Dexamethasone-darnitsa
Ukraine
Table of Contents
INSTRUCTIONS FOR MEDICAL USE OF THE MEDICINAL PRODUCT DEXAMETHASONE–DARNITSA (DEXAMETHASONE–DARNITSA)
Composition:
Active substance: dexamethasone;
1 ml of solution contains 4 mg of dexamethasone sodium phosphate;
Excipients: disodium phosphate dodecahydrate, potassium dihydrogen phosphate, glycerol, benzyl alcohol, disodium edetate (EDTA disodium), water for injections.
Pharmaceutical form. Injection solution.
Main physicochemical properties: clear, colorless liquid.
Pharmacotherapeutic group. Systemic corticosteroids. Glucocorticoids. Dexamethasone. ATC code H02AB02.
Pharmacological properties.
Pharmacodynamics.
Dexamethasone-Darnytsia is a synthetic adrenal cortex hormone (corticosteroid) exerting glucocorticoid effects. It produces anti-inflammatory and immunosuppressive actions, and also affects energy metabolism, glucose metabolism, and (via negative feedback) the secretion of hypothalamic activation factor and adenohypophyseal tropic hormones.
The mechanism of action of glucocorticosteroids is not yet fully understood. However, sufficient data have been obtained to confirm that glucocorticosteroids act at the cellular level. Within the cell cytoplasm, there are two well-studied receptor systems. By binding to glucocorticoid receptors, glucocorticosteroids exert anti-inflammatory and immunosuppressive effects and regulate glucose metabolism. Through binding to mineralocorticoid receptors, they regulate sodium and potassium metabolism and water-electrolyte balance.
Glucocorticosteroids are lipid-soluble and readily penetrate target cells through the cell membrane. Hormone binding to the receptor induces a conformational change in the receptor, increasing its affinity for DNA. The hormone/receptor complex enters the cell nucleus and binds to a regulatory site on the DNA molecule, known as the glucocorticoid response element (GRE). The activated receptor, bound to GRE or specific genes, modulates mRNA transcription, which may be either increased or decreased. The newly formed mRNA is transported to the ribosome, leading to the synthesis of new proteins. Depending on the target cells and cellular processes, protein synthesis may be enhanced (e.g., tyrosine aminotransferase production in liver cells) or reduced (e.g., IL-2 production in lymphocytes). Since glucocorticosteroid receptors are present in all tissue types, it can be assumed that glucocorticosteroids affect most cells in the body.
Clinical efficacy and safety – COVID-19
Clinical efficacy
An investigator-initiated, individually randomized, controlled, open-label, adaptive platform trial RECOVERY (Randomised Evaluation of Covid-19 Therapy)\textsuperscript{1}, designed to assess outcomes of potential treatments in patients hospitalized with COVID-19.
The trial was conducted in 176 hospitals across the United Kingdom. A total of 6425 patients were randomized to receive either dexamethasone (2104 patients) or usual care (4321 patients). 89% of patients had laboratory-confirmed SARS-CoV-2 infection.
At randomization, 16% of patients were receiving invasive mechanical ventilation (MV) or extracorporeal membrane oxygenation, 60% received oxygen only (with or without non-invasive ventilation), and 24% received neither.
The mean age of patients was 66.1 ± 15.7 years. 36% of patients were women. Medical history included diabetes in 24% of patients, heart disease in 27%, and chronic lung diseases in 21%.
Primary endpoint
Mortality at day 28 was significantly lower in the dexamethasone group compared to the usual care group: 482 out of 2104 patients (22.9%) versus 1110 out of 4321 patients (25.7%), respectively (rate ratio, 0.83; 95% confidence interval (CI), 0.75–0.93; p < 0.001).
Among patients receiving invasive MV, the mortality rate in the dexamethasone group was lower than in the usual care group (29.3% vs. 41.4%; rate ratio, 0.64; 95% CI, 0.51–0.81). Similarly, among patients receiving supplemental oxygen without invasive MV, mortality was lower in the dexamethasone group (23.3% vs. 26.2%; rate ratio, 0.82; 95% CI, 0.72–0.94).
There was no clear benefit of dexamethasone among patients who were not receiving any respiratory support at randomization (17.8% vs. 14.0%; rate ratio, 1.19; 95% CI, 0.91–1.55).
Secondary endpoint
Patients in the dexamethasone group had a shorter duration of hospitalization compared to those in the usual care group (median, 12 days vs. 13 days) and a higher probability of hospital discharge within 28 days (rate ratio, 1.10; 95% CI, 1.03–1.17).
Consistent with the primary endpoint, the greatest reduction in hospitalization duration by day 28 was observed in patients receiving invasive MV at randomization (rate ratio, 1.48; 95% CI, 1.16–1.90), followed by patients receiving oxygen only (rate ratio, 1.15; 95% CI, 1.06–1.24), with no favorable effect observed in patients not receiving oxygen (rate ratio, 0.96; 95% CI, 0.85–1.08).
| Result |
Dexamethasone |
Usual care |
Rate ratio* |
| (N = 2104) |
(N = 4321) |
(95% CI) |
|
| Number/total number of patients (%) |
|||
| Primary endpoint |
482/2104 (22.9) |
1110/4321 (25.7) |
0.83 (0.75–0.93) |
| 28-day mortality |
|||
| Secondary endpoint |
|||
| Discharged from hospital within 28 days |
1413/2104 (67.2) |
2745/4321 (63.5) |
1.10 (1.03–1.17) |
| Invasive ventilation or death†: |
456/1780 (25.6) |
994/3638 (27.3) |
0.92 (0.84–1.01) |
|
102/1780 (5.7) |
285/3638 (7.8) |
0.77 (0.62–0.95) |
|
387/1780 (21.7) |
827/3638 (22.7) |
0.93 (0.84–1.03) |
* The ratio of outcomes was adjusted for age based on 28-day mortality and hospital discharge results. The risk ratios were adjusted for age regarding the outcome of receiving invasive mechanical ventilation or death, and its components;
† Patients who received invasive mechanical ventilation at randomization were excluded from this category.
