Jadese®
Ukraine
Table of Contents
INSTRUCTIONS FOR MEDICAL USE OF THE MEDICINAL PRODUCT JAYDESS®
Composition:
Active substance: levonorgestrel;
1 intrauterine system contains 13.5 mg of levonorgestrel;
Excipients: polydimethylsiloxane elastomer core;
silica-filled polydimethylsiloxane elastomer; polyethylene; barium sulfate; iron oxide (E 172); silver (E 174).
Pharmaceutical form. Levonorgestrel-releasing intrauterine system.
Main physicochemical characteristics: intrauterine system with a silver ring, without visible damage. The color of the reservoir containing the active substance is whitish or pale yellow.
Pharmacotherapeutic group. Agents affecting the genitourinary system and sex hormones. Local contraceptive. Intrauterine contraceptives. Plastic intrauterine antifertility devices with progestogens.
ATC code G02BA03.
Pharmacological Properties
Pharmacodynamics
The Jaydess® system has primarily a local progestogenic effect on the uterine cavity.
The high concentration of levonorgestrel in the endometrium suppresses the synthesis of endometrial estrogen and progesterone receptors. The endometrium becomes relatively insensitive to circulating estradiol, resulting in a significant antiproliferative effect. With use of the Jaydess® system, morphological changes in the endometrium and a weak reaction to a foreign body have been observed. Thickening of cervical mucus prevents sperm penetration through the cervical canal. The local microenvironment of the uterus and fallopian tubes inhibits sperm motility and function, thereby preventing fertilization. In clinical studies of the Jaydess® system, ovulation was observed in the majority of women in the respective subgroup. Signs of ov游戏副本
| Time |
Determined rate of drug release in vivo (micrograms/24 hours) |
| 24 days after administration |
14 |
| 60 days after administration |
10 |
| 1 year after administration |
6 |
| 3 years after administration |
5 |
| Mean value over the 1st year |
8 |
| Mean value over 3 years |
6 |
Absorption. Based on serum concentration measurements, it has been determined that after insertion of the Jaydess® system, levonorgestrel is immediately released into the uterine cavity. More than 90% of the released levonorgestrel is systemically available. Maximum serum concentration of levonorgestrel is reached within the first two weeks after insertion of the Jaydess® system. Seven days after insertion, the mean concentration of levonorgestrel was 162 pg/mL (5th percentile: 102 pg/mL – 95th percentile: 249 pg/mL). Thereafter, serum concentrations of levonorgestrel gradually decline over time, reaching 59 pg/mL after 3 years (5th percentile: 36 pg/mL – 95th percentile: 92 pg/mL). With the use of the levonorgestrel-releasing IUD, high local concentrations of the drug in the uterine cavity result in a significant concentration gradient between endometrium and myometrium (endometrium–myometrium concentration ratio > 100-fold) and low serum concentrations of levonorgestrel (endometrium–serum concentration ratio > 1000-fold).
Distribution. Levonorgestrel binds non-specifically to serum albumin and specifically to sex hormone-binding globulin (SHBG). Less than 2% of circulating levonorgestrel is present in the free steroid form. Levonorgestrel binds with high affinity to SHBG. Therefore, changes in serum SHBG concentration lead to increased (with higher SHBG concentration) or decreased (with lower SHBG concentration) total serum concentrations of levonorgestrel. Within one month after insertion of the Jaydess® system, SHBG concentration decreases on average by 15% and remains stable throughout 3 years of use. The mean apparent volume of distribution of levonorgestrel is approximately 106 L.
Metabolism. Levonorgestrel is extensively metabolized. The most important metabolic pathways are reduction of the Δ4-3-oxo group and hydroxylation at positions 2α, 1β, and 16β, followed by conjugation. CYP3A4 is the primary enzyme involved in the oxidative metabolism of levonorgestrel. Available in vitro data indicate that this oxidative pathway is of lesser importance for levonorgestrel compared to reduction and conjugation.
Elimination. Total plasma clearance of levonorgestrel is approximately 1.0 mL/min/kg. Only trace amounts of unchanged levonorgestrel are excreted. Metabolites are excreted in urine and feces with an excretion coefficient of approximately 1.
The elimination half-life is approximately 1 day.
