Eligard 45 mg
Ukraine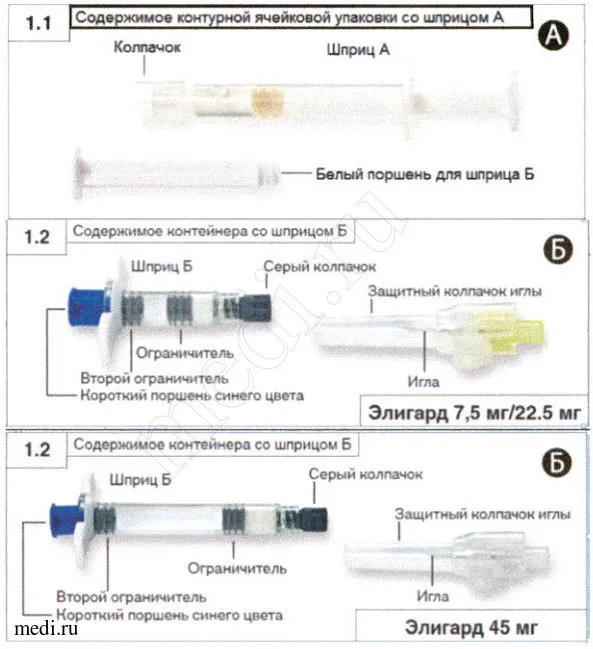
Table of Contents
INSTRUCTIONS FOR MEDICAL USE OF THE MEDICINAL PRODUCT ELIGARD 45 mg (ELIGARD® 45 mg)
Composition:
Active substance: leuprolide;
Prefilled syringe B contains: reconstituted amount of leuprolide acetate 45 mg (equivalent to leuprolide 41.7 mg);
Excipients: prefilled syringe A contains solvent (poly(DL-lactide-co-glycolide) polymer, N-methyl-2-pyrrolidone) 436 mg.
Pharmaceutical form. Powder for solution for subcutaneous injection, 45 mg, in a set with solvent.
Main physicochemical properties: prefilled syringe B – white or almost white powder, without signs of melting, free from visible foreign particles;
prefilled syringe A – solvent: clear, viscous liquid, colorless to light yellow; may contain air bubbles, but free from visible particles and mechanical inclusions.
Pharmacotherapeutic group. Gonadotropin-releasing hormone analogs. Leuprolide.
ATC code L02A E02.
Pharmacological Properties
Pharmacodynamics
Leuprolide acetate is a synthetic nonapeptide analogue of the natural gonadotropin-releasing hormone (GnRH). With prolonged administration, it inhibits pituitary gonadotropin secretion and suppresses testicular steroidogenesis in men. This effect is reversible upon discontinuation of treatment with the medicinal product. The analogue is more potent than the natural hormone, and its effects are reversible after cessation of therapy.
Administration of leuprolide acetate initially causes an increase in circulating levels of luteinizing hormone (LH) and follicle-stimulating hormone (FSH), resulting in a temporary rise in gonadal steroid levels, testosterone and dihydrotestosterone in men. With prolonged administration of leuprolide acetate, levels of LH and FSH decrease. In men, testosterone levels decline to castrate levels (≤ 50 ng/dL). This occurs within 3–4 weeks after initiation of treatment.
The mean testosterone level after 6 months of treatment with leuprolide acetate 45 mg is 10.4 (±0.53) ng/dL, which is comparable to the level achieved after bilateral orchidectomy. In all patients except one participating in the main clinical study receiving leuprolide acetate 45 mg, castrate levels were achieved within 4 weeks. In most patients, testosterone levels were below 20 ng/dL. Prostate-specific antigen (PSA) levels decreased by 97% at a dose of 45 mg over 6 months.
Long-term studies have shown that with prolonged treatment, testosterone levels remain below castrate levels for up to 7 years and even throughout the remainder of life.
