains visible inside the device.
Children
Formoterol Iciheiler should not be prescribed to children under 6 years of age due to insufficient experience with the use of this medication in this patient group.
Overdose
Symptoms
Clinical experience with overdose treatment is limited. Overdose is likely to be associated with symptoms typically observed with β2-agonist overdose: tremor, headache, tachycardia. In individual cases, symptoms such as tachycardia, hyperglycemia, hypokalemia, prolonged QTc interval, arrhythmia, nausea, and vomiting have been reported.
Treatment
Supportive and symptomatic treatment is indicated. Hospitalization is required in severe cases.
The use of cardioselective beta-blockers may be considered, but with extreme caution, as β-adrenolytics may provoke bronchospasm. Serum potassium levels should be monitored.
Adverse Reactions
The most commonly reported adverse effects associated with β2-agonist therapy, such as tremor and tachycardia, are generally mild and tend to resolve within a few days of continued treatment.
The adverse reactions associated with formoterol are listed below by system organ class and frequency of occurrence. Frequency is defined according to the following scale: very common (>1/10), common (>1/100 to <1/10), uncommon (>1/1000 to <1/100), rare (>1/10,000 to <1/1000), very rare (<1/10,000), frequency not known (cannot be estimated from available data).
Immune System Disorders.
Rare: hypersensitivity reactions such as bronchospasm, severe hypotension, urticaria, angioedema, pruritus, exanthema, peripheral edema.
Very rare: allergic reactions, rash.
Metabolism and Nutrition Disorders.
Rare: hypokalemia.
Very rare: hyperkalemia, hyperglycemia.
Psychiatric Disorders.
Uncommon: feeling of anxiety, restlessness, sleep disturbances, feeling of fear.
Nervous System Disorders.
Common: headache, tremor.
Uncommon: excitement, anxiousness, nervousness, insomnia, convulsions, agitation.
Rare: dizziness, taste disturbance.
Cardiac Disorders.
Common: palpitations.
Uncommon: tachycardia, increased blood pressure (including arterial hypertension).
Rare: cardiac arrhythmias, e.g., atrial fibrillation, supraventricular tachycardia, supraventricular tachycardia, extrasystoles.
Very rare: angina pectoris, QTc interval prolongation, peripheral edema, arterial hypotension, blood pressure fluctuations.
Respiratory, Thoracic and Mediastinal Disorders.
Rare: increased bronchospasm, paradoxical bronchospasm, irritation of the mucous membranes of the mouth and pharynx.
Uncommon: cough, worsening of clinical condition.
Gastrointestinal Disorders.
Rare: nausea.
Musculoskeletal and Connective Tissue Disorders.
Uncommon: muscle cramps, myalgia.
Other.
Frequency not known: dry mouth, irritation of the conjunctiva, eyelid edema.
As with any other inhaled therapy, paradoxical bronchospasm occurs very rarely.
Treatment with β2-agonists may lead to increased plasma levels of insulin, free fatty acids, glycerol, and ketone bodies.
Lactose monohydrate contains small amounts of milk proteins and may therefore cause allergic reactions.
Shelf life. 2 years.
Storage period after opening of the package – 4 months.
Storage conditions.
Store in the original packaging prior to first use.
After opening the package, store at a temperature not exceeding 30°C in a dry place.
Packaging.
120 doses (12 μg/dose) in an inhaler with a protective cap in a laminated pouch.
1 laminated pouch in a cardboard box.
120 doses (12 μg/dose) in an inhaler with a protective cap in a laminated pouch.
1 laminated pouch and a protective container for the inhaler in a cardboard box.
Prescription status. Prescription only.
Manufacturer. Orion Corporation.
Manufacturer's address.
Orionintie 1, 02200 Espoo, Finland / Orionintie 1, 02200 Espoo, Finland.