IG Vena
Italy
Table of Contents
- PACKAGE LEAFLET: INFORMATION FOR THE USER
- Ig VENA 50 g/l Solution for infusion
- 1. What Ig VENA is and what it is used for
- 2. What you should know before using Ig VENA
- 3. How to use Ig VENA
- 4. Possible side effects
- 5. How to store Ig VENA
- 6. Package contents and other information
- PATIENT INFORMATION LEAFLET: INFORMATION FOR THE USER
- Ig VENA 50 g/l Solution for infusion
- 1. What Ig VENA is and what it is used for
- 2. What you should know before using Ig VENA
- 3. How to use Ig VENA
- 4. Possible side effects
- 5. How to store Ig VENA
- 6. Package contents and other information
PACKAGE LEAFLET: INFORMATION FOR THE USER
Ig VENA 50 g/l Solution for infusion
Normal human immunoglobulin (IVIg) for intravenous use
Please read this leaflet carefully before using this medicine because it contains
important information for you.
- Keep this leaflet. You may need to read it again.
- If you have any questions, ask your doctor or nurse.
- If you experience any side effects, including those not listed in this leaflet, tell your doctor or nurse. See section 4.
Contents of this leaflet:
- What Ig VENA is and what it is used for
- What you need to know before using Ig VENA
- How to use Ig VENA
- Possible side effects
- How to store Ig VENA
- Contents of the pack and other information
1. What Ig VENA is and what it is used for
Ig VENA is a normal human immunoglobulin solution for intravenous use.
Immunoglobulins are human antibodies also present in blood.
Ig VENA is used for:
Treatment of adults, children and adolescents (0–18 years) who do not have sufficient antibodies
(replacement therapy) in the following cases:
- Patients with congenital deficiency in antibody production (primary immunodeficiency syndromes).
- Patients with acquired deficiency in antibody production (secondary immunodeficiencies) suffering from severe or recurrent infections due to various medical conditions (e.g. oncological or autoimmune diseases or as a consequence of treatment for such diseases). These patients have been treated with antibiotics proven ineffective and have not shown a sufficiently positive increase in IgG antibody titres after vaccination (pneumococcal vaccines with polysaccharide and polypeptide antigens), or have an IgG level in their blood < 4 g/l.
Treatment of adults, children and adolescents (0–18 years) with certain inflammatory diseases
(immunomodulation) in the following conditions:
- Patients with insufficient platelets (Primary Immune Thrombocytopenia, ITP) who are at high risk of bleeding or prior to surgical procedures to correct platelet count.
- Patients with Guillain-Barré syndrome. This is an acute disease characterized by inflammation of the peripheral nerves, causing severe muscle weakness, particularly in the legs and upper limbs.
- Patients with Kawasaki disease (in combination with acetylsalicylic acid). This is an acute disease affecting mainly young children, characterized by inflammation of blood vessels throughout the body.
- Patients with Chronic Inflammatory Demyelinating Polyradiculoneuropathy (CIDP). This chronic disease is a rare disorder of the peripheral nerves characterized by a gradual increase in weakness of the legs and, to a lesser extent, the arms.
- Patients with Multifocal Motor Neuropathy (MMN). This is a rare condition affecting motor nerves and characterized by slowly progressive, asymmetric limb weakness without loss of sensation.
2. What you should know before using Ig VENA
Do not use Ig VENA
If you are allergic (hypersensitive) to human immunoglobulins or to any of the other
components of this medicine (listed in section 6).
If you have antibodies in your blood directed against IgA-type immunoglobulins, because
administration of a product containing IgA may cause a severe allergic reaction.
Warnings and precautions
Talk to your doctor or nurse before using Ig VENA.
Your doctor or another healthcare professional will closely monitor and carefully observe you
throughout the entire Ig VENA infusion period to ensure no reactions occur.
Some adverse reactions may occur more frequently:
- if the infusion rate is too high;
- if you have untreated, uncontrolled infection symptoms (e.g., fever) or symptoms of chronic inflammation;
- if you are receiving normal human immunoglobulins for the first time;
- in the rare cases when the type of normal human immunoglobulin medicinal product has been changed, or when a long interval has passed since the previous infusion.
- In certain conditions, immunoglobulins may increase the risk of myocardial infarction, stroke, pulmonary embolism, or deep vein thrombosis because they increase blood viscosity. Therefore, your doctor will pay particular attention in the following circumstances:
- if you are overweight,
- if you are elderly,
- if you have diabetes,
- if you have high blood pressure (hypertension),
- if your blood volume is too low (hypovolemia),
- if you have or have had blood vessel problems (vascular diseases),
- if you have an increased tendency for blood clotting (inherited or acquired thrombophilic disorders),
- if you suffer from thrombotic episodes,
- if you have diseases that increase blood density (viscosity),
- if you have had a prolonged period of immobility,
- if you have or have had kidney problems or if you are taking medicines that may damage the kidneys (nephrotoxic medicines), as cases of acute kidney failure have been reported. If kidney damage occurs, your doctor will consider discontinuing treatment.
- You may be allergic (hypersensitive) to immunoglobulins (antibodies) without knowing it.
This may occur even if you have previously received normal human immunoglobulins and
tolerated prior administrations. This possibility is particularly relevant if you lack sufficient IgA-type immunoglobulins (IgA deficiency with anti-IgA antibodies).
In these rare cases, allergic (hypersensitivity) reactions such as a drop in blood pressure or shock may occur.
In case of an adverse reaction, your doctor will decide whether to reduce the infusion rate or
stop the infusion. Additionally, your doctor will determine the necessary treatment based on the nature
and severity of the adverse effect.
In case of shock, standard shock treatment must be administered. Inform your doctor if
you suffer from any of the conditions described above; your doctor will exercise particular caution when prescribing and administering Ig VENA to you.
Viral safety
Medicines prepared from human blood or plasma are subject to a number of safety measures to prevent transmission of infections to patients. These measures include careful selection of blood or plasma donors to ensure potentially infected donors are excluded, and testing of each donation and plasma pool to detect possible viral presence. In addition, manufacturers incorporate into the processing of blood or plasma certain steps capable of inactivating or removing pathogens.
Despite these measures, when administering medicines prepared from human blood or plasma, the possibility of transmitting infection cannot be completely excluded. This also applies to emerging or unknown viruses or other infectious agents.
The measures taken are considered effective against lipid-enveloped viruses such as human immunodeficiency virus (HIV), hepatitis B virus (HBV), hepatitis C virus (HCV), and the non-lipid-enveloped hepatitis A virus (HAV). The measures have limited effectiveness against non-lipid-enveloped viruses such as parvovirus B19.
Immunoglobulins have not been associated with hepatitis A or parvovirus B19 infections, which may be due to the protective capacity of the antibodies against these infections contained in the product.
It is strongly recommended to record the brand name and batch number each time you
receive a dose of Ig VENA, in order to maintain documentation of the batches used.
Children and adolescents
A mild and transient glycosuria (presence of glucose in urine) without clinical signs has been
observed in pediatric patients after administration of Ig VENA. This event may be related to the maltose content in Ig VENA, since in the renal tubules, maltose is hydrolyzed to glucose, which is reabsorbed and excreted in urine only in small amounts. Glucose reabsorption is an age-dependent mechanism. The transient increase in plasma maltose may exceed the kidney's capacity to reabsorb sugar, resulting in a positive glucose test in urine.
