Bufomix isiheiler
Ukraine
Table of Contents
INSTRUCTIONS FOR MEDICAL USE OF THE MEDICINAL PRODUCT BUFOMIX EASYHALER
Composition:
Active substances: 1 dose contains budesonide 160 mcg and formoterol fumarate dihydrate 4.5 mcg;
Excipient: lactose monohydrate.
Pharmaceutical form. Powder for inhalation.
Main physicochemical properties: white or yellowish-white powder.
Pharmacotherapeutic group.
Medicinal products used in obstructive airway diseases.
Adrenergic agents in combination with corticosteroids or other agents, excluding anticholinergic agents. Formoterol and budesonide. ATC code R03A K07.
Pharmacological Properties.
Pharmacodynamics.
Mechanisms of Action and Pharmacodynamic Effects
Bucomix Easyhaler contains formoterol and budesonide, which have different mechanisms of action and demonstrate additive effects in reducing asthma exacerbations. The specific properties of budesonide and formoterol allow the combination to be used for maintenance treatment and symptom relief or for maintenance therapy of bronchial asthma.
Budesonide. Budesonide is a glucocorticosteroid that, when inhaled, exerts a dose-dependent anti-inflammatory action in the airways, resulting in reduced symptoms of bronchial asthma. Inhaled budesonide is associated with fewer adverse effects compared to systemic corticosteroids. The precise mechanism of the anti-inflammatory effect of glucocorticosteroids is unknown.
Formoterol. Formoterol is a selective β2-adrenergic receptor agonist that, when inhaled, provides rapid and prolonged relaxation of bronchial smooth muscle in patients with reversible airway obstruction. The bronchodilating effect is dose-dependent and occurs within 1–3 minutes. The duration of effect lasts for at least 12 hours after a single dose.
Clinical Efficacy and Safety
Bronchial Asthma
Studies in adult patients have shown that adding formoterol to budesonide alleviates symptoms of bronchial asthma, improves lung function, and reduces the frequency of exacerbations.
The use of budesonide/formoterol for maintenance treatment and symptom relief provided a statistically significant and clinically relevant reduction in the rate of severe asthma exacerbations compared to all comparator groups and other therapies.
In patients seeking medical help due to acute asthma symptoms, the use of budesonide/formoterol provided rapid and effective relief of bronchospasm symptoms similar to that achieved with salbutamol or formoterol.
Chronic Obstructive Pulmonary Disease (COPD)
In two 12-month studies, the effect of the drug on lung function and the frequency of exacerbations (defined by the number of courses of oral steroids and/or antibiotics and/or hospitalizations) was evaluated in patients with moderate to severe COPD. The inclusion criterion for both studies was a pre-bronchodilator FEV1 value of <50% of predicted normal. The median post-bronchodilator FEV1 at study entry was 42% of predicted normal.
The mean number of exacerbations per year (as defined above) was significantly reduced in the budesonide/formoterol group compared to formoterol monotherapy or placebo (mean rate 1.4 vs. 1.8–1.9 in the placebo/formoterol groups). The mean number of days of oral corticosteroid use per patient over 12 months was slightly reduced in the budesonide/formoterol group (7–8 days/patient/year compared to 11–12 and 9–12 days in the placebo and formoterol groups, respectively). Regarding changes in lung function parameters such as FEV1, treatment with budesonide/formoterol did not exceed that of formoterol alone.
Pharmacokinetics.
Absorption
Fixed-dose combinations of budesonide and formoterol have been shown to be bioequivalent to the corresponding monoproducts with respect to systemic exposure to budesonide and formoterol, respectively. Despite this, a slight suppression of cortisol was observed after administration of the fixed-dose combination compared to the monoproducts. This difference is considered not to affect clinical efficacy.
There is no evidence of pharmacokinetic interactions between budesonide and formoterol.