Linearity/Non-linearity. The pharmacokinetics of levonorgestrel depend on SHBG concentration, which in turn is influenced by estrogens and androgens. The decline in SHBG levels leads to an overall reduction in total serum levonorgestrel concentration, indicating non-linear kinetics of levonorgestrel concentration decline over time. Since the Jaydess® system acts predominantly locally, no impact on its efficacy is expected.
Paediatric patients. In a one-year Phase III study involving post-menarcheal adolescent girls (mean age 16.2 years; age range 12 to 18 years), pharmacokinetic analysis of data from 283 study participants showed that expected serum concentrations of levonorgestrel are slightly higher (approximately 10%) in adolescents compared to adult women. This correlates with the generally lower body weight in adolescents. The expected range in adolescents falls within the range observed in adults and shows high similarity.
No differences in the pharmacokinetics of levonorgestrel between adolescents and adult women are expected after insertion of the Jaydess® IUD.
Ethnic differences. A three-year Phase III study of the Jaydess® system was conducted in the Asia-Pacific region (93% of participants were of Asian origin, 7% from other ethnic groups). A comparison of the pharmacokinetic characteristics of levonorgestrel in Mongoloid women from this study with those in Caucasian women from another Phase III study showed no clinically significant differences in systemic distribution or other pharmacokinetic parameters. Furthermore, the daily release rate of levonorgestrel from the Jaydess® system was similar in both populations.
No differences in the pharmacokinetics of levonorgestrel are expected between Mongoloid and Caucasian women after insertion of the Jaydess® system.
Clinical characteristics.
Indications.
Contraception for a period of three years.
Contraindications.
- Pregnancy.
- Acute or recurrent inflammatory diseases of the pelvic organs or conditions associated with an increased risk of pelvic infection.
- Acute cervicitis or vaginitis.
- Postpartum endometritis or infected abortion within the past three months.
- Cervical intraepithelial neoplasia until full recovery.
- Malignant tumors of the cervix or uterus.
- Progesterone-dependent tumors, including breast cancer.
- Pathological uterine bleeding of unknown cause.
- Congenital or acquired uterine abnormalities, including leiomyomas, which may interfere with insertion and/or retention of the intrauterine system (e.g., if they distort the uterine cavity).
- Acute liver disease or liver tumors.
- Hypersensitivity to the active substance or to any of the excipients.
Interaction with other medicinal products and other forms of interaction.
Note: To identify potential interactions, refer to the package leaflet of any concurrently administered medicinal product.
Effect of other medicinal products on Jaydess® IUS
Interactions are possible when used concomitantly with drugs that induce hepatic enzymes and may increase the clearance of sex hormones.
Active substances that increase levonorgestrel clearance, e.g.: phenytoin, barbiturates, primidone, carbamazepine, rifampicin, and possibly oxcarbazepine, topiramate, felbamate, griseofulvin, and products containing St. John's wort.
The effect of these medicinal products on the contraceptive efficacy of Jaydess® is unknown; however, it is considered to be negligible due to the predominantly local mechanism of action of the device.
Active substances with variable effects on levonorgestrel clearance:
When used concomitantly with sex hormones, a large number of HIV/HCV protease inhibitors and non-nucleoside reverse transcriptase inhibitors may either increase or decrease plasma concentrations of progestin.
Active substances that decrease levonorgestrel clearance (enzyme inhibitors): concomitant use of strong and moderate CYP3A4 inhibitors, such as azole antifungals (e.g., fluconazole, itraconazole, ketoconazole, voriconazole), verapamil, macrolides (e.g., clarithromycin, erythromycin), diltiazem, and grapefruit juice, may increase progestin plasma concentrations.
Magnetic resonance imaging (MRI)
Non-clinical studies have demonstrated that MRI procedures are safe for patients after insertion of Jaydess® under the following conditions: static magnetic field of 3-Tesla or less, maximum spatial gradient magnetic field of 720-gauss/cm or less. Under these conditions, the maximum temperature rise at the site of Jaydess® during a 15-minute procedure was 1.8°C. MRI image quality may be slightly reduced if the area being examined is in the same location or relatively close to the position of Jaydess®.
Special precautions for use.
