Ozurdex 700 micrograms intravitreal implant in applicator
Spain
Instructions for Use
Patient Information Leaflet
Introduction
Package leaflet: Information for the patient
OZURDEX 700 micrograms intravitreal implant in applicator
dexamethasone
Read this entire leaflet carefully before you start using this medicine, as it contains important information for you.
- Keep this leaflet, as you may need to read it again.
- If you have any questions, consult your doctor.
- If you consider any of the side effects you experience to be severe, or if you notice any side effect not listed in this leaflet, inform your doctor. See section 4.
Contents of the leaflet
- What OZURDEX is and what it is used for
- What you need to know before using OZURDEX
- How to use OZURDEX
- Possible side effects
- How to store OZURDEX
- Contents of the pack and other information
1. What OZURDEX is and what it is used for
The active substance of OZURDEX is dexamethasone. Dexamethasone belongs to a group of medicines called corticosteroids.
OZURDEX is used to treat adult patients with:
-
Vision impairment due to diabetic macular edema (DME), if you have already undergone cataract surgery, or if you have not responded to other types of treatment or they are not suitable for you. Diabetic macular edema is swelling of the light-sensitive layer at the back of the eye called the macula. DME is a condition affecting some people with diabetes.
-
Vision loss in adults caused by blockage of the veins in the eye. This blockage leads to fluid buildup causing swelling in the area of the retina (a light-sensitive layer located at the back of the eye) known as the macula.
Inflammation of the macula may cause damage affecting your central vision, which is used for tasks such as reading. OZURDEX works by reducing this macular inflammation, helping to reduce or prevent further damage to the macula.
- Inflammation of the back of the eye. This inflammation causes decreased vision and/or the presence of floaters in the eye (black spots or fine lines moving across the field of vision). OZURDEX reduces this inflammation.
2. What you need to know before using OZURDEX
Do not use OZURDEX
- if you are allergic to dexamethasone or any of the other components of this medicine (listed in section 6);
- if you have any type of infection in or around the eye (bacterial, viral, or fungal);
- if you have glaucoma or elevated eye pressure that cannot be adequately controlled with your current medications;
- if the eye to be treated lacks a natural lens or if the posterior capsule of the lens is ruptured;
- if the eye to be treated has undergone cataract surgery and has an artificial lens implanted in the front compartment of the eye (anterior chamber intraocular lens), or if the lens is attached to the white part of the eye (sclera) or to the colored part of the eye (iris), and if the posterior capsule of the lens is ruptured.
Warnings and precautions
Before your OZURDEX injection, inform your doctor if:
- you have had cataract surgery, iris surgery (the colored part of the eye that controls the amount of light entering the eye), or surgery to remove the gel (called vitreous) inside the eye;
- you are taking any blood-thinning medication;
- you are taking any oral or eye-applied anti-inflammatory steroid or non-steroidal medication; or
- you have previously had a herpes simplex infection in your eye (a long-lasting corneal ulcer or an eye wound).
Occasionally, OZURDEX injection may cause infection, pain, or redness inside the eye, or even retinal detachment or tear. It is important to identify and treat these problems as early as possible. Immediately inform your doctor if, after the injection, you experience increased eye pain or discomfort, worsening red eyes, flashes of light, a sudden increase in floaters, partially blocked vision, reduced vision, or increased sensitivity to light.
In some patients, eye pressure may increase, possibly leading to glaucoma. You may not notice this, so your doctor will perform regular check-ups and, if necessary, provide treatment to reduce intraocular pressure.
In most patients who have not undergone cataract surgery, clouding of the lens (cataracts) may occur after repeated treatment with OZURDEX, which could reduce your vision and likely require surgery to remove the cataracts. Your doctor will help you decide the best time for surgery, but you should know that until you are ready for surgery, your vision may be as poor or worse than before you started receiving OZURDEX injections.
The implant may move from the back to the front of the eye in patients with a tear in the posterior lens capsule and/or those with an opening in the iris. This displacement may cause swelling of the transparent layer at the front of the eye and blurred vision. If this persists for a long time and is not treated, a tissue transplant may eventually be required.