The pharmacokinetic parameters of budesonide and formoterol were comparable after administration as monoproducts or as a fixed-dose combination. For budesonide, the area under the concentration-time curve (AUC) and absorption rate were slightly higher, and the maximum plasma concentration (Cmax) was higher after administration of the fixed combination. For formoterol, Cmax was similar after administration of the fixed combination. Inhaled budesonide is rapidly absorbed, with Cmax reached within 30 minutes after inhalation. In studies, the mean lung deposition of budesonide after inhalation via a dry powder inhaler ranged from 32% to 44% of the delivered dose. Systemic bioavailability was approximately 49% of the delivered dose. In children aged 6 to 16 years, lung deposition is within the same range as in adults when the same nominal dose is administered. Resulting plasma concentrations were not detectable.
Inhaled formoterol is rapidly absorbed, with Cmax reached within 10 minutes after inhalation. In studies, the mean lung deposition of formoterol after inhalation via a dry powder inhaler ranged from 28% to 49% of the delivered dose. Systemic bioavailability was approximately 61% of the delivered dose.
Distribution and Metabolism
Plasma protein binding is approximately 50% for formoterol and 90% for budesonide. The volume of distribution is approximately 4 L/kg for formoterol and 3 L/kg for budesonide. Formoterol is inactivated via conjugation reactions (active O-demethylated and deformylated metabolites are formed, but they are predominantly observed as inactivated conjugates). Budesonide undergoes extensive (approximately 90%) first-pass metabolism in the liver to metabolites with low glucocorticosteroid activity. The glucocorticosteroid activity of the main metabolites—6-β-hydroxybudesonide and 16-α-hydroxyprednisolone—is less than 1% of that of budesonide. There are no indications of any metabolic interactions or displacement reactions between formoterol and budesonide.
Elimination
The majority of the formoterol dose is transformed via hepatic metabolism, followed by renal excretion. After inhalation, 8–13% of the delivered dose of formoterol is excreted in urine in unchanged form. Formoterol has a high systemic clearance (approximately 1.4 L/min), and the terminal half-life averages 17 hours.
Budesonide is eliminated via metabolism, primarily catalyzed by the CYP3A4 enzyme. Budesonide metabolites are excreted in urine either in free form or as conjugates. Only very low amounts of unchanged budesonide are detected in urine. Budesonide has a high systemic clearance (approximately 1.2 L/min), and the elimination half-life from plasma after intravenous administration is 4 hours.
The pharmacokinetics of budesonide or formoterol in patients with renal impairment is unknown. The effects of budesonide and formoterol may be increased in patients with hepatic disease.
Linearity/Non-linearity
Systemic exposure to budesonide and formoterol is linearly correlated with the administered dose.
Clinical characteristics.
Indications.
Bronchial asthma
Budamex Easyhaler is indicated for adults and adolescents (aged 12 years and older) for regular treatment of bronchial asthma when use of a combination (inhaled corticosteroids and long-acting β2-adrenergic agonists) is appropriate: for patients in whom adequate control is not achieved with inhaled corticosteroids and short-acting β2-adrenergic agonists used on an "as needed" basis, or for patients in whom adequate control has already been achieved with both inhaled corticosteroids and long-acting β2-adrenergic agonists.
COPD
Budamex Easyhaler is indicated for symptomatic treatment in adult patients aged 18 years and older with COPD and forced expiratory volume in 1 second (FEV1) <70% of predicted (post-bronchodilator) and a history of exacerbations despite regular bronchodilator therapy.
Contraindications.
Hypersensitivity to budesonide, formoterol, or lactose (which contains a small amount of milk protein).
Interaction with other medicinal products and other forms of interaction.
Pharmacokinetic interactions
Potent CYP3A4 inhibitors (e.g., ketoconazole, itraconazole, voriconazole, posaconazole, clarithromycin, telithromycin, nefazodone, and HIV protease inhibitors) are highly likely to increase plasma levels of budesonide; therefore, their concomitant use should be avoided. If concomitant use cannot be avoided, the time intervals between administration of these drugs should be as long as possible. Maintenance therapy is not recommended for patients receiving potent CYP3A4 inhibitors.
The potent CYP3A4 inhibitor ketoconazole at a dose of 200 mg once daily increases plasma levels of orally administered budesonide (single dose of 3 mg) by an average of 6-fold. When ketoconazole was administered 12 hours after budesonide, plasma concentrations increased on average only 3-fold, indicating that staggered administration may reduce the increase in plasma levels. Some data suggest that a significant increase in plasma levels of budesonide (on average 4-fold) may occur when inhaled budesonide (single dose of 1000 μg) is used concomitantly with itraconazole at a dose of 200 mg once daily.