Pharmacokinetics
Absorption: In patients with advanced prostate cancer, after administration of leuprolide acetate 45 mg, serum concentration increased to 82 ng/dL at 4.4 hours (Cmax). Following the initial peak after each injection, serum levels remained relatively stable during the plateau phase (from day 3 to day 168 after administration of leuprolide acetate 45 mg), ranging between 0.2–2.0 ng/mL for leuprolide acetate 45 mg. Data on accumulation of the substance with repeated injections are not available.
Distribution: The mean volume of distribution of leuprolide after intravenous administration in healthy male volunteers was 27 liters. In vitro plasma protein binding in humans for leuprolide acetate 45 mg ranges from 43% to 49%.
Elimination: After intravenous administration of 1 mg leuprolide acetate to healthy volunteers, the mean clearance was 8.34 L/h, with a terminal half-life of approximately 3 hours.
No studies on the elimination of the Eligarde 45 mg formulation have been conducted.
No studies on the metabolism of the Eligarde 45 mg formulation have been conducted.
Clinical characteristics.
Indications.
Treatment of hormone-dependent advanced prostate cancer and treatment of high-risk localized prostate cancer and locally advanced prostate cancer in combination with radiation therapy.
Contraindications.
Hypersensitivity to leuprorelin acetate, other gonadotropin-releasing hormone (GnRH) agonists, or to any of the excipients.
Patients who have previously undergone orchidectomy (like other GnRH agonists, Eligard 45 mg does not cause further reduction in serum testosterone levels following surgical castration).
As monotherapy in patients with prostate cancer and spinal cord compression or significant spinal metastases (see section "Special precautions").
Eligard 45 mg is contraindicated in women and children.
Interaction with other medicinal products and other forms of interaction.
No studies on the pharmacokinetic interaction of Eligard 45 mg with other drugs have been conducted. There are no reports on interactions between leuprorelin acetate and other medicinal products.
Since androgen deprivation therapy may prolong the QT interval, concomitant use of Eligard 45 mg with medicinal products that prolong the QT interval or that may induce torsades de pointes, such as Class I antiarrhythmics (e.g., quinidine, disopyramide) or Class III antiarrhythmics (e.g., amiodarone, sotalol, dofetilide, ibutilide), methadone, moxifloxacin, and neuroleptics, should be carefully evaluated (see section "Special precautions").
Special precautions for use.
Proper reconstitution. Incorrect preparation of the injection solution may result in lack of efficacy (see section "Instructions for use, handling and disposal"). In case of suspected or known administration errors, testosterone levels in blood should be assessed.
Androgen deprivation therapy may prolong the QT interval.
In patients with a history of risk factors for QT interval prolongation, and in patients concurrently receiving medicinal products that may prolong the QT interval (see section "Interaction with other medicinal products and other forms of interaction"), physicians must evaluate the benefit-risk ratio before initiating treatment with Eligard 45 mg, including the potential risk of torsades de pointes.
Cardiovascular diseases. With GnRH agonist therapy in men, an increased risk of myocardial infarction, sudden cardiac death, or stroke has been reported. Although this risk is relatively low, cardiovascular risk factors should be carefully evaluated before initiating treatment in patients with prostate cancer. Patients receiving GnRH agonists should be monitored for symptoms and signs suggestive of cardiovascular disease and managed according to current clinical practice.
Idiopathic intracranial hypertension. Idiopathic intracranial hypertension (pseudotumor cerebri) has been reported in patients receiving leuprolide. Patients should be informed about the signs and symptoms of idiopathic intracranial hypertension, including severe or recurring headache, visual disturbances, and tinnitus. If idiopathic intracranial hypertension occurs, discontinuation of leuprolide should be considered.
Severe skin adverse reactions. Severe skin adverse reactions (SCARs), including Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN), which may be life-threatening or fatal, have been reported in patients receiving leuprolide. Patients should be informed about the signs and symptoms and closely monitored for serious skin reactions. If signs or symptoms suggestive of these reactions occur, leuprolide should be discontinued immediately and alternative treatment considered (if necessary).
