Pharmasulin® h np
Ukraine
Table of Contents
INSTRUCTIONS FOR MEDICAL USE OF THE MEDICINAL PRODUCT FARMASULIN® H NP (FARMASULIN® H NP)
Composition:
Active substance: biosynthetic human insulin (recombinant DNA);
1 ml of suspension contains 100 IU of biosynthetic human insulin (recombinant DNA);
Excipients: metacresol; glycerin; liquefied phenol; protamine sulfate; disodium hydrogen phosphate heptahydrate (sodium phosphate dibasic, heptahydrate); zinc oxide; diluted hydrochloric acid or sodium hydroxide solution; water for injections.
Pharmaceutical form. Injection suspension.
Main physicochemical properties: white-colored suspension, which upon standing separates into a white sediment and a colorless or almost colorless supernatant liquid. The sediment readily resuspends upon shaking.
Pharmacotherapeutic group. Antidiabetic agents. Insulin preparations. Intermediate-acting insulin and analogues. ATC code A10AC01.
Pharmacological properties.
Pharmacodynamics.
Pharmasulin® H NP is an intermediate-acting insulin preparation.
The primary action of insulin is regulation of glucose metabolism. In addition, insulin affects various anabolic and anticatabolic processes in different tissues. In muscle tissues, these effects include enhanced synthesis of glycogen, fatty acids, glycerol, and protein, as well as increased amino acid uptake, accompanied by simultaneous suppression of glycogenolysis, gluconeogenesis, ketogenesis, lipolysis, protein catabolism, and amino acid release.
The typical insulin activity profile (glucose utilization curve) following subcutaneous injection is shown below by the bold line. The possible variability in duration and/or intensity of insulin activity among different patients is illustrated by the shaded area on the graph. Individual variability depends on factors such as dose volume, temperature at the injection site, and the patient's level of physical activity.
| Insulin activity |
|
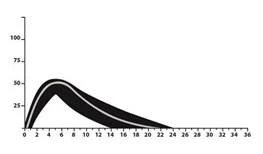
Time (hours)
Pharmacokinetics.
Pharmasulin® H NP is human insulin produced using recombinant DNA technology.
The pharmacokinetics of insulin does not reflect the metabolic activity of the hormone. Therefore, when considering insulin activity, studying glucose utilization curves (shown above) is more appropriate.
Toxicological studies did not reveal any serious adverse effects associated with the use of the drug.
Clinical characteristics.
Indications.
Treatment of patients with diabetes mellitus who require insulin administration to maintain normal glucose homeostasis.
Contraindications.
Hypoglycemia. Hypersensitivity to the active substance or to any of the excipients of the medicinal product, except in cases where desensitization therapy is applied. Intravenous administration is contraindicated.
Interaction with other medicinal products and other forms of interaction.
Some medicinal products affect glucose metabolism; therefore, consultation with a physician is recommended regarding the concomitant use of any other medicinal products with human insulin. The physician should consider possible interactions if the patient is taking any medicinal products.
Insulin requirement may increase when using medicinal products with hyperglycemic activity, such as glucocorticoids, thyroid hormones and growth hormone, danazol, β2-sympathomimetics (e.g. ritodrine, salbutamol, terbutaline), thiazides.
Insulin requirement may decrease when using medicinal products with hypoglycemic activity, such as oral hypoglycemic agents, salicylates (e.g. acetylsalicylic acid), certain antidepressants (monoamine oxidase inhibitors), certain angiotensin-converting enzyme inhibitors (captopril, enalapril), angiotensin II receptor blockers, non-selective β-blockers, or alcohol.
Somatostatin analogues (octreotide, lanreotide) may either increase or decrease insulin requirement.
Special precautions for use
Patients should be advised to regularly rotate injection sites to reduce the risk of lipodystrophy and cutaneous amyloidosis. There is a potential risk of delayed insulin absorption and impaired glycemic control following insulin injections into areas affected by such reactions. It has been reported that changing the injection site to an unaffected area of skin may lead to hypoglycemia. It is recommended to monitor blood glucose levels after changing the injection site, and dose adjustment of antidiabetic medications may be considered.
Any substitution of insulin type or brand must be carried out under close medical supervision. Changes in concentration, brand (manufacturer), type (regular, NPH, mixed), species (animal-sourced insulin, human insulin, human insulin analog), and/or method of production (recombinant DNA insulin or animal-sourced insulin) may require dosage adjustment.
Dosage when treating patients with human insulin may differ from that used with animal-sourced insulin. Dose adjustments may be required starting with the first dose or during the first several weeks or months of treatment.
In some patients who experienced hypoglycemic reactions after switching from animal-sourced insulin to human insulin, early warning symptoms of hypoglycemia were less pronounced or different from those previously observed during treatment with animal insulin. Patients who achieve significantly improved blood glucose levels (e.g., due to intensified insulin therapy) may no longer experience some or any of the early warning symptoms of hypoglycemia, and they should be informed accordingly. Conditions in which early warning symptoms of hypoglycemia may be less specific or less pronounced include long-standing diabetes, diabetic neuropathy, or concomitant use of medications such as β-adrenergic blockers.