Concomitant treatment with drugs containing cobicistat is expected to increase the risk of systemic adverse effects. Combinations should be avoided unless the benefit outweighs the increased risk of systemic corticosteroid adverse effects. In such cases, patients should be monitored for systemic corticosteroid-related adverse effects.
Pharmacodynamic interactions
β-adrenergic blockers may reduce the effect of formoterol. Therefore, Budamex Easyhaler should not be used concomitantly with β-adrenergic blockers (including ophthalmic drops), unless there are compelling reasons.
Concomitant treatment with quinidine, disopyramide, procainamide, phenothiazines, antihistamines (terfenadine), and tricyclic antidepressants may prolong the QTc interval and increase the risk of ventricular arrhythmia.
In addition, levodopa, levothyroxine, oxytocin, and alcohol may impair cardiac tolerance to β2-sympathomimetics.
Concomitant use of monoamine oxidase inhibitors, including medicinal products with similar properties such as furazolidone and procarbazine, may cause hypertensive reactions.
The risk of arrhythmia increases during anesthesia with halogenated hydrocarbons.
Concomitant use of other β-adrenergic agonists or anticholinergic drugs may enhance the bronchodilating effect.
Hypokalemia may increase susceptibility to cardiac arrhythmia in patients treated with digitalis glycosides.
Hypokalemia may occur as a result of β2-agonist therapy and may be potentiated by concomitant use of xanthine derivatives, corticosteroids, and diuretics (see section "Special precautions for use").
No interactions between budesonide and formoterol with any other medicinal products used for the treatment of bronchial asthma have been observed.
Paediatric populations
Drug interaction studies have been conducted only in adults.
Monoamine oxidase inhibitors and tricyclic antidepressants
Budamex Easyhaler should be used with caution in patients receiving monoamine oxidase inhibitors or tricyclic antidepressants, or within 2 weeks after discontinuation of such treatment, because the effects of formoterol (a component of Budamex Easyhaler) on the vascular system may be potentiated by these medicinal products.
Diuretics
ECG changes and/or hypokalemia caused by non-potassium-sparing diuretics (such as loop or thiazide diuretics) may be suddenly exacerbated by β-agonists, particularly in cases of exceeding the recommended dose of β-agonists. Although the clinical significance of these effects is not fully understood, caution is recommended when concomitantly using Budamex Easyhaler and non-potassium-sparing diuretics.
Special precautions for use.
It is recommended to gradually reduce the dose when discontinuing the medication and not to abruptly stop treatment. Inhaled corticosteroids should not be completely withdrawn except in cases where temporary discontinuation is necessary to confirm the diagnosis of bronchial asthma.
If patients find that treatment is ineffective or if there is a need to exceed the maximum recommended dose of Bufomix Easyhaler, they should consult their physician. Sudden or progressive worsening of bronchial asthma or COPD control may be potentially life-threatening, and the patient should seek immediate medical evaluation. In such cases, intensification of corticosteroid therapy, for example with a course of oral corticosteroids, or antibiotic treatment in case of infection, should be considered.
Patients should be advised to always carry their inhaler as a rescue medication: either Bufomix Easyhaler (for patients with bronchial asthma who use Bufomix Easyhaler for maintenance and symptom relief) or a separate short-acting bronchodilator (for all patients using Bufomix Easyhaler as maintenance therapy).
Patients should be reminded to take the maintenance dose of Bufomix Easyhaler as prescribed, even in the absence of symptoms. Once bronchial asthma symptoms are under control, gradual dose reduction of Bufomix Easyhaler should be considered. It is important to regularly monitor patients during dose reduction. The lowest effective dose of Bufomix Easyhaler should be used.
Treatment with this medication should not be initiated during exacerbations, significant worsening, or sudden complications of bronchial asthma.
Serious adverse events and exacerbations related to bronchial asthma may occur during treatment. Patients should be informed of the need to continue treatment and to consult their physician if asthma symptoms are not controlled or worsen after starting Bufomix Easyhaler.
