Berotec n
Ukraine
Table of Contents
INSTRUCTIONS FOR MEDICAL USE OF THE MEDICINAL PRODUCT BEROTEC® N (BEROTEC® N)
Composition:
Active substance: fenoterol hydrobromide;
1 inhalation contains fenoterol hydrobromide 100 mcg;
Excipients: norflurane (propellant), anhydrous citric acid, purified water, anhydrous ethanol.
Pharmaceutical form. Metered aerosol.
Main physicochemical properties: clear, colorless, slightly yellowish or slightly brownish liquid, free from suspended particles.
Pharmacotherapeutic group. Drugs used in obstructive airway diseases. Selective beta-2-adrenergic agonists.
ATC code R03A C04.
Pharmacological properties.
Pharmacodynamics.
Berotec N is an effective bronchodilator for use in acute asthma attacks and other conditions with reversible airway narrowing, such as obstructive bronchitis with or without pulmonary emphysema. After oral administration, Berotec N begins to act within a few minutes, with a duration of action up to 8 hours.
After inhalation of fenoterol hydrobromide in obstructive lung diseases, bronchodilation occurs within a few minutes. The bronchodilator effect lasts 3–5 hours.
When higher doses are used, the drug stimulates beta-1-adrenoceptors.
Fenoterol relaxes bronchial and vascular smooth muscle. The smooth muscle relaxation effect is dose-dependent. It is believed to be enhanced via influence on the adenylate cyclase system, whereby binding of beta-agonists to their receptors (stimulated by a guanine-binding protein) leads to activation of adenylate cyclase. As a result, phosphorylation of protein (protein kinase A) increases intracellular cAMP levels, leading to smooth muscle relaxation. At high doses, fenoterol also affects striated muscles (tremor). In addition, fenoterol inhibits mediator release from mast cells. After administration of fenoterol at a dose of 0.6 mg, improvement in mucociliary clearance has been observed.
Fenoterol has positive inotropic and chronotropic (direct and/or reflex) effects on the heart. When high doses are used, metabolic effects such as lipolysis, glycogenolysis, hyperglycemia, and hypokalemia are observed; the latter is caused by increased uptake of K+ ions, primarily by skeletal muscle. As with other beta-adrenergic agents, prolongation of the QTc interval has been reported. For fenoterol metered dose inhalers, such events were isolated and occurred at doses higher than recommended. Clinical significance has not been established.
Due to the high concentration of beta-2 receptors in the myometrium, fenoterol may relax uterine muscle. This effect is often observed during pregnancy. The tocolytic dose of fenoterol is much higher than the bronchospasmolytic dose. Therefore, the risk of adverse effects is high.
Pharmacokinetics.
The pharmacokinetics of fenoterol have been studied after intravenous, inhalation, and oral administration. The therapeutic effect of Berotec N is achieved through local action on the respiratory tract. Thus, plasma concentration of the drug does not necessarily correlate with bronchodilator effect.
Absorption. After inhalation, depending on the inhalation technique and delivery system used, approximately 10–30% of the active substance released from the aerosol formulation reaches the lower respiratory tract. The remainder deposits in the upper respiratory tract and oral cavity and is subsequently swallowed. The absolute bioavailability of fenoterol from the metered-dose aerosol Berotec N after inhalation is 18.7%.
Absorption after inhalation follows a biphasic pattern, with an extent of 13% of the dose. 30% of the fenoterol hydrobromide dose is rapidly absorbed with a half-life of 11 minutes, and 70% is slowly absorbed with a half-life of 120 minutes.
After oral administration, approximately 60% of the fenoterol hydrobromide dose is absorbed. The absorbed amount undergoes extensive first-pass metabolism, resulting in oral bioavailability reduced to approximately 1.5%. Thus, the contribution of the active ingredient dose swallowed by the patient to plasma concentration after inhalation is negligible. Maximum plasma concentration is reached approximately 60–120 minutes after administration.