Safety
During the study, 4 serious adverse events related to the investigational treatment were recorded: 2 cases of hyperglycemia development, 1 case of steroid-induced psychosis, and 1 case of upper gastrointestinal tract bleeding. All cases were resolved.
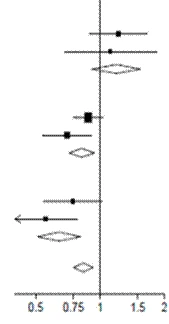
Subgroup Analysis
Effects of dexamethasone administration on 28-day mortality, according to age and respiratory support method received at randomization2
| Dexamethasone |
Usual care |
RR (95% Cl) |
||||||||
| No oxygen (x |
2 |
= 0.70; p=0.40) |
||||||||
| 1 |
||||||||||
| < 70 |
10/197 (5.1%) |
18/462 (3.9%) |
|
|
||||||
| ≥ 70 < 80 |
25/114 (21.9%) |
35/224 (15.6%) |
|
|||||||
| ≥ 80 |
54/190 (28.4%) |
92/348 (26.4%) |
|
|||||||
| Subtotal |
89/501 (17.8%) |
145/1034 (14.0%) |
|
|||||||
| Oxygen only (x |
2 |
= 2.54; p=0.11) |
||||||||
| 1 |
||||||||||
| < 70 |
53/675 (7.9%) |
193/1473 (13.1%) |
|
|||||||
| ≥ 70 < 80 |
104/306 (34.0%) |
178/531 (33.5%) |
|
|||||||
| ≥ 80 |
141/298 (47.3%) |
311/600 (51.8%) |
|
|||||||
| Subtotal |
298/1279 (23.3%) |
682/2604 (26.2%) |
|
|||||||
| Mechanical ventilation (x |
2 |
= 0.28; p=0.60) |
||||||||
| 1 |
||||||||||
| < 70 |
66/269 (24.5%) |
217/569 (38.1%) |
|
|||||||
| ≥ 70 < 80 |
26/49 (53.1%) |
58/104 (55.8%) |
|
|||||||
| ≥ 80 |
3/6 (50.0%) |
8/10 (80.0%) |
|
|||||||
| Subtotal |
95/324 (29.3%) |
283/683 (41.4%) |
|
|||||||
| All participants |
482/2104 (22.9%) |
1110/4321 (25.7%) |
p < 0.001 |
|||||||
| Dexamethasone better |
Usual care better |
|||||||||

Effects of dexamethasone on 28-day mortality, according to the type of respiratory support received at randomization, and in the presence of any chronic comorbidity3
| Dexamethasone |
Usual Care |
RR (95% Cl) |
|||||||||
| No oxygen (x |
2 |
= 0.08; p=0.78) |
|
||||||||
| 1 |
|||||||||||
| Pre-existing comorbidity |
65/313 (20.8%) |
100/598 (16.7%) |
|
||||||||
| Without pre-existing comorbidity |
24/188 (12.8%) |
45/436 (10.3%) |
|
||||||||
| Intermediate total |
89/501 (17.8%) |
145/1034 (14.0%) |
|
||||||||
| Oxygen only (x |
2 |
= 2.05; p=0.15 |
|||||||||
| 1 |
|||||||||||
| Pre-existing comorbidity |
221/702 (31.5%) |
481/1473 (32.7%) |
|
||||||||
| Without pre-existing comorbidity |
77/577 (13.3%) |
201/1131 (17.8%) |
|
||||||||
| Intermediate total |
298/1279 (23.3%) |
682/2604 (26.2%) |
|
||||||||
| Mechanical ventilation (x |
2 |
= 1.52; p=0.22 |
|||||||||
| 1 |
|||||||||||
| Pre-existing comorbidity |
51/159 (32.1%) |
150/346 (43.4%) |
|
||||||||
| Without pre-existing comorbidity |
44/165 (26.7%) |
133/337 (39.5%) |
|
||||||||
| Intermediate total |
95/324 (29.3%) |
283/683 (41.4%) |
|
||||||||
| All participants |
482/2104 (22.9%) |
1110/4321 (25.7%) |
p < 0.001 |
||||||||
| Dexamethasone better |
Usual Care better |
||||||||||

1 www.recoverytrial.net
2, 3 (source: Horby P. et al., 2020; https://www.medrxiv.org/content/10.1101/2020.06.22.20137273v1;
doi: https://doi.org/10.1101/2020.06.22.20137273).
Pharmacokinetics.
Absorption.
Dexamethasone is rapidly absorbed from the site of injection. Maximum plasma concentration is achieved within the first 5 minutes after intravenous administration and within 1 hour after intramuscular administration.
