Numeta g16%e
Poland
Table of Contents
Package leaflet: Information for the user
NUMETA G16%E, infusion emulsion
Please read all of this leaflet carefully before the medicine is administered, because it contains
important information for the patient.
- Keep this leaflet, as you may need to read it again.
- If you have any further questions, please ask your child's doctor, pharmacist, or nurse.
- If your child experiences any adverse reactions, including any not listed in this leaflet, tell your doctor or nurse. See section 4.
Leaflet contents
- What NUMETA G16%E is and what it is used for
- Important information before administering NUMETA G16%E to your child
- How to use NUMETA G16%E
- Possible side effects
- How to store NUMETA G16%E
- Contents of the pack and other information
1. What NUMETA G16%E is and what it is used for
NUMETA G16%E is a specialized infusion emulsion for nutritional support intended for term newborns and children up to 2 years of age. It is administered through a tube inserted into the child's vein when the child cannot receive all nutritional components orally.
NUMETA is supplied as a three-compartment bag, with each compartment containing:
50% glucose solution;
5.9% pediatric amino acid solution with electrolytes;
12.5% fat emulsion.
Depending on the child's needs, two or three of these solutions are mixed within the bag before administration to the child.
NUMETA G16%E must only be used under medical supervision.
2. Important information before administering NUMETA G16%E to a child
When NUMETA G16%E must not be given to a child:
For the 2-component solution mixed in the bag ("2 in 1"):
- if the child has a known allergy to egg protein, soy, peanuts, or any of the components contained in the glucose or amino acid chamber (listed in section 6);
- if the child’s body is unable to metabolize protein building blocks;
- if the child has high blood levels of any of the electrolytes present in NUMETA G16%E;
- in newborns (≤28 days of life), NUMETA G16%E (or other calcium-containing solutions) must not be administered simultaneously with ceftriaxone (an antibiotic), even when separate infusion lines are used. There is a risk of particle formation in the newborn’s circulation, which may lead to death.
- if the child has hyperglycemia (particularly high blood sugar levels).
For the 3-component solution mixed in the bag ("3 in 1"):
- in all the above-mentioned situations for the "2 in 1" solution, and additionally:
- if the child has markedly elevated blood lipid levels.
In all cases, the physician will make the decision to administer NUMETA G16%E after considering the child’s age, body weight, and clinical condition. The physician will also take into account the results of all performed tests.
Warnings and precautions
Before starting administration of NUMETA G16%E, discuss this with the attending physician or nurse.
When used in newborns and children under 2 years of age, the solution (in bags and administration sets) must be protected from light until the end of the infusion. Exposure of NUMETA G16%E to ambient light, especially after mixing with trace elements and (or) vitamins, leads to the formation of peroxides and other degradation products, which can be minimized by protecting from light.
Allergic reactions:
If any signs or symptoms of an allergic reaction occur (such as fever, sweating, chills, headache, skin rash, or breathing difficulties), the infusion must be stopped immediately.
This medicine contains soy oil, which rarely may cause hypersensitivity reactions. In some individuals allergic to peanut proteins, cross-reactivity with soy proteins has been rarely observed.
NUMETA G16%E contains glucose derived from corn starch. Therefore, NUMETA G16%E should be used with caution in patients with a known allergy to corn or corn-containing products.
Risk of precipitate formation with ceftriaxone (antibiotic):
The antibiotic ceftriaxone must not be mixed or administered simultaneously with any calcium-containing solutions (including NUMETA G16%E) via intravenous infusion.
The physician is aware of this and will not administer them simultaneously to the patient, even through different infusion lines or at different infusion sites.
However, the physician may administer calcium and ceftriaxone sequentially, one after the other, provided the infusion lines are placed at different sites, or are replaced or thoroughly flushed with saline solution between infusions, to prevent precipitation.
Formation of small particles in pulmonary blood vessels:
Breathing difficulties may also indicate the formation of small particles blocking blood vessels in the lungs (pulmonary vessel deposits). If the child experiences any breathing difficulties, inform the physician or nurse immediately. They will decide on appropriate actions.
Infection and sepsis:
The physician will closely monitor the child for signs of infection. Adhering to aseptic techniques (procedures protecting against microorganisms) during catheter insertion and maintenance, as well as during the preparation of the nutrient mixture, may reduce the risk of infection.
Sometimes, when a tube (intravenous catheter) is placed in a vein, the child may develop an infection and sepsis (presence of bacteria in the blood). Certain medications and diseases may increase the risk of infection or sepsis. Patients requiring parenteral nutrition (nutrient delivery via a tube placed in a vein) may be more susceptible to infection due to their underlying health condition.
Fat overload syndrome:
Fat overload syndrome has been reported during the use of similar medications.
Reduced or limited ability of the body to eliminate fats contained in NUMETA G16%E, or overdose, may result in so-called fat overload syndrome (see sections 3 and 4).
Changes in blood chemical composition:
The physician will check and monitor the child’s fluid status, blood chemistry, and levels of other substances, as parenteral nutrition in severely malnourished patients may sometimes cause changes in blood composition. Additional fluid accumulation in tissues and swelling (edema) may also occur. Slow and cautious initiation of parenteral nutrition is recommended.