Distribution. Fenoterol is widely distributed throughout the body. The volume of distribution at steady state (Vss) after intravenous administration ranges from 1.9 to 2.7 L/kg. Distribution of fenoterol in plasma after intravenous administration is adequately described by a three-compartment pharmacokinetic model with half-lives of tα = 0.42 minutes, tβ = 14.3 minutes, and tγ = 3.2 hours. Plasma protein binding ranges from 40 to 55%.
Metabolism. In humans, fenoterol undergoes extensive metabolism via conjugation to glucuronides and sulfates. After oral administration, fenoterol is metabolized predominantly by sulfonation. This metabolic inactivation of the parent compound begins in the intestinal wall.
Elimination. After intravenous administration, biotransformation, including biliary excretion, accounts for the majority (approximately 85%) of total systemic clearance, which equals 1.1–1.8 L/min. Renal clearance of fenoterol (0.27 L/min) accounts for approximately 15% of the total systemic clearance of the bioavailable dose. Considering the fraction of drug bound to plasma proteins, the magnitude of renal clearance suggests, in addition to glomerular filtration, tubular secretion of fenoterol.
Within 48 hours after oral and intravenous administration, total urinary excretion of radioactivity accounts for approximately 39% and 65% of the dose, respectively, while total fecal excretion of radioactivity equals 40.2% and 14.8% of the dose, respectively. After oral administration, 0.38% of the dose is excreted unchanged in urine, whereas after intravenous administration, 15% of the compound is excreted unchanged. After inhalation from a metered-dose inhaler, 2% of the dose is excreted unchanged by the kidneys within 24 hours.
Unmetabolized fenoterol can cross the placental barrier. Sympathomimetic effects may occur in the fetus. After prolonged infusion, fenoterol levels in fetal blood have been observed to reach up to 50% of maternal plasma concentrations. Fenoterol is eliminated more slowly in premature infants than in adults.
Fenoterol passes into breast milk.
Data on effects in patients with diabetes mellitus are insufficient.
There may be minor effects on infants or neonates up to 20 months of age.
Clinical characteristics.
Indications.
- Symptomatic treatment of acute asthma attacks.
- Prophylaxis of exercise-induced asthma.
- Symptomatic treatment of bronchial asthma of allergic and non-allergic origin and/or other conditions with reversible airway obstruction, such as chronic obstructive bronchitis with or without emphysema.
Long-term therapy should always be accompanied by concomitant anti-inflammatory treatment.
Contraindications.
• Hypersensitivity to fenoterol hydrobromide or to any of the excipients of the metered aerosol (see section "Composition").
• Hypertrophic obstructive cardiomyopathy.
• Tachyarrhythmia.
Interaction with other medicinal products and other forms of interaction.
Concomitant use of other beta-2 adrenergic agents, methylxanthines (e.g., theophylline), anticholinergics, and corticosteroids may enhance the effect of the medicinal product BEROTEC N. If BEROTEC N is used concomitantly with other beta-2 adrenergic agents, methylxanthines (e.g., theophylline), or systemic-acting anticholinergics (agents containing pirenzepine), an increased risk of adverse effects (such as tachycardia, arrhythmia) may occur.
Hypokalemia induced by beta-2 agonists may be exacerbated by concomitant therapy with xanthine derivatives, corticosteroids, and diuretics. This should be taken into account, particularly in patients with severe airway obstruction. In such cases, electrolyte levels should be monitored, especially when diuretics and cardiac glycosides (digitalis) are used concomitantly.
Concomitant use of BEROTEC N and beta-blockers results in mutual attenuation of effects and poses a risk of beta-blocker-induced severe bronchospasm in patients with bronchial asthma.
Treatment with BEROTEC N may also reduce the hypoglycemic effect of antidiabetic medicinal products. However, this is expected only at high doses, typically used for systemic administration (tablets or injections/infusions).
Concomitant use of BEROTEC N and monoamine oxidase inhibitors (MAOIs) or tricyclic antidepressants may potentiate the cardiovascular effects of fenoterol.