After local administration into a joint or soft tissues (site of inflammation), absorption occurs more slowly compared to injection administration.
With intravenous administration, onset of action is immediate; with intramuscular administration, onset occurs after 8 hours.
The medicinal product belongs to long-acting glucocorticosteroids. The effect lasts 17–28 days after intramuscular administration and from 3 days to 3 weeks after local administration.
Distribution.
In plasma, approximately 77% of dexamethasone is protein-bound, primarily to albumin. Only a small amount of dexamethasone binds to other proteins. Dexamethasone is lipophilic, therefore it freely penetrates into cells and interstitial space. In the central nervous system (hypothalamus, pituitary gland), it binds and acts via membrane receptors. In peripheral tissues, it binds and acts via cytoplasmic receptors.
Biotransformation.
Dexamethasone metabolism occurs at the site of action, i.e., within the cell itself. Dexamethasone is primarily metabolized in the liver, and possibly also in the kidneys and other tissues.
Elimination.
The biological half-life of dexamethasone is 24–72 hours. Approximately 80% of administered dexamethasone is eliminated by the kidneys as glucuronide within 24 hours.
Clinical characteristics.
Indications.
Dexamethasone is administered intravenously or intramuscularly in emergency situations and when oral administration is not feasible.
Endocrine disorders:
- Replacement therapy for primary or secondary (pituitary) adrenal insufficiency (except in acute adrenal insufficiency, where hydrocortisone or cortisone are more suitable due to their stronger mineralocorticoid effect);
- Acute adrenal insufficiency (hydrocortisone or cortisone are drugs of choice; concomitant use with mineralocorticoids may be necessary, especially when using synthetic analogs);
- Preoperatively and in cases of severe trauma or illness in patients with established adrenal insufficiency or uncertain adrenocortical reserve;
- Shock unresponsive to conventional therapy, with known or suspected adrenal insufficiency;
- Congenital adrenal hyperplasia;
- Non-purulent thyroiditis and severe forms of radiation-induced thyroiditis.
Rheumatological disorders (as adjunctive therapy during periods when basic therapy has failed, i.e., in patients in whom analgesic and anti-inflammatory effects of nonsteroidal anti-inflammatory drugs have been unsatisfactory):
- Rheumatoid arthritis, including juvenile rheumatoid arthritis and extra-articular manifestations of rheumatoid arthritis (rheumatoid lung, cardiac, ocular, and cutaneous vasculitis);
- Synovitis in osteoarthritis; post-traumatic osteoarthritis; epicondylitis; acute nonspecific tenosynovitis; acute gouty arthritis; psoriatic arthritis; ankylosing spondylitis; systemic connective tissue diseases; vasculitis.
Skin disorders:
- Pemphigus; severe erythema multiforme (Stevens-Johnson syndrome); exfoliative dermatitis; bullous dermatitis herpetiformis; severe forms of exudative erythema; nodular erythema; severe forms of seborrheic dermatitis; severe forms of psoriasis; urticaria unresponsive to standard treatment; mycosis fungoides; dermatomyositis.
Allergic disorders (unresponsive to conventional therapy):
- Bronchial asthma; contact dermatitis; atopic dermatitis; serum sickness; chronic or seasonal allergic rhinitis; drug allergy; transfusion-related urticaria.
Ophthalmic disorders:
- Inflammatory eye diseases (acute central choroiditis, optic neuritis); allergic disorders (conjunctivitis, uveitis, scleritis, keratitis, iritis); systemic immune disorders (sarcoidosis, temporal arteritis); proliferative changes in the orbit (endocrine ophthalmopathy, pseudotumor); immunosuppressive therapy in corneal transplantation. The solution may be administered systemically or locally (subconjunctival, retrobulbar, or parabulbar injection).
Gastrointestinal disorders:
- To manage critical periods in: ulcerative colitis (severe course), Crohn's disease (severe course); chronic autoimmune hepatitis; rejection reaction following liver transplantation.
Respiratory disorders:
- Symptomatic sarcoidosis (symptomatic); acute toxic bronchiolitis; chronic bronchitis and asthma (during exacerbation); focal or disseminated pulmonary tuberculosis (in combination with appropriate antituberculosis therapy); berylliosis (granulomatous inflammation); radiation or aspiration pneumonitis.
Hematological disorders:
- Acquired or congenital chronic aplastic anemia; autoimmune hemolytic anemia;
- Secondary thrombocytopenia in adults; erythroblastopenia; acute lymphoblastic leukemia (induction therapy); idiopathic thrombocytopenic purpura in adults (intravenous administration only – intramuscular administration is contraindicated).
Kidney disorders:
- Immunosuppressive therapy in kidney transplantation; stimulation of diuresis or reduction of proteinuria in idiopathic nephrotic syndrome (without uremia) and renal dysfunction in systemic lupus erythematosus.
Malignant neoplastic disorders:
- Palliative treatment of leukemia and lymphoma in adults; acute leukemia in children; hypercalcemia associated with malignancy.
Cerebral edema:
- Cerebral edema due to primary or metastatic brain tumors, craniotomy, and traumatic brain injury.
Shock:
- Shock unresponsive to conventional treatment; shock in patients with adrenal cortex insufficiency; anaphylactic shock (intravenous after epinephrine administration); preoperative use to prevent shock in suspected or confirmed adrenal insufficiency.