Elevated magnesium blood levels:
The amount of magnesium present in NUMETA G16%E may cause increased magnesium levels in the blood. In such cases, the following symptoms may occur: weakness, slowed reflexes, nausea, vomiting, low blood calcium levels, breathing difficulties, low blood pressure, and irregular heartbeat. These symptoms may be difficult to detect; therefore, the physician may monitor magnesium levels in the child’s blood, especially in children with risk factors for elevated magnesium levels, such as impaired kidney function. If blood magnesium levels are elevated, the infusion will be paused or the infusion rate reduced.
Monitoring and adjustment:
The physician will closely monitor and adjust the administration of NUMETA G16%E according to the child’s individual needs in the following circumstances:
- severe post-traumatic conditions;
- severe diabetes;
- shock;
- heart attack;
- severe infection;
- certain types of coma.
Use with caution:
NUMETA G16%E should be used with caution if the child has:
- pulmonary edema (fluid in the lungs) or heart failure;
- severe liver dysfunction;
- impaired nutrient absorption;
- high blood sugar levels;
- kidney disease;
- severe metabolic disorders (when metabolic processes do not function normally);
- blood coagulation disorders.
The child’s fluid balance and laboratory test results (liver and/or blood tests) will be carefully monitored.
NUMETA G16%E and other medicines
Inform the physician about all medicines currently used or recently used by the child, as well as any medicines the child may take in the future.
NUMETA G16%E must not be administered at the same time as:
- ceftriaxone (antibiotic), even through separate infusion lines, due to the risk of solid particle formation;
- blood through the same infusion set, due to the risk of pseudoagglutination (clumping of red blood cells);
- ampicillin, fosphenytoin, or furosemide through the same infusion line, due to the risk of solid particle formation.
Coumarin and warfarin (anticoagulants):
The physician will closely monitor the child if coumarin or warfarin is being used.
Vitamin K1 is a natural component of olive oil and soybean oil. Vitamin K1 may interact with medications such as coumarin and warfarin. These drugs are anticoagulants used to prevent blood clotting.
Laboratory tests:
Lipids contained in this emulsion may affect the results of certain laboratory tests. Laboratory tests should be performed at least 5 to 6 hours after the last lipid administration.
Interactions of NUMETA G16%E with drugs affecting potassium levels/metabolism:
NUMETA G16%E contains potassium. High potassium levels in the blood may cause abnormal heart rhythms. Special care is required in patients receiving diuretics (medications intended to reduce fluid retention), ACE inhibitors (used for high blood pressure), angiotensin II receptor antagonists (used for high blood pressure), or immunosuppressive drugs (medications that may reduce the body’s normal immune response). These types of medications may increase potassium levels.
3. How to use NUMETA G16%E
NUMETA G16%E should always be administered to the child according to the doctor's instructions. In case of doubt, consult the doctor.
Age group
NUMETA G16%E has been designed to meet the nutritional needs of full-term newborns and children up to 2 years of age.
The child's doctor will decide whether this medicine is suitable for the child.
Administration
This medicine is an emulsion for infusion. It is administered through a plastic tube into a vein in the arm or into a large vein in the child's chest.
The doctor may decide not to administer lipids to the child. The NUMETA G16%E bag is designed so that, if necessary, only the partition between the chamber containing amino acids/electrolytes and the chamber containing glucose can be opened. In such a case, the partition between the amino acid chamber and the lipid chamber remains intact. In this way, the contents of the bag can be administered without lipids.
When used in newborns and children under 2 years of age, the solution (in bags and administration sets) must be protected from light until administration is completed (see section 2).
Dosage and duration of treatment
The doctor will determine the dose of the medicine and how long it will be administered. The dose depends on the child's nutritional needs. The dose will be established based on the child's body weight, clinical condition, and the body's ability to metabolize and utilize the components of NUMETA G16%E. Additional nutritional components or proteins administered orally or enterally may also be given.
Accidental administration of a higher dose of NUMETA G16%E than recommended
Symptoms
An overdose or too rapid administration may cause:
- nausea;
- vomiting;
- seizures;
- electrolyte disturbances (abnormal levels of electrolytes in the blood);
- symptoms of hypervolemia (increased circulating blood volume);
- acidosis (increased blood acidity).
In such situations as above, the infusion should be stopped immediately. The doctor will decide whether further actions are required.
Overdose of the fats contained in NUMETA G16%E may lead to the occurrence of a "fat overload syndrome," which usually resolves after stopping the infusion. In newborns (infants) and small children (children under 2 years of age), fat overload syndrome is associated with respiratory disturbances leading to reduced oxygen levels in the body (respiratory failure) and conditions leading to increased blood acidity (acidosis).
To prevent such situations, the doctor will systematically monitor the child's condition and perform blood tests during treatment.
4. Possible adverse reactions
Like all medicines, this medicine can cause adverse reactions, although not every child will experience them.
If you notice any changes in your child's health during or after treatment, inform the doctor or nurse immediately.