Other medicines and Ig VENA
Inform your doctor if you are taking, have recently taken, or might take any other
medicines.
Normal human immunoglobulins for intravenous use must not be mixed with other medicinal products, nor with other IVIg-based products.
Live attenuated virus vaccines
Administration of immunoglobulin may impair the efficacy of live attenuated virus vaccines such as those for measles, rubella, mumps, and varicella for a period of at least 6 weeks and up to 3 months. After administration of this product, a three-month interval must pass before vaccination with live attenuated virus vaccines. In the case of measles, this weakening of the immune response may last up to one year. Therefore, antibody levels should be monitored in patients receiving the measles vaccine.
Loop diuretics (a group of medicines that increase urine production)
Avoid concomitant use of loop diuretics.
Blood tests
Ig VENA may interfere with certain blood tests due to the temporary increase of various antibodies that, after immunoglobulin infusion, are passively transferred into your bloodstream; this increase in antibodies may cause certain blood tests to yield results that may not be accurate. Passive transfer of antibodies against erythrocyte antigens, e.g., A, B, D (determining blood group), may interfere with certain serological tests for red blood cell antibodies, for example, the direct antiglobulin test (DAT, direct Coombs test).
Blood glucose testing
Some blood glucose monitoring systems (e.g., those based on pyrroloquinoline quinone glucose dehydrogenase (GDH-PQQ) or glucose oxidoreductase colorimetric methods) falsely recognize the maltose (100 mg/ml) contained in Ig VENA as glucose. This may result in falsely elevated blood glucose readings during the infusion and for approximately 15 hours after the infusion ends, potentially leading to inappropriate insulin administration, posing a life-threatening risk or even fatal hypoglycemia.
Additionally, actual hypoglycemia may go untreated if the hypoglycemic state is masked by falsely elevated glucose values. Therefore, during administration of Ig VENA or other parenteral products containing maltose, blood glucose measurement must be performed using glucose-specific methods. The instructions for use of the glucose monitoring system, including those for test strips, must be carefully reviewed to determine whether the system is suitable for use in patients treated with parenteral products containing maltose. If in doubt, contact the manufacturer of the glucose monitoring system to determine its suitability for use with parenteral products containing maltose.
Children and adolescents
Although specific interaction studies have not been conducted in the pediatric population, no differences from adult patients are expected.
Pregnancy, breastfeeding, and fertility
- If you are pregnant, suspect you may be pregnant, are planning pregnancy, or are breastfeeding, consult your doctor before taking this medicine. Your doctor will decide whether it is appropriate to use Ig VENA during pregnancy and breastfeeding.
- Clinical studies with Ig VENA have not been conducted in pregnant women. It has been shown that intravenous human immunoglobulin products cross the placenta increasingly during the third trimester. However, antibody-containing medicines have been used for years in pregnant women, and no harmful effects on the course of pregnancy, the fetus, or the newborn are expected.
- If you are breastfeeding and receiving Ig VENA treatment, the antibodies contained in the product may pass into breast milk. Therefore, your baby may be protected from certain infections.
- Clinical experience with immunoglobulins suggests that no harmful effects on fertility are expected.
Driving and operating machinery
The ability to drive vehicles or operate machinery may be impaired by certain adverse
reactions associated with Ig VENA. Patients experiencing adverse reactions during treatment should wait until symptoms resolve before driving or operating machinery.
Ig VENA contains maltose and sodium
The product contains 100 mg of maltose per ml.
This medicinal product contains approximately 69 mg of sodium per liter. This should be taken into account for patients on a controlled sodium diet.
3. How to use Ig VENA
Ig VENA can only be used in hospitals or clinics and healthcare facilities by medical professionals
or other healthcare providers.
The dose and treatment schedule depend on the indication; your doctor will determine the appropriate
dose and treatment regimen for you.
At the beginning of the infusion, you will receive Ig VENA at a low infusion rate. If you tolerate it well,
your doctor may gradually increase the infusion rate.
Use in children and adolescents
The dosage in children and adolescents (0–18 years) is not different from that in adults, since the dosage
for each indication is based on body weight and adjusted according to the patient's clinical response.
If you use more Ig VENA than you should
If you are administered more Ig VENA than recommended, fluid overload may occur and the blood may become too thick (hyperviscous); this is particularly evident in at-risk patients, especially elderly patients or those with impaired cardiac or renal function.
If you have any doubts about the use of this medicine, consult your doctor or nurse.
4. Possible side effects
Like all medicines, this medicine can cause side effects, although not everybody gets them.
The following side effects may generally occur after treatment with immunoglobulins:
- chills, headache, dizziness, fever, vomiting, nausea, allergic reactions, arthralgia (joint pain), drop in blood pressure, and moderate lower back pain have been reported occasionally;
- isolated cases of temporary reduction in red blood cells (reversible haemolytic anaemia/haemolysis);
- a sudden drop in blood pressure has been reported rarely and, in some isolated cases, hypersensitivity reactions (anaphylactic shock) may occur, even when the patient has not shown reactions to previous administrations;
- rare cases of transient skin reactions have been observed;
- very rarely, thromboembolic reactions (blood clot formation) have been observed, which may lead to myocardial infarction, stroke, blockage of the pulmonary veins (pulmonary embolism), and deep vein thrombosis;
- cases of transient non-infectious meningitis (reversible aseptic meningitis);
- increased creatinine levels in the blood and/or cases of sudden kidney failure have been reported;
- cases of transfusion-related acute lung injury (TRALI).
The side effects reported during administration of Ig VENA in clinical studies and those reported after marketing of the medicine are listed below in order of decreasing frequency.
Common (may affect up to 1 in 10 people):
- Back pain
- Nausea
- Generalised weakness, fatigue, fever
- Muscle pain
- Headache, drowsiness
Frequency not known (cannot be estimated from the available data):
- Non-infectious meningitis
- Destruction and consequent lack of red blood cells
- Allergic reactions and life-threatening allergic shock
- Confusion
- Stroke, dizziness, involuntary tremor, numbness and tingling of the skin or a limb
- Heart attack, bluish or purplish skin discolouration, rapid heartbeat, slow heartbeat, irregular heartbeat
- Blood clots in major veins and blood vessels, low blood pressure, high blood pressure, pallor
- Blood clots in a major artery of the lungs, abnormal fluid volume in the lungs, difficulty breathing with shortness of breath and cough
- Vomiting, diarrhoea, abdominal pain
- Rapid swelling of the skin, hives, redness and inflammation of the skin, skin rash, itching, eczema, excessive sweating
- Pain in muscles and joints, back pain, neck pain, musculoskeletal stiffness
- Sudden kidney failure
- Vein inflammation at the injection site, chills, chest pain or discomfort, facial swelling, general feeling of malaise
- Increased creatinine levels in the blood
Additional side effects in children and adolescents
The frequency, type, and severity of adverse reactions in children are expected to be the same as in adults.
A slight and transient glycosuria (presence of glucose in urine) without clinical significance has been observed in children after administration of Ig VENA.
For information on viral safety, see section 2 "Before you use Ig VENA".