Coronavirus disease 2019 (COVID-19):
- Treatment of coronavirus disease 2019 (COVID-19) in adults and adolescent patients (aged 12 years and older with body weight ≥40 kg) who require supplemental oxygen therapy.
Other indications:
- Tuberculous meningitis with subarachnoid block (in combination with appropriate antituberculosis therapy); trichinellosis with neurological symptoms or myocardial involvement; cystic tumor of aponeurosis or tendon (ganglion).
Indications for intra-articular or soft tissue injection:
- Rheumatoid arthritis (severe inflammation of a single joint); ankylosing spondylitis (when inflamed joints are unresponsive to conventional therapy); psoriatic arthritis (oligoarticular form and tenosynovitis); monoarthritis (after evacuation of synovial fluid); osteoarthritis of joints (only in cases of synovitis and effusion); periarticular rheumatism (epicondylitis, tenosynovitis, bursitis); acute and gouty arthritis.
Local injection (into the affected site):
- Keloid lesions; hypertrophic, inflammatory, and infiltrated lesions in lichen planus, psoriasis, granuloma annulare, sclerosing folliculitis, discoid lupus, and cutaneous sarcoidosis; discoid lupus erythematosus; Urbach-Wiethe disease; localized alopecia.
Contraindications.
- Hypersensitivity to the active substance or to any of the excipients.
- Acute viral, bacterial, or systemic fungal infections (unless appropriate therapy is administered).
- Vaccination with live vaccines.
- Cushing's syndrome.
- Intramuscular injection is contraindicated in patients with severe coagulation disorders.
- In case of local application – bacteremia, systemic fungal infections, infections at the site of application, including septic arthritis due to gonorrhea or tuberculosis, and in patients with unstable joints.
Interaction with other medicinal products and other forms of interaction.
When dexamethasone is used concomitantly with other medicinal products, the following interactions are possible:
With CYP3A4 enzyme inhibitors (e.g., ketoconazole, macrolide antibiotics) – increased plasma concentration of dexamethasone; ketoconazole may suppress adrenal synthesis of glucocorticoids, thus adrenal insufficiency may develop due to decreased dexamethasone concentration;
With aminoglutethimide, ephedrine, adrenal cortex function inhibitors (e.g., mitotane), carbamazepine, primidone, rifampicin, rifabutin, phenobarbital, phenytoin – reduced efficacy of dexamethasone; dose adjustment (increase) of dexamethasone may be required when used concomitantly;
With azathioprine, antipsychotics, other glucocorticoids, carbutoamide – increased risk of cataract development;
With albendazole, heparin, potassium-depleting diuretics, cyclosporine – enhanced effect of the latter; seizures may occur when cyclosporine and glucocorticoids are used together;
With amphotericin B, β2-adrenergic agonists, potassium-depleting drugs (e.g., diuretics) – increased risk of hypokalemia, which may lead to cardiac failure; concomitant use of amphotericine B and glucocorticoids also increases the risk of osteoporosis;
With antihypertensive agents, natriuretic agents, praziquantel, hypoglycemic agents, salicylates, somatotropin (at high doses) – reduced efficacy of the latter; when dexamethasone and salicylates are used together, dose reduction of dexamethasone should be done cautiously, as increased plasma salicylate concentration and salicylate toxicity may occur;
With antihistamines, M-cholinergic blockers, nitrates, tricyclic antidepressants – risk of increased intraocular pressure; concomitant use of tricyclic antidepressants and glucocorticoids also increases the risk of depression;
With anticholinesterase agents – increased risk of severe weakness in patients with myasthenia gravis;
With vitamin D – reduced effect of the latter on intestinal calcium absorption;
With thyroid hormones – increased clearance of glucocorticoids;
With isoniazid, mexiletine – decreased plasma concentration of the latter due to enhanced metabolism;
With immunosuppressants – increased risk of infections, lymphoma, or other Epstein-Barr virus-related lymphoproliferative disorders;
With carbonic anhydrase inhibitors – increased risk of osteoporosis;
With indomethacin – enhanced toxic effects of dexamethasone (due to displacement from albumin binding);
With live antiviral vaccines and other forms of immunization – increased risk of viral reactivation and infection;
With coumarin anticoagulants – altered effect of the latter; prothrombin time should be monitored when used concomitantly;
With muscle relaxants – enhanced intensity and duration of muscle blockade due to glucocorticoid-induced hypokalemia;
With nonsteroidal anti-inflammatory drugs, ethanol – increased risk of gastrointestinal bleeding and ulcer formation;
With paracetamol – enhanced risk of hepatotoxic effects of paracetamol due to induction of "hepatic" enzymes and formation of its toxic metabolite;
With drugs metabolized by CYP3A4 (indinavir, erythromycin) – decreased concentration of the latter due to increased clearance;
With ritodrine – possible development of pulmonary edema; fatal outcomes in parturients have been reported; concomitant use of ritodrine and dexamethasone is contraindicated during labor;
With cardiac glycosides – risk of cardiac arrhythmias in patients with hypokalemia and enhanced toxic effects of glucocorticoids;
With steroidal hormonal drugs (e.g., androgens, anabolics, estrogens, oral contraceptives) – acne and hirsutism may occur; estrogens and oral contraceptives enhance therapeutic and toxic effects of glucocorticoids by reducing glucocorticoid clearance;
With thalidomide – increased risk of toxic epidermal necrolysis.