Untreated hypoglycemic or hyperglycemic reactions may lead to loss of consciousness, coma, or fatal outcomes.
Use of incorrect doses or abrupt discontinuation of treatment, especially in insulin-dependent diabetes, may lead to hyperglycemia and ketoacidosis—conditions that are potentially life-threatening.
Antibody formation may occur during treatment with human insulin, although usually to a lesser extent than with purified animal-sourced insulin.
Insulin requirements may change significantly in adrenal, pituitary, or thyroid gland disorders, as well as in the presence of renal or hepatic insufficiency.
Insulin requirements may also increase during illness or emotional stress.
Dose adjustments may be necessary when there are changes in the intensity of physical activity or usual dietary patterns.
This medicinal product contains no more than 29 mmol/L (100 IU) of sodium. Caution is advised when administering to patients on a sodium-restricted diet.
Combination with pioglitazone
Cases of heart failure have been reported with concomitant use of pioglitazone and insulin, particularly in patients with risk factors for heart failure. This information should be considered when prescribing the combination of Pharmasulin® H NP with pioglitazone. When using this combination, patients should be monitored for signs and symptoms of heart failure, weight gain, and edema. Treatment with pioglitazone should be discontinued if cardiac symptoms worsen.
Use during pregnancy or breastfeeding
Patients with insulin-dependent diabetes mellitus or gestational diabetes receiving insulin therapy require careful monitoring throughout pregnancy. Insulin requirements typically decrease during the first trimester and then increase during the second and third trimesters. Patients with diabetes should inform their physician as soon as pregnancy is confirmed or planned.
During pregnancy, patients with diabetes require careful monitoring of blood glucose levels and overall health status.
Breastfeeding women with diabetes may require adjustments in insulin dosage and/or dietary regimen.
Ability to affect reaction speed when driving or operating machinery
The ability of insulin-treated patients to concentrate and react may be impaired as a result of hypoglycemia. This may represent a risk factor when such abilities are of particular importance (e.g., when driving a vehicle or operating machinery).
Patients should be informed about the necessary preventive measures to avoid hypoglycemia while driving. This is especially important for patients with reduced or absent awareness of hypoglycemic warning symptoms or those who frequently experience episodes of hypoglycemia. In such cases, the appropriateness of driving should be evaluated.
Method of Administration and Dosage.
The dose is determined by a physician according to the individual needs of the patient.
Pharmasulin® H NP must be administered only by subcutaneous injection, using either a reusable insulin pen device for cartridges or insulin syringes—for vials.
Pharmasulin® H NP must not be administered intravenously.
Subcutaneous injections should be administered into the abdominal wall, thigh, buttocks, or upper arm. Injection sites should be rotated to avoid using the same site more than once per month, in order to reduce the risk of developing lipodystrophy or cutaneous amyloidosis (see sections "Special Warnings" and "Adverse Reactions").
Care must be taken during injection of Pharmasulin® H NP to avoid intravascular injection. The injection site must not be massaged after administration. Patients must be trained in the correct injection technique.
- Instructions for Use of the Medicinal Product.
Cartridges.
Each pen/cartridge must be used by only one patient, even if the needle is changed, to prevent the possible transmission of infectious diseases.
The 3 mL suspension for injection in cartridges must be used with an insulin pen device marked with the "CE" symbol, in accordance with the manufacturer's recommendations.
Immediately before use, Pharmasulin® H NP in cartridges must be resuspended by rolling the cartridge between the palms 10 times and inverting it 180° 10 times until the suspension becomes uniformly cloudy or milky. If the liquid in the cartridge does not achieve the proper appearance, the procedure should be repeated until the contents are fully resuspended. Cartridges contain a small glass ball to facilitate mixing. Cartridges must not be shaken vigorously, as this may cause foaming, which can interfere with accurate dose measurement.
The appearance of the cartridge contents should be regularly checked. Do not use if the suspension contains clumps or if white particles adhere to the bottom or sides of the cartridge, making the glass appear frosted.
Cartridges are not intended for mixing different insulins. Empty cartridges must not be reused.
For instructions on loading the cartridge into the insulin pen, attaching the needle, and administering the insulin injection, refer to the manufacturer's instructions for the insulin pen device.
Each time a new insulin pen is used, the instructions for use should be carefully read, as they may contain updated information. This information does not replace the necessity of discussing the patient's health status and prescribed treatment with a physician.
Use of the insulin pen is not recommended for patients with complete vision loss or impaired vision unless they are assisted by individuals trained in the proper use of the pen.
Vials.
The appearance of the vial contents should be regularly checked. Do not use the product if, after shaking, the suspension contains flakes or if white particles adhere to the bottom or sides of the vial, creating a frost-like appearance.
Use a syringe with markings corresponding to the insulin dose prescribed by the physician. It is essential to use syringes of the same type and brand. Inattention when using syringes may lead to incorrect insulin dosing.
Preparation of the Dose.