The simultaneous injection of OZURDEX in both eyes has not been studied and is therefore not recommended. Your doctor should not inject OZURDEX in both eyes at the same time.
Children and adolescents
The use of OZURDEX has not been studied in children and adolescents, and therefore is not recommended.
Other medicines and OZURDEX
Tell your doctor if you are using or have recently used any other medicines, including those obtained without a prescription.
Pregnancy and breastfeeding
There is no experience regarding the use of OZURDEX in pregnant or breastfeeding women. OZURDEX should not be used during pregnancy or breastfeeding unless your doctor considers it absolutely necessary. If you are pregnant, breastfeeding, think you may be pregnant, or plan to become pregnant, consult your doctor before using OZURDEX treatment. Consult your doctor before using any medicine.
Driving and use of machines
After treatment with OZURDEX, your vision may be reduced for a short period of time. If this occurs, do not drive or operate tools or machinery until your vision improves.
3. How to use OZURDEX
All OZURDEX injections must be administered by a qualified eye specialist.
The recommended dose is one implant injected into the eye. If the effect of this injection wears off and your doctor recommends it, another implant may be injected into the eye.
Your doctor will instruct you to use an antibiotic eye drop daily for 3 days before and after each injection to help prevent the development of an eye infection. Follow these instructions carefully.
On the day of the injection, your doctor may use an antibiotic eye drop to help prevent infections. Before the injection, your doctor will clean your eye and eyelid. Your doctor will also administer a local anesthetic to reduce or prevent any pain caused by the injection. You may hear a "click" during the injection of OZURDEX, which is normal.
Detailed instructions for the administration of OZURDEX are provided in the medicine carton for your doctor.
If you have any further questions about the use of this medicine, ask your doctor.
4. Possible side effects
Like all medicines, this medicine can cause side effects, although not everyone will experience them.
The following side effects may occur with OZURDEX:
Very common (may affect more than 1 in 10 people):
- increased eye pressure
- clouding of the lens (cataracts), bleeding on the surface of the eye*
Common (may affect up to 1 in 10 people):
- elevated eye pressure
- clouding of the back part of the lens
- bleeding inside the eye*
- worsening of vision*
- difficulty seeing clearly
- detachment of the gel from the light-sensitive layer at the back of the eye (vitreous detachment)*
- sensation of spots in front of the eye (including floaters)*
- sensation of seeing through a fog*
- eyelid swelling
- eye pain*
- seeing flashes of light*
- swelling of the layer covering the white part of the eye*
- eye redness*
- headache
Uncommon (may affect up to 1 in 100 people):
- severe inflammation at the back of the eye (usually due to viral infection)
- severe infection or inflammation inside the eye*
- glaucoma (an eye disease in which high eye pressure is associated with damage to the optic nerve)
- detachment of the light-sensitive layer from the back of the eye* (retinal detachment)
- tear in the light-sensitive layer at the back of the eye (retinal tear)*
- decrease in eye pressure associated with leakage of gel (vitreous) from inside the eye*
- inflammation inside the front part of the eye*
- increased proteins and cells in the front part of the eye due to inflammation*
- abnormal sensation in the eye*
- eyelid itching
- redness of the white part of the eye*
- migration of the OZURDEX implant from the back to the front part of the eye, causing blurred vision or worsening of vision, which may or may not lead to swelling of the transparent layer of the eye (cornea)*
- accidental incorrect placement of the OZURDEX implant*
- migraine
*These side effects may be caused by the injection procedure and not by the OZURDEX implant. The more injections you receive, the greater the likelihood that these side effects may occur.
Reporting of side effects
If you experience any type of side effect, consult your doctor, even if it is a possible side effect not listed in this leaflet. You may also report them directly through the national reporting system detailed in Appendix V. By reporting side effects, you can help provide more information on the safety of this medicine.
5. Storage of OZURDEX
Keep this medicine out of the sight and reach of children.
Do not use OZURDEX after the expiry date stated on the carton and on the bag, after “EXP”. The expiry date refers to the last day of the month indicated.
This medicine does not require any special storage conditions.
Medicines must not be disposed of via wastewater or household waste. Ask your pharmacist how to dispose of medicines and packaging you no longer need. This will help protect the environment.