Transient increase in testosterone concentration. Leuprolide acetate, like other GnRH agonists, causes a transient increase in serum testosterone, dihydrotestosterone, and acid phosphatase concentrations during the first week of treatment. This may exacerbate existing symptoms or lead to new symptoms, including bone pain, neuropathy, hematuria, ureteral obstruction, or intravesical obstruction (see section "Undesirable effects"). These symptoms usually resolve with continued treatment.
Concomitant administration of an appropriate antiandrogen should be initiated three days before starting leuprolide therapy and continued for the first two to three weeks of treatment to prevent the consequences of the initial rise in serum testosterone levels.
After surgical castration, Eligard 45 mg does not cause further reduction in serum testosterone levels in male patients.
Bone mineral density. Decreased bone mineral density has been reported in men undergoing orchiectomy or receiving GnRH agonist therapy (see section "Undesirable effects").
Antiandrogen therapy significantly increases the risk of fracture due to osteoporosis. Limited data are available on this issue. Fractures due to osteoporosis occurred in 5% of patients after 22 months of pharmacological androgen deprivation therapy and in 4% of patients after 5–10 years of treatment. The risk of fractures due to osteoporosis is generally higher than the risk of pathological fractures.
In addition to prolonged testosterone deficiency, osteoporosis development may be influenced by advanced age, smoking, alcohol consumption, obesity, and insufficient physical activity.
Pituitary haemorrhage. During post-marketing surveillance following administration of GnRH agonists, cases of pituitary haemorrhage (the second most common clinical syndrome after pituitary infarction) have been rarely reported, mostly within two weeks after the first dose, and in some cases within the first hour. In these cases, pituitary haemorrhage caused sudden severe headache, vomiting, visual deterioration, ophthalmoplegia, mental status changes, and sometimes cardiovascular collapse. Emergency medical intervention is required.
Metabolic changes. Hyperglycaemia and an increased risk of developing diabetes have been reported in some patients receiving GnRH agonist therapy. Hyperglycaemia may indicate the onset of diabetes mellitus or worsening glycaemic control in diabetic patients. Patients receiving GnRH agonists should be monitored periodically for blood glucose and/or glycated haemoglobin (HbA1c) levels, and hyperglycaemia or diabetes should be managed according to current clinical practice.
Metabolic changes associated with GnRH agonists may also include hepatic steatosis.
Seizures. Post-marketing reports have documented seizures in patients receiving leuprolide acetate, with or without pre-existing risk factors for seizures. If seizures occur, treatment should be initiated according to current clinical practice.
Other events. With the use of GnRH agonists, cases of ureteral obstruction and spinal cord compression have been reported, which may lead to paralysis, with or without fatal outcomes. Standard treatment for these complications should be initiated promptly if spinal cord compression or renal failure occurs.
Close monitoring is recommended during the first few weeks of treatment in patients with metastases to the spine and/or brain, as well as in patients with urinary tract obstruction.
Use during pregnancy or breastfeeding.
Data are lacking. Eligard 45 mg is contraindicated in women.
Ability to affect reaction speed when driving or operating machinery.
No studies on the effect of Eligard 45 mg on the ability to drive or operate machinery have been conducted.
The ability to drive or operate machinery may be impaired due to fatigue, dizziness, and visual disturbances—these are possible adverse effects of treatment or consequences of the underlying disease.
Administration and Dosage
Eligard 45 mg must be administered under the supervision of a healthcare professional experienced in evaluating the response to treatment.
Eligard 45 mg should be given as a subcutaneous injection once every 6 months. The injected solution forms a depot that ensures continuous release of leuprolide acetate over a period of 6 months.
Generally, treatment of hormone-dependent advanced prostate cancer with Eligard 45 mg is intended as long-term therapy, and should not be discontinued after improvement or remission occurs.
Eligard 45 mg should be used as part of neoadjuvant or adjuvant therapy in combination with radiation therapy for the treatment of high-risk localized prostate cancer and locally advanced prostate cancer.
Response to treatment with Eligard 45 mg should be monitored by observing clinical symptoms of the disease and measuring serum prostate-specific antigen (PSA) levels.