- Immediately before injection, gently roll the vial of insulin suspension between the palms to achieve a uniform cloudy appearance throughout the vial. Do not shake the vial vigorously, as this may cause foaming, which can interfere with accurate dose measurement.
- Draw up the insulin from the vial by inserting a sterile needle through the rubber stopper, previously cleaned with alcohol. The insulin should be at room temperature when administered.
- Draw air into the syringe up to the mark corresponding to the required insulin dose, then inject this air into the vial.
- Invert the syringe and vial together so that the vial is upside down, and draw up the required dose of insulin.
- Remove the needle from the vial. Expel air from the syringe and verify the correct insulin dose has been drawn.
Aseptic technique must be followed during injection. To avoid infectious complications, single-use syringes must not be reused.
Separate syringes must be used for administering Pharmasulin® H and Pharmasulin® H NP.
- Administration of the Medicinal Product.
Administer the prescribed insulin dose as directed by the physician.
Injections should be given into different body areas, ensuring that the same site is not used more than once per month.
Children.
Dosage, administration schedule, and number of injections for children are determined by a physician based on individual needs and specific circumstances.
Overdose.
There is no specific definition for insulin overdose, as blood glucose levels result from a complex interaction between insulin levels, glucose intake, and other metabolic processes. Hypoglycemia may result from an excess of insulin relative to food intake and energy expenditure.
Symptoms of hypoglycemia include lethargy, confusion, tachycardia, headache, sweating, and vomiting.
Mild hypoglycemia is usually treated by oral administration of glucose or sugar-containing products. Moderate to severe hypoglycemia may be managed by intramuscular or subcutaneous administration of glucagon, followed by oral carbohydrate intake once the patient's condition stabilizes. In patients who do not respond to glucagon, intravenous glucose solution must be administered. If the patient is comatose, glucagon should be given intramuscularly or subcutaneously. In the absence of glucagon or if there is no response to glucagon, intravenous glucose solution must be administered. The patient should be fed as soon as consciousness is regained.
Continued carbohydrate intake and medical monitoring may be necessary, as recurrence of hypoglycemia may occur after apparent clinical improvement.
Adverse Reactions
Hypoglycemia is the most common adverse effect of insulin therapy in patients with diabetes mellitus. Severe hypoglycemia may lead to loss of consciousness and, in extreme cases, to fatal outcome. The exact frequency of hypoglycemic episodes cannot be established, as it results from the combined influence of insulin dose and other factors such as the patient's diet and level of physical activity.
Local allergic reactions are common (frequency from 1/100 to < 1/10) and include injection site reactions such as erythema, swelling, and pruritus. These reactions usually resolve within a few days to several weeks. In some cases, such reactions may not be related to insulin itself but rather to other factors, for example, irritant substances in skin cleansing agents or improper injection technique.
Systemic allergic reaction is very rare (< 1/10,000), but potentially more serious and represents a generalized allergic reaction to insulin. It may manifest as generalized rash, dyspnea, wheezing, hypotension, tachycardia, and increased sweating. Severe cases of generalized allergy can be life-threatening. In exceptional cases of severe allergy to Pharmasulin® H NP, appropriate measures must be taken immediately. Insulin substitution or desensitization therapy may be required.
Lipodystrophy at the injection site occurs uncommonly (frequency from 1/1000 to < 1/100).
Skin and subcutaneous tissue disorders of unknown frequency – skin amyloidosis.
Disorders of the skin and subcutaneous tissue – lipodystrophy and skin amyloidosis – may occur at the injection site and may delay local absorption of insulin. Regular rotation of injection sites within the same injection area may help reduce or prevent these reactions (see section "Special Instructions").
Cases of edema during insulin therapy have been reported, particularly when intensive insulin therapy improves previously poor metabolic control.
Reporting of suspected adverse reactions
Reporting of adverse reactions after marketing authorization is of great importance. It allows continued monitoring of the benefit-risk balance of the medicinal product. Medical and pharmaceutical professionals, as well as patients or their legal representatives, should report all suspected adverse reactions and lack of efficacy through the Automated Pharmacovigilance Information System at the following link: https://aisf.dec.gov.ua.
Shelf life
2 years.
The shelf life of the product in cartridges and vials after first opening is 28 days at a temperature from 15 °C to 25 °C, protected from overheating and direct sunlight. Cartridges in use should not be stored in the refrigerator.
Do not use the medicinal product after the expiry date stated on the packaging.
Storage conditions
Store in the original packaging at a temperature from 2 °C to 8 °C (in the refrigerator). Do not freeze.
Keep out of the reach and sight of children.
Incompatibilities
Pharmasulin® H NP must not be mixed with insulins from other manufacturers or with animal-sourced insulins.
Packaging
3 mL in a cartridge. 5 cartridges in a blister pack. 1 blister pack in a carton.
5 mL or 10 mL in vials. 1 vial in a carton.
Prescription status By prescription only.
Manufacturer JSC "Farmak".
Address of manufacturer and location of manufacturing site
74 Kyrylivska Street, Kyiv, 04080, Ukraine.