When inhaling halogenated anesthetics such as halothane, methoxyflurane, or enflurane, there is an increased risk of severe cardiac arrhythmias and decreased arterial blood pressure in patients receiving BEROTEC N.
If inhalation anesthetics are planned, it should be noted that fenoterol administration must be discontinued at least 6 hours prior to the start of anesthesia.
Special precautions for use.
BEROTEK N should be used with caution, especially when administering the highest recommended dose, and only after careful assessment of risk versus benefit in the following cases: severe heart disease, particularly recent myocardial infarction and coronary heart disease; when patients are taking cardiac glycosides; severe and untreated arterial hypertension; aneurysm; hyperthyroidism; poorly controlled diabetes mellitus; and phaeochromocytoma.
This is particularly relevant when using the highest recommended doses.
Paradoxical bronchospasm
Like other inhaled medicinal products, BEROTEK N may cause paradoxical bronchospasm, which may be life-threatening. In the event of paradoxical bronchospasm, BEROTEK N must be discontinued immediately and alternative therapy initiated.
Cardiovascular effects
Cardiovascular effects may occur with sympathomimetic agents, including BEROTEK N. There is some evidence of myocardial ischemia associated with beta-agonists from post-marketing data and isolated publications. Patients with significant underlying heart disease (e.g., ischemic heart disease, arrhythmia, or severe heart failure) who are taking BEROTEK N should be warned to seek medical advice if they experience chest pain or other symptoms indicating worsening cardiac disease.
Careful evaluation of symptoms such as dyspnea and chest pain is necessary, as these may be of either respiratory or cardiac origin.
Hypokalemia
Severe hypokalemia may occur during treatment with beta-2-agonists. Particular caution is required in severe asthma, as hypokalemia may be potentiated by concomitant administration of xanthine derivatives, glucocorticosteroids, and diuretics. In addition, hypoxia as a symptom of bronchial asthma may intensify the effects of hypokalemia on cardiac rhythm. In patients taking digoxin, hypokalemia may increase susceptibility to arrhythmias. Monitoring of serum potassium levels is recommended in such conditions.
Acute worsening dyspnea
In case of acute, rapidly worsening dyspnea, patients should seek immediate medical attention.
Worsening asthma symptoms, frequency of use, anti-inflammatory therapy
Patients prescribed regular anti-inflammatory therapy should be advised to continue using anti-inflammatory medications even when symptoms improve and they do not require BEROTEK N.
If a previously effective dosing regimen no longer provides the same relief of symptoms, the patient should seek medical advice as soon as possible, as this may indicate worsening asthma control and requires reassessment of asthma therapy.
Excessive use of short-acting beta-agonists may mask progression of the underlying disease and contribute to deterioration in asthma control, leading to an increased risk of severe asthma exacerbations and increased mortality.
Patients using fenoterol more than twice a week on an "as-needed" basis, excluding prophylactic use before physical exertion, should be re-evaluated for appropriate adjustment of treatment, as these patients belong to a high-risk group for excessive fenoterol use.
Concomitant use with sympathomimetic or anticholinergic bronchodilators
Other sympathomimetic bronchodilators should be used concomitantly with BEROTEK N only under medical supervision (see section "Interaction with other medicinal products and other forms of interaction"). Anticholinergic bronchodilators may be used together with BEROTEK N.
Due to the potential for increased blood glucose levels, glucose levels should be monitored in patients with diabetes mellitus.
Due to lack of pharmacokinetic data on fenoterol in patients with hepatic or renal impairment, BEROTEK N should be prescribed with caution in these patient groups.
The medicinal product contains 16 mg of alcohol (ethanol) per inhalation. The amount of alcohol in each inhalation is equivalent to less than the amount found in 1 ml of beer or 1 ml of wine. The small amount of alcohol in this medicinal product is not expected to have any noticeable effects.
Note for athletes
Use of BEROTEK N may result in positive doping test outcomes.
Use during pregnancy or breastfeeding
Pregnancy. Fenoterol crosses the placental barrier.