Medical examinations carried out while your child is receiving the medicine should minimize the risk of adverse reactions.
If symptoms of an allergic reaction occur, the infusion must be stopped immediately and the doctor should be contacted without delay. This may be serious, and symptoms may include:
- sweating
- chills
- headache
- skin rash
- breathing difficulties
Other observed adverse reactions:
Common: may affect up to 1 in 10 people
- Low phosphate levels in the blood (hypophosphatemia)
- High blood sugar levels (hyperglycemia)
- High calcium levels in the blood (hypercalcemia)
- High triglyceride levels in the blood (hypertriglyceridemia)
- Electrolyte disturbances (hyponatremia)
Uncommon: may affect up to 1 in 100 people
- High lipid levels in the blood (hyperlipidemia)
- Condition in which bile cannot flow from the liver to the duodenum (cholestasis). The duodenum is part of the intestine.
Unknown frequency: frequency cannot be estimated from the available data (These adverse reactions
have been reported only after peripheral administration of NUMETA G13%E Preterm and NUMETA G16%E
with insufficient dilution).
- Skin necrosis
- Soft tissue damage
- Extravasation
The following adverse reactions have been reported with other parenteral nutrition medicines:
Reduced or limited ability to clear lipids contained in NUMETA may lead to fat overload syndrome. The following signs and symptoms of this syndrome usually resolve after discontinuation of the fat emulsion infusion:
- Sudden and severe deterioration in the patient's clinical condition
- High fat levels in the blood (hyperlipidemia)
- Fever
- Fatty infiltration of the liver (hepatomegaly)
- Worsening liver function
- Decreased number of red blood cells, which may cause paleness of the skin and lead to weakness or shortness of breath (anemia)
- Decreased number of white blood cells, which may increase the risk of infection (leukopenia)
- Decreased number of platelets, which may increase the risk of bruising and/or bleeding (thrombocytopenia)
- Blood clotting disorders affecting the blood's ability to form clots
- Breathing disorders leading to reduced oxygen levels in the body (respiratory failure)
- Conditions leading to increased blood acidity (acidosis)
- Coma requiring hospitalization
Formation of small particles that may cause blockage of blood vessels in the lungs (pulmonary vessel deposits) or breathing difficulties.
Reporting of adverse reactions
If your child experiences any adverse reactions, consult the doctor or nurse. This includes any adverse effects not listed in this leaflet.
Adverse reactions can be reported directly to the Department of Monitoring Adverse Drug Reactions at the Office for Registration of Medicinal Products, Medical Devices and Biocidal Products
Al. Jerozolimskie 181 C
PL 02-222 Warsaw
Tel.: + 48 22 49 21 301
Fax: + 48 22 49 21 309
Website: https://smz.ezdrowie.gov.pl
Adverse reactions can also be reported to the marketing authorization holder.
By reporting adverse reactions, additional information on the safety of the medicine can be collected.
5. How to store NUMETA G16%E
The medicine should be stored out of sight and reach of children when not in use.
When used in newborns and children below 2 years of age, the solution (in bags and administration sets) must be protected from light until the end of administration (see section 2).
Do not use this medicine after the expiry date stated on the bag and outer packaging (MM/YYYY). The expiry date refers to the last day of the stated month.
Do not freeze.
Store in the protective bag.
Medicines must not be disposed of via wastewater or household waste. Ask your pharmacist how to dispose of medicines no longer required. Such measures help protect the environment.
6. Contents of the pack and other information
What NUMETA G16%E looks like and contents of the pack
NUMETA G16%E is contained in a three-compartment bag. The contents of each bag are sterile and consist of
a glucose solution, an amino acid solution for paediatric use with electrolytes, and a lipid emulsion,
as described below.
| Container size | 50% glucose solution | 5.9% amino acid solution with electrolytes | 12.5% fat emulsion |
| 500 ml | 155 ml | 221 ml | 124 ml |
Appearance before preparation:
- Solutions in chambers containing amino acids and glucose are clear, colorless or slightly yellow
- The chamber with fat emulsion is a homogeneous, milky white liquid
Appearance after preparation:
- "2 in 1" infusion solutions are clear, colorless or slightly yellow
- "3 in 1" infusion emulsion is homogeneous and milky white
The triple-chamber bag is a multilayer plastic bag.
To protect against exposure to air, the NUMETA bag is packaged in a protective bag that prevents oxygen access, containing an oxygen absorber and an oxygen indicator.
Pack sizes
500 ml bags: 6 bags in a cardboard box
1 x 500 ml bag
Not all pack sizes may be marketed.
Marketing Authorization Holder and Manufacturer
Marketing Authorization Holder
Baxter Polska Sp. z o.o.
ul. Kruczkowskiego 8
00-380 Warsaw
Manufacturer
Baxter S.A.