There are no clinical study data on the use of Bufomix Easyhaler in COPD patients with pre-bronchodilator FEV1 >50% of predicted and post-bronchodilator FEV1 <70% of predicted.
As with other forms of inhaled therapy, there is a risk of paradoxical bronchospasm. In such cases, wheezing and shortness of breath increase immediately after dosing. If paradoxical bronchospasm occurs, Bufomix Easyhaler should be discontinued immediately, the patient should be evaluated, and alternative therapy should be considered if necessary. Paradoxical bronchospasm responds to short-acting inhaled bronchodilators and requires immediate treatment.
Systemic effects of inhaled corticosteroids may occur, particularly with prolonged use of high doses. These effects are less likely than with oral corticosteroids. Possible systemic effects include Cushing’s syndrome, Cushingoid appearance, adrenal suppression, growth retardation in children and adolescents, decreased bone mineral density, cataract, glaucoma, and, more rarely, various psychological and behavioral disturbances such as psychomotor hyperactivity, sleep disturbances, anxiety, depression, or aggression (especially in children).
Visual disturbances may occur with both systemic and local corticosteroid use. If a patient reports symptoms such as blurred vision or other visual disturbances, they should be referred to an ophthalmologist for evaluation of possible causes, including cataract, glaucoma, or rare conditions such as central serous chorioretinopathy (CSCR), which has been reported after systemic and topical corticosteroid use.
The potential impact on bone density should be considered, particularly in patients receiving high doses over a prolonged period and those with concomitant risk factors for osteoporosis. Long-term studies of inhaled budesonide in children at mean daily doses of 400 mcg (delivered dose) and in adults at daily doses of 800 mcg (delivered dose) did not show a significant effect on bone mineral density. Information on the effects of high doses is lacking.
Caution is advised when switching patients to Bufomix Easyhaler therapy if there is reason to suspect impaired adrenal cortex function due to prior systemic steroid therapy.
The benefits of inhaled budesonide therapy usually minimize the need for oral steroids; however, patients transitioning from oral steroids may remain at risk of reduced adrenal reserve for a prolonged period. Recovery may take a long time after discontinuation of oral steroid therapy. Therefore, patients previously treated with oral steroids and switched to inhaled budesonide may remain at risk due to adrenal dysfunction for a significant period. In such cases, regular monitoring of the hypothalamic-pituitary-adrenal (HPA) axis function is required.
Long-term treatment with high doses of inhaled corticosteroids, especially when higher than recommended doses are used, may lead to clinically significant adrenal cortex suppression. Therefore, during periods of stress, such as severe infections or planned surgeries, additional systemic corticosteroid therapy should be considered. Rapid steroid dose reduction may trigger acute adrenal insufficiency. Symptoms of acute adrenal insufficiency may include anorexia, abdominal pain, weight loss, fatigue, headache, nausea, vomiting, decreased level of consciousness, seizures, hypotension, and hypoglycemia.
Treatment with additional systemic steroids or inhaled budesonide must not be abruptly discontinued.
When switching from oral steroids to Bufomix Easyhaler, the overall lower systemic steroid effect may lead to the emergence of allergic or arthritic symptoms such as rhinitis, eczema, muscle and joint pain. In such cases, specific treatment should be initiated. General glucocorticoid insufficiency should be suspected if symptoms such as fatigue, headache, nausea, and vomiting occur. In such cases, temporary increase in oral glucocorticoid dose may sometimes be necessary.
To reduce the risk of oropharyngeal candidiasis, patients should thoroughly rinse their mouth with water after each inhalation of the maintenance dose. If oropharyngeal candidiasis develops, patients should also rinse their mouth with water after each dose as needed.
Concomitant treatment with itraconazole, ritonavir, or other potent CYP3A4 inhibitors should be avoided. If this is unavoidable, the time intervals between drug administrations should be maximized. For patients taking potent CYP3A4 inhibitors, it is not recommended to use Bufomix Easyhaler simultaneously for both maintenance and symptom relief.