Ergocalciferol and parathyroid hormone counteract glucocorticoid-induced osteopathy.
Interactions with therapeutic benefits: concomitant administration of dexamethasone with metoclopramide, diphenhydramine, prochlorperazine, or 5-HT3 receptor antagonists (serotonin or 5-hydroxytryptamine type 3 receptors, such as ondansetron or granisetron) is effective in preventing nausea and vomiting induced by chemotherapy with cisplatin, cyclophosphamide, methotrexate, or fluorouracil.
Interactions between dexamethasone and all the above-mentioned medicinal products may interfere with the dexamethasone suppression test. This should be considered when interpreting test results.
Antacids reduce dexamethasone absorption in the stomach. The effect of dexamethasone when taken with food and alcohol has not been studied, but concomitant use of the drug with food high in sodium is not recommended.
Smoking does not affect the pharmacokinetics of dexamethasone.
Special precautions for use.
Before and during glucocorticoid therapy, a complete blood count should be performed, and blood glucose levels and plasma electrolyte concentrations should be monitored.
During treatment with dexamethasone (especially prolonged therapy), ophthalmological monitoring is required, along with regular control of arterial pressure and water-electrolyte balance, particularly serum potassium levels, as well as peripheral blood picture and blood glucose levels.
During parenteral corticosteroid therapy, hypersensitivity reactions may occur in isolated cases. Therefore, appropriate precautions should be taken before initiating dexamethasone treatment, considering the possibility of allergic reactions (especially in patients with a history of allergic reactions to any other drugs).
When discontinuing the drug after prolonged use, withdrawal syndrome may develop (without apparent signs of adrenal insufficiency), with symptoms such as fever, rhinitis, conjunctival hyperemia, headache, dizziness, drowsiness or irritability, lethargy, muscle and joint pain, nausea, vomiting, weight loss, general weakness, and seizures. Therefore, the dose of dexamethasone should be tapered gradually. Sudden discontinuation may result in fatal outcomes.
If a patient experiences severe stress (due to trauma, surgery, or serious illness) during or after termination of dexamethasone therapy, the dose should be increased or hydrocortisone or cortisone should be administered.
Patients who have received prolonged dexamethasone treatment and experience severe stress after stopping therapy should resume dexamethasone, as induced adrenal insufficiency may persist for several months after discontinuation of treatment.
Treatment with dexamethasone or natural glucocorticosteroids may mask symptoms of existing or newly developed infections, as well as symptoms of intestinal perforation. During therapy, contact with individuals suffering from colds or other infections should be avoided.
Dexamethasone may cause exacerbation of systemic fungal infections, latent amoebiasis, and pulmonary tuberculosis.
Patients with active pulmonary tuberculosis should receive dexamethasone (in combination with anti-tuberculosis agents) only in cases of fulminant or disseminated pulmonary tuberculosis. Patients with inactive pulmonary tuberculosis receiving dexamethasone, or patients with a positive tuberculin reaction, should receive chemoprophylaxis.
Live vaccination is contraindicated during dexamethasone therapy. Inactivated viral or bacterial vaccines do not elicit the expected antibody response and do not provide adequate protective effect. Dexamethasone should not be administered within 8 weeks before vaccination and should not be initiated earlier than 2 weeks after vaccination.
The drug should be prescribed cautiously to patients with infections, especially varicella and measles, as these diseases may have a more severe course when dexamethasone is used. Therefore, individuals who have not had these diseases should take care to avoid exposure to infection. In case of contact with infected individuals, immediate medical consultation is required. Prophylactic treatment with immunoglobulin is recommended.
Glucocorticosteroids should be used cautiously in patients with herpes simplex eye infections (herpes simplex), as their use may lead to corneal perforation.
Caution and medical supervision are recommended for patients with osteoporosis, arterial hypertension, heart failure, tuberculosis, glaucoma, hepatic or renal insufficiency, diabetes mellitus, gastritis, esophagitis, diverticulitis, active peptic ulcer, recent intestinal anastomosis, colitis, epilepsy, thyrotoxicosis, obesity (III–IV degree), nephrolithiasis, hyperlipidemia, poliomyelitis (except bulbar encephalitis form), hypoalbuminemia, and conditions leading to its development, as well as patients with immunodeficiency states (including AIDS or HIV infection), and lymphadenitis following BCG vaccination.
Special care is required for patients during the first weeks after myocardial infarction, patients with thromboembolism, severe myasthenia gravis, hypothyroidism, psychosis or psychoneurosis, and elderly patients.
During dexamethasone therapy, diabetes mellitus may worsen or latent diabetes may progress to clinical manifestation.
The effect of glucocorticosteroids is enhanced in patients with liver cirrhosis or hypothyroidism.
Patients with disturbances in water-electrolyte balance should use dexamethasone cautiously, as medium and high doses of glucocorticosteroids may cause salt and fluid retention and increased potassium excretion. In such cases, salt restriction and additional potassium supplementation are indicated. All corticosteroids enhance calcium excretion, which may impair mineralocorticoid secretion. Therefore, additional salt and/or mineralocorticoid administration may be required.
Prolonged use of glucocorticosteroids may lead to the development of posterior subcapsular cataracts, glaucoma with optic nerve damage, and increases the risk of secondary viral or fungal ocular infections.