Boulevard Rene Branquart 80
7860 Lessines
Belgium
This medicinal product is authorized for marketing in the European Economic Area member states under the following names:
| Austria Germany | Numeta G 16 % E Emulsion for Infusion |
| Belgium Luxembourg | NUMETZAH G16%E, émulsion pour perfusion |
| France | NUMETAH G16 %E, émulsion pour perfusion |
| Denmark Norway Sweden | Numeta G16E |
| Czech Republic Greece | NUMETA G 16 % E |
| Netherlands | NUMETA G16%E emulsie voor infusie |
| Ireland United Kingdom | Numeta G16%E, Emulsion for Infusion |
| Italy | NUMETA G16%E emulsione per infusione |
| Finland | Numeta G16E infuusioneste, emulsio |
| Poland | NUMETA G16%E |
| Portugal | Numeta G16%E |
| Spain | NUMETA G16%E, emulsión para perfusión |
Information intended exclusively for healthcare professionals or medical personnel
*In some cases, this medicine may be administered at home by parents or other caregivers.
In such cases, parents/caregivers should read the information below.
Do not add any additional components to the bag without first checking compatibility.
This could lead to the formation of particulate matter or destabilization of the fat emulsion,
which may result in venous occlusion.
The NUMETA G16%E medicine should reach room temperature before administration.
Before administering NUMETA G16%E, prepare the bag as shown below.
Ensure the bag is undamaged. The bag may only be used if it is intact. The following are characteristics of an undamaged bag:
- Compartments are intact, indicated by the absence of mixing between the contents of any of the three chambers.
- The solutions containing amino acids and glucose are clear, colorless or slightly yellow, and free from visible particles.
- The fat emulsion is a uniform milky white liquid.
Before opening the protective overwrap, check the color of the oxygen absorber indicator.
- Compare it with the reference color printed next to the OK symbol and shown on the labeled area of the indicator label.
- Do not use the medicine if the oxygen indicator color does not match the reference color printed next to the OK symbol.
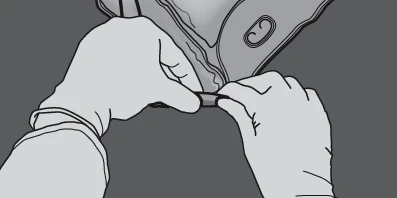
Figures 1 and 2 illustrate how to remove the protective overwrap. Discard the protective overwrap,
oxygen indicator, and oxygen absorber.
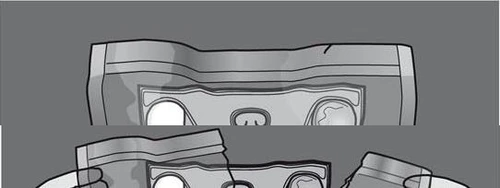

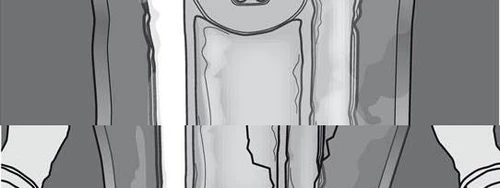





Figure 1 Figure 2
Preparation of the mixed emulsion:
- Before breaking the seals, ensure the medicine has reached room temperature.
- Place the bag on a flat, clean surface.
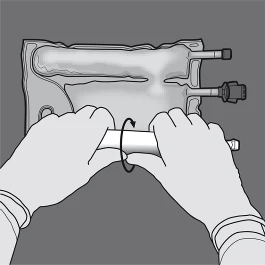
Activating the three-chamber bag (mixing 3 solutions by opening two breakable seals)
Step 1: Begin rolling the bag from the side with the hanger.
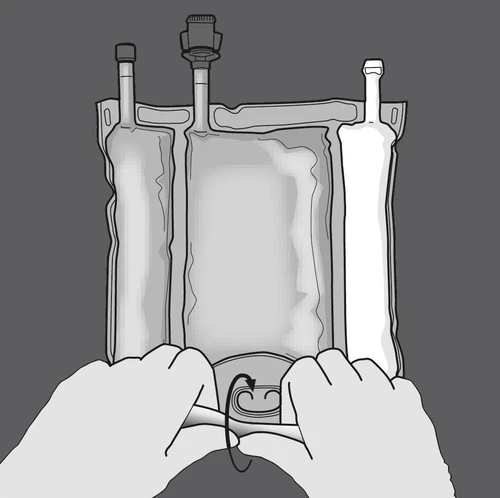
Step 2: Press until the seals open.
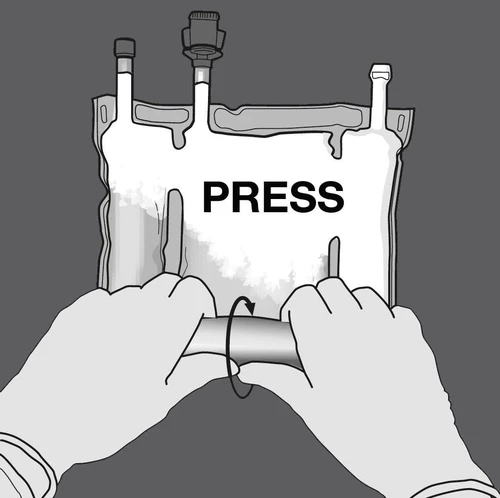
PRESS
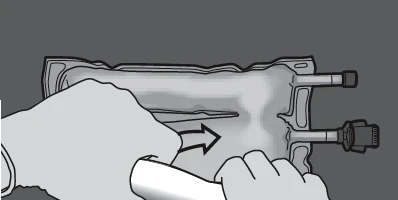
Step 3: Change direction by rolling the bag toward the hanger.