Bufomix Easyhaler should be prescribed with caution in patients with thyrotoxicosis, pheochromocytoma, diabetes mellitus, untreated hypokalemia, hypertrophic obstructive cardiomyopathy, idiopathic subaortic stenosis, severe hypertension, aneurysm, or other severe cardiovascular disorders such as ischemic heart disease, tachyarrhythmia, or severe heart failure.
Caution is advised when treating patients with prolonged QTc interval. Formoterol itself may cause QTc interval prolongation.
In patients with active or inactive pulmonary tuberculosis, or fungal or viral respiratory tract infections, the need for and dosage of inhaled corticosteroids should be reassessed.
Potentially life-threatening hypokalemia may develop during treatment with high doses of β2-adrenergic agonists. The hypokalemic effect of β2-agonists may be potentiated when used concomitantly with other drugs that may cause or exacerbate hypokalemia, such as xanthine derivatives, steroids, and diuretics. Particular caution is required in patients with unstable bronchial asthma receiving intermittent rescue bronchodilators, acute severe asthma, due to increased risk exacerbated by hypoxia, and in other conditions with increased risk of hypokalemia. In such cases, serum potassium levels should be monitored.
In patients with diabetes mellitus, additional monitoring of blood glucose concentration is recommended.
Pneumonia and other lower respiratory tract infections
Physicians should consider the possibility of pneumonia in patients with COPD due to frequent overlap of clinical signs of pneumonia and exacerbation of the underlying disease. Lower respiratory tract infections, including pneumonia, have been observed following inhaled corticosteroid use.
Immunosuppression
Patients receiving medications that suppress the immune system are more susceptible to infections than healthy individuals.
Pneumonia in patients with COPD
An increased incidence of pneumonia, including cases requiring hospitalization, has been observed in COPD patients receiving inhaled corticosteroids. Some data suggest an increased risk of pneumonia with higher steroid doses, although this has not been consistently demonstrated in all studies.
There is no convincing clinical evidence of class differences in the magnitude of pneumonia risk among inhaled corticosteroid products.
Physicians should remain vigilant for possible pneumonia in COPD patients, as clinical signs of such infections overlap with symptoms of COPD exacerbation.
Risk factors for pneumonia in COPD patients include smoking, advanced age, low body mass index (BMI), and severe COPD.
Bufomix Easyhaler contains approximately 4 mg of lactose per inhalation. This amount usually does not cause problems in patients with lactose intolerance. The excipient lactose contains small amounts of milk proteins, which may cause allergic reactions.
Use during pregnancy or breastfeeding.
Pregnancy. There are no clinical data on the effects of Bufomix Easyhaler or combined formoterol and budesonide therapy during pregnancy. Animal embryofetal development studies did not demonstrate any additional effects of the combination.
There are insufficient data on formoterol use in pregnant women. Formoterol caused adverse effects in animals during reproductive toxicity studies at very high systemic exposure levels.
Data from approximately 2000 studied pregnancy cases did not show an increased teratogenic risk associated with inhaled budesonide. Animal studies have shown that glucocorticoids can cause developmental abnormalities. This is unlikely in humans receiving recommended doses.
Animal studies have also shown that excessive prenatal glucocorticoid exposure increases the risk of intrauterine growth restriction, adult cardiovascular disease, irreversible changes in glucocorticoid receptor density, neurotransmitter turnover, and behavior at concentrations below the teratogenic dose range.
Bufomix Easyhaler should be used during pregnancy only if the expected benefit outweighs the potential risks. The lowest effective budesonide dose required to maintain adequate asthma control should be used.
Breastfeeding period. Budesonide is excreted in breast milk. However, no effects on the breastfed infant are expected at therapeutic doses. It is unknown whether formoterol is excreted in human breast milk. Small amounts of formoterol have been detected in the milk of animals. The use of Bufomix Easyhaler in breastfeeding women should be considered only if the expected benefit to the mother outweighs any potential risk to the infant.
Fertility. There are no data on the potential effect of budesonide on fertility. Studies on the effects of formoterol on reproductive function in animals showed slightly reduced fertility in male rats at high systemic exposure.
Ability to affect reaction speed when driving or operating machinery.
Bufomix Easyhaler has no or negligible effect on the ability to drive or operate machinery.
If dizziness, tremor, or seizures occur during treatment, patients should not drive or operate machinery.