Caution is recommended for patients recovering from surgery or bone fractures, as dexamethasone may delay wound healing and bone tissue formation.
Systemic corticosteroids should not be discontinued in patients who are already receiving systemic (oral) corticosteroids for other reasons (e.g., patients with chronic obstructive pulmonary disease) and do not require additional oxygen.
Particular attention should be paid to the use of systemic glucocorticosteroids in patients with severe affective disorders, including depression, manic-depressive psychosis, previous steroid-induced psychosis, including those with such disorders in their history. Patients and/or caregivers should be warned about the possibility of serious psychiatric side effects. Symptoms usually appear within several days or weeks after starting treatment. The risk of these side effects is higher with high-dose regimens. Most reactions resolve after dose reduction or discontinuation of the drug, although specific treatment may sometimes be necessary.
Psychiatric status should be monitored, and changes such as depressive mood, suicidal thoughts, and intentions should be promptly identified. Corticosteroids should be used with particular caution in patients with a history of affective disorders, especially those with a history of allergic reactions to any other drugs or in their close relatives. Medical consultation is required if such symptoms develop. Psychiatric disorders may also occur during glucocorticosteroid withdrawal.
Glucocorticosteroids may distort the results of skin allergy tests.
Hypertrophic cardiomyopathy has been reported after systemic corticosteroid use in preterm infants. This phenomenon is mostly reversible after discontinuation of treatment. Diagnostic evaluation and monitoring of cardiac function and structure are recommended in preterm infants who have received systemic dexamethasone.
Children may be treated with dexamethasone only when clearly indicated. Careful monitoring of growth and development is required during dexamethasone therapy in children.
There is evidence of long-term neurological side effects after early treatment (<96 hours) of preterm infants with chronic lung disease using initial doses of 0.25 mg/kg twice daily.
Intra-articular administration of the drug may lead to local or systemic adverse reactions. Frequent use may cause cartilage damage or bone necrosis.
Before intra-articular injection of dexamethasone, synovial fluid should be aspirated from the joint and examined (to check for infection). The drug should not be used in patients with infected joints. If joint infection develops after injection, appropriate antibiotic therapy should be initiated.
Frequent intra-articular injections may damage joint tissues. During treatment, patients should avoid excessive loading of affected joints until complete resolution of inflammation, even if symptomatic improvement occurs.
The drug should be discontinued in patients who experience a significant increase in pain accompanied by swelling, further limitation of joint mobility, fever, and general malaise after intra-articular glucocorticosteroid injection (these symptoms indicate the development of septic arthritis). In case of septic arthritis and confirmed diagnosis of sepsis, appropriate antibacterial therapy must be initiated.
Pheochromocytoma crisis
Development of pheochromocytoma crisis, which may lead to fatal outcomes, has been reported after systemic corticosteroid therapy. Corticosteroids should be prescribed to patients with suspected or diagnosed pheochromocytoma only after appropriate benefit-risk assessment.
Excipients
This medicinal product contains less than 1 mmol (23 mg)/dose of sodium, i.e., essentially "sodium-free."
Use during pregnancy or breastfeeding.
Pregnancy.
Glucocorticosteroids cross the placenta and reach high concentrations in the fetus. Harmful effects on the fetus and newborn infant cannot be excluded. Dexamethasone suppresses intrauterine fetal development. According to some data, even pharmacological doses of glucocorticosteroids may increase the risk of placental insufficiency, oligohydramnios, delayed fetal development or intrauterine death, elevated leukocyte (neutrophil) counts in the fetus, and adrenal insufficiency. Data on the teratogenic effects of dexamethasone are lacking. Infants born to mothers who received glucocorticosteroids during pregnancy should be carefully examined for signs of adrenal insufficiency.
Some studies have also shown an increased risk of neonatal hypoglycemia after prenatal short-term corticosteroid use in women at risk of late preterm delivery.
The drug should be used only in emergency situations when the expected benefit to the mother outweighs the potential risk to the fetus.
Particular caution is recommended in preeclampsia. According to general recommendations, the lowest effective dose should be used during pregnancy to control the underlying condition.
Women who received glucocorticosteroids during pregnancy are recommended to receive additional doses during labor. In cases of prolonged labor or planned cesarean section, intravenous administration of 100 mg hydrocortisone every 8 hours is recommended.
Breastfeeding.
The drug is contraindicated during breastfeeding (except in emergency situations).
Glucocorticosteroids are excreted in breast milk. Breastfeeding is not recommended during dexamethasone use, especially at doses exceeding physiological levels (approximately 1 mg), as this may lead to impaired infant growth and reduced secretion of endogenous corticosteroids.
Ability to influence reaction rate when driving or operating machinery.
No data are available; however, the possibility of adverse reactions affecting the nervous system and visual organs should be considered.
Administration and Dosage.
The medicinal product is intended for use in adults and children from birth.
It should be administered intravenously (by injection or infusion), intramuscularly, or locally—via intra-articular injections or injections into the affected skin area or soft tissue infiltrate. For intravenous infusion, 0.9% sodium chloride solution or 5% glucose solution should be used as a solvent.
When administering to infants, especially premature newborns, solutions intended for intravenous administration or for further dilution of the medicinal product must not contain preservatives.
When mixing the medicinal product with an infusion solvent, aseptic techniques must be strictly followed. The prepared mixture should be used within 24 hours, as infusion solutions generally do not contain preservatives.