6. Contents of the pack and other information
Composition of OZURDEX
-
The active substance is dexamethasone.
-
Each implant contains 700 micrograms of dexamethasone.
-
The other components are: 50:50 poly D,L-lactide-co-glycolide in ester form and
50:50 poly D,L-lactide-co-glycolide in acid form and hypromellose.
Appearance of OZURDEX and contents of the pack
OZURDEX is a rod-shaped implant contained within the needle of an applicator. A sealed laminated pouch, inside a carton, contains the applicator and a desiccant packet. The pouch is packaged in a plastic tray with a lid, which is then placed into a cardboard outer box. One carton contains one applicator with one implant, intended for single use and to be discarded after use.
Marketing Authorization Holder
AbbVie Deutschland GmbH & Co. KG
Knollstrasse
67061 Ludwigshafen
Germany
Manufacturer responsible for production
Allergan Pharmaceuticals Ireland
Castlebar Road
Westport
Co. Mayo
Ireland
For further information about this medicinal product, please contact the local representative of the Marketing Authorization Holder:
Belgium/Belgium/Belgium AbbVie SA Tel/Tel: +32 10 477811 | Lithuania AbbVie UAB Tel: + 370 5 205 3023 |
| Luxembourg/Luxembourg AbbVie SA Belgium/Belgium Tel/Tel: +32 10 477811 |
Czech Republic AbbVie s.r.o. Tel.: +420 233 098 111 | Hungary AbbVie Kft. Tel:+36 1 455 8600 |
Denmark AbbVie A/S Tlf.: +45 72 30 20 28 | Malta Vivian Corporation Ltd. Tel: +356 27780331 |
Germany AbbVie Deutschland GmbH & Co. KG Tel.: 00800 222843 33 (toll-free) Tel.: +49 (0) 611 / 1720-0 | Netherlands AbbVie B.V. Tel: +31 (0)88 322 2843 |
Estonia AbbVie OÜ Tel. +372 6231011 | Norway AbbVie AS Tlf: +47 67 81 80 00 |
Greece AbbVie PHARMACEUTICAL S.A. Tel: +30 214 4165 555 | Austria AbbVie GmbH? Tel: +43 1 20589-0 |
Spain AbbVie Spain, S.L.U. Tel: +34 913840910 | Poland AbbVie Sp. z o.o. Tel.: +48 22 372 78 00 |
France AbbVie Tel: +33 (0) 1 45 60 13 00 | Portugal AbbVie, Lda. Tel.: +351 (0)21 1908400 |
Croatia AbbVie d.o.o. Tel: + 385 (0)1 5625 501 | Romania AbbVie S.R.L. Tel: +40 21 529 30 35 |
Ireland AbbVie Limited Tel: +353 (0)1 4287900 | Slovenia AbbVie Biofarmacevtska družba d.o.o. Tel: +386 (1)32 08 060 |
Iceland Vistor hf. Sími: +354 535 7000 | Slovakia AbbVie s.r.o. Tel: +421 2 5050 0777 |
Italy AbbVie S.r.l. Tel: +39 06 928921 | Finland AbbVie Oy Puh/Tel: +358 (0)10 2411 200 |
Cyprus Lifepharma (Z.A.M.) Ltd Tel: +357 22 34 74 40 | Sweden AbbVie AB Tel: +46 (0)8 684 44?600 |
Latvia AbbVie SIA Tel: +371 67605000 |
Date of the most recent review of this leaflet
Detailed information on this medicine is available on the European Medicines Agency website: http://www.ema.europa.eu/.
To request a copy of this leaflet in large print, please contact the local representative of the marketing authorization holder.
[To be provided on the carton]
This information is intended for healthcare professionals only and includes the numbered sections of the SmPC, which provide practical information for the use of the medicine. Please also refer to the SmPC for complete information on the medicine.