Reporting of side effects
If you experience any side effects, including those not listed in this leaflet, talk to your doctor or nurse. You can also report side effects directly via the national reporting system at:
https://www.aifa.gov.it/content/segnalazioni-reazioni-avverse.
By reporting side effects, you can help provide more information on the safety of this medicine.
5. How to store Ig VENA
Keep this medicine out of the sight and reach of children.
Do not use this medicine after the expiry date stated on the label and outer packaging following “Exp.”. The expiry date refers to the last day of the month.
Store in a refrigerator (2 °C - 8 °C).
Once the infusion container has been opened, the contents must be used immediately.
Keep the vial in the outer packaging.
Do not freeze.
Do not use this medicine if you notice that the solution is cloudy or contains particles or has changed in colour.
Do not dispose of medicines via wastewater or household waste. Ask your pharmacist how to dispose of medicines no longer required. This will help protect the environment.
6. Package contents and other information
What Ig VENA contains
The active substance in Ig VENA is normal human immunoglobulin.
One ml of solution contains 50 mg of normal human immunoglobulin.
The solution contains human proteins at a concentration of 50 g/l, of which at least 95% consists of
immunoglobulin G (IgG).
The distribution of immunoglobulin G (IgG) subclasses is as follows:
IgG 62.1%
IgG 34.8%
IgG 2.5%
IgG 0.6%
The maximum IgA content is 50 micrograms/ml.
Prepared from plasma obtained from human donors.
The other components are maltose and water for injections.
Description of the appearance of Ig VENA and contents of the package
Ig VENA is an infusion solution contained in single vials of 20 ml. The solution is clear or slightly opalescent, colourless or pale yellow.
Packaging:
1 vial containing 1 g/20 ml.
Marketing Authorisation Holder and Manufacturer
Marketing Authorisation Holder:
Kedrion S.p.A. - Loc. Ai Conti, 55051 Castelvecchio Pascoli, Barga (Lucca) - ITALY.
Manufacturer: Kedrion S.p.A., 55027 Bolognana, Gallicano (Lucca) - ITALY.
This medicinal product is authorised in the Member States of the European Economic Area under the following names:
| Austria | Ig Vena 50 g/l Infusion solution |
| Germany | Ig Vena 50 g/l Infusion solution |
| Greece | Ig VENA |
| Italy | Ig VENA |
| Poland | Ig VENA |
| Portugal | Ig Vena |
The following information is intended exclusively for physicians or healthcare professionals:
Instructions for Proper Use
- Prior to administration, bring the product to room or body temperature.
- Prior to administration, visually inspect the solution for particulate matter or discoloration. Do not use solutions that are cloudy or contain deposits.
- Normal human immunoglobulin must be administered intravenously at an initial rate of 0.46–0.92 mL/kg/h (10–20 drops per minute) for 20–30 minutes. In case of an adverse reaction, the infusion rate must be reduced or the infusion stopped. If well tolerated, the infusion rate may be gradually increased up to a maximum of 1.85 mL/kg/h (40 drops/minute).
- In patients with PID who tolerate an infusion rate of 0.92 mL/kg/h, the infusion rate may be gradually increased to 2 mL/kg/h, then 4 mL/kg/h, and up to a maximum of 6 mL/kg/h, every 20–30 minutes, but only if the patient tolerates the infusion well.
- In general, dosage and infusion rate must be individually adjusted according to the patient's needs. Depending on body weight, dosage, and the occurrence of adverse reactions, the patient may not reach the maximum infusion rate. In case of an adverse reaction, the infusion must be stopped immediately and restarted at the most appropriate rate for the patient.
Special Populations
In pediatric patients (0–18 years) and elderly patients (>64 years), the initial infusion rate should be 0.46–0.92 mL/kg/h (10–20 drops per minute) for 20–30 minutes. If well tolerated and based on the patient's clinical condition, the infusion rate may be gradually increased up to a maximum of 1.85 mL/kg/h (40 drops/minute).
Special Precautions
Some serious adverse reactions to the product may be due to the infusion rate. Potential complications can often be avoided by ensuring:
- that patients are not sensitive to normal human immunoglobulin by initially administering the product slowly (at an infusion rate between 0.46 and 0.92 mL/kg/h);
- that patients are closely monitored for any symptoms during the infusion period. In particular, patients receiving normal human immunoglobulin for the first time, patients who have switched from another IVIg product, and patients with a long interval since their previous infusion should be monitored during and for the first hour after the first infusion to detect potential signs of adverse reactions. All other patients should be observed for at least 20 minutes after administration. In all patients, IVIg administration requires:
- adequate hydration before starting IVIg infusion;
- monitoring of urinary output;
- monitoring of serum creatinine levels;
- avoidance of concomitant use of loop diuretics. In case of an adverse reaction, the infusion rate must be reduced or the infusion stopped. The necessary treatment depends on the nature and severity of the adverse effect. In case of shock, standard medical treatment for shock must be initiated.
Infusion Reactions
Some adverse reactions (e.g., headache, flushing, chills, myalgia, wheezing, tachycardia, back pain, nausea, and hypotension) may be related to the infusion rate. The recommended infusion rate must be carefully followed. Patients must be closely monitored and carefully observed for any symptoms during the infusion period.
Adverse reactions may occur more frequently:
- in patients receiving normal human immunoglobulin for the first time, or, in rare cases, when switching to a different immunoglobulin product, or after a long interval since the previous infusion;
- in patients with untreated infection or chronic inflammation.
Children and Adolescents
No specific measures or monitoring are required for the pediatric population.
No differences are expected in the pediatric population (0–18 years).
Thromboembolism
Clinical evidence shows an association between IVIg administration and thromboembolic events such as myocardial infarction, cerebrovascular accident (including stroke), pulmonary embolism, and deep vein thrombosis, presumed to be related to a relative increase in blood viscosity due to a high influx of immunoglobulin in at-risk patients.
Caution is required when prescribing and infusing IVIg in obese patients and in patients with pre-existing risk factors for thrombotic events (such as advanced age, hypertension, diabetes mellitus, history of vascular disease or thrombotic episodes, patients with inherited or acquired thrombophilic disorders, patients immobilized for prolonged periods, severely hypovolemic patients, or patients with conditions that increase blood viscosity).
In patients at risk of thromboembolic adverse reactions, IVIg products should be administered at the lowest feasible infusion rate and dose.
Acute Renal Failure
Cases of acute renal failure have been reported in patients receiving IVIg. In most cases, risk factors were identified, including pre-existing renal insufficiency, diabetes mellitus, hypovolemia, overweight, concomitant administration of nephrotoxic drugs, or age over 65 years.
Renal parameters should be evaluated before IVIg infusion, particularly in patients considered potentially at risk of developing acute renal failure, and again at appropriate intervals. In patients at risk of acute renal failure, IVIg products should be administered at the lowest feasible infusion rate and dose.
If renal function changes occur, discontinuation of IVIg treatment should be considered. Although cases of renal dysfunction and acute renal failure have been associated with the use of many IVIg products containing various excipients such as sucrose, glucose, and maltose, those containing sucrose as a stabilizer represent a very high proportion of the total number. In at-risk patients, the use of IVIg products not containing these excipients may be considered.
Aseptic Meningitis Syndrome (AMS)
Aseptic meningitis syndrome may occur in association with IVIg treatment.
