Eclira® jenueir®
Ukraine
Table of Contents
INSTRUCTIONS FOR MEDICAL USE OF THE MEDICINAL PRODUCT Eklira® Genuair® (Eklira® Genuair®)
Composition:
Active substance: aclidinium bromide;
One delivered dose (dose emitted from the mouthpiece) contains 375 mcg of aclidinium bromide, equivalent to 322 mcg of aclidinium. This corresponds to a metered dose of 400 mcg of aclidinium bromide, equivalent to 343 mcg of aclidinium;
Excipient: lactose monohydrate.
Pharmaceutical form. Powder for inhalation.
Main physicochemical properties: white or almost white, fine granular, free-flowing powder without visible agglomerates or foreign particles.
Pharmacotherapeutic group.
Drugs for treatment of obstructive respiratory diseases, anticholinergic agents. ATC code R03B B05.
Pharmacological Properties.
Pharmacodynamics.
Mechanism of action.
Aclidinium bromide is a competitive, selective antagonist of muscarinic receptors (anticholinergic agent) with a longer duration of binding to M3 receptors than to M2 receptors. M3 receptors mediate contraction of smooth muscle in the airways. Inhaled aclidinium bromide acts locally in the lungs as an antagonist of M3 receptors on airway smooth muscle, resulting in bronchodilation. Preclinical studies in vitro and in vivo demonstrated rapid, dose-dependent, and prolonged inhibition by aclidinium of acetylcholine-induced bronchospasm. Aclidinium bromide is rapidly degraded in blood plasma; therefore, the incidence of systemic anticholinergic adverse effects is low.
Pharmacodynamic effect.
Clinical efficacy studies showed that Eklira® Genuair® provides clinically significant improvement in lung function (measured by forced expiratory volume in 1 second [FEV1]) over 12 hours after both morning and evening dosing, evident within 30 minutes after the first dose (increase in FEV1 from baseline was 124–133 mL). Maximum bronchodilation was achieved within 1–3 hours after dosing, with a mean peak improvement in FEV1 from baseline of 227–268 mL at steady state.
Cardiac electrophysiology.
No effect on QT interval (corrected by Fridericia or Bazett methods or individually corrected) was observed when aclidinium bromide (200 mcg or 800 mcg) was administered once daily for 3 days to healthy subjects.
Additionally, no clinically significant effect of Eklira® Genuair® on heart rhythm was observed during 24-hour Holter monitoring after 3 months of treatment in 336 patients (164 of whom received Eklira® Genuair® twice daily at a dose of 322 mcg).
Clinical efficacy and safety.
The Phase III clinical development program included 269 patients receiving Eklira® Genuair® 322 mcg twice daily in one 6-month placebo-controlled randomized trial, and 190 patients receiving Eklira® Genuair® 322 mcg twice daily in one 3-month placebo-controlled randomized trial. Efficacy was assessed by lung function and symptomatic outcomes such as dyspnea, disease-specific health status, use of rescue medication, and exacerbation frequency. In long-term safety studies, Eklira® Genuair® demonstrated bronchodilator efficacy for more than 1 year.
Bronchodilation.
In the 6-month study, patients receiving Eklira® Genuair® 322 mcg twice daily showed clinically significant improvement in lung function (measured by FEV1). Maximum bronchodilatory effect was evident from the first day and increased over the 6-month treatment period. After 6 months of therapy, the mean improvement in pre-morning dose (trough) FEV1 compared to placebo was 128 mL (95% CI 85–170; p < 0.0001).
Similar observations were made for Eklira® Genuair® in 3-month studies.
Eklira® Genuair® provided clinically significant reduction in dyspnea (assessed by the Transition Dyspnea Index [TDI]), with a TDI improvement of 1.0 unit compared to placebo after 6 months of treatment (p < 0.001).
The proportion of patients achieving clinically significant improvement in TDI (defined as an increase of at least 1 unit in TDI score) was higher in the Eklira® Genuair® group compared to placebo (56.9% vs. 45.5%; p = 0.004).
Eklira® Genuair® demonstrated clinically significant symptom relief with improvement in overall scores compared to placebo—4.6 units (p < 0.0001). The proportion of patients achieving clinically significant improvement from baseline was higher in the Eklira® Genuair® group compared to placebo (57.3% vs. 41.0%, respectively; p < 0.001).