JAYDES® should be used with caution after consultation with a specialist. Consideration should be given to removing the system in the presence of any of the conditions listed below or if any of these conditions have newly developed:
- Migraine, particularly focal migraine accompanied by asymmetric visual disturbances or other symptoms suggestive of transient cerebral ischemia;
- Extremely severe headache;
- Jaundice;
- Marked increase in blood pressure;
- Severe cardiovascular diseases, such as stroke or myocardial infarction.
Low doses of levonorgestrel may affect glucose tolerance; therefore, blood glucose levels should be monitored in patients with diabetes mellitus who are using the JAYDES® system. However, dosage adjustments are generally not required for women with diabetes who use levonorgestrel-releasing IUS.
Medical examination/consultation
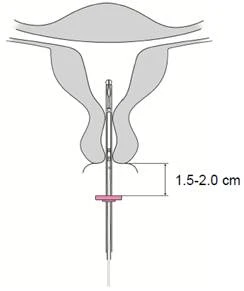
Prior to administration, women should be informed about the benefits and risks associated with the use of the JAYDES® system, including signs and symptoms of perforation and the risk of ectopic pregnancy (see below). A physical examination of the patient, including pelvic and breast examination, should be performed. A cervical cytology smear test should be carried out as clinically indicated, based on the physician’s assessment. Pregnancy and sexually transmitted infections must be ruled out. Any genital tract infections should be treated prior to IUS insertion. The position and size of the uterine cavity should be determined. It is particularly important to place the JAYDES® system at the fundus of the uterus to achieve maximum effectiveness and reduce the risk of expulsion. The instructions for system insertion must be strictly followed.
Special attention should be paid to training and mastering the correct technique of system insertion.
Insertion and removal of the system may cause pain and bleeding. The procedure may provoke vasovagal reactions (e.g., dizziness or seizures in patients with epilepsy).
Women should undergo a follow-up examination 4–6 weeks after insertion to verify correct placement of the system and the presence of the retrieval threads. Subsequently, annual visits to the physician are recommended, or more frequently if medically indicated.
The JAYDES® system is not intended for use as a postcoital contraceptive method.
The use of the JAYDES® system for the treatment of severe menstrual bleeding or for protection against endometrial hyperplasia during estrogen replacement therapy has not been studied. Therefore, use of the system for these conditions is not recommended.
Ectopic pregnancy
In clinical studies, the overall incidence of ectopic pregnancy among women using the JAYDES® system was approximately 0.11 per 100 women per year. Approximately half of the pregnancies occurring in women with an in situ JAYDES® system may be ectopic. Women considering use of the JAYDES® system should be counselled regarding the signs, symptoms, and risks of ectopic pregnancy. In women who become pregnant while using the JAYDES® system, ectopic pregnancy should be considered and evaluated.
Women with a history of ectopic pregnancy, tubal surgery, or pelvic inflammatory disease are at increased risk of ectopic pregnancy. Ectopic pregnancy should be considered in the presence of lower abdominal pain, particularly in the absence of menstruation, or if bleeding occurs in a woman with amenorrhea.
Because ectopic pregnancy may affect future fertility, the benefits and risks of using the JAYDES® system should be carefully evaluated, particularly in women who have not yet given birth.
Use in women who have not given birth. The JAYDES® system is not a first-line contraceptive method for women who have not given birth, as clinical experience with the system in this group of women is limited.
Effect on menstrual bleeding pattern
Changes in menstrual bleeding patterns are expected in most patients using the JAYDES® system and are considered a direct effect of levonorgestrel on the endometrium; these changes may not correlate with ovarian activity.
Irregular bleeding/spotting is common during the first months of use. Subsequently, strong suppression of endometrial activity leads to reduced duration and volume of menstrual bleeding. Light spotting often progresses to oligomenorrhea or amenorrhea.
Clinical data indicate that infrequent bleeding and/or amenorrhea may gradually develop. By the end of the third year, approximately 22.3% and 11.6% of women using the IUS experience infrequent bleeding and/or amenorrhea, respectively. If a woman has not had a menstrual period within 6 weeks after her last menstruation, pregnancy should be considered. If no other signs of pregnancy are present, there is no need to repeat a pregnancy test in women with amenorrhea until other symptoms of pregnancy appear.