The syndrome typically begins within several hours to 2 days after IVIg administration. Cerebrospinal fluid (CSF) studies often show pleocytosis (up to several thousand cells/mm³), predominantly granulocytes, and elevated protein levels (up to several hundred mg/dL).
AMS may occur more frequently with high-dose IVIg (2 g/kg).
Patients presenting with such signs and symptoms should undergo a complete neurological evaluation, including CSF studies, to exclude other causes of meningitis.
Discontinuation of IVIg treatment has led to resolution of AMS within a few days, without sequelae.
Hemolytic Anemia
IVIg products may contain blood group-specific antibodies that can act as hemolysins and induce in vivo coating of red blood cells with immunoglobulins, resulting in a positive direct antiglobulin reaction (Coombs test) and, rarely, hemolysis.
Hemolytic anemia may develop following IVIg therapy due to increased sequestration of red blood cells. Patients receiving IVIg should be monitored for clinical signs and symptoms of hemolysis.
Neutropenia/Leukopenia
A transient decrease in neutrophil count and/or episodes of neutropenia, sometimes severe, have been reported after IVIg treatment. This typically occurs within a few hours or days after IVIg administration and resolves spontaneously within 7–14 days.
Transfusion-Related Acute Lung Injury (TRALI)
A few cases of non-cardiogenic acute pulmonary edema (transfusion-related acute lung injury, TRALI) have been reported in patients receiving IVIg. TRALI is characterized by severe hypoxia, dyspnea, tachypnea, cyanosis, fever, and hypotension. Symptoms associated with TRALI typically appear during or within 6 hours of infusion, usually within 1–2 hours. Therefore, patients receiving IVIg must be monitored, and IVIg infusion must be immediately stopped if pulmonary adverse reactions occur. TRALI is a condition that may be life-threatening and may require immediate admission to an intensive care unit.
This product contains 100 mg of maltose per mL as an excipient. Maltose interference with blood glucose testing may lead to overestimation of glucose values and, consequently, inappropriate insulin administration, which may result in life-threatening hypoglycemia and patient death. Additionally, true hypoglycemia may remain untreated if the hypoglycemic state is masked by falsely elevated glucose readings. For further details, see the section “Blood Glucose Testing”.
Dosage Recommendations
Replacement therapy must be initiated and monitored under the supervision of a physician experienced in the treatment of immunodeficiency.
Dosage
The dose and dosing regimen depend on the indication. The dose must be individualized for each patient based on clinical response. Weight-based dosing may require adjustment in underweight or overweight patients.
The following dosing regimens may be used as a reference.
Replacement Therapy in Primary Immunodeficiency Syndromes
The dosing regimen should aim to achieve a trough IgG level (measured just before the next infusion) of at least 6 g/L or within the normal reference range for the patient's age group. From the start of therapy, it may take 3 to 6 months to reach steady-state IgG levels.
The recommended initial dose is 0.4–0.8 g/kg as a single infusion, followed by at least 0.2 g/kg administered every 3–4 weeks. The monthly dose required to achieve a trough IgG level of 6 g/L is approximately 0.2–0.8 g/kg/month. The interval between doses ranges from 3 to 4 weeks once steady state is achieved. Trough IgG levels should be measured and evaluated together with the frequency of infections. Dose increases and higher trough levels may be necessary to reduce the frequency of bacterial infections.
Secondary Immunodeficiencies
The recommended dose is 0.2–0.4 g/kg every 3–4 weeks.
Trough IgG levels should be measured and evaluated together with infection frequency. The dose should be adjusted as needed to achieve optimal protection against infections. Dose increases may be necessary in patients with persistent infection; dose reduction may be considered when the patient remains infection-free.
Primary Immune Thrombocytopenia
Two alternative treatment regimens are available:
- 0.8–1 g/kg administered on Day 1; this dose may be repeated once within 3 days;
- 0.4 g/kg/day for 2–5 days. Treatment may be repeated in case of relapse.
Guillain-Barré Syndrome
0.4 g/kg/day for 5 days (dose repetition possible in case of relapse).
Kawasaki Disease
2.0 g/kg should be administered as a single dose. Patients must receive concomitant treatment with acetylsalicylic acid.
Chronic Inflammatory Demyelinating Polyradiculoneuropathy (CIDP)
Initial dose: 2 g/kg divided over 2–5 consecutive days.
Maintenance doses: 1 g/kg over 1–2 consecutive days every 3 weeks.
The treatment effect should be evaluated after each cycle; if no treatment effect is observed after 6 months, treatment should be discontinued.
If therapy is effective, long-term administration is at the physician’s discretion based on patient response and maintenance of response. Dose and intervals may need to be adjusted according to the individual disease course.
Multifocal Motor Neuropathy (MMN)
Initial dose: 2 g/kg administered over 2–5 consecutive days.
Maintenance doses: 1 g/kg every 2–4 weeks or 2 g/kg every 4–8 weeks.
The treatment effect should be evaluated after each cycle; if no treatment effect is observed after 6 months, treatment should be discontinued.
If therapy is effective, long-term administration is at the physician’s discretion based on patient response and maintenance of response. Dose and intervals may need to be adjusted according to the individual disease course.
The recommended doses are summarized in the following table:
| Indication | Dose | Frequency of injections |
| Replacement therapy | ||
| Primary immunodeficiency syndromes | Initial dose: 0.4–0.8 g/kg Maintenance dose: 0.2–0.8 g/kg | every 3–4 weeks |
| Secondary immunodeficiencies | 0.2–0.4 g/kg | every 3–4 weeks |
| Immunomodulation: | ||
| Primary immune thrombocytopenia | 0.8–1 g/kg Or 0.4 g/kg/day | Day 1, possibly repeated once within 3 days for 2–5 days |
| Guillain-Barré syndrome | 0.4 g/kg/day | for 5 days |
| Kawasaki disease | 2 g/kg | single dose, in combination with acetylsalicylic acid |
| Chronic inflammatory demyelinating polyradiculoneuropathy (CIDP) | Initial dose: 2 g/kg Maintenance dose: 1 g/kg | divided over 2–5 days every 3 weeks; administered over 1–2 days |
| Multifocal motor neuropathy (MMN) | Initial dose: 2 g/kg Maintenance dose: 1 g/kg Or 2 g/kg | over 2–5 consecutive days every 2–4 weeks Or every 4–8 weeks over 2–5 days |
Use in children and adolescents
The dosage in children and adolescents (0–18 years) does not differ from that in adults, as the dosage for each indication is based on body weight and adjusted according to the clinical outcome of the aforementioned conditions.
Hepatic impairment
There is no evidence to require dose adjustment.
Renal impairment
No dose adjustment is necessary unless clinically justified.
Elderly
No dose adjustment is necessary unless clinically justified.
CIDP
Due to the rarity of the disease and, consequently, the small overall number of patients, experience with the use of intravenous immunoglobulins in children with CIDP is limited; therefore, only literature data are available. However, published data consistently show that IVIg treatment is equally effective in children and adults, in line with what is observed for the established indications for IVIg.
PATIENT INFORMATION LEAFLET: INFORMATION FOR THE USER
Ig VENA 50 g/l Solution for infusion
Human normal immunoglobulin (IVIg) for intravenous use
Please read this leaflet carefully before using this medicine
because it contains important information for you.