Patients receiving Eklira® Genuair® required less rescue medication than those receiving placebo (a reduction of 0.95 inhalations per day over 6 months [p = 0.005]). Eklira® Genuair® also improved daytime symptoms of chronic obstructive pulmonary disease (COPD) (dyspnea, cough, and sputum production), as well as nighttime and early morning symptoms.
A pooled analysis of efficacy from the 6-month and 3-month placebo-controlled trials demonstrated a significant reduction in the frequency of moderate and severe exacerbations (requiring treatment with antibiotics or corticosteroids or resulting in hospitalization) with twice-daily 322 mcg aclidinium compared to placebo.
Long-term safety and efficacy study with treatment duration up to 3 years.
The effect of aclidinium bromide on the occurrence of major adverse cardiovascular events (MACE) was evaluated in a randomized, double-blind, placebo-controlled, parallel-group study involving 3630 adult patients aged 40 to 91 years with moderate to very severe COPD, treated for up to 36 months. Of these, 58.7% were male and 90.7% were of Caucasian race, with a mean post-bronchodilator FEV1 of 47.9% of predicted value and a mean COPD Assessment Test (CAT) score of 20.7. All patients had a history of cardiovascular or cerebrovascular disease and/or significant risk factors for cardiovascular disease. 59.8% of patients had experienced at least one COPD exacerbation in the 12 months prior to the screening visit. Approximately 48% of study participants had a documented history of at least one cardiovascular event; cerebrovascular disease (13.1%), coronary artery disease (35.4%), peripheral vascular disease or claudication (13.6%).
The study was event-driven and was terminated once a sufficient number of MACE events had occurred to allow the primary safety analysis. Treatment was discontinued upon occurrence of a MACE, and patients were transferred to a post-treatment observation phase. According to investigator assessment, 70.7% of patients completed the study. The mean duration of treatment in the groups receiving Eklira® Genuair® and placebo was 1.1 and 1.0 years, respectively. The mean duration of study participation in the Eklira® Genuair® and placebo groups was approximately 1.4 and 1.3 years, respectively.
The primary safety endpoint was time to first occurrence of MACE, defined as any of the following adjudicated events: death due to cardiovascular causes, non-fatal myocardial infarction (MI), or non-fatal ischemic stroke. The incidence of at least one MACE was 3.85% and 4.23% in the aclidinium and placebo groups, respectively. Treatment with Eklira® Genuair® did not increase the risk of MACE in patients with COPD compared to placebo when added to background therapy (hazard ratio [HR] 0.89; 95% CI: 0.64, 1.23). The upper limit of the confidence interval excludes a risk margin of 1.8.
The rate of moderate or severe COPD exacerbations per patient per year during the first year of treatment was assessed as the primary efficacy endpoint. In patients receiving Eklira® Genuair®, there was a statistically significant 22% reduction compared to placebo (rate ratio [RR] 0.78; 95% CI: 0.68, 0.89; p < 0.001). Furthermore, treatment with Eklira® Genuair® resulted in a statistically significant 35% reduction in hospitalization rates due to COPD exacerbations during the first year of treatment compared to placebo (RR 0.65; 95% CI: 0.48, 0.89; p = 0.006).
In the group receiving Eklira® Genuair®, the delay in time to first moderate or severe exacerbation during treatment was statistically significant compared to the placebo group. In the aclidinium bromide group, there was a relative 18% reduction in the risk of exacerbation (HR 0.82; 95% CI [0.73, 0.92], p < 0.001).
Exercise tolerance.
In a 3-week crossover, randomized, placebo-controlled clinical trial, treatment with Eklira® Genuair® was associated with a statistically significant improvement in exercise endurance compared to placebo by 58 seconds. Eklira® Genuair® significantly reduced resting lung hyperinflation, increased inspiratory volume, and reduced dyspnea during exercise.
Pharmacokinetics.
Absorption.
Aclidinium bromide is rapidly absorbed from the lungs, reaching peak plasma concentration within 5 minutes after inhalation in healthy subjects and typically within the first 15 minutes in patients with COPD. The fraction of the inhaled dose reaching systemic circulation as unchanged aclidinium was very low, less than 5%.
At steady state, peak plasma concentration achieved in patients with COPD after inhalation of 400 mcg aclidinium bromide dry powder was approximately 224 pg/mL. Steady state in plasma was reached within 7 days with twice-daily dosing.
Distribution.
The total amount of aclidinium bromide inhaled via the Eklira® Genuair® inhaler that reaches the lungs is approximately 30% of the metered dose.