If bleeding increases in volume and/or becomes more irregular over time, appropriate diagnostic measures should be considered, as irregular bleeding may be a symptom of endometrial polyps, hyperplasia, or cancer. Heavy bleeding may indicate undetected IUS expulsion.
Pelvic infections
The JAYDES® system and the insertion tube are sterile but may act as vectors for microorganisms into the upper genital tract due to bacterial contamination during insertion. Pelvic infections have been reported during use of any IUS or intrauterine device. Clinical studies have shown that pelvic inflammatory disease (PID) most commonly occurs at the beginning of JAYDES® use, consistent with data from copper-containing intrauterine devices. The highest risk of PID occurs within the first three weeks after insertion, after which the risk of infection decreases.
Prior to initiating use of the JAYDES® system, patients should be examined and assessed for risk factors for pelvic infections (e.g., multiple sexual partners, sexually transmitted infections, history of pelvic inflammatory disease). Pelvic infections such as PID may lead to serious complications, affect fertility, and increase the risk of ectopic pregnancy.
As with other gynecological or surgical procedures, severe infections or sepsis (including sepsis caused by Group A streptococcus) may occur following intrauterine device insertion, although the likelihood of such complications is extremely low.
If a woman experiences recurrent endometritis or pelvic inflammatory disease, or acute severe inflammation or inflammation unresponsive to treatment within several days, the JAYDES® system should be removed.
Bacteriological investigations should be performed, and careful monitoring of the patient is recommended even in the presence of isolated symptoms of infection.
Expulsion
In clinical studies, the rate of expulsion (spontaneous loss) of the JAYDES® system was low (< 4% of insertions) and within the same range as other IUS or intrauterine devices. Symptoms of partial or complete expulsion of the JAYDES® system may include pain and bleeding. However, the system may be expelled from the uterine cavity unnoticed by the woman, resulting in loss of contraceptive protection. Because the JAYDES® system reduces menstrual flow, increased bleeding may be a sign of expulsion.
The risk of expulsion is increased in:
- Women with a history of heavy menstrual bleeding;
- Women with a body mass index (BMI) above normal at the time of insertion; this risk increases progressively with higher BMI.
Women should be counselled about possible signs of expulsion and how to check for the presence of the JAYDES® system threads, and advised to consult a physician if the threads cannot be felt. Barrier contraceptives (e.g., condoms) should be used until the correct position of the JAYDES® system is confirmed.
Partial expulsion of the JAYDES® system may reduce its effectiveness.
A partially expelled JAYDES® system should be removed. A new system may be inserted immediately after removal, provided pregnancy is excluded.
Perforation
In rare cases, usually during insertion, an intrauterine contraceptive may cause perforation or penetration of the uterine wall or cervix, although this may remain undetected for some time, potentially reducing the contraceptive efficacy of the JAYDES® system. If difficulties occur during insertion and/or unusual pain or bleeding occurs during or after insertion, appropriate measures should be taken immediately, such as gynecological examination and ultrasound, to rule out uterine wall perforation. Such a system should be removed. Surgical intervention may be necessary.
In a prospective comparative non-interventional cohort study among users of other intrauterine devices (N = 61,448 women), the rate of perforations during the 1-year observation period was 1.3 (95% confidence interval: 1.1–1.6) per 1,000 insertions in the entire cohort; 1.4 (95% confidence interval: 1.1–1.8) per 1,000 insertions of other levonorgestrel-releasing IUS, and 1.1 (95% confidence interval: 0.7–1.6) per 1,000 insertions of copper-containing intrauterine devices.
Study data indicate that both insertion during breastfeeding and insertion within 36 weeks postpartum are associated with an increased risk of perforation (see Table 2). Both risk factors were independent of the type of intrauterine device inserted.