- Keep this leaflet. You may need to read it again.
- If you have any questions, ask your doctor or nurse.
- If you experience any side effects, including those not listed in this leaflet, tell your doctor or nurse. See section 4.
Contents of this leaflet:
- What Ig VENA is and what it is used for
- What you need to know before using Ig VENA
- How to use Ig VENA
- Possible side effects
- How to store Ig VENA
- Contents of the pack and other information
1. What Ig VENA is and what it is used for
Ig VENA is a normal human immunoglobulin solution for intravenous use.
Immunoglobulins are human antibodies also present in blood.
Ig VENA is used for:
Treatment of adults, children and adolescents (0–18 years) who do not have sufficient antibodies
(replacement therapy) in the following cases:
- Patients with congenital deficiency in antibody production (primary immunodeficiency syndromes).
- Patients with acquired deficiency in antibody production (secondary immunodeficiencies) suffering from severe or recurrent infections due to various medical conditions (e.g. oncological or autoimmune diseases or as a consequence of treatment for such diseases). These patients have undergone antibiotic treatment proven ineffective and have not shown a sufficiently positive increase in IgG antibody titers after vaccination (pneumococcal vaccines with polysaccharide and polypeptide antigens), or have an IgG level in their blood < 4 g/l.
Treatment of adults, children and adolescents (0–18 years) with certain inflammatory diseases
(immunomodulation) in the following conditions:
- Patients with insufficient platelets (Primary Immune Thrombocytopenia, ITP) who are at high risk of bleeding or prior to surgical procedures to correct platelet count.
- Patients with Guillain-Barré syndrome. This is an acute disease characterized by inflammation of the peripheral nerves, causing severe muscle weakness, particularly in the legs and upper limbs.
- Patients with Kawasaki disease (in combination with acetylsalicylic acid). This is an acute disease affecting mainly young children, characterized by inflammation of blood vessels throughout the body.
- Patients with Chronic Inflammatory Demyelinating Polyradiculoneuropathy (CIDP). This chronic disease is a rare disorder of the peripheral nerves characterized by a gradual increase in weakness of the legs and, to a lesser extent, the arms.
- Patients with Multifocal Motor Neuropathy (MMN). This is a rare condition affecting motor nerves and characterized by slowly progressive, asymmetric limb weakness without loss of sensation.
2. What you should know before using Ig VENA
Do not use Ig VENA
If you are allergic (hypersensitive) to human immunoglobulins or to any of the other
components of this medicine (listed in section 6).
If you have antibodies in your blood directed against IgA-type immunoglobulins, because
administration of a product containing IgA may cause a severe allergic reaction.
Warnings and precautions
Talk to your doctor or nurse before using Ig VENA.
Your doctor or another healthcare professional will closely monitor you and observe you carefully
throughout the entire Ig VENA infusion period to ensure that no reactions occur.
Adverse reactions may occur more frequently:
-
if the infusion rate is too high;
-
if you have uncontrolled symptoms of untreated infections (e.g. fever) or symptoms of chronic inflammation;
-
if you are receiving normal human immunoglobulins for the first time;
-
in rare cases when switching from another type of normal human immunoglobulin medicinal product, or after a long interval since the previous infusion.
-
In certain conditions, immunoglobulins may increase the risk of myocardial infarction, stroke, pulmonary embolism, or deep vein thrombosis because they increase blood viscosity. Therefore, your doctor will exercise particular caution in the following circumstances:
-
if you are overweight,
-
if you are elderly,
-
if you have diabetes,
-
if you have high blood pressure (hypertension),
-
if your blood volume is too low (hypovolemia),
-
if you have or have had blood vessel problems (vascular diseases),
-
if you have an increased tendency for blood to clot (inherited or acquired thrombophilic disorders),
-
if you suffer from thrombotic episodes,
-
if you have diseases that increase blood density (viscosity),
-
if you have had a prolonged period of immobility,
-
if you have or have had kidney problems or if you are taking medicines that may damage the kidneys (nephrotoxic medicines), as cases of acute kidney failure have been reported. In case of kidney damage, your doctor will consider stopping treatment.
-
You may be allergic (hypersensitive) to immunoglobulins (antibodies) without knowing it. This may occur even if you have previously received normal human immunoglobulins and tolerated prior administrations. This possibility is particularly relevant if you lack sufficient IgA-type immunoglobulins (IgA deficiency with anti-IgA antibodies).
In these rare cases, allergic reactions (hypersensitivity reactions) such as a drop in blood pressure or shock may occur.
If an adverse reaction occurs, your doctor will decide whether to reduce the infusion rate or
stop the infusion. Additionally, your doctor will determine the necessary treatment based on the
nature and severity of the adverse effect.
In case of shock, standard shock treatment must be administered. Inform your doctor if you
have any of the conditions described above; your doctor will use particular caution when prescribing and administering Ig VENA to you.
Viral safety
Medicines prepared from human blood or plasma are subject to a number of safety measures to
prevent transmission of infections to patients. These measures include careful selection of blood or plasma donors to ensure potentially infected donors are excluded, and testing of each donation and plasma pool to detect possible presence of viruses. Manufacturers of these medicines also include in the manufacturing process certain steps capable of inactivating or removing pathogens.
Despite these measures, when administering medicines prepared from human blood or plasma,
the possibility of transmitting an infection cannot be completely ruled out. This also applies to
emerging or unknown viruses or other types of infectious agents.
The measures taken are considered effective against lipid-enveloped viruses such as human
immunodeficiency virus (HIV), hepatitis B virus (HBV), hepatitis C virus (HCV), and against the non-lipid-enveloped hepatitis A virus (HAV). The measures have limited effectiveness against non-lipid-enveloped viruses such as parvovirus B19.
Immunoglobulins have not been associated with hepatitis A or parvovirus B19 infections, which may be due to the presence of antibodies against these infections in the product, providing protective effects.
It is strongly recommended to record the brand name and batch number each time you receive a dose of Ig VENA, to maintain documentation of the batches used.
Children and adolescents
A slight and transient glucosuria (presence of glucose in urine) without clinical signs has been
observed in pediatric patients after administration of Ig VENA. This event may be related to the
maltose content in Ig VENA, since in the renal tubules, maltose is hydrolyzed to glucose, which is
reabsorbed and excreted in urine only in small amounts under normal conditions. Glucose reabsorption is an age-dependent mechanism. The transient increase in plasma maltose may exceed the kidney's capacity to reabsorb sugar, resulting in a positive urine glucose test.
Other medicines and Ig VENA
Inform your doctor if you are taking, have recently taken, or might take any other medicines.
Normal human immunoglobulins for intravenous use must not be mixed with other medicinal
products, nor with other IVIg-based products.
Live attenuated virus vaccines
Administration of immunoglobulin may alter the efficacy of live attenuated virus vaccines such as those for measles, rubella, mumps, and varicella for a period of at least 6 weeks and up to 3 months. A three-month interval should elapse after administration of this product before vaccination with live attenuated virus vaccines. In the case of measles, this weakening of the immune response may last up to one year. Therefore, antibody levels should be monitored in patients receiving the measles vaccine.
Loop diuretics (a group of medicines that increase urine production)
Avoid concomitant use of loop diuretics.