Binding of aclidinium bromide to plasma proteins in vitro is likely due to metabolite binding, as aclidinium bromide undergoes rapid hydrolysis in plasma. Plasma protein binding was 87% for the carboxylic acid metabolite and 15% for the alcohol metabolite. The main plasma protein binding aclidinium bromide is albumin.
Biotransformation.
Aclidinium bromide is rapidly and actively hydrolyzed to its pharmacologically inactive alcohol and carboxylic acid derivatives. Both chemical (non-enzymatic) and enzymatic hydrolysis (via esterases) occur. The main esterase involved in hydrolysis in humans is butyrylcholinesterase. Plasma levels of the acid metabolite after inhalation are approximately 100 times higher than those of the alcohol metabolite and unchanged active substance. The low absolute bioavailability of aclidinium bromide after inhalation (< 5%) is due to extensive systemic and pre-systemic hydrolysis in both the lungs and following oral administration. Metabolism involving CYP450 enzymes plays a negligible role in the overall metabolic clearance of aclidinium bromide.
In vitro studies showed that aclidinium bromide at therapeutic doses or its metabolites do not inhibit or induce any cytochrome P450 (CYP450) enzymes and do not inhibit esterase activity (carboxylesterase, acetylcholinesterase, or butyrylcholinesterase). In vitro studies also showed that aclidinium bromide or its metabolites are not substrates or inhibitors of P-glycoprotein.
Elimination.
In patients with COPD, after twice-daily inhalation of 400 mcg, the terminal and effective half-lives of aclidinium bromide are approximately 14 hours and 10 hours, respectively.
After intravenous administration of 400 mcg radiolabeled aclidinium bromide to healthy volunteers, approximately 1% of the dose was excreted unchanged in urine. Up to 65% of the dose was excreted as metabolites in urine and up to 33% as metabolites in feces.
After inhaled administration of 200 mcg and 400 mcg aclidinium bromide to healthy subjects and patients with COPD, a very small amount, approximately 0.1% of the administered dose, was excreted unchanged in urine, indicating that renal clearance plays a minor role in the overall clearance of aclidinium from plasma.
Linearity/Non-linearity.
Aclidinium bromide demonstrated linear kinetics and time-independent pharmacokinetics within the therapeutic range.
Special patient populations.
Patients with hepatic impairment.
Studies in patients with hepatic impairment have not been conducted. Since aclidinium bromide is primarily metabolized via chemical and enzymatic hydrolysis in plasma, it is highly unlikely that hepatic impairment alters its systemic effects. Dose adjustment is not required for patients with COPD and hepatic impairment.
Elderly patients.
Pharmacokinetic properties of aclidinium bromide in patients with moderate to severe COPD are similar in patients aged 40–59 years and those over 70 years of age. Therefore, dose adjustment is not required for elderly patients with COPD.
Patients with renal impairment.
No significant differences in pharmacokinetics were observed between patients with normal renal function and those with renal impairment. Therefore, dose adjustment and additional monitoring are not required for patients with COPD and renal impairment.
Racial origin.
After repeated inhalations, systemic exposure to aclidinium bromide was similar in Japanese and Caucasian subjects.
Pharmacokinetic/pharmacodynamic relationship.
Since aclidinium bromide exerts a local effect in the lungs and is rapidly degraded in plasma, there is no direct correlation between pharmacokinetics and pharmacodynamics.
Preclinical safety data.
Preclinical safety data based on conventional safety pharmacology, repeated-dose toxicity, genotoxicity, carcinogenicity, and reproductive toxicity studies revealed no special risk to humans. In preclinical studies, effects on cardiovascular parameters (increased heart rate in dogs), reproductive toxicity (fetotoxic effects), and fertility (slight reduction in conception rate, number of corpora lutea, and pre- and post-implantation embryo loss) were observed only at exposure levels significantly exceeding the maximum human exposure, indicating low relevance for clinical use. The low toxicity observed in preclinical toxicity studies is partly due to the rapid metabolism of aclidinium bromide in plasma and the lack of significant pharmacological activity of most metabolites. The safety margin for systemic exposure in humans at 400 mcg twice daily in these studies ranged from 7- to 73-fold of the maximum dose not causing observed adverse effects.
Clinical characteristics.
Indications.
Maintenance bronchodilator therapy to relieve symptoms of chronic obstructive pulmonary disease (COPD) in adults (see section "Pharmacodynamics").