Parenteral medicinal products should be visually inspected for particulate matter and discoloration prior to each administration.
The dose of the medicinal product should be individually determined based on the patient's specific condition, duration of treatment, tolerance to glucocorticoids, and individual response.
Adults.
The medicinal product should be administered parenterally in emergency situations when oral therapy is not feasible, and in cases indicated in the "Indications" section.
Intravenous and intramuscular administration.
The initial dose of the medicinal product ranges from 0.5 to 9 mg per day; the dose may be increased if necessary.
Initial doses of dexamethasone should be maintained until a clinical response is achieved, after which the dose should be gradually reduced to the lowest clinically effective dose. When high doses are used for more than several days, the dose should be tapered gradually over several subsequent days or even over a longer period.
Local administration.
The medicinal product is typically administered in doses of 0.2–4 mg, specifically:
- large joints (e.g., knee) – 2–4 mg;
- small joints (e.g., interphalangeal, temporomandibular) – 0.8–1 mg;
- bursae – 2–3 mg;
- tendon sheaths – 0.4–1 mg;
- soft tissue infiltration – 2–6 mg;
- ganglia – 1–2 mg.
Repeat intra-articular injections may be performed after 3–4 months. A maximum of 3 or 4 injections into a single joint are recommended over a lifetime. More frequent intra-articular administration may damage joint cartilage and lead to bone necrosis. Intra-articular injections should not be administered into more than 2 joints simultaneously.
The dose of dexamethasone administered at a site of injury is considered equivalent to an intra-articular dose. Dexamethasone should not be administered into more than 2 injury sites simultaneously.
Intra-articular injections of glucocorticosteroids may lead to systemic reactions in addition to local effects.
Intra-articular administration of glucocorticosteroids should be avoided in infected joints, as well as in unstable or deformed joints.
Children.
Replacement therapy: the medicinal product should be administered at a dose of 0.02 mg/kg body weight (0.67 mg/m² body surface area) per day in 3 divided doses, or 0.008–0.01 mg/kg body weight (0.2–0.3 mg/m² body surface area).
Other indications: the medicinal product should be administered at a dose of 0.02–0.1 mg/kg (0.8–5 mg/m² body surface area) every 12–24 hours.
For the treatment of COVID-19:
Adults and children (adolescents aged 12 years and older with body weight of at least 40 kg): 6 mg of dexamethasone intravenously once daily for up to 10 days.
The duration of treatment is determined individually based on the patient's clinical condition.
Elderly patients, and those with impaired renal or hepatic function.
Dose adjustment is not required.
For comparison, the following table lists equivalent doses of various glucocorticosteroids in milligrams:
| Dexamethasone 0.75 mg |
Prednisone 5 mg |
| Cortisone 25 mg |
Methylprednisolone 4 mg |
| Hydrocortisone 20 mg |
Triamcinolone 4 mg |
| Prednisolone 5 mg |
Betamethasone 0.75 mg |
Children
The medicinal product should be used during the neonatal period only if absolutely necessary. Careful monitoring of growth and development of children and adolescents is required during dexamethasone treatment.
Overdose
Symptoms: There have been isolated reports of acute overdose or fatal outcomes due to acute overdose. Overdose (usually occurring only after several weeks of excessive dosing) manifests as an exacerbation of the described adverse effects, particularly: Cushing's syndrome, acne, ecchymoses, hirsutism, nausea, anorexia, peptic ulcer of the gastrointestinal tract, arthralgia, myopathy, myalgia, dyspnea, dizziness, loss of consciousness, fever, increased arterial pressure, hyperlipidemia, osteoporosis, orthostatic hypotension, development of infections, steroid-induced diabetes, "moon face," sexual dysfunction.
Treatment: symptomatic and supportive therapy. There is no specific antidote. Hemodialysis is not effective.
Adverse Reactions
The frequency of adverse reactions depends on the dose and duration of treatment.
Adverse Reactions During Short-Term Treatment
Gastrointestinal system: Peptic ulcer, acute pancreatitis.
Endocrine system: Transient suppression of adrenal function.
Metabolism and nutritional disorders: Decreased carbohydrate tolerance, increased appetite, weight gain, hypertriglyceridemia.
Psychiatric disorders: Psychiatric disorders.
Immune system disorders: Hypersensitivity reactions.
Adverse Reactions During Long-Term Treatment
Eye disorders: Cataract, glaucoma.
Endocrine system: Prolonged suppression of adrenal function, growth retardation in children, premature closure of epiphyseal growth zones.
Metabolism and nutritional disorders: Obesity.
Cardiovascular system: Arterial hypertension, telangiectasia.
Immune system disorders: Reduced immune response and increased susceptibility to infectious diseases.
Skin and subcutaneous tissue disorders: Skin thinning.
Musculoskeletal and connective tissue disorders: Muscle atrophy, osteoporosis, long bone fractures, aseptic bone necrosis.
Adverse Reactions That May Occur in Individual Organs and Systems During Dexamethasone Treatment
Eye disorders: Increased intraocular pressure, glaucoma, cataract, exophthalmos, papilledema, corneal or scleral thinning, retrolental fibroplasia, exacerbation of viral or fungal ophthalmic infections.
Respiratory, thoracic and mediastinal disorders: Pulmonary edema.