Method of Administration and Dosage
Dosing
Bronchial Asthma
Bufomix Easyhaler is not intended for the initial treatment of bronchial asthma. The doses of the components in Bufomix Easyhaler are individually selected and adjusted according to the severity of the disease. This should be taken into account not only at the beginning of treatment with combination drugs but also during adjustments of the maintenance dose. If a patient requires a combination of doses different from those available in the combined inhaler, appropriate doses of β2-adrenergic agonists and/or corticosteroids should be prescribed using separate inhalers.
The dose should be titrated to the lowest dose that effectively controls symptoms. Patients must undergo regular follow-up evaluations by the prescribing physician to ensure that the dose of Bufomix Easyhaler remains optimal. After achieving long-term symptom control with the lowest recommended dose, an attempt should be made to maintain symptom control using only an inhaled corticosteroid.
There are two regimens for using Bufomix Easyhaler.
A. Maintenance therapy: Bufomix Easyhaler is used for regular maintenance treatment in combination with a separate rapid-acting bronchodilator used as a rescue medication.
B. Maintenance therapy and symptom relief: Bufomix Easyhaler is used for regular maintenance therapy and, as needed, for symptom relief.
A. Maintenance therapy
Patients should be advised to always carry a separate rapid-acting bronchodilator for use as a rescue medication.
Recommended doses:
Adults (aged 18 years and older): 1–2 inhalations twice daily. Some patients may require up to 4 inhalations twice daily.
Adolescents (12–17 years of age): 1–2 inhalations twice daily.
Typically, after achieving symptom control with twice-daily administration, the dose should be titrated down to the lowest effective dose, including reducing the dose to once daily with Bufomix Easyhaler, when, in the physician’s opinion, the patient requires maintenance therapy with a long-acting bronchodilator in combination with an inhaled corticosteroid.
Increased use of a rapid-acting bronchodilator indicates worsening of the patient’s condition and the need to reassess the treatment regimen for bronchial asthma.
B. Maintenance therapy and symptom relief
The patient takes the daily maintenance dose of Bufomix Easyhaler and additionally uses Bufomix Easyhaler as needed for symptom relief. Patients should be advised to always carry Bufomix Easyhaler for immediate use as a rescue medication.
The physician and patient using Bufomix Easyhaler for symptom relief should discuss preventive use of the medication in cases of bronchospasm triggered by allergens or physical exertion, and consider the recommended frequency of administration. If frequent bronchodilation is required without a corresponding need to increase the dose of inhaled corticosteroids, alternative therapy should be considered.
The use of Bufomix Easyhaler for maintenance therapy and symptom relief should be particularly considered in patients:
-
with poorly controlled bronchial asthma who frequently require medications for symptom relief;
-
with a history of asthma exacerbations requiring medical intervention.
Patients who frequently and in large quantities use Bufomix Easyhaler on an as-needed basis require close monitoring for the development of dose-dependent adverse effects.
Recommended doses:
Adults and adolescents (aged 12 years and older): The recommended maintenance dose is 2 inhalations per day—1 inhalation in the morning and 1 in the evening, or 2 inhalations either in the morning or in the evening. Some patients may require a maintenance dose of 2 inhalations twice daily. As needed, for symptom relief, 1 additional inhalation should be taken. If symptoms persist after several minutes, an additional inhalation may be administered. In any single episode, no more than 6 inhalations should be used.
The total daily dose should generally not exceed 8 inhalations; however, during a limited period, the total daily dose may reach up to 12 inhalations. Patients using more than 8 inhalations per day are strongly advised to consult their physician. They should undergo reassessment and review of their maintenance therapy.
Children under 12 years of age: The use of Bufomix Easyhaler for maintenance therapy and symptom relief is not recommended in children.
COPD
Recommended doses:
Adults: 2 inhalations twice daily.
General Information
Special patient groups
No special dosing requirements are necessary for elderly patients. Data on the use of Bufomix Easyhaler in patients with impaired renal or hepatic function are lacking. Since both budesonide and formoterol are primarily eliminated via hepatic metabolism, increased systemic effects of the drug may be expected in patients with severe liver cirrhosis.
Method of Administration
For inhalation use.