Blood tests
Ig VENA may interfere with certain blood tests due to the temporary increase in various antibodies that are passively transferred into your bloodstream after immunoglobulin infusion; this increase in antibodies may cause certain blood tests to yield results that may not be accurate. Passive transfer of antibodies against erythrocyte antigens, e.g., A, B, D (determining blood group), may interfere with certain serological tests for red blood cell antibodies, for example, the direct antiglobulin test (DAT, direct Coombs test).
Blood glucose testing
Some blood glucose monitoring systems (e.g., those based on pyrroloquinoline quinone glucose dehydrogenase (GDH-PQQ) or glucose oxidoreductase colorimetric methods) falsely recognize the maltose (100 mg/ml) contained in Ig VENA as glucose. This may result in falsely elevated blood glucose readings during the infusion and for approximately 15 hours after the infusion ends, potentially leading to inappropriate insulin administration, posing a life-threatening risk or even fatal hypoglycemia.
Additionally, actual episodes of hypoglycemia may remain untreated if the hypoglycemic state is masked by falsely elevated glucose readings.
Therefore, during administration of Ig VENA or other parenteral products containing maltose, blood glucose measurement must be performed using glucose-specific methods. The instructions for use of the glucose monitoring system, including those for test strips, must be carefully reviewed to determine whether the system is suitable for use in patients receiving parenteral products containing maltose. If in doubt, contact the manufacturer of the glucose monitoring system to confirm its suitability for use with parenteral products containing maltose.
Children and adolescents
Although no specific interaction studies have been conducted in the pediatric population, no differences from adult patients are expected.
Pregnancy, breastfeeding, and fertility
- If you are pregnant, suspect you may be pregnant, planning a pregnancy, or breastfeeding, consult your doctor before taking this medicine. Your doctor will decide whether it is appropriate to use Ig VENA during pregnancy and breastfeeding.
- Clinical studies with Ig VENA have not been conducted in pregnant women. It has been shown that intravenous human immunoglobulin products cross the placenta increasingly during the third trimester. However, antibody-containing medicines have been used for years in pregnant women, and no harmful effects on the course of pregnancy, the fetus, or the newborn are expected.
- If you are breastfeeding while receiving Ig VENA, the antibodies contained in the product may pass into breast milk. Therefore, your baby may be protected from certain infections.
- Clinical experience with immunoglobulins suggests that no harmful effects on fertility are expected.
Driving and use of machinery
The ability to drive vehicles or operate machinery may be impaired by some adverse reactions
associated with Ig VENA. Patients experiencing adverse reactions during treatment should wait until these resolve before driving or operating machinery.
Ig VENA contains maltose and sodium
The product contains 100 mg of maltose per ml.
This medicinal product contains approximately 69 mg of sodium per litre. This should be taken into account for patients on a controlled-sodium diet.
3. How to use Ig VENA
Ig VENA can only be used in hospitals or clinics and nursing homes by medical professionals or other healthcare providers.
The dose and treatment regimen depend on the indication; your doctor will determine the appropriate dose and treatment schedule for you.
At the beginning of the infusion, you will receive Ig VENA at a low infusion rate. If you tolerate it well, your doctor may gradually increase the infusion rate.
Use in children and adolescents
The dosage in children and adolescents (0–18 years) is not different from that in adults, as the dosage for each indication is based on body weight and adjusted according to the patient's clinical response.
If you use more Ig VENA than you should
If you are administered more Ig VENA than intended, fluid overload may occur and the blood may become too thick (hyperviscous); this is particularly observed in at-risk patients, especially elderly patients or those with impaired cardiac or renal function.
If you have any doubts about the use of this medicine, consult your doctor or nurse.
4. Possible side effects
Like all medicines, this medicine can cause side effects, although not everybody gets them.
The following side effects may generally occur after treatment with immunoglobulins:
- chills, headache, dizziness, fever, vomiting, nausea, allergic reactions, arthralgia (joint pain), drop in blood pressure, and moderate lower back pain have been reported occasionally;
- isolated cases of temporary reduction in red blood cells (reversible haemolytic anaemia/haemolysis);
- a sudden drop in blood pressure has been reported rarely and, in some isolated cases, hypersensitivity reactions (anaphylactic shock) may occur, even when the patient has not shown reactions to previous administrations;
- rare cases of transient skin reactions have been observed;
- very rarely, thromboembolic reactions (blood clot formation) have been observed, which may lead to myocardial infarction, stroke, blockage of the pulmonary arteries (pulmonary embolism), and deep vein thrombosis;
- cases of transient non-infectious meningitis (reversible aseptic meningitis);
- increased blood creatinine levels and/or cases of sudden kidney failure have been reported;
- cases of transfusion-related acute lung injury (TRALI).
The side effects reported during administration of Ig VENA in clinical studies and those reported after the medicine has been marketed are listed below in order of decreasing frequency.
Common (may affect up to 1 in 10 people):
- Back pain
- Nausea
- Generalised weakness, fatigue, fever
- Muscle pain
- Headache, drowsiness
Frequency not known (cannot be estimated from the available data):
- Non-infectious meningitis
- Destruction and consequent deficiency of red blood cells
- Allergic reactions and life-threatening allergic shock
- Confusional state
- Stroke, dizziness, involuntary tremor, numbness and tingling of the skin or a limb
- Heart attack, bluish or purplish skin discoloration, rapid heartbeat, slow heartbeat, irregular heartbeat
- Blood clots in large veins and blood vessels, low blood pressure, high blood pressure, pallor
- Blood clots in a major artery of the lungs, abnormal fluid volume in the lungs, difficulty breathing with shortness of breath and cough
- Vomiting, diarrhoea, abdominal pain
- Rapid swelling of the skin, hives, redness and inflammation of the skin, rash, itching, eczema, excessive sweating
- Muscle and joint pain, back pain, neck pain, musculoskeletal stiffness
- Sudden kidney failure
- Vein inflammation at the injection site, chills, chest pain or discomfort, facial swelling, general feeling of malaise
- Increased blood creatinine levels
Additional side effects in children and adolescents
The frequency, type, and severity of adverse reactions in children are expected to be the same as in adults.
A slight and transient glucosuria (presence of glucose in urine) without clinical significance has been observed in children after administration of Ig VENA.
For information on viral safety, see section 2 "Before using Ig VENA".
Reporting of side effects
If you experience any side effect, including those not listed in this leaflet, talk to your doctor or nurse. You can also report side effects directly via the national reporting system at the following address:
https://www.aifa.gov.it/content/segnalazioni-reazioni-avverse.
By reporting side effects, you can help provide more information on the safety of this medicine.
5. How to store Ig VENA
Keep this medicine out of the sight and reach of children.
Do not use this medicine after the expiry date stated on the label and outer packaging after “Exp.”. The expiry date refers to the last day of the month.
Store in a refrigerator (2 °C - 8 °C).
Before use and within the expiry date, the product may be stored at room temperature, not exceeding 25°C, for up to 6 consecutive months. After this period, the product must be disposed of. In any case, the product must not be returned to the refrigerator if it has been stored at room temperature.
Record the date of the start of storage at room temperature on the outer carton.
Once the infusion container has been opened, the contents must be used immediately.
Keep the vial in the outer packaging.