Gastrointestinal disorders: Nausea, vomiting, dyspepsia, hiccups, flatulence, esophagitis, candidiasis of the esophagus, increased or decreased appetite; rarely – peptic ulcers of the stomach and duodenum, possible ulcer perforations and gastrointestinal bleeding (hematemesis, melena), pancreatitis, gallbladder or intestinal perforation (especially in patients with chronic bowel inflammation), gastrointestinal atony.
Hepatobiliary disorders: Increased liver enzyme levels, hepatomegaly.
Endocrine disorders: Suppression of function and atrophy of adrenal glands (reduced stress response), suppression of the hypothalamic-pituitary-adrenal system, Cushing's syndrome, delayed sexual development in children, impaired sex hormone secretion (menstrual cycle disturbances, amenorrhea, hirsutism, impotence), hyperglycemia, "steroid" diabetes mellitus, transition of latent diabetes to clinically active form, reduced carbohydrate tolerance, increased insulin requirement or need for oral antidiabetic drugs in diabetic patients.
Metabolism and nutritional disorders: Increased excretion of calcium ions, hypocalcemia, weight gain, negative nitrogen balance (increased protein breakdown), fluid and sodium ion retention (peripheral edema), hypernatremia, increased excretion of potassium ions, hypokalemic syndrome: hypokalemia, hypokalemic alkalosis, arrhythmia, myalgia or muscle cramps, tumor lysis syndrome.
Nervous system disorders: After treatment, optic disc edema and increased intracranial pressure (pseudotumor) may occur; exacerbation of epilepsy, dizziness, fainting, convulsions, headache, hyperkinesia, neuritis, neuropathy, paresthesia; in children, the drug may cause cerebral cortex paralysis.
Psychiatric disorders: Personality and behavioral changes, often manifesting as affective disorders (irritability, euphoria, delirium, paranoia, nervousness, anxiety, disorientation, depression, mood lability, suicidal thoughts), sleep disturbances, cognitive dysfunction (including confusion and amnesia), psychotic reactions (including mania, hallucinations, psychosis, and exacerbation of schizophrenia).
Cardiovascular disorders: Paroxysmal bradycardia, cardiac arrest, cardiac arrhythmias, angina attack, enlarged heart, vascular insufficiency, congestive heart failure, chronic heart failure, fat embolism, arterial hypertension, hypertrophic cardiomyopathy in premature infants; very rarely – cardiac rupture in patients who recently suffered myocardial infarction; also possible: multifocal ventricular extrasystoles, hypertensive encephalopathy, tachycardia, thromboembolism, thrombophlebitis, vasculitis.
Blood and lymphatic system disorders: Cases of thromboembolism, thrombophlebitis, decreased number of monocytes and/or lymphocytes, leukocytosis, eosinophilia (as with other glucocorticoids), rarely – thrombocytopenia and non-thrombocytopenic purpura.
Immune system disorders: Hypersensitivity reactions, including rash, pruritus, hyperemia, allergic dermatitis, urticaria, angioedema (Quincke's edema), bronchospasm, anaphylactic shock, immunosuppression.
Skin and subcutaneous tissue disorders: Suppression of skin regenerative and reparative functions, delayed wound healing, thin and sensitive skin, dry skin, skin atrophy, hyper- or hypopigmentation, altered subcutaneous fat distribution, ecchymosis, sterile abscess, petechiae, acne, striae, telangiectasia, suppressed response to skin tests and vaccinations.
Musculoskeletal and connective tissue disorders: Muscle weakness, muscle atrophy, steroid myopathy (muscle weakness causing muscle catabolism), osteoporosis (increased calcium excretion), long bone fractures or vertebral compression fractures, aseptic osteonecrosis (most commonly of femoral and humeral heads), tendon ruptures (especially when co-administered with certain quinolones), growth retardation and impaired bone mineralization in children, premature closure of epiphyseal growth zones.
General disorders and administration site reactions: Hypersensitivity reactions, including rash, pruritus, hyperemia, and skin tingling; painless joint destruction clinically resembling neurogenic arthropathy (Charcot joint).
Other: Unusual weakness and increased fatigue, increased risk of developing or exacerbating fungal, viral, or bacterial infections, development of opportunistic infections, suppression of regenerative and reparative processes, edema, increased sweating, leukocyturia, withdrawal syndrome. The drug may cause physical dependence.
Signs of Glucocorticosteroid Withdrawal Syndrome
In patients treated with dexamethasone for a prolonged period, a very rapid dose reduction may lead to withdrawal syndrome and cause adrenal insufficiency, arterial hypotension, and potentially fatal outcomes. In some cases, withdrawal symptoms may resemble signs of worsening or relapse of the disease being treated.
Shelf Life. 2 years.
Storage Conditions.
Store in original packaging at a temperature not exceeding 15 °C. Do not freeze. Keep out of reach of children.
Incompatibility.
Concomitant use of ritodrine and dexamethasone is contraindicated, as it may lead to pulmonary edema. Fatal outcomes in postpartum women due to this condition have been reported.
Packaging.
1 ml in ampoule; 5 ampoules in a blister pack; 2 blister packs in a carton; 5 or 10 ampoules in a blister pack; 1 blister pack in a carton.
Prescription Category. Prescription only.
Manufacturer. JSC "Pharmaceutical Company "Darnitsya".
Manufacturer's Address and Place of Business.
13, Boryspilska Street, Kyiv, 02093, Ukraine.