Contraindications.
Hypersensitivity to aclidinium bromide or to any of the excipients.
Interaction with other medicinal products and other forms of interactions.
Concomitant use of aclidinium bromide with other anticholinergic medicinal products is not recommended, as it has not been studied. Although formal in vivo drug interaction studies have not been conducted, aclidinium bromide administered by inhalation has been used together with other medicinal products for COPD therapy, including bronchodilators: sympathomimetics, methylxanthines, and steroids – administered by inhalation or orally, without clinical evidence of drug interactions. In vitro studies have shown that aclidinium bromide at therapeutic doses or its metabolites do not interact with active substances that are substrates of P-glycoprotein (P-gp), or with active substances metabolized by cytochrome P450 (CYP450) enzymes and esterases (see section "Pharmacokinetics").
Special precautions for use.
Paradoxical bronchospasm.
The use of Eklira® Genuair® may induce paradoxical bronchospasm. If this occurs, treatment with Eklira® Genuair® must be discontinued and alternative therapy should be considered.
Worsening of disease.
Aclidinium bromide is a maintenance bronchodilator and should not be used for the relief of acute bronchospasm episodes, i.e., as a rescue therapy medication. If during treatment with aclidinium bromide a patient experiences a change in the severity of COPD symptoms requiring additional rescue therapy, the patient's condition and treatment regimen should be re-evaluated.
Effect on the cardiovascular system.
Cardiac arrhythmias, including atrial fibrillation and paroxysmal tachycardia, have been observed following administration of the medicinal product Eklira® Genuair® (see section "Adverse reactions"). Therefore, Eklira® Genuair® should be used with caution in patients with cardiac arrhythmias, a history of cardiac arrhythmias, or risk factors for cardiac arrhythmias.
Experience in patients with concomitant cardiovascular diseases during clinical trials is limited (see section "Pharmacodynamics"). These conditions may be influenced by the anticholinergic mechanism of action.
Anticholinergic effects.
Dry mouth, commonly observed during treatment with anticholinergic medications, may be associated with dental caries during prolonged use.
Due to the anticholinergic action of aclidinium bromide, caution is advised when administering the drug to patients with symptomatic benign prostatic hyperplasia, bladder neck contracture, or narrow-angle glaucoma (despite the very low likelihood of direct contact of the drug with the eyes).
Excipients.
This medicinal product contains lactose. Each delivered dose contains approximately 12 mg of lactose (as monohydrate). This medicinal product should not be administered to patients with rare hereditary forms of galactose intolerance, severe lactase deficiency, or glucose-galactose malabsorption.
Use during pregnancy or breastfeeding.
Pregnancy.
There are no data on the use of aclidinium bromide in pregnant women.
Animal studies have demonstrated fetal toxicity only at doses substantially exceeding the maximum human exposure to aclidinium bromide (see "Non-clinical safety data"). Aclidinium bromide may be used during pregnancy only if the expected benefit outweighs the potential risk.
Breastfeeding.
It is unknown whether aclidinium bromide/metabolites are excreted in human breast milk. Animal studies have shown that aclidinium bromide and/or its metabolites are excreted into milk in small quantities. Risk to the newborn/infant cannot be excluded. A decision on whether to discontinue breastfeeding or discontinue/abstain from treatment with Eklira® Genuair® should be made taking into account the benefit of breastfeeding for the child and the benefit of treatment for the woman.
Fertility.
Animal studies have demonstrated a slight reduction in fertility only at doses substantially exceeding the maximum human exposure to aclidinium bromide (see "Non-clinical safety data"). It is considered unlikely that aclidinium bromide administered at the recommended dose affects fertility in humans.
Ability to affect reaction speed while driving or operating machinery.
Aclidinium bromide may have a minor influence on reaction speed while driving or operating machinery. The occurrence of headache, dizziness, or blurred vision after administration of aclidinium bromide (see section "Adverse reactions") may affect reaction speed while driving or operating machinery.
Method of Administration and Dosage.
For inhalation.
Patients must be instructed on the correct use of the medicinal product, as the Genuair® inhaler may function differently from inhalers patients may have used previously. It is important that the patient reads the instructions for use carefully.
The recommended dose is 1 inhalation of 322 mcg aclidinium twice daily.
If a dose is missed, the next dose should be taken as soon as possible. However, if it is almost time for the next scheduled dose, the missed dose should not be administered.
Elderly patients.