INFORMATION FOR HEALTHCARE PROFESSIONALS
1. NAME OF THE MEDICINAL PRODUCT
OZURDEX 700 micrograms intravitreal implant in applicator
4. CLINICAL PARTICULARS
4.1 Therapeutic indications
OZURDEX is indicated in adults for the treatment of:
-
visual impairment due to diabetic macular edema (DME) in pseudophakic patients, or patients in whom an inadequate response is expected, or in whom non-corticosteroid therapy is not appropriate
-
macular edema following branch retinal vein occlusion (BRVO) or central retinal vein occlusion (CRVO) (see section 5.1 of the SmPC)
-
inflammation presenting as non-infectious posterior segment uveitis of the eye
4.2 Posology and method of administration
OZURDEX must be administered by an ophthalmologist experienced in intravitreal injections.
Posology
The recommended dose is one OZURDEX implant administered intravitreally into the affected eye. Simultaneous administration in both eyes is not recommended (see section 4.4 of the SmPC).
Patients should be monitored after injection so that early treatment can be initiated if infection or increased intraocular pressure occurs (see section 4.4 of the SmPC).
Special populations
Elderly patients (≥65 years)
No dose adjustment is required for elderly patients.
Method of administration
OZURDEX is a single-use intravitreal implant in an applicator for intravitreal administration only.
Each applicator must be used for the treatment of one eye only.
The intravitreal injection must be performed under controlled aseptic conditions, including the use of sterile gloves, sterile drapes, and a sterile eyelid speculum (or equivalent).
Patients should be instructed to self-administer a broad-spectrum antimicrobial eye drop daily for 3 days before and after each injection. Prior to injection, the periocular skin, eyelid, and ocular surface should be disinfected (e.g., using drops of 5% povidone-iodine solution on the conjunctiva as used in the clinical trials for Ozurdex marketing authorisation), and appropriate local anaesthesia should be administered. Remove the laminated pouch from the carton and inspect it for damage (see section 6.6 of the SmPC). Then, in a sterile field, open the laminated pouch and gently place the applicator on a sterile tray. Once the pouch is opened, the applicator should be used immediately.
Perform a careful visual inspection of the applicator, ensuring that the activation button is not depressed and that the safety tab is in place. Carefully remove the plastic safety cap, avoiding contact with the needle tip. Inspect the needle tip for any damage before use; the implant retention plug may be visible at the bevel and must not be removed. Hold the applicator in one hand and remove the safety tab from the applicator. Do not twist or bend the tab.
With the needle bevel facing upwards and away from the sclera, insert the needle approximately 1 mm into the sclera. Then direct it towards the centre of the eye into the vitreous cavity until the sleeve touches the conjunctiva. Slowly press the activation button until an audible and/or palpable click is felt. Before removing the applicator from the eye, ensure that the activation button is fully depressed and locked flush with the applicator surface. Withdraw the needle in the same direction as insertion into the vitreous cavity.
For instructions on administration of the intravitreal implant, see section 6.6.
Immediately after OZURDEX injection, perform indirect ophthalmoscopy in the quadrant where the injection was administered to confirm correct implantation. Visualization is possible in the vast majority of cases. In cases where the implant cannot be observed, use a sterile cotton swab and gently press over the injection site to displace the implant until it becomes visible.
After intravitreal injection, patients should continue treatment with a broad-spectrum antimicrobial eye drop.
4.3 Contraindications
- Hypersensitivity to the active substance or to any of the excipients listed in section 6.1 of the SmPC.
- Active ocular or periocular infection or suspicion thereof, including most viral diseases of the cornea and conjunctiva, such as active epithelial herpes simplex (dendritic keratitis), vaccinia, varicella, bacterial infections, and fungal diseases.
- Advanced glaucoma that cannot be adequately controlled with medication alone.
- Aphakic eyes with damaged posterior lens capsule.
- Eyes with anterior chamber intraocular lenses, iris-fixated or transscleral intraocular lenses, and damaged posterior lens capsule.
4.4 Special warnings and precautions for use
Intravitreal injections, including those with OZURDEX, may be associated with endophthalmitis, intraocular inflammation, increased intraocular pressure, and retinal detachment. Appropriate aseptic injection techniques must always be used. Patients should also be monitored after injection so that early treatment can be initiated if any signs of infection or increased intraocular pressure occur. This monitoring may include assessment of optic nerve head perfusion immediately after injection, tonometry within 30 minutes after injection, and biomicroscopy between two and seven days after injection.