Continue until the seal is fully opened.
Repeat the same procedure to completely open the second seal.

PRESS

Step 4: Rotate the bag at least three times to thoroughly mix the contents.
The mixed solution should appear as a milky white emulsion.




Step 5: Remove the protective cap from the medication administration port and insert the intravenous administration set.



Activating the two-chamber bag (mixing 2 solutions by opening the breakable seal between the chambers containing amino acids and glucose)
Step 1: To mix only 2 solutions, roll the bag starting from the upper corner (with the hanger) adjacent to the seal separating the solutions.
Press to open the seal between the glucose and amino acid compartments.

PRESS
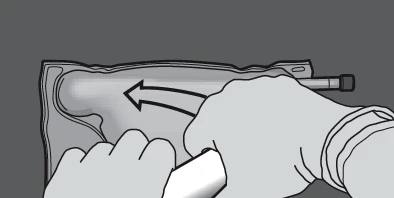
Step 2: Position the bag so that the fat emulsion chamber is closest to the user.
Roll the bag while protecting the fat emulsion chamber with your hands.
Step 3: Press with one hand and roll the bag toward the tubing.
PRESS

Step 4: Change direction by rolling the bag toward the upper end (with the hanger).
Press with the other hand until the seal separating the amino acid and glucose solutions is completely opened.
PRESS

Step 5: Rotate the bag at least three times to thoroughly mix the contents.
The mixed solution should be clear, colorless or slightly yellow.




Step 6: Remove the protective cap from the medication administration port and insert the intravenous administration set.




During the first hour, the infusion flow rate should be gradually increased. The infusion flow rate must be adjusted based on the following factors:
- dose administered
- total daily volume
- duration of infusion.
Method of administration:
When used in neonates and children under 2 years of age, the solution (in bags and administration sets) must be protected from light until the end of administration.
A 1.2-micron filter is recommended for administration of NUMETA G16%E.
Due to its high osmolarity, undiluted NUMETA G16%E must be administered only through a central vein.
Proper dilution of NUMETA G16%E with water for injections reduces osmolarity and allows infusion into a peripheral vessel.
The following formula illustrates the effect of dilution on the osmolarity of the medicine.

The table below provides examples of osmolarity of the activated two-chamber bag and the activated three-chamber bag after addition of water for injections:
| Amino acids and glucose (activated W2K) | Amino acids, glucose and lipids (activated W3K) | |
| Initial volume in the bag (ml) | 376 | 500 |
| Initial osmolarity (mOsm/l approximately) | 1585 | 1230 |
| Volume of added water (ml) | 376 | 500 |
| Final volume after addition (ml) | 752 | 1000 |
| Osmolarity after addition (mOsm/l approximately) | 792.5 | 615 |
Addition of additional components:
Exposure to light of solutions for parenteral nutrition, especially after mixing with trace elements and/or vitamins, may have an adverse effect on clinical outcomes in neonates due to the formation of peroxides and other degradation products. When used in neonates and children below 2 years of age, NUMETA G16%E must be protected from ambient light until the end of administration.
Compatible additional components may be added into the reconstituted mixture via the injection site (after breaking the peelable seals and after mixing the contents of two or three compartments). Vitamins may also be added into the glucose compartment prior to reconstitution (before breaking the peelable seals and before mixing the solutions and emulsion).
Possible additions of ready-to-use solutions of trace elements (identified as TE1, TE2 and TE4), vitamins (identified as lyophilisate V1 and emulsion V2) and electrolytes in specified quantities are presented in Tables 1–6.