Clinical studies have shown that in most patients without orchidectomy, testosterone levels increase during the first three days of treatment, then decrease over 3–4 weeks to below medical castration levels. Castration levels of testosterone are maintained during long-term use of the drug (testosterone levels <1% are achieved). If the patient's response to treatment is inadequate, it is recommended to verify whether castration-level testosterone has been achieved and maintained.
Inadequate preparation of the injectable solution or incorrect administration of the drug may result in lack of therapeutic efficacy. In cases of suspected or confirmed incorrect administration, testosterone levels should be assessed (see section "Special Warnings and Precautions for Use").
In patients with metastatic castration-resistant prostate cancer who have not undergone surgical castration and who are receiving GnRH agonists such as leuprolide, and who have no contraindications to treatment with androgen biosynthesis inhibitors or androgen receptor inhibitors, GnRH agonist therapy may be continued.
Administration. Eligard 45 mg is prepared and administered only by healthcare professionals experienced in its use.
The contents of two pre-filled sterile syringes should be mixed immediately prior to administration of Eligard 45 mg as a subcutaneous injection.
The mixing procedure is described below in the section "Instructions for Use and Handling of Syringes".
Accidental intravascular (arterial or venous) injection must be strictly avoided.
As with other subcutaneously administered drugs, the injection site for Eligard 45 mg should be rotated regularly.
Dose Adjustment in Special Patient Populations
Clinical studies in patients with hepatic or renal impairment have not been conducted.
Instructions for Use and Handling of Syringes
Prior to use, allow the medicinal product to stand at room temperature for 30 minutes.
The patient should be prepared for injection first, followed by preparation of the medicinal product according to the instructions below.
Incorrect preparation of the subcutaneous injection solution may result in lack of therapeutic efficacy.
Step 1. Open the tray by pulling the free end of the aluminum foil. Remove the desiccant. Place the pre-connected syringe system on a clean working surface (Fig. 1.1). Open the needle guard by peeling off the paper protective label (Fig. 1.2). Note: Syringe A and Syringe B should not be aligned in a straight line.
|
| Step 2. Using the index and thumb fingers, grasp the connector button and press until a distinct click is heard (Fig. 2). The syringes must be kept in a horizontal position. Do not tilt the syringes (note that this may cause leakage of liquid, as the syringes may partially unscrew). |
Fig. 2 |
| Step 3. Thoroughly mix the medication by holding the syringe system in a horizontal position and alternately pressing the plunger of syringe A and syringe B a total of 60 times (1 cycle is one press of syringe A followed by one press of syringe B) until a homogeneous viscous solution is obtained (Fig. 3). Do not tilt the syringes (note that this may cause leakage, as the syringes may partially unscrew). |
Fig. 3 |
After thorough mixing, a viscous solution ranging from colorless to light yellow is obtained (shades of white or light yellow may be observed).
Important: The solution must be used immediately after preparation, as its viscosity increases over time. Do not freeze the prepared medicinal product.
Note that the medicinal product must be mixed exactly as described above; shaking does not ensure adequate mixing of the medicinal product.
| Step 4. After mixing, hold the syringes vertically (syringe A above syringe B). The syringes must remain securely connected. By pushing the plunger of syringe A and slightly pulling the plunger of syringe B, transfer the entire mixture into syringe B (short wide syringe) (Fig. 4). |
Fig. 4 |
| Step 5. After confirming that the plunger of syringe A is fully depressed, unscrew it from syringe B by holding the connector. Syringe A remains attached to the connector (Fig. 5). Ensure that the medicinal product does not leak, as the attached needle will no longer provide leak protection. Note. One large or several small air bubbles may appear. This is a normal phenomenon and does not affect depot formation after administration. Please do not attempt to remove air bubbles from syringe B at this stage, as this may result in loss of some of the medicinal product. |
Fig. 5 |
| Step 6.