Patients should be advised to report immediately any symptoms that may indicate endophthalmitis or any of the aforementioned disorders, e.g., eye pain, blurred vision, etc. (see section 4.8 of the SmPC).
Patients with posterior capsule tear, such as those with posterior lens (e.g., following cataract surgery) and/or those with an opening from the iris into the vitreous cavity (e.g., due to iridectomy), with or without history of vitrectomy, are at risk of implant displacement into the anterior chamber. Displacement of the implant into the anterior chamber may cause corneal oedema. Persistent severe corneal oedema may progress to the point where corneal transplantation is required. In addition to patients with contraindications (see section 4.3 of the SmPC), in whom OZURDEX must not be used, OZURDEX should be used with caution and only after careful assessment of risks and benefits. Such patients should be closely monitored so that implant displacement can be diagnosed and treated promptly.
The use of corticosteroids, including OZURDEX, may induce cataracts (including posterior subcapsular cataracts), increased intraocular pressure (IOP), steroid-induced glaucoma, and secondary ocular infections.
In 3-year clinical studies of DME, 59% of phakic study eye patients treated with OZURDEX underwent cataract surgery in the study eye (see section 4.8 of the SmPC).
After the first injection, the incidence of cataracts appears higher in patients with non-infectious posterior segment uveitis than in patients with BRVO/CRVO. In BRVO/CRVO clinical trials, cataracts were reported more frequently in phakic patients who received a second injection (see section 4.8 of the SmPC). Of these 368 cases, cataract surgery was required in only one during the first treatment course, and in 3 of 302 cases during the second treatment course. In the uveitis study, one of 62 phakic patients underwent cataract surgery after a single injection.
The prevalence of conjunctival haemorrhage in patients with non-infectious posterior segment uveitis appears higher compared to BRVO/CRVO and DME, which may be attributed to the intravitreal injection procedure or concomitant use of topical and/or systemic corticosteroids or non-steroidal anti-inflammatory drugs. No treatment is required, as it resolves spontaneously.
As expected with ocular corticosteroid therapy and intravitreal injections, increases in intraocular pressure (IOP) may occur. Elevated IOP can usually be managed with IOP-lowering medication (see section 4.8 of the SmPC). Among patients who experienced an IOP increase of ≥10 mm Hg from baseline, most showed this increase between 45 and 60 days after injection. Therefore, regular monitoring of IOP is required regardless of baseline IOP, and any post-injection increase should be appropriately managed. Patients under 45 years of age with macular oedema following retinal vein occlusion or posterior segment inflammation presenting as non-infectious uveitis are more likely to experience an IOP increase.
Corticosteroids should be used with caution in patients with a history of ocular viral infection (e.g., herpes simplex) and must not be used in cases of active ocular herpes simplex.
The safety and efficacy of OZURDEX administered simultaneously in both eyes have not been studied and is therefore not recommended.
The use of OZURDEX in patients with macular oedema following retinal vein occlusion with significant retinal ischaemia has not been studied and is therefore not recommended.
A limited number of subjects with type 1 diabetes were included in phase 3 studies, and the response to OZURDEX in these subjects was not significantly different from that observed in subjects with type 2 diabetes.
In retinal vein occlusion (RVO), anticoagulant therapy was used in 2% of patients receiving OZURDEX, with no haemorrhagic adverse events reported. In DME, 8% of patients used anticoagulant therapy. In patients using anticoagulant therapy, the frequency of haemorrhagic adverse events was similar in the OZURDEX group and the sham injection group (29% vs. 32%). Among patients not using anticoagulant therapy, 27% of those treated with OZURDEX reported haemorrhagic adverse events, compared to 20% in the sham injection group. Vitreous haemorrhage was reported in a higher proportion of OZURDEX-treated patients receiving anticoagulant therapy (11%) compared to those not receiving anticoagulant therapy (6%).
Antiplatelet agents such as clopidogrel were used at some point during the clinical studies in up to 56% of patients. In patients with concomitant use of antiplatelet agents, haemorrhagic adverse events were reported in a slightly higher percentage of patients receiving OZURDEX (up to 29%) compared to the sham injection group (up to 23%), regardless of indication or number of treatments. The most frequently reported haemorrhagic adverse event was conjunctival haemorrhage (up to 24%).