How to correctly use Bufomix Easyhaler
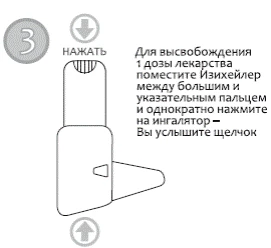
The inhaler is activated by the airflow during inhalation. This means that when the patient inhales through the mouthpiece, the medication is delivered into the airways along with the inhaled air.





It is important to emphasize the following points to the patient:
- Carefully read the instructions for medical use.
- After opening the foil package, it is recommended to store the device in its protective container to protect it from impact and ensure reliable device function.
- Shake the device and activate it before each inhalation.
- Inhale through the mouthpiece sufficiently actively and deeply to ensure optimal delivery of the medication to the lungs.
- Do not exhale through the mouthpiece, as this will reduce the delivered dose. If this occurs, the patient should tap the inhaler gently on a hard surface or the palm of the hand to remove powder from the mouthpiece and then repeat the inhalation procedure.
- Do not activate the device more than once without inhaling the powder. If this occurs, the patient should tap the inhaler gently on a hard surface or the palm of the hand to remove powder from the mouthpiece and then repeat the inhalation procedure.
- Always replace the dust cap and close the protective container lid after using the inhaler to prevent accidental powder dispersion (which could lead to either overdose or insufficient medication delivery during the next use).
- Rinse the mouth with water after each inhalation to minimize the risk of developing oral candidiasis. If oral candidiasis develops, patients should rinse their mouth with water after each "as-needed" inhalation.
- Clean the mouthpiece regularly with a dry cloth. Do not use water for cleaning, as the powder is hygroscopic.
- Replace the Bufomix Easyhaler inhaler when the counter displays zero, even if some powder remains visible inside the device.
Children
Bufomix Easyhaler is not recommended for children under 12 years of age for the treatment of bronchial asthma.
In children receiving long-term therapy with inhaled corticosteroids, regular monitoring of growth is recommended. If growth retardation occurs, the treatment regimen should be reassessed with the aim of reducing the inhaled corticosteroid dose to the lowest level that maintains effective asthma control. The benefits of corticosteroid therapy should be carefully weighed against the risk of growth suppression. Additionally, the patient should be referred to a pediatric pulmonologist.
Long-term studies suggest that most children and adolescents treated with inhaled budesonide eventually achieve their target adult height. However, a small, transient initial reduction in growth (approximately 1 cm) has been observed, typically during the first year of treatment.
Bufomix Easyhaler should not be used in children for the treatment of COPD.
Overdose
Symptoms. Overdose of formoterol may be associated with symptoms typically observed with β2-adrenergic agonist overdose: tremor, headache, tachycardia. In individual cases, symptoms such as tachycardia, hyperglycemia, hypokalemia, prolonged QTc interval, arrhythmia, nausea, and vomiting have been reported. Supportive and symptomatic treatment is indicated. A dose of 90 mcg administered over three hours in patients with acute bronchial obstruction was found to be safe.
Acute overdose of budesonide, even with excessive doses, is not expected to cause clinical problems. However, chronic use of excessive doses may lead to glucocorticoid effects such as hypercorticism and suppression of adrenal cortex function.
If treatment with Bufomix Easyhaler must be discontinued due to formoterol overdose, appropriate therapy with inhaled corticosteroids should be considered.
Adverse Reactions.
Since Bufomix Izihealer contains both budesonide and formoterol, patients may experience adverse effects typical of these two substances. No increase in the frequency of adverse reactions has been observed following concomitant administration of these two compounds. The most commonly reported drug-related adverse events correspond to the pharmacologically predictable side effects of β2-agonist therapy. These include tremor and tachycardia, which are usually mild and resolve within a few days.
The adverse reactions associated with formoterol are listed below by system organ class and frequency of occurrence. Frequency is defined according to the following scale: very common (≥1/10), common (≥1/100, <1/10), uncommon (≥1/1000, <1/100), rare (≥1/10000, <1/1000), very rare (<1/10000). Infections and infestations.
Common: oropharyngeal candidiasis, pneumonia (in patients with COPD).
Immune system disorders.