Dose adjustment is not required in elderly patients (see section "Pharmacokinetics").
Renal impairment.
Dose adjustment is not required in patients with renal impairment (see section "Pharmacokin游戏副本)."
Hepatic impairment.
Dose adjustment is not required in patients with hepatic impairment (see section "Pharmacokinetics").
Instructions for Use.
Starting Treatment.
Read these instructions for use before starting the medication.
The inhaler is white with an integrated dose indicator and a green dosing button. The mouthpiece is covered by a removable protective cap. The inhaler comes in a laminated plastic pouch, packed in a cardboard box.
Familiarize yourself with the parts of the Genuair® inhaler.
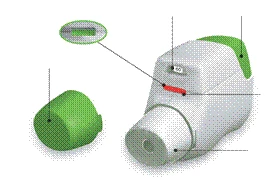
Figure A
Before use:
- Before first use, tear open the sealed pouch and remove the inhaler. Discard the pouch.
- Do not press the green button until you are ready to take a dose.
- Remove the cap by gently pressing the arrows marked on each side (Figure B).

Figure B
-
- Hold the inhaler horizontally with the mouthpiece facing toward you, and the green button facing upward (Figure C).
**

**
Figure C
-
- Press the green button fully downward to prepare a dose of the medication (Figure E).
When you press the button fully down, the control window changes color from red to green.
Ensure the green button is on top. Do not tilt the inhaler.
-
- Release the green button (Figure D).
Make sure you have released the button so the inhaler can function properly.

Figure E
The dose of medication has not been prepared. Return to section "STEP 1: Prepare the Medication Dose" and repeat steps 1.1 to 1.6.
STEP 2: Inhale the Medication
Read steps 2.1 to 2.7 completely before using the medication. Do not tilt the inhaler.
-
- Holding the inhaler away from your mouth, breathe out fully. Never breathe out into the inhaler (Figure F).
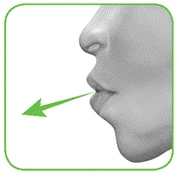
Figure F
-
- Keep your head upright, place the mouthpiece between your lips, and seal your lips tightly around it (Figure G).
Do not hold the green button pressed during inhalation.
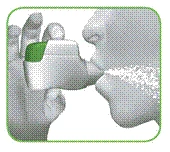
Figure G
-
- Take a strong, deep breath in through your mouth. Continue inhaling for as long as possible.
If the inhalation is performed correctly, a click will be heard. After you hear the click, continue inhaling for as long as possible. Some patients may not hear the click. Use the control window to confirm that the inhalation was performed correctly.
-
- Remove the inhaler from your mouth.
-
- Hold your breath for as long as possible.
-
- Breathe out slowly, but not into the inhaler.
Some patients may feel a gritty sensation in the mouth or a mild sweet or bitter taste. Do not inhale additional medication, even if you do not taste anything or feel nothing after inhalation.
Stop and check:
-
- Make sure the control window is now red (Figure I). This indicates that the medication inhalation was performed correctly.

Figure I
This means the medication inhalation was performed incorrectly. Return to section "STEP 2: Inhale the Medication" and repeat steps 2.1 to 2.7.
If the control window still has not turned red, you may have forgotten to release the green button before inhalation, or your inhalation may not have been strong enough. In this case, try again. Make sure you have released the green button and breathed out fully. Then take a strong, deep breath in through the mouthpiece.
Consult your doctor if, after repeated attempts, the control window remains green.
After each use, replace the protective cap over the mouthpiece (Figure J) to prevent contamination of the inhaler by dust or other substances. If the cap is lost, the inhaler should be discarded.

Additional Information.
What to do if you accidentally prepared a dose before use?
Keep the inhaler with the protective cap in place until it is time to take your scheduled dose, then remove the cap and proceed to step 1.6.
How does the dose indicator work?
The dose indicator shows the total number of doses remaining in the inhaler (Figure K).
Each inhaler contains at least 60 doses or at least 30 doses, depending on the pack size, when first used.
Each time a dose is prepared by pressing the green button, the dose indicator moves slightly toward the next number (50, 40, 30, 20, 10, or 0).
When do you need a new inhaler?
You need a new inhaler:
If your inhaler is damaged or if you have lost the cap, or
When red stripes appear on the dose indicator, indicating that the last dose is approaching (Figure K), or
If your inhaler is empty (Figure L).