Important: Do not overtighten the needle, as this may crack the needle hub, leading to leakage of the medicinal product during injection. If the needle hub is cracked, shows visible signs of damage, or leakage has occurred, the medicinal product must not be used. Replacing a damaged needle with an identical one is not permitted; the product must not be administered if the needle is damaged. The entire medicinal product should be safely disposed of. If the needle hub is damaged, another package of the medicinal product must be used. |
Fig. 6 |
| Step 7. Move the protective device away from the needle and, prior to administering the medication, remove the needle cap (Fig. 7). Important: do not activate the needle safety device before administering the medication. If the needle hub is damaged or leaking, do not replace the damaged needle, and do not use the medication. In case of damage to the needle hub, a new medication kit should be used. |
Fig. 7 |
| Step 8. Before injection, remove large air bubbles from syringe B. Inject the medicinal product subcutaneously, holding the safety device parallel and away from the needle. Injection procedure:
|
Fig. 8.1 Fig. 8.2 |
Step 9. Immediately activate the needle safety cap after injection, using either of the two methods described below.
| Method 1. Closing on a flat surface. Place the syringe with the needle on a flat surface with the lever of the safety device facing down and activate the safety mechanism by pressing the lever (Fig. 9.1). Ensure that the lever is moved into the closed position and the needle tip is completely covered (until a distinct click is heard). |
Fig. 9.1 |
| Method 2. Closing with the thumb. Place your thumb on the safety device (Fig. 9.2), cover the needle tip and activate the safety mechanism. Ensure that the lever is moved into the closed position and the needle tip is completely covered (until a distinct click is heard). After closing the safety mechanism, immediately place the needle and syringe into an appropriate sharps container. |
Fig. 9.2 |
Children. The safety and efficacy of the drug in children have not been evaluated, as it is not used in pediatric practice.
Overdose. There have been no cases of overdose with the drug Eligard 45 mg in clinical practice.
In the event of overdose, the patient should be monitored and appropriate symptomatic treatment should be administered if necessary.
Adverse reactions
Adverse effects observed with administration of the medicinal product Eligard 45 mg are mainly due to the specific pharmacological action of leuprorelin—fluctuations in levels of certain hormones. The most commonly reported adverse reactions include hot flashes, nausea, malaise, fatigue, and transient local irritation at the injection site. Mild or moderate hot flashes occur in approximately 58% of patients.
The adverse reactions listed below were observed during clinical studies of Eligard 45 mg in patients with advanced prostate cancer. Adverse reactions are classified according to frequency of occurrence: very common (≥ 1/10), common (≥ 1/100, < 1/10), uncommon (≥ 1/1000, < 1/100), rare (≥ 1/10,000, < 1/1000), very rare (< 1/10,000), and not known (cannot be estimated from the available data).
| Adverse reactions in clinical trials of the drug |
|
| Infections and infestations common uncommon |
nasopharyngitis urinary tract infection, local skin infections |
| Metabolism and nutrition disorders uncommon |
exacerbation of diabetes mellitus |
| Psychiatric disorders uncommon |
abnormal dreams, depression, decreased libido |
| Nervous system disorders uncommon rare |
dizziness, headache, hypaesthesia, insomnia, taste disorders and smell disorders, vertigo abnormal involuntary movements |
| unknown |
idiopathic intracranial hypertension (pseudotumor cerebri) [see section "Special precautions"] |
| Cardiac disorders unknown |
QT interval prolongation (see sections "Special precautions", "Interaction with other medicinal products and other forms of interactions") |
| Vascular disorders very common uncommon rare |
hot flushes increased blood pressure, decreased blood pressure fainting, collapse |
| Respiratory, thoracic and mediastinal disorders uncommon unknown |
rhinorrhea, dyspnea interstitial lung disease |
| Gastrointestinal disorders common uncommon rare |
nausea, diarrhea, gastroenteritis/colitis constipation, dry mouth, dyspepsia, vomiting flatulence, belching |
| Skin and subcutaneous tissue disorders very common common uncommon rare unknown |