- 1. Compatibility with TE4, V1 and V2
Table 1: Compatibility of 3-in-1 (activated W3K) with and without dilution with water
| For 500 ml (after mixing 3 compartments, with lipids) | ||||||
| Addition without dilution | Addition with dilution | |||||
| Additional components | Amount contained | Maximum added amount | Maximum total amount | Amount contained | Maximum added amount | Maximum total amount |
| Sodium (mmol) | 12.0 | 25.6 | 37.6 | 12.0 | 25.6 | 37.6 |
| Potassium (mmol) | 11.4 | 26.2 | 37.6 | 11.4 | 26.2 | 37.6 |
| Magnesium (mmol) | 1.6 | 3.6 | 5.2 | 1.6 | 3.6 | 5.2 |
| Calcium (mmol) | 3.1 | 16.4 | 19.5 | 3.1 | 8.2 | 11.3 |
| Phosphates* (mmol) | 4.4 | 6.9 | 11.3 | 4.4 | 6.9 | 11.3 |
| Trace elements and vitamins | 10 mL TE4 + 1 vial V1 + 30 mL V2 | 10 mL TE4 + 1 vial V1 + 30 mL V2 | 5 mL TE4 + ½ vial V1 + 5 mL V2 | 5 mL TE4 + ½ vial V1 + 5 mL V2 | ||
| Water for injections | 350 mL | 350 mL | ||||
Table 2: 2-in-1 compatibility (activated W2K) with dilution in water and without dilution
| For 376 ml (after mixing 2 chambers, without lipids) | ||||||
| Addition without dilution | Addition with dilution | |||||
| Additional components | Contained amount | Maximum added amount | Maximum total amount | Contained amount | Maximum added amount | Maximum total amount |
| Sodium (mmol) | 11.6 | 26.0 | 37.6 | 11.6 | 0.0 | 11.6 |
| Potassium (mmol) | 11.4 | 26.2 | 37.6 | 11.4 | 0.0 | 11.4 |
| Magnesium (mmol) | 1.6 | 3.6 | 5.2 | 1.6 | 0.0 | 1.6 |
| Calcium (mmol) | 3.1 | 8.2 | 11.3 | 3.1 | 0.0 | 3.1 |
| Phosphates* (mmol) | 3.2 | 8.1 | 11.3 | 3.2 | 0.0 | 3.2 |
| Trace elements and vitamins | 5 ml TE4 + ½ vial V1 | 5 ml TE4 + ½ vial V1 | 5 ml TE4 + ½ vial V1 | 5 ml TE4 + ½ vial V1 | ||
| Water for injections | 450 ml | 450 ml | ||||
- 2. Compatibility with TE1, V1 and V2 Table 3: 3-in-1 compatibility (activated W3K) with and without dilution in water
| For 500 ml (after mixing 3 compartments, with lipids) | ||||||
| Addition without dilution | Addition with dilution | |||||
| Additional components | Contained amount | Maximum added amount | Maximum total amount | Contained amount | Maximum added amount | Maximum total amount |
| Sodium (mmol) | 12.0 | 4.0 | 16.0 | 12.0 | 0.0 | 12.0 |
| Potassium (mmol) | 11.4 | 6.2 | 17.6 | 11.4 | 0.0 | 11.4 |
| Magnesium (mmol) | 1.6 | 0 | 1.6 | 1.6 | 0.0 | 1.6 |
| Calcium (mmol) | 3.1 | 2.1 | 5.2 | 3.1 | 0.0 | 3.1 |
| Phosphates* (mmol) | 4.4 | 2.0 | 6.4 | 4.4 | 0.0 | 4.4 |
| Trace elements and vitamins | 5 ml TE1 + ½ vial V1 + 5 ml V2 | 5 ml TE1 + ½ vial V1 + 5 ml V2 | 5 ml TE1 + ½ vial V1 + 5 ml V2 | 5 ml TE1 + ½ vial V1 + 5 ml V2 | ||
| Water for injections | 350 ml | 350 ml | ||||
Table 4: Compatibility of 2-in-1 (activated W2K) with dilution in water and without dilution
| For 376 ml (after mixing 2 compartments, without lipids) | ||||||
| Addition without dilution | Addition with dilution | |||||
| Additional components | Contained amount | Maximum added amount | Maximum total amount | Contained amount | Maximum added amount | Maximum total amount |
| Sodium (mmol) | 11.6 | 26.0 | 37.6 | 11.6 | 0.0 | 11.6 |
| Potassium (mmol) | 11.4 | 26.2 | 37.6 | 11.4 | 0.0 | 11.4 |
| Magnesium (mmol) | 1.6 | 3.6 | 5.2 | 1.6 | 0.0 | 1.6 |
| Calcium (mmol) | 3.1 | 8.2 | 11.3 | 3.1 | 0.0 | 3.1 |
| Phosphates* (mmol) | 3.2 | 8.1 | 11.3 | 3.2 | 0.0 | 3.2 |
| Trace elements and vitamins | 5 ml TE1 + ½ vial V1 | 5 ml TE1 + ½ vial V1 | 5 ml TE1 + ½ vial V1 | 5 ml TE1 + ½ vial V1 | ||
| Water for injections | 450 ml | 450 ml | ||||
- 3. Compatibility with TE2, V1 and V2 Table 5: 3-in-1 compatibility (activated W3K) with dilution in water and without dilution
| For 500 ml (after mixing 3 compartments, with lipids) | ||||||
| Additive without dilution | Additive with dilution | |||||
| Additional components | Amount contained | Maximum added amount | Maximum total amount | Amount contained | Maximum added amount | Maximum total amount |
| Sodium (mmol) | 12.0 | 4.0 | 16.0 | 12.0 | 0.0 | 12.0 |
| Potassium (mmol) | 11.4 | 6.2 | 17.6 | 11.4 | 0.0 | 11.4 |
| Magnesium (mmol) | 1.6 | 0 | 1.6 | 1.6 | 0.0 | 1.6 |
| Calcium (mmol) | 3.1 | 2.1 | 5.2 | 3.1 | 0.0 | 3.1 |
| Phosphates* (mmol) | 4.4 | 2.0 | 6.4 | 4.4 | 0.0 | 4.4 |