The use of BEROTEK N during pregnancy is only recommended after careful assessment of benefit versus risk, particularly during the first trimester. Although the active substance does not demonstrate a tocolytic effect with inhaled administration, the possibility of such an effect cannot be completely ruled out.
Breastfeeding. It is unknown whether fenoterol has a negative effect on the infant. Since fenoterol passes into breast milk, use of the medicinal product during breastfeeding is recommended only after careful assessment of benefit versus risk.
Fertility. There are no clinical data on the effect of fenoterol hydrobromide on fertility. Preclinical studies with fenoterol hydrobromide showed no adverse effects on fertility.
Ability to affect reaction speed when driving or operating machinery.
No studies on the effect of BEROTEK N on the ability to drive or operate machinery have been conducted. However, patients should be warned about the possible occurrence of adverse effects such as dizziness during treatment with BEROTEK N. Therefore, caution should be exercised when driving or operating machinery. If the aforementioned effects occur, patients should avoid potentially hazardous activities such as driving or operating machinery.
Method of Administration and Dosage.
The dose should be adjusted according to the nature and severity of the disease.
For adults and children aged 6 years and older, the following dosage regimens are recommended.
To relieve an acute attack of bronchial asthma or an episode of dyspnea, the recommended dose is 100 mcg of fenoterol hydrobromide (1 inhalation).
Generally, 1 inhalation is sufficient during an acute attack of dyspnea to achieve rapid relief of breathing. If breathing does not significantly improve within 5 minutes after administration, a second inhalation may be given. If no effect is observed after 2 inhalations, additional inhalations may become necessary. In such cases, the patient must seek immediate medical attention (see section "Special Precautions").
If long-term treatment with beta-2-sympathomimetics is considered necessary, the recommended dose is 1–2 inhalations of BEROTEC N 3–4 times daily. In general, the timing and dose of each administration of BEROTEC N should be determined based on the frequency and severity of dyspnea (according to symptoms). Treatment should be accompanied by anti-inflammatory therapy, especially in bronchial asthma. There should be an interval of at least 3 hours between inhalations. The total daily dose must not exceed 8 inhalations, and the maximum single dose must not exceed 4 inhalations, since higher doses do not provide additional therapeutic benefits overall but may cause severe adverse effects.
For specific prophylaxis of exercise-induced asthma or when exposure to an allergen is expected, 1–2 inhalations of BEROTEC N should be administered, preferably 10–15 minutes before the anticipated incident.
For children aged 4–6 years, unless otherwise prescribed, the following dosage regimens are recommended.
To relieve an acute attack of bronchial asthma or an episode of dyspnea, the recommended dose is 100 mcg of fenoterol hydrobromide (1 inhalation).
For long-term treatment or prevention of attacks, 100 mcg (1 inhalation) of fenoterol hydrobromide should be administered 4 times daily. The timing and dose of each administration of BEROTEC N should be determined based on the frequency and severity of dyspnea (according to symptoms). Treatment should be accompanied by anti-inflammatory therapy, especially in bronchial asthma. There should be an interval of at least 3 hours between inhalations. The total daily dose must not exceed 4 inhalations, and the maximum single dose must not exceed 2 inhalations, since higher doses do not provide additional therapeutic benefits overall but may cause severe adverse effects.
For specific prophylaxis of exercise-induced asthma or when exposure to an allergen is expected, 100 mcg (1 inhalation) of fenoterol hydrobromide should be administered, preferably 10–15 minutes before the anticipated incident.
This medicinal form is not suitable for use in children under 4 years of age.
WARNING. In the absence of significant improvement or if the condition worsens despite prescribed treatment, medical advice should be sought to review the treatment plan, possibly combining with other medications (anti-inflammatory agents such as corticosteroids, or bronchodilators such as theophylline) or adjusting the dosage. Sudden and progressive worsening of asthma symptoms may be life-threatening. In such cases, immediate medical assistance is required. The use of doses significantly exceeding the recommended ones is dangerous.