bruising, erythema itching, night sweats clammy sweat, increased sweating alopecia, skin rash Stevens-Johnson syndrome/toxic epidermal necrolysis (SJS/TEN), (see section "Special precautions"), toxic skin eruptions, erythema multiforme |
| Musculoskeletal and connective tissue disorders, bone common uncommon |
arthralgia, limb pain, muscle pain, tremor, weakness back pain, muscle spasms |
| Renal and urinary disorders common uncommon |
urination frequency disturbance, difficulty in urination, dysuria, nocturia, oliguria bladder spasm, blood in urine, increased frequency of urination, urinary retention |
| Reproductive system and breast disorders common uncommon very rare |
breast tenderness, testicular atrophy, testicular pain, infertility, gynecomastia, erectile dysfunction, reduction in penis size gynecomastia, impotence, testicular disorders breast pain |
| General disorders very common common uncommon rare very rare |
fatigue, burning sensation at injection site, paraesthesia at injection site malaise, pain, bruising and stinging at injection site itching at injection site, induration at injection site, lethargy, pain, increased temperature ulcer at injection site injection site necrosis |
| Blood and lymphatic system disorders common |
changes in complete blood count, anemia |
| Investigations common uncommon |
increased blood creatine phosphokinase, prolonged blood coagulation time increased alanine aminotransferase, increased blood triglycerides, prolonged prothrombin time, increased body weight |
Other adverse effects generally observed during treatment with leuprorelin acetate include peripheral edema, pulmonary embolism, tachycardia, muscle pain, muscle weakness, altered skin sensation, chills, rash, amnesia, and visual disturbances. With prolonged use of this class of drugs, muscle atrophy has been reported. Rare cases of pituitary infarction, previously occurred, have been reported after administration of GnRH agonists. Thrombocytopenia and leukopenia have also been rarely reported. Changes in glucose tolerance have been reported.
Seizures have been observed following administration of GnRH agonist analogs (see section "Special precautions").
Local adverse reactions occurring after administration of Eligard 45 mg are similar to local reactions associated with other subcutaneously administered drugs.
Generally, these local adverse reactions occurring after subcutaneous injections are mild and transient.
Anaphylactic/anaphylactoid reactions have been reported following administration of GnRH agonist analogs.
Bone density changes
Reduced bone density has been reported in the medical literature in men who have undergone orchidectomy or who have been treated with GnRH analogs. Prolonged treatment with leuprorelin may likely lead to increased symptoms of osteoporosis. Increased risk of fractures – a consequence of osteoporosis – should be considered (see section "Special precautions").
Worsening of disease signs and symptoms
Treatment with leuprorelin may cause a temporary worsening of disease signs and symptoms during the first few weeks. Metastases to the spine and/or urinary tract obstruction or hematuria, neurological disorders such as weakness and/or paresthesia of the lower limbs, or worsening urinary symptoms may occur.
Shelf life. 2 years.
After removal from the refrigerator, the product may be stored in the original packaging at room temperature (not exceeding 25 °C) for up to 4 weeks.
After first opening of the vials, the powder and solvent for injection solution must be mixed immediately and administered to the patient.
After mixing: administration should be performed immediately, as the viscosity of the solution continuously increases.
Storage conditions.
Store in the original packaging at 2–8 °C. Before administration, the medicinal product should be kept at room temperature. After removal from the refrigerator, it may be stored in the original packaging at room temperature (not exceeding 25 °C) for up to 4 weeks.
Keep out of reach and sight of children.
Incompatibility. Use only the provided solvent.
Packaging. The kit contains 1 vial and a sterile needle. The vial contains a desiccant packet and a pre-connected syringe system: pre-filled syringe A containing solvent, pre-filled syringe B containing powder, and a connecting device with button for syringes A and B.
Kit in a cardboard box.
Prescription status. Prescription only.
Manufacturer. TOLMAR Inc.
Manufacturer's address and place of business.
701 Center Avenue, Fort Collins, CO 80526, USA.
Marketing Authorization Holder. Recordati Industria Chimica e Farmaceutica S.p.A.
Address of Marketing Authorization Holder. Via M. Civitali 1, 20148, Milan, Italy.