| Trace elements and vitamins | 5 ml TE2 + ½ vial V1 + 5 ml V2 | 5 ml TE2 + ½ vial V1 + 5 ml V2 | 5 ml TE2 + ½ vial V1 + 5 ml V2 | 5 ml TE2 + ½ vial V1 + 5 ml V2 | ||
| Water for injections | 350 ml | 350 ml | ||||
Table 6: Compatibility of 2-in-1 (activated W2K) with dilution in water and without dilution
| For 376 ml (after mixing 2 compartments, without lipids) | ||||||
| Addition without dilution | Addition with dilution | |||||
| Additional components | Content amount | Maximum added amount | Maximum total amount | Content amount | Maximum added amount | Maximum total amount |
| Sodium (mmol) | 11.6 | 26.0 | 37.6 | 11.6 | 0.0 | 11.6 |
| Potassium (mmol) | 11.4 | 26.2 | 37.6 | 11.4 | 0.0 | 11.4 |
| Magnesium (mmol) | 1.6 | 3.6 | 5.2 | 1.6 | 0.0 | 1.6 |
| Calcium (mmol) | 3.1 | 8.2 | 11.3 | 3.1 | 0.0 | 3.1 |
| Phosphates* (mmol) | 3.2 | 8.1 | 11.3 | 3.2 | 0.0 | 3.2 |
| Trace elements and vitamins | 5 ml TE2 + ½ vial V1 | 5 ml TE2 + ½ vial V1 | 5 ml TE2 + ½ vial V1 | 5 ml TE2 + ½ vial V1 | ||
| Water for injections | 450 ml | 450 ml | ||||
The composition of preparations containing vitamins and trace elements is presented in Tables 7 and 8.
Table 7: Composition of the ready-to-use trace element preparation used:
| Composition per 10 ml vial | TE1 | TE2 | TE4 |
| Iron | 8.9 µmol or 0.5 mg | ||
| Zinc | 38.2 µmol or 2.5 mg | 15.3 µmol or 1 mg | 15.3 µmol or 1 mg |
| Selenium | 0.253 µmol or 0.02 mg | 0.6 µmol or 0.05 mg | 0.253 µmol or 0.02 mg |
| Copper | 3.15 µmol or 0.2 mg | 4.7 µmol or 0.3 mg | 3.15 µmol or 0.2 mg |
| Iodine | 0.0788 µmol or 0.01 mg | 0.4 µmol or 0.05 mg | 0.079 µmol or 0.01 mg |
| Fluoride | 30 µmol or 0.57 mg | 26.3 µmol or 0.5 mg | |
| Molybdenum | 0.5 µmol or 0.05 mg | ||
| Manganese | 0.182 µmol or 0.01 mg | 1.8 µmol or 0.1 mg | 0.091 µmol or 0.005 mg |
| Cobalt | 2.5 µmol or 0.15 mg | ||
| Chromium | 0.4 µmol or 0.02 mg 18 |
Table 8: Composition of the ready-to-use preparation containing vitamins:
| Composition per vial | V1 | V2 |
| Vitamin B1 | 2.5 mg | |
| Vitamin B2 | 3.6 mg | |
| Nicotinamide | 40 mg | |
| Vitamin B6 | 4.0 mg | |
| Pantothenic acid | 15.0 mg | |
| Biotin | 60 µg | |
| Folic acid | 400 µg | |
| Vitamin B12 | 5.0 µg | |
| Vitamin C | 100 mg | |
| Vitamin A | 2300 IU | |
| Vitamin D | 400 IU | |
| Vitamin E | 7 IU | |
| Vitamin K | 200 µg |
Adding additional components:
- Aseptic conditions must be maintained.
- Prepare the injection site on the bag.
- Pierce the injection site and inject the additional components using a syringe or drug preparation device.
- Mix the contents of the bag containing the additional components.
Preparation of infusion:
- Aseptic conditions must be maintained.
- Hang the bag.
- Remove the plastic protector from the medication administration port.
- Firmly insert the infusion set spike into the medication administration port.
Infusion administration:
- For single use only.
- Administer the medicinal product only after breaking the seals between two or three chambers and mixing the contents of two or three chambers.
- Ensure that the final emulsion in the activated three-compartment infusion bag shows no phase separation, or that the final solution in the two-compartment infusion bag contains no solid particles.
- Immediate use after opening the peelable seals is recommended. NUMETA G16%E must not be stored for subsequent infusions.
- Partially used bags must not be connected.
- To avoid air embolism caused by residual air in the first bag, do not connect bags in series.
- A 1.2 micron filter is recommended for administration of NUMETA G16%E.
- When used in neonates and children below 2 years of age, protect from light until the end of administration. Exposure of NUMETA G16%E to ambient light, especially after mixing with trace elements and (or) vitamins, leads to the formation of peroxides and other degradation products, which can be reduced by protecting from light.
- Any unused medicinal product residues, waste, and all required single-use equipment must be appropriately disposed of.
Shelf-life after mixing solutions:
The medicinal product must be used immediately after opening the peelable seals between two or three chambers.
Stability studies of mixtures were conducted for 7 days at a temperature of 2°C to 8°C, followed by 48 hours at 30°C.