Rare: immediate or delayed hypersensitivity reactions such as exanthema, urticaria, pruritus, dermatitis, angioedema, and anaphylactic reaction.
Endocrine system disorders.
Very rare: Cushing's syndrome, adrenal suppression, growth retardation, decreased bone mineral density.
Metabolism and nutrition disorders.
Rare: hypokalaemia.
Very rare: hyperglycaemia.
Psychiatric disorders.
Uncommon: aggression, psychomotor hyperactivity, anxiety, sleep disturbances.
Very rare: depression, behavioral changes (mainly in children).
Nervous system disorders.
Common: headache, tremor.
Uncommon: dizziness.
Very rare: taste disturbance.
Eye disorders.
Uncommon: blurred vision.
Very rare: cataract, glaucoma.
Cardiac disorders.
Common: palpitations.
Uncommon: tachycardia.
Rare: cardiac arrhythmias, e.g. atrial fibrillation, supraventricular tachycardia, extrasystoles.
Very rare: angina pectoris, QTc interval prolongation, blood pressure fluctuations.
Respiratory, thoracic and mediastinal disorders.
Common: mild irritation in the throat, cough, dysphonia including hoarseness.
Rare: bronchospasm.
Gastrointestinal disorders.
Uncommon: nausea.
Skin and subcutaneous tissue disorders.
Uncommon: bruising.
Musculoskeletal and connective tissue disorders.
Uncommon: muscle cramps.
Oropharyngeal candidiasis is caused by deposition of the drug in the oropharynx. Patients should be advised to rinse the mouth with water after each dose to minimize the risk. Oropharyngeal candidiasis usually responds to local antifungal treatment and does not require discontinuation of inhaled corticosteroids. In case of oropharyngeal candidiasis, patients should also rinse the mouth with water after using the product as needed.
As with other forms of inhaled therapy, paradoxical bronchospasm may occur in rare cases, affecting approximately 1 in 10,000 patients. In such cases, wheezing and shortness of breath increase immediately after dosing. Paradoxical bronchospasm responds to fast-acting inhaled bronchodilators and requires immediate treatment. Bufomix Izihealer should be discontinued immediately, the patient should be evaluated, and alternative therapy should be considered if necessary.
Systemic effects of inhaled corticosteroids may occur, particularly with long-term use of high doses. These effects are much less likely than those associated with oral corticosteroids. Possible systemic effects include Cushing's syndrome, Cushingoid appearance, adrenal suppression, growth retardation in children and adolescents, decreased bone mineral density, cataract, and glaucoma. Increased susceptibility to infections and impaired ability to adapt to stress may also develop. These effects are likely dose-, duration-, and individual-sensitivity-dependent and may be influenced by concomitant or prior steroid therapy.
Treatment with β2-agonists may lead to increased levels of insulin, free fatty acids, glycerol, and ketone bodies in the blood.
The use of systemic and inhaled corticosteroids may lead to pneumonia or lower respiratory tract infections in patients with COPD and to immunosuppression.
Paediatric populations
Regular monitoring of growth in children receiving long-term inhaled corticosteroids is recommended (see section "Special precautions").
Reporting of suspected adverse reactions
It is important to report suspected adverse reactions after marketing authorization of the medicinal product. This allows continuous monitoring of the benefit-risk balance of the medicinal product. Healthcare professionals are requested to report any suspected adverse reactions via the national reporting system.
Shelf life. 2 years in the laminated pouch.
Use within 4 months after opening the laminated pouch.
Storage conditions.
Prior to opening the laminated pouch, the product does not require special storage conditions.
After opening the laminated pouch, store at a temperature not exceeding 25 °C in a dry place protected from moisture.
Packaging.
60 doses or 120 doses in an inhaler with a protective cap in a laminated pouch.
1 laminated pouch in a cardboard box.
60 doses or 120 doses in an inhaler with a protective cap in a laminated pouch.
1 laminated pouch and a protective container for the inhaler in a cardboard box.
Prescription status. Prescription only.
Manufacturer.
Orion Corporation.
Manufacturer's address and place of business.
Orionintie 1, 02200 Espoo, Finland / Orionintie 1, 02200 Espoo, Finland.