Table 2. Perforation rate per 1,000 insertions in the cohort of women participating in the study during 1 year of observation, by presence of breastfeeding at insertion and timing of insertion after childbirth.
| Breastfeeding at the time of administration |
No breastfeeding at the time of administration |
|
| Administration ≤ 36 weeks postpartum |
5.6 95 % confidence interval: 3.9–7.9; n = 6047 administrations |
1.7 95 % confidence interval: 0.8–3.1; n = 5927 administrations |
| Administration > 36 weeks postpartum |
1.6 95 % confidence interval: 0.0–9.1; n = 608 administrations |
0.7 95 % confidence interval: 0.5–1.1; n = 41910 administrations |
When the observation period was extended to 5 years in a subgroup of this study (n = 39009 women using another LNG-IUS or copper intrauterine devices; for 73 % of these women, data were available throughout the entire 5-year observation period), the incidence of perforations detected at any time during the 5-year period was 2.0 (95 % CI: 1.6–2.5) per 1000 insertions. Insertion during lactation and within 36 weeks after childbirth were confirmed as risk factors for perforation also in the 5-year observation subgroup.
The risk of perforation may be increased in women with a fixed retroversion of the uterus.
A follow-up examination should be performed after insertion according to the recommendations outlined in the section "Medical examination/consultation", which may be adapted according to clinical indications for women with risk factors for perforation.
Missing threads
If during a routine examination the removal threads are not visually identified at the cervix, expulsion or pregnancy should be ruled out. The threads may have retracted into the uterus or cervical canal and may reappear during the next menstruation. If pregnancy is excluded, the location of the threads can be determined by careful sounding of the cervical canal using an appropriate instrument. If the threads cannot be located, perforation or expulsion should be considered. Ultrasound examination may be performed to determine the location of the system. If ultrasound examination is not available or does not provide satisfactory results, X-ray examination may be used to determine the position of the Jaydess® system.
Ovarian cysts / ovarian follicle enlargement
Since the contraceptive effect of the Jaydess® system is primarily achieved through local action in the uterus, there is generally no change in ovulation; in particular, regular follicular maturation, release of the oocyte following rupture of the mature follicle, and follicular atresia occur in women of reproductive age. Occasionally, follicular atresia is delayed, and follicular development may continue. Such enlarged follicles cannot be clinically distinguished from ovarian cysts and were diagnosed in approximately 13.2 % of women using the Jaydess® system. Most of these follicles are asymptomatic, although some may be associated with pelvic pain or dyspareunia.
In most cases, enlarged follicles resolve spontaneously within two to three months of observation. If follicles do not resolve, ongoing ultrasound monitoring or other diagnostic/therapeutic procedures are recommended. In isolated cases, surgical intervention may be required.
Psychiatric disorders
Depressed mood and depression are well-known adverse reactions that may occur during the use of hormonal contraceptives (see section "Adverse reactions"). Depression can be a serious condition and is a well-known risk factor for suicidal behaviour and suicide. Women should be advised to consult a physician if they experience mood changes or symptoms of depression, including shortly after starting the medicinal product.
Use during pregnancy or breastfeeding
Pregnancy. Use of the Jaydess® system in pregnant women is contraindicated (see section "Contraindications").
If a woman becomes pregnant with the Jaydess® system in place, ectopic pregnancy should be ruled out and the system should be removed as soon as possible, as any intrauterine contraceptive remaining in the uterus during pregnancy increases the risk of miscarriage and preterm delivery. Removal of the Jaydess® system or uterine sounding may also lead to spontaneous abortion. Ectopic pregnancy should be ruled out. If a woman wishes to continue the pregnancy and the system cannot be removed, she should be informed about the risks and possible consequences of preterm delivery and the birth of a premature infant. Such a pregnancy requires careful monitoring. The woman should inform her physician about any symptoms that may be associated with pregnancy complications, such as colicky abdominal pain with fever.
Furthermore, an increased risk of virilization in female fetuses due to intrauterine exposure to levonorgestrel cannot be excluded. Isolated cases of masculinization of external genitalia in female fetuses have been reported following local exposure to levonorgestrel during pregnancy with an implanted levonorgestrel-releasing IUD.
Lactation. Generally, no harmful effects on the growth and development of the child have been observed with the use of a progestogen-only contraceptive starting six weeks after childbirth. The levonorgestrel IUD does not affect the quantity or quality of breast milk. Progestogens pass into breast milk in small amounts (about 0.1 % of levonorgestrel).
Fertility. Use of the levonorgestrel IUD does not affect future fertility. Fertility in women returns after removal of the IUD (see section "Pharmacodynamics").
Ability to affect reaction speed when driving vehicles or operating machinery.
The Jaydess® system does not affect the ability to drive a vehicle or operate machinery.