Shelf-life after adding additional components (electrolytes, trace elements, vitamins, water):
For specific additional components, physical stability of NUMETA has been demonstrated for 7 days at a temperature of 2°C to 8°C, followed by 48 hours at 30°C.
From a microbiological standpoint, the medicinal product should be used immediately. If not used immediately, the responsibility for storage conditions and duration prior to use lies with the user; however, standard practice should not exceed 24 hours at a temperature of 2°C to 8°C, unless preparation/dissolution/addition of components was performed under controlled and validated aseptic conditions.
Do not use NUMETA G16%E if the bag is damaged. The following are signs of a damaged bag:
- Peelable seals are open
- Any of the chambers already contain a mixture of solutions
- Solutions containing amino acids and glucose are not clear, colorless or slightly yellow, and (or) contain visible particles
- The fat emulsion is not a uniform milky-white liquid.
Medicinal products must not be disposed of via wastewater or household waste. Ask your pharmacist how to dispose of medicines no longer required. Such measures help protect the environment.
What NUMETA G16%E contains
Active substances:
| Composition | ||
| Active substance | Activated W2K (376 ml) | Activated W3K (500 ml) |
| Amino acid compartment | ||
| Alanine | 1.03 g | 1.03 g |
| Arginine | 1.08 g | 1.08 g |
| Aspartic acid | 0.77 g | 0.77 g |
| Cysteine | 0.24 g | 0.24 g |
| Glutamic acid | 1.29 g | 1.29 g |
| Glycine | 0.51 g | 0.51 g |
| Histidine | 0.49 g | 0.49 g |
| Isoleucine | 0.86 g | 0.86 g |
| Leucine | 1.29 g | 1.29 g |
| Lysine monohydrate (corresponds to lysine) | 1.59 g (1.42 g) | 1.59 g (1.42 g) |
| Methionine | 0.31 g | 0.31 g |
| Ornithine hydrochloride (corresponds to ornithine) | 0.41 g (0.32 g) | 0.41 g (0.32 g) |
| Phenylalanine | 0.54 g | 0.54 g |
| Proline | 0.39 g | 0.39 g |
| Serine | 0.51 g | 0.51 g |
| Taurine | 0.08 g | 0.08 g |
| Threonine | 0.48 g | 0.48 g |
| Tryptophan | 0.26 g | 0.26 g |
| Tyrosine | 0.10 g | 0.10 g |
| Valine | 0.98 g | 0.98 g |
| Sodium chloride | 0.30 g | 0.30 g |
| Potassium acetate | 1.12 g | 1.12 g |
| Calcium chloride dihydrate | 0.46 g | 0.46 g |
| Magnesium acetate tetrahydrate | 0.33 g | 0.33 g |
| Sodium glycerophosphate hydrate | 0.98 g | 0.98 g |
| Glucose compartment | ||
| Glucose monohydrate (corresponds to anhydrous glucose) | 85.25 g (77.50 g) | 85.25 g (77.50 g) |
| Lipid compartment | ||
| Purified olive oil (approx. 80%) + purified soybean oil (approx. 20%) | 15.5 g | |
The solution after mixing/emulsion contains the following ingredients:
| Composition | ||||
| Activated W2K | Activated W3K | |||
| Per unit volume (ml) Nitrogen (g) Amino acids (g) Glucose (g) Lipids (g) Energy value Total energy value (kcal) Non-protein energy value (kcal) Glucose energy value (kcal) Lipid energy value (kcal) Non-protein energy value/nitrogen (kcal/g N) Lipid energy value / non-protein energy value (%) Lipid energy value / total energy value (%) Electrolytes Sodium (mmol) Potassium (mmol) Magnesium (mmol) Calcium (mmol) Phosphatesb (mmol) | 376 2.0 13.0 77.5 0 362 310 310 0 158 Not applicable Not applicable 11.6 11.4 1.6 3.1 3.2 | 100 0.52 3.5 20.6 0 96 82 82 0 158 Not applicable Not applicable 3.1 3.0 0.41 0.82 0.85 | 500 2.0 13.0 77.5 15.5 517 465 310 155 237 33 30 12.0 11.4 1.6 3.1 4.4 | 100 0.39 2.6 15.5 3.1 103 93 62 31 237 33 30 2.4 2.3 0.31 0.62 0.87 |
| Acetates (mmol) Malate (mmol) Chloride (mmol) | 14.5 4.3 13.8 | 3.9 1.1 3.7 | 14.5 4.3 13.8 | 2.9 0.86 2.8 |
| pH (approximate) Approximate osmolarity (mOsm/l) | 5.5 1585 | 5.5 1585 | 5.5 1230 | 5.5 1230 |
This includes the energy value of egg phospholipids for injection.
This includes phosphates from egg phospholipids for injection, which are components of the lipid emulsion.
Other ingredients:
L-malic acid
Hydrochloric acid
Egg phospholipids for injection
Glycerol
Sodium oleate
Sodium hydroxide
Water for injections
for pH adjustment
Baxter, Numeta, Numetzah, and Numetah are trademarks of Baxter International Inc.