The dose indicator moves slowly from 60 to 0: 60, 50, 40, 30, 20, 10, 0.
How to keep the inhaler clean?
NEVER use water to clean the inhaler, as this may damage the medication.
If you wish to clean it, simply wipe the mouthpiece externally with a dry cloth or paper towel.
Children.
The medicinal product Eklira® Genuair® is not recommended for use in children (under 18 years of age) due to insufficient clinical experience.
Overdose.
High doses of aclidinium bromide may cause signs and symptoms of anticholinergic effects. However, a single inhaled dose of up to 6000 mcg of aclidinium bromide in healthy subjects did not result in systemic anticholinergic adverse reactions. Furthermore, clinically significant adverse reactions were not observed after 7 days of treatment with up to 800 mcg of aclidinium bromide twice daily in healthy subjects.
Acute intoxication following accidental ingestion of aclidinium bromide is unlikely due to its low oral bioavailability and the inhalation dosing mechanism of the Genuair® inhaler.
Adverse Reactions
The most commonly observed adverse reactions during the use of Eklira® Genuair® are headache (6.6%) and nasopharyngitis (5.5%).
The frequencies of the adverse reactions listed below were determined based on overall incidence rates of adverse reactions (i.e., reactions occurring in connection with the use of Eklira® Genuair®). These reactions were observed during the administration of Eklira® Genuair® at a dose of 322 mcg (636 patients) in one 6-month and two 3-month randomized, placebo-controlled clinical trials, as well as in post-marketing surveillance studies.
In a placebo-controlled study involving 1791 patients with moderate to very severe COPD, in which the treatment duration with Eklira® Genuair® was up to 36 months, no other adverse reactions were identified.
The frequency of adverse reactions is defined as follows: very common (≥ 1/10), common (≥ 1/100 to < 1/10), uncommon (≥ 1/1000 to < 1/100), rare (≥ 1/10,000 to < 1/1000), very rare (< 1/10,000); frequency not known (cannot be estimated from the available data).
| System organ classes |
Adverse reactions |
Frequency |
| Infections and infestations |
Sinusitis |
Common |
| Nasopharyngitis |
Common |
|
| Immune system disorders |
Hypersensitivity reactions |
Uncommon |
| Angioedema |
Frequency unknown |
|
| Anaphylactic reaction |
Frequency unknown |
|
| Nervous system disorders |
Headache |
Common |
| Dizziness |
Uncommon |
|
| Eye disorders |
Blurred vision |
Uncommon |
| Cardiac disorders |
Cardiac arrhythmias, including atrial fibrillation and paroxysmal tachycardia |
Uncommon |
| Tachycardia |
Uncommon |
|
| Palpitations |
Uncommon |
|
| Respiratory, thoracic and mediastinal disorders |
Cough |
Common |
| Dysphonia |
Uncommon |
|
| Gastrointestinal disorders |
Diarrhea |
Common |
| Nausea |
Common |
|
| Dry mouth |
Uncommon |
|
| Stomatitis |
Uncommon |
|
| Skin and subcutaneous tissue disorders |
Rash |
Uncommon |
| Pruritus |
Uncommon |
|
| Renal and urinary disorders |
Urinary retention |
Uncommon |
Reporting of suspected adverse reactions.
Reporting of adverse reactions after the medicinal product has been registered is of great importance. This enables ongoing monitoring of the benefit-risk balance of the medicinal product. Medical and pharmaceutical professionals, as well as patients or their legal representatives, should report all suspected adverse reactions and lack of effectiveness of the medicinal product through the Automated Information System for Pharmacovigilance at the following link: https://aisf.dec.gov.ua.
Shelf life.
3 years. Use within 90 days after opening.
Storage conditions.
No special storage conditions required. The Jenuair® inhaler should be stored in its original packaging until first use. Keep out of reach of children.
Packaging.
30 doses of powder in an inhaler; 1 inhaler in a plastic bag in a cardboard box;
60 doses of powder in an inhaler; 1 or 3 inhalers, each in a plastic bag, in a cardboard box.
Prescription status.
Prescription only.
Manufacturer.
Industrias Farmaceuticas Almirall S.A.
Manufacturer's address and place of business.
Ctra. de Martorell 41-61, 08740 Sant Andreu de la Barca (Barcelona), Spain.
Marketing Authorisation Holder.
Berlin-Chemie AG.
Address of the Marketing Authorisation Holder.
Glinkiker Weg 125, 12489 Berlin, Germany.