Method of Administration and Dosage
The Jaydess® intrauterine system is inserted into the uterine cavity and remains effective for up to three years.
Insertion
It is recommended that the Jaydess® system be inserted only by a physician experienced in intrauterine device (IUD) insertion and/or who has received specific training in the insertion of the Jaydess® system.
Prior to insertion, the patient should be thoroughly examined to identify any contraindications to IUD use. Pregnancy must be excluded before insertion. The possibility of ovulation and conception should be considered before using this medicinal product. The Jaydess® system is not intended for use as a postcoital contraceptive (see section "Contraindications" and "Medical Examination/Consultation" in the "Special Warnings and Precautions for Use" section).
Table 3. Timing of Jaydess® system insertion in women of reproductive age.
| Initiation of Jaydess® use |
|
| Postpartum insertion |
Postpartum insertion should be delayed until complete uterine involution is achieved, but it may be performed no earlier than 6 weeks after delivery. If involution is proceeding too slowly, insertion of the device should be carried out 12 weeks after delivery. |
| Insertion after first-trimester abortion |
The system can be inserted immediately after a first-trimester abortion. In this case, no additional contraception is required. |
| Replacement of Jaydess® |
Replacement of Jaydess® with a new system can be performed on any day of the menstrual cycle. In this case, no additional contraception is required. |
| Switching from another contraceptive method (e.g., combined hormonal contraceptives, implants) |
|
If there are difficulties during insertion and/or unusual pain or bleeding during or after insertion, perforation should be considered and appropriate measures taken, such as performing a physical examination and ultrasound.
The woman should have a follow-up examination 4–6 weeks after insertion to check for the presence of the threads and correct positioning of the system. Physical examination alone (including checking for the presence of threads) may not be sufficient to exclude partial perforation.
Jadelle® can be distinguished from other IUDs by visualization of the silver ring on ultrasound and by the brown-colored removal threads. The T-shaped body of the Jadelle® system contains barium sulfate, which is radiographically visible.
Removal/replacement
Jadelle® is removed by gently pulling on the threads with a surgical forceps. If the threads are not visible but the system is located in the uterine cavity, it can be removed using narrow surgical forceps. This may require cervical dilation or surgical intervention. After removal, Jadelle® should be examined to ensure it is not damaged.
The system should be removed no later than at the end of the three-year period.
Continuation of contraceptive protection after removal
- If the patient wishes to continue using this method, a new system may be inserted immediately after removal of the previous system.
- If the patient does not wish to use the same contraceptive method but pregnancy is not desired, removal of the system should be performed within 7 days of the onset of menstruation, provided the woman has a regular menstrual cycle. If removal occurs at any other time or if the woman does not have regular menstruation, and if the woman had sexual intercourse within the week prior to removal, there is a risk of pregnancy. To ensure contraceptive efficacy, a barrier method of contraception (condoms) should be used at least 7 days before removal. After removal, a new contraceptive method should be started immediately (follow instructions for use of the new contraceptive method).
Additional information on use in specific patient groups
Elderly patients. Use of Jadelle® in women over 65 years of age has not been studied. There are no indications for use of Jadelle® in postmenopausal women.
Patients with hepatic impairment. Use of Jadelle® in women with impaired liver function has not been studied. Use of Jadelle® in women with acute liver disease or liver tumors is contraindicated (see section "Contraindications").
Patients with renal impairment. Use of Jadelle® in women with impaired kidney function has not been studied.
Method of administration
Jadelle® is intended for insertion by a physician under aseptic conditions.
Jadelle® is supplied in a sterile package, which should not be opened until the time of insertion. Do not sterilize. For single use only. If the protective layer of the sterile packaging is torn or damaged, the system must not be used. Do not use after the expiry date stated on the packaging.
Any unused product or waste material should be disposed of in accordance with local requirements.
Jadelle® is supplied with a patient card inserted into the cardboard carton. Complete the patient card and give it to the patient after insertion of the system.
Preparation for insertion
- Examine the patient to identify contraindications to insertion of Jadelle® (see section "Contraindications" and information "Medical examination/consultation" in section "Special precautions for use").
- Insert a speculum, examine the cervix, and then thoroughly clean the cervix and vagina with an appropriate antiseptic solution.