Do not freeze.
Do not use this medicine if you notice that the solution is cloudy or contains deposits or shows any change in colour.
Do not dispose of medicines via wastewater or household waste. Ask your pharmacist how to dispose of medicines no longer required. This will help protect the environment.
6. Package contents and other information
What Ig VENA contains
The active substance of Ig VENA is normal human immunoglobulin.
One ml of solution contains 50 mg of normal human immunoglobulin.
The solution contains human proteins at a concentration of 50 g/l, of which at least 95% consists of
immunoglobulin G (IgG).
The immunoglobulin G (IgG) subclasses have the following distribution:
IgG 62.1%
IgG 34.8%
IgG 2.5%
IgG 0.6%
Maximum IgA content is 50 micrograms/ml.
Prepared from plasma of human donors.
The other components are maltose and water for injections.
Description of the appearance of Ig VENA and contents of the pack
Ig VENA is an infusion solution contained in single vials of 50, 100 or 200 ml, with an extendable hanger (vial + extendable hanger). The solution is clear or slightly opalescent, colourless or pale yellow.
Packs:
Single packs:
1 vial containing 2.5 g/50 ml
1 vial containing 5 g/100 ml
1 vial containing 10 g/200 ml.
Multiple packs:
Multiple pack composed of 2 single packs each containing 1 vial of 10 g/200 ml
Multiple pack composed of 3 single packs each containing 1 vial of 10 g/200 ml.
Not all pack sizes may be marketed.
Marketing Authorization Holder and Manufacturer
Marketing Authorization Holder:
Kedrion S.p.A. - Loc. Ai Conti, 55051 Castelvecchio Pascoli, Barga (Lucca) - ITALY.
Manufacturer: Kedrion S.p.A., 55027 Bolognana, Gallicano (Lucca) - ITALY.
This medicinal product is authorised in the Member States of the European Economic Area under the following names:
| Austria | Ig Vena 50 g/l Infusion solution |
| Germany | Ig Vena 50 g/l Infusion solution |
| Greece | Ig VENA |
| Italy | Ig VENA |
| Poland | Ig VENA |
| Portugal | Ig Vena |
The following information is intended exclusively for physicians or healthcare professionals:
Instructions for Proper Use
- Prior to administration, bring the product to room or body temperature.
- Prior to administration, visually inspect the solution for particulate matter or discoloration. Do not use solutions that are cloudy or contain deposits.
- Normal human immunoglobulin must be administered intravenously at an initial rate of 0.46–0.92 mL/kg/h (10–20 drops per minute) for 20–30 minutes. In case of an adverse reaction, reduce the infusion rate or stop the infusion. If well tolerated, the infusion rate may be gradually increased up to a maximum of 1.85 mL/kg/h (40 drops per minute).
- In patients with PID who tolerate an infusion rate of 0.92 mL/kg/h, the infusion rate may be gradually increased to 2 mL/kg/h, then 4 mL/kg/h, and up to a maximum of 6 mL/kg/h, every 20–30 minutes, only if the patient continues to tolerate the infusion well.
- In general, dosage and infusion rate must be individually adjusted according to the patient's needs. Depending on body weight, dosage, and occurrence of adverse reactions, the patient may not reach the maximum infusion rate. In case of an adverse reaction, the infusion must be immediately stopped and restarted at the most appropriate rate for the patient.
Special Populations
In pediatric patients (0–18 years) and elderly patients (>64 years), the initial infusion rate should be 0.46–0.92 mL/kg/h (10–20 drops per minute) for 20–30 minutes. If well tolerated and based on the patient's clinical condition, the infusion rate may be gradually increased up to a maximum of 1.85 mL/kg/h (40 drops per minute).
Instructions for Using the Extendable Hanger Label
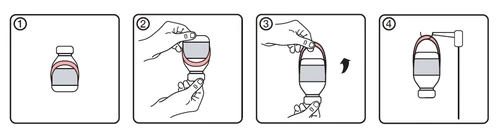
- Initial condition of the vial with the hanger label attached
- Invert the vial
- Rotate the lower edge of the hanger label upward to extend it
- Suspend the vial from the support
Special Precautions
Some serious adverse reactions to the product may be due to the rate of infusion.
Potential complications can often be avoided by ensuring:
- that patients are not sensitive to normal human immunoglobulin by starting administration slowly (at an infusion rate between 0.46 and 0.92 mL/kg/h);
- that patients are closely monitored for any symptoms during the infusion period. In particular, patients receiving normal human immunoglobulin for the first time, patients switching from one IVIg product to another, and patients who have had a long interval since their last infusion should be monitored during the first infusion and for the first hour afterward for potential signs of adverse reactions. All other patients should be observed for at least 20 minutes after administration. In all patients, IVIg administration requires:
- adequate hydration before starting IVIg infusion;
- monitoring of urine output;
- monitoring of serum creatinine levels;
- avoidance of concomitant use of loop diuretics.
In case of an adverse reaction, the infusion rate must be reduced or the infusion stopped. The required treatment depends on the nature and severity of the adverse effect. In case of shock, standard medical treatment for shock must be initiated.
Infusion Reactions
Some adverse reactions (e.g., headache, flushing, chills, myalgia, wheezing, tachycardia, back pain, nausea, and hypotension) may be related to the rate of infusion. The recommended infusion rate must be carefully followed. Patients must be closely monitored and carefully observed for any symptoms during the infusion period.
Adverse reactions may occur more frequently:
- in patients receiving normal human immunoglobulin for the first time, or, rarely, when switching to a different immunoglobulin product, or after a long interval since the last infusion;
- in patients with untreated infection or chronic inflammation.
Children and Adolescents
No specific measures or monitoring are required for the pediatric population.
No differences are expected in the pediatric population (0–18 years).
Thromboembolism
Clinical evidence shows an association between IVIg administration and thromboembolic events such as myocardial infarction, cerebrovascular accident (including stroke), pulmonary embolism, and deep vein thrombosis, presumed to be related to a relative increase in blood viscosity due to a high influx of immunoglobulin in at-risk patients.
Caution is advised when prescribing and administering IVIg to obese patients and to patients with pre-existing risk factors for thrombotic events (such as advanced age, hypertension, diabetes mellitus, history of vascular disease or thrombotic episodes, patients with inherited or acquired thrombophilic disorders, patients immobilized for prolonged periods, severely hypovolemic patients, or patients with conditions that increase blood viscosity).
In patients at risk for thromboembolic adverse reactions, IVIg products should be administered at the lowest feasible infusion rate and dose.
Acute Renal Failure
Cases of acute renal failure have been reported in patients receiving IVIg. In most cases, risk factors have been identified and include pre-existing renal insufficiency, diabetes mellitus, hypovolemia, overweight, concomitant administration of nephrotoxic drugs, or age over 65 years.
Renal function parameters should be evaluated before IVIg infusion, particularly in patients considered potentially at risk of developing acute renal failure, and again at appropriate intervals. In patients at risk of acute renal failure, IVIg products should be administered at the lowest feasible infusion rate and dose.
If renal function changes occur, discontinuation of IVIg treatment should be considered. Although cases of renal dysfunction and acute renal failure have been associated with the use of many IVIg products containing various excipients such as sucrose, glucose, and maltose, those containing sucrose as a stabilizer represent a very high proportion of the total number. In at-risk patients, the use of IVIg products not containing these excipients may be considered.