There have been reports of several cases of increased risk of serious complications of the underlying disease, as well as fatal outcomes, during long-term treatment of bronchial asthma with excessively high doses of inhaled beta-2-sympathomimetics without adequate anti-inflammatory therapy. A causal relationship has not been fully established. However, inadequate anti-inflammatory therapy appears to play a decisive role.
Special Warnings During Therapy. Treatment of bronchial asthma should be stepwise and adapted to the severity of the condition. Response to treatment should be monitored regularly.
Self-adjustment of the dose of beta-2-sympathomimetics such as BEROTEC N may be dangerous for the patient.
From a medical standpoint, daily self-monitoring by the patient according to physician instructions is important for assessing disease progression and the effectiveness of bronchodilator and anti-inflammatory therapy. This may include recording the forced expiratory volume measured by a peak flow meter.
Instructions for Use of the Metered Aerosol.
Proper use of the metered aerosol is essential for successful treatment. Patients should be instructed on the correct use of the metered aerosol. The arrow on the container should point straight upward and the mouthpiece downward, regardless of the inhalation position. The aerosol should be used, if possible, while sitting or standing.
Before the first use of the inhaler, press the valve twice.
Steps to follow before each administration:
- Remove the protective cap (Fig. 1).
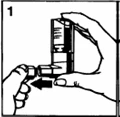
Fig. 1.

Fig. 2.
- Exhale fully.
- Hold the metered aerosol as shown in Fig. 2, placing the mouthpiece in the mouth. The arrow and base of the container should be facing upward, and the mouthpiece downward.
- Inhale as deeply as possible, simultaneously pressing firmly on the base of the container, which releases the measured dose. Hold the breath for several seconds, then remove the mouthpiece and exhale.
If the patient cannot inhale deeply due to severe dyspnea, first spray 1 inhalation into the oral cavity: this will ease breathing and allow proper administration of the medication.
If another inhalation is needed, repeat the steps described above (steps 2–4).
- After use, replace the protective cap.
BEROTEC N should be used in advance to prepare for "opening the lungs" and to support aerosol therapy with corticosteroids, saline solution, and sodium cromoglicate.
The duration of treatment is determined based on the nature, severity, and progression of the disease. The physician must individually adjust the dose.
Additional Instructions. Patients should be instructed on the correct use of the metered aerosol. Children should only use the metered aerosol BEROTEC N upon a physician's recommendation and under adult supervision.
If the metered aerosol inhaler has not been used for more than 3 days, press the valve once before use until the aerosol appears.
Clean the inhaler at least once a week.
It is important to keep the inhaler mouthpiece clean to ensure that the medication does not thicken and block the aerosol release.
To clean, first remove the dust cap and detach the container from the inhaler. Rinse the inhaler with water until the thickened medication and/or dirt are washed away (Fig. 3).

Fig. 3
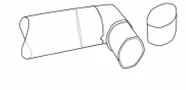
Fig. 4
After cleaning, shake the inhaler and let it air-dry without using any heating device (Fig. 4). Once the mouthpiece is dry, reattach the container and the dust cap.
The plastic mouthpiece is specifically designed for use with BEROTEC N metered aerosol, 100 mcg. The mouthpiece must not be used with any other metered aerosol. BEROTEC N metered aerosol must only be used with the mouthpiece supplied with the product.
The container is under pressure and must never be opened by force under any circumstances.
The container is opaque; therefore, it is not possible to see when it is empty. The aerosol canister provides 200 doses. When all doses have been used, it may appear that a small amount of liquid remains in the canister. However, the canister must be replaced at this point, otherwise the patient will not receive the accurate amount of medication.
The amount of medication in the aerosol canister can be checked as follows: detach the plastic mouthpiece from the canister and place the canister in a container of water. The level of medication in the aerosol canister can be estimated by observing its position in the water (see Fig. 5).
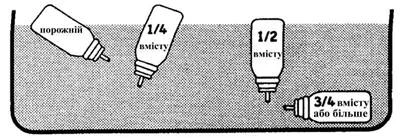
Fig. 5.
Children.