- Use assistant help if necessary.
- Grasp the anterior lip of the cervix with a tenaculum or other uterine stabilizing forceps. If the uterus is retroflexed, grasping the posterior lip of the cervix may be more appropriate. Gently pull the forceps to straighten the cervical canal. The forceps should remain in place, gently pulling the cervix throughout the entire insertion procedure.
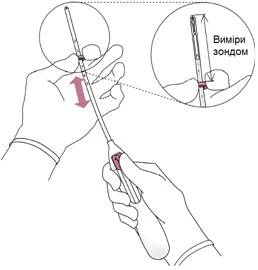
- A uterine sound is inserted through the cervical canal to the fundus to measure depth and determine the direction of the uterine cavity, and to exclude any intrauterine pathology (e.g., septum, submucosal fibroid) or a previously inserted and not removed intrauterine contraceptive device. If resistance is encountered during advancement of the sound, consider the need for cervical dilation. If cervical dilation is required, consider the possibility of using analgesics and/or paracervical block.
Insertion
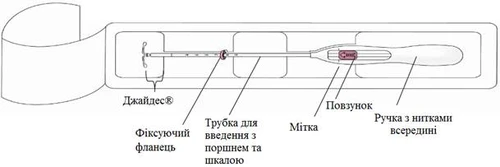
- First, fully open the sterile package (Fig. 1). Proceed with the procedure under aseptic conditions wearing sterile gloves.
Figure 1
|
Figure 2
|
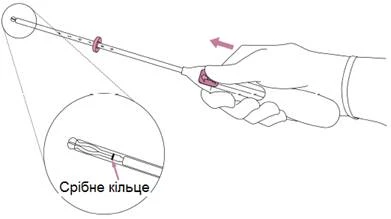
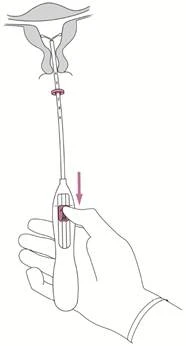
WARNING! Do not pull the slider downward, as this may cause premature activation of the JETREA® system. If this occurs, the JETREA® system can no longer be reinserted into the administration tube.
|
Figure 3
|
|
Figure 4
|
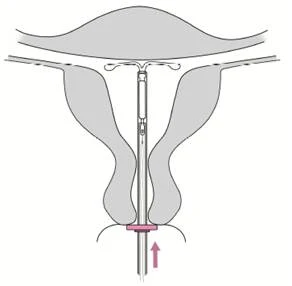
WARNING! Do not forcibly advance the device. If necessary, perform cervical dilation.
|
Figure 5
|
|
Figure 6
|
|
Figure 7
|
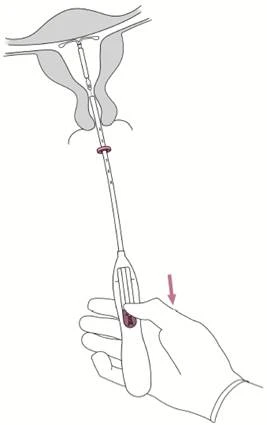
WARNING! If you suspect that the system is not in the correct position, check its placement (e.g., using ultrasound examination). Remove the system if it is not correctly positioned within the uterine cavity. A removed system must not be reinserted.
Removal/replacement
| For removal/replacement, see information in the section "Insertion and Removal/Replacement". The Jaydess® system is removed by pulling the threads with forceps (Figure 8). A new Jaydess® system may be inserted immediately after removal of the previous system. After removal, the Jaydess® system should be checked for integrity. |
Figure 8
|

Children.
The safety and efficacy of the system in women under 18 years of age have not been studied. There are no indications for the use of JADES® system before menarche.
Data on safety and efficacy are presented in section "Pharmacological properties".
Overdose.
Not possible.
Adverse reactions.
In most women, menstrual patterns changed after insertion of the Jaydess® system.
Over time, the frequency of amenorrhea and infrequent bleeding increases, while the frequency of prolonged irregular bleeding decreases.
The following bleeding patterns were observed in clinical trials with the Jaydess® system.