OZURDEX should be used with caution in patients taking anticoagulant or antiplatelet medications.
Visual disturbances
Visual disturbances may occur with systemic and topical use of corticosteroids. If a patient experiences symptoms such as blurred vision or other visual disturbances, possible causes should be evaluated, which may include cataracts, glaucoma, or rare conditions such as central serous chorioretinopathy (CSCR), which have been reported following systemic and topical corticosteroid use.
4.5 Interaction with other medicinal products and other forms of interaction
No interaction studies have been conducted.
Systemic absorption is minimal and interactions are not expected.
4.6 Fertility, pregnancy and lactation
Pregnancy
Animal studies have shown teratogenic effects following topical ophthalmic administration (see section 5.3 of the SmPC). There are insufficient data on the use of intravitreal dexamethasone in pregnant women. Long-term systemic treatment with glucocorticoids during pregnancy increases the risk of intrauterine growth retardation and neonatal adrenal insufficiency. Therefore, although systemic exposure to dexamethasone following local intraocular administration is expected to be very low, OZURDEX is not recommended during pregnancy unless the potential benefit justifies the risk to the foetus.
Lactation
Dexamethasone is excreted in breast milk. No effect on the infant is expected due to the route of administration and resulting systemic levels. However, the use of OZURDEX during lactation is not recommended unless clearly necessary.
Fertility
There are no data available on fertility.
4.7 Effects on ability to drive and use machines
The influence of OZURDEX on the ability to drive and use machines may be moderate. Patients may experience temporarily reduced vision after administration of OZURDEX via intravitreal injection (see section 4.8 of the SmPC). Patients should not drive or operate machinery until this effect has resolved.
- Adverse reactions
Summary of safety profile
The most frequently reported adverse events following treatment with OZURDEX are those commonly observed with ophthalmic corticosteroid therapy or intravitreal injections (elevated IOP, cataract formation, and conjunctival or vitreous haemorrhage, respectively).
Other less frequent but more serious adverse reactions include endophthalmitis, necrotizing retinitis, retinal detachment, and retinal tear.
No systemic adverse drug reactions were identified with OZURDEX use, except for headache and migraine.
Table of adverse reactions
Adverse reactions considered related to OZURDEX treatment in phase III clinical trials (DME, BRVO/CRVO, and uveitis), as well as spontaneous reports, are listed below by MedDRA system organ class using the following convention:
Very common (≥1/10); common (≥1/100 to <1/10); uncommon (≥1/1,000 to <1/100); rare (≥1/10,000 to <1/1,000); very rare (<1/10,000). Adverse reactions are listed in decreasing order of severity within each frequency category.
Table 1. Adverse reactions
Organ system classification | Frequency | Adverse reaction |
Nervous system disorders | Common | Headache |
Uncommon | Migraine | |
Eye disorders | Very common | Increased intraocular pressure**, cataracts**, conjunctival haemorrhage* |
Common | Ocular hypertension, subcapsular cataracts, vitreous haemorrhage**, reduced visual acuity*, vision deterioration/impairment, vitreous detachment*, floaters*, vitreous opacities*, blepharitis, eye pain*, photopsia*, conjunctival oedema*, conjunctival hyperaemia* | |
Uncommon | Necrotizing retinitis, endophthalmitis*, glaucoma, retinal detachment*, retinal tear*, ocular hypotony*, anterior chamber inflammation*, flare cells/flare in anterior chamber*, abnormal sensation in eye*, eyelid pruritus, scleral hyperaemia* | |
General disorders and administration site conditions | Uncommon | Device displacement* (implant migration) with or without corneal oedema (see also section 4.4), complication during device insertion leading to ocular tissue injury* (incorrect placement) |
*Indicates adverse reactions considered related to the intravitreal injection procedure (the frequency of these adverse reactions is proportional to the number of administered treatments).
** In a 24-month observational clinical practice study on the treatment of macular edema following RVO and non-infectious posterior segment uveitis, the following adverse reactions were reported more frequently in patients treated with >2 injections compared to those treated with ≤2 injections: cataract formation (24.7% vs. 17.7%), progression of cataracts (32.0% vs. 13.1%), vitreous hemorrhage (6.0% vs. 2.0%), and increased IOP (24.0% vs. 16.6%).