To be used in children aged 4 years and older, only upon physician's prescription and under adult supervision.
Overdose.
Symptoms. Depending on the duration of overdose, the following adverse reactions typical of beta-2-adrenergic agents may occur: flushing, mild dizziness, headache, tachycardia, rapid heartbeat, arrhythmia, hypotension or even shock, arterial hypertension, restlessness, chest pain, excitement, possible extrasystoles, and severe tremor in fingers and throughout the body. Hyperglycemia, hyperlipidemia, and hyperketonemia may also develop.
Metabolic acidosis and hypokalemia have been observed when fenoterol was administered in doses higher than recommended according to the approved indications for BEROTEC N.
Gastrointestinal reactions, including nausea and vomiting, may occur, especially after oral overdose.
Treatment. Administration of BEROTEC N should be discontinued. Monitoring of acid-base balance and electrolytes should be considered. Treatment of overdose with beta-sympathomimetics is symptomatic. The effects of fenoterol may be counteracted by beta-receptor blockers. However, possible worsening of bronchial obstruction must be taken into account; therefore, dosage must be carefully selected for patients with bronchial asthma. This also applies to so-called cardioselective beta-receptor blockers.
Monitoring of cardiac function, including ECG, is recommended.
Adverse Reactions
As with all medicinal products, BEROTEK N may cause adverse reactions.
Frequency of adverse reactions:
very common ≥ 1/10;
common ≥ 1/100 to < 1/10;
uncommon ≥ 1/1,000 to < 1/100;
rare ≥ 1/10,000 to < 1/1,000;
very rare < 1/10,000;
unknown – cannot be estimated from the available data.
Immune system disorders:
unknown – hypersensitivity (e.g. pruritus, rash, purpura, thrombocytopenia, facial edema).
Metabolism and nutrition disorders:
uncommon – hypokalemia (including severe hypokalemia);
rare – hyperglycemia.
Hypokalemia is more frequently observed in patients with severe bronchial asthma who are concurrently treated with xanthine derivatives (e.g. theophylline), corticosteroids and/or diuretics. In addition, hypoxia may influence the effect of hypokalemia on cardiac rhythm. In such cases, monitoring of serum potassium levels is recommended.
Increased levels of insulin, free fatty acids, glycerol and ketone bodies in blood have been observed.
Psychiatric disorders:
uncommon – psychiatric disturbances, excitation;
unknown – nervousness.
Psychiatric disturbances manifest as increased excitability, hyperactive behavior, sleep disorders, and hallucinations. These have been observed primarily in children under 12 years of age.
Nervous system disorders:
common – tremor, dizziness;
unknown – headache.
Cardiac disorders:
uncommon – arrhythmia, angina pectoris, ventricular extrasystoles;
unknown – tachycardia, palpitations, myocardial ischemia.
Respiratory, thoracic and mediastinal disorders:
common – cough;
uncommon – paradoxical bronchospasm;
unknown – local irritation.
If paradoxical bronchospasm occurs, treatment should be discontinued immediately.
Gastrointestinal disorders:
common – nausea;
uncommon – vomiting, heartburn.
Skin and subcutaneous tissue disorders:
common – hyperhidrosis;
uncommon – pruritus;
unknown – urticaria, skin reactions such as rash.
Musculoskeletal and connective tissue disorders:
uncommon – muscle cramps;
unknown – muscle weakness, myalgia.
Renal and urinary disorders:
uncommon – urinary disorders.
Investigations:
uncommon – increased blood pressure, decreased blood pressure.
Shelf life. 3 years.
Storage conditions. Store at temperatures not exceeding 25 °C. Protect from direct sunlight, heat and frost. Keep out of reach of children.
Packaging. 10 ml (200 inhalations) in a metal pressurized canister with a metering valve; 1 canister per cardboard box.
Prescription category. Prescription only.
Manufacturer.
Boehringer Ingelheim Pharma GmbH & Co. KG.
Manufacturer's address.
Binger Strasse 173, 55216 Ingelheim am Rhein, Germany.