Table 4. Bleeding patterns observed during clinical studies with the Jaydess® system
| Jadges® |
First 90 days |
Next 90 days |
End of 1st year |
End of 3rd year |
| Amenorrhea |
< 1 % |
3 % |
6 % |
12 % |
| Infrequent menstruation |
8 % |
19 % |
20 % |
22 % |
| Frequent menstruation |
31 % |
12 % |
8 % |
4 % |
| Irregular menstruation* |
39 % |
25 % |
18 % |
15 % |
| Extended menstruation* |
55 % |
14 % |
6 % |
2 % |
* Women with prolonged menstruation may also fall into one of the other categories (except amenorrhea).
The frequency of adverse reactions reported during the use of the Jaydess® system is presented in Table 4. Within each frequency group, adverse reactions are listed in order of decreasing severity.
Adverse reactions are classified according to frequency as follows: very common (≥ 1/10), common (≥ 1/100 to < 1/10), uncommon (≥ 1/1000 to < 1/100), rare (≥ 1/10000, < 1/1000), very rare (< 1/10000).
Table 5. Frequency of adverse reactions associated with the Jaydess® system
| System organ class |
Very common |
Common |
Uncommon |
| Psychiatric disorders |
Depressed mood/depression, decreased libido |
||
| Nervous system disorders |
Headache |
Migraine |
|
| Vascular disorders |
Dizziness |
||
| Gastrointestinal disorders |
Abdominal/pelvic pain |
Nausea |
|
| Skin and subcutaneous tissue disorders |
Acne/seborrhea |
Alopecia |
Hirsutism |
| Reproductive system and breast disorders |
Changes in bleeding pattern including increased and decreased menstrual bleeding, intermenstrual bleeding, oligomenorrhea and amenorrhea, ovarian cyst*, vulvovaginitis |
Infections of the upper genital tract, dysmenorrhea, breast pain/tenderness, expulsion (complete and partial) of the system, vaginal discharge |
Uterine perforation** |
| Investigations |
Weight increased |
* Ovarian cysts were reported as adverse reactions in clinical trials when they were of abnormal, non-functional type and/or had a diameter > 3 cm on ultrasound.
** This frequency is based on data from a large prospective comparative non-interventional cohort study involving women using other levonorgestrel-releasing IUDs and copper-containing intrauterine devices. The study showed that breastfeeding at the time of device insertion and insertion within 36 weeks postpartum are independent risk factors for perforation (see section "Special warnings and precautions for use"). In clinical trials with the Jaydess® IUD that did not include breastfeeding women, the frequency of perforation was reported as "rare".
Description of selected adverse reactions
Cases of hypersensitivity, including rash, urticaria, and angioedema, have been reported with use of levonorgestrel-releasing IUDs.
If a woman becomes pregnant while using Jaydess®, the relative risk of ectopic pregnancy increases (see section "Special warnings and precautions for use").
The removal threads of the system may be felt by the partner during sexual intercourse.
The following adverse reactions have been reported in connection with the insertion or removal procedure of Jaydess®: procedural pain, procedure-related bleeding, vasovagal reactions associated with device insertion, dizziness or fainting. The procedure may trigger a seizure in patients with epilepsy.
Cases of sepsis (including sepsis caused by group A streptococcus) have been reported following insertion of intrauterine systems (see section "Special warnings and precautions for use").
Paediatric patients
The safety profile of Jaydess® observed in a study involving 304 adolescents was comparable to that in adults.
Reporting of suspected adverse reactions
Reporting suspected adverse reactions after authorization of the medicinal product is important. It allows continued monitoring of the benefit-risk balance of the medicinal product. Medical and pharmaceutical professionals, as well as patients or their legal representatives, should report any suspected adverse reactions and lack of efficacy via the Automated Pharmacovigilance Information System at the following link: https://aisf.dec.gov.ua.
Shelf life. 3 years.
Storage conditions.
Keep out of the reach of children.
Packaging.
The intrauterine system mounted on the upper part of the insertion device, sealed in an individual blister with one side of the foil easily removable. 1 blister in a cardboard box.
Prescription status.
Prescription only.
Manufacturer.
Bayer Oy, Finland / Bayer Oy, Finland.
Manufacturer's address and location of operations.
Pansiontie 47, 20210, Turku, Finland / Pansiontie 47, 20210, Turku, Finland.