Aseptic Meningitis Syndrome (AMS)
Aseptic meningitis syndrome may occur in association with IVIg treatment.
Typically, the syndrome begins several hours to 2 days after IVIg administration. Cerebrospinal fluid (CSF) studies often show pleocytosis up to several thousand cells/mm³, predominantly granulocytes, and elevated protein levels up to several hundred mg/dL.
AMS may occur more frequently with high-dose IVIg (2 g/kg).
Patients presenting with such signs and symptoms should undergo a complete neurological evaluation, including CSF studies, to exclude other causes of meningitis.
Discontinuation of IVIg treatment has led to resolution of AMS within a few days, without sequelae.
Hemolytic Anemia
IVIg products may contain blood group-specific antibodies that can act as hemolysins and induce in vivo coating of red blood cells with immunoglobulins, causing a positive direct antiglobulin reaction (Coombs test) and, rarely, hemolysis.
Hemolytic anemia may develop following IVIg therapy due to increased sequestration of red blood cells. Patients receiving IVIg should be monitored for clinical signs and symptoms of hemolysis.
Neutropenia/Leukopenia
A transient decrease in neutrophil count and/or episodes of neutropenia, sometimes severe, have been reported after IVIg treatment. This typically occurs within a few hours or days after IVIg administration and resolves spontaneously within 7–14 days.
Transfusion-Related Acute Lung Injury (TRALI)
Cases of non-cardiogenic acute pulmonary edema (transfusion-related acute lung injury, TRALI) have been reported in patients receiving IVIg. TRALI is characterized by severe hypoxia, dyspnea, tachypnea, cyanosis, fever, and hypotension. Symptoms associated with TRALI typically appear during or within 6 hours of infusion, usually within 1–2 hours. Therefore, patients receiving IVIg must be monitored, and IVIg infusion must be immediately stopped if pulmonary adverse reactions occur. TRALI is a potentially life-threatening condition requiring immediate admission to intensive care.
This product contains 100 mg of maltose per mL as an excipient. Maltose interference with blood glucose testing may lead to overestimation of glucose values and, consequently, inappropriate insulin administration, which may cause life-threatening hypoglycemia and patient death. Additionally, true hypoglycemia may remain untreated if the hypoglycemic state is masked by falsely elevated glucose readings. For further details, see the section “Blood Glucose Testing”.
Dosage Recommendations
Replacement therapy should be initiated and monitored under the supervision of a physician experienced in the treatment of immunodeficiency.
Dosage
The dose and dosing regimen depend on the indication. The dose should be individualized for each patient based on clinical response. Weight-based dosing may require adjustment in underweight or overweight patients.
The following dosing regimens may be used as reference.
Replacement Therapy in Primary Immunodeficiency Syndromes
The dosing regimen should aim to achieve a trough IgG level (measured just before the next infusion) of at least 6 g/L or within the normal reference range for the patient's age group. From the start of therapy, it may take 3 to 6 months to reach steady-state (stable IgG levels).
The recommended initial dose is 0.4–0.8 g/kg as a single infusion, followed by at least 0.2 g/kg every 3–4 weeks. The monthly dose required to achieve a trough IgG level of 6 g/L is approximately 0.2–0.8 g/kg/month. The interval between doses may range from 3 to 4 weeks once steady-state is achieved. Trough IgG levels should be measured and evaluated together with the frequency of infections. The dose may need to be increased to achieve higher trough levels to reduce the frequency of bacterial infections.
Secondary Immunodeficiencies
The recommended dose is 0.2–0.4 g/kg every 3–4 weeks.
Trough IgG levels should be measured and evaluated together with infection frequency. The dose should be adjusted as needed to achieve optimal protection against infections; an increase may be necessary in patients with persistent infection; a dose reduction may be considered when the patient remains infection-free.
Primary Immune Thrombocytopenia
Two alternative treatment regimens are available:
- 0.8–1 g/kg on Day 1; this dose may be repeated once within 3 days;
- 0.4 g/kg/day for 2–5 days. Treatment may be repeated in case of relapse.
Guillain-Barré Syndrome
0.4 g/kg/day for 5 days (repetition of the regimen may be considered in case of relapse).
Kawasaki Disease
2.0 g/kg should be administered as a single dose. Patients must receive concomitant treatment with acetylsalicylic acid.
Chronic Inflammatory Demyelinating Polyradiculoneuropathy (CIDP)
Initial dose: 2 g/kg divided over 2–5 consecutive days.
Maintenance doses: 1 g/kg over 1–2 consecutive days every 3 weeks.
The treatment effect should be evaluated after each cycle; if no treatment effect is observed after 6 months, treatment should be discontinued.
If therapy is effective, long-term administration is at the physician’s discretion based on patient response and maintenance of response. Dose and intervals may need to be adjusted according to the individual disease course.
Multifocal Motor Neuropathy (MMN)
Initial dose: 2 g/kg administered over 2–5 consecutive days.
Maintenance doses: 1 g/kg every 2–4 weeks or 2 g/kg every 4–8 weeks.
The treatment effect should be evaluated after each cycle; if no treatment effect is observed after 6 months, treatment should be discontinued.
If therapy is effective, long-term administration is at the physician’s discretion based on patient response and maintenance of response. Dose and intervals may need to be adjusted according to the individual disease course.
The recommended doses are summarized in the following table:
| Indication | Dose | Frequency of injections |
| Replacement therapy | ||
| Primary immunodeficiency syndromes | Initial dose: 0.4–0.8 g/kg Maintenance dose: 0.2–0.8 g/kg | every 3–4 weeks |
| Secondary immunodeficiencies | 0.2–0.4 g/kg | every 3–4 weeks |
| Immunomodulation: | ||
| Primary immune thrombocytopenia | 0.8–1 g/kg Or 0.4 g/kg/day | Day 1, possibly repeated once within 3 days for 2–5 days |
| Guillain-Barré syndrome | 0.4 g/kg/day | for 5 days |
| Kawasaki disease | 2 g/kg | as a single dose, in combination with acetylsalicylic acid |
| Chronic inflammatory demyelinating polyradiculoneuropathy (CIDP) | Initial dose: 2 g/kg Maintenance dose: 1 g/kg | divided over 2–5 days every 3 weeks; maintenance in 1–2 days |
| Multifocal motor neuropathy (MMN) | Initial dose: 2 g/kg Maintenance dose: 1 g/kg Or 2 g/kg | for 2–5 consecutive days every 2–4 weeks Or every 4–8 weeks for 2–5 days |
Use in children and adolescents
The dosage in children and adolescents (0–18 years) is not different from that in adults, as the dosage for each indication is based on body weight and adjusted according to the clinical outcome of the respective conditions.
Hepatic impairment
There is no evidence requiring dose adjustment.
Renal impairment
No dose adjustment is necessary unless clinically justified.
Elderly
No dose adjustment is necessary unless clinically justified.
CIDP
Due to the rarity of the disease and, consequently, the small total number of patients, experience with the use of intravenous immunoglobulins in children with CIDP is limited; therefore, only literature data are available. However, published data consistently show that IVIg treatment is equally effective in children and adults, consistent with findings for other established IVIg indications.