Description of selected adverse reactions
Diabetic macular edema
The clinical safety of OZURDEX in patients with diabetic macular edema was evaluated in two phase III, randomized, double-blind, sham-injection controlled studies. In both studies, a total of 347 patients were randomized to receive OZURDEX and 350 received sham injection.
The adverse reactions reported most frequently in the study eye throughout the study period in patients who received OZURDEX were cataracts and increased IOP (see below).
In the 3-year DME clinical studies, 87% of phakic study eye patients treated with OZURDEX showed some degree of lens opacification/early cataracts at baseline. The incidence of all observed types of cataracts (i.e., cortical cataracts, diabetic cataracts, nuclear cataracts, subcapsular cataracts, lenticular cataracts, cataracts) was 68% in OZURDEX-treated patients with a phakic study eye over the 3-year study period. 59% of patients with a phakic study eye required cataract surgery before the final visit at 3 years, with most surgeries occurring in the 2nd and 3rd years.
At baseline, both treatment groups had the same mean IOP (15.3 mmHg) in the study eye. The mean increase from baseline IOP did not exceed 3.2 mmHg at any visit in the OZURDEX group, with the highest IOP value observed at the 1.5-month post-injection visit and returning to approximately baseline levels 6 months after each injection. The frequency and magnitude of IOP increases following OZURDEX treatment did not increase with repeated OZURDEX injections.
28% of OZURDEX-treated patients experienced an IOP increase ≥10 mmHg from baseline at one or more visits during the study. At baseline, 3% of patients required medication to reduce IOP. Overall, 42% of patients required medication to reduce IOP in the study eye at some point during the 3-year study period, with most patients requiring more than one medication. Maximum usage (33%) occurred during the first 12 months and remained similar each year.
Among OZURDEX-treated patients, a total of 4 (1%) underwent surgical interventions in the study eye to treat elevated IOP. One OZURDEX-treated patient required incisional surgery (trabeculectomy) to treat steroid-induced IOP elevation; 1 patient underwent trabeculectomy due to fibrin in the anterior chamber obstructing aqueous humor outflow, which caused elevated IOP; 1 patient underwent iridotomy for narrow-angle glaucoma; and 1 patient underwent iridectomy due to cataract surgery. No patient required implant removal by vitrectomy to control IOP.
RVO/BRVO
The clinical safety of OZURDEX in patients with macular edema following central retinal vein occlusion or branch retinal vein occlusion was evaluated in two phase III, randomized, double-blind, sham-injection controlled trials. A total of 427 patients were randomized to receive OZURDEX and 426 to receive sham injection in the two phase III trials. A total of 401 patients (94%) randomized and treated with OZURDEX completed the initial treatment period (up to Day 180).
47.3% of patients experienced at least one adverse reaction. The most frequently observed adverse reactions in patients who received OZURDEX were increased intraocular pressure (24%) and conjunctival hemorrhage (14.7%).
The adverse reaction profile in patients with CRVO was similar to that observed in patients with BRVO, although the overall incidence of adverse reactions was higher in the BRVO subgroup.
Increased intraocular pressure (IOP) with OZURDEX peaked on Day 60 and returned to baseline levels around Day 180. IOP increases either did not require treatment or responded to temporary use of topical IOP-lowering medications. During the initial treatment period, 0.7% (3/421) of OZURDEX-treated patients required laser or surgical procedures to manage increased IOP in the study eye, compared to 0.2% (1/423) of patients in the sham-injection control group.
The adverse reaction profile in 341 patients evaluated after a second OZURDEX injection was similar to that after the first injection. 54% of patients experienced at least one adverse reaction. The incidence of increased IOP (24.9%) was similar to that observed after the first injection and also returned to baseline levels by Day 180 of the open-label phase. The overall incidence of cataracts was higher after 1 year compared to the initial 6 months.
Uveitis
The clinical safety of OZURDEX in patients with posterior segment inflammation presenting as non-infectious uveitis has been evaluated in a single, multicenter, masked, randomized trial.
A total of 77 patients were randomized to receive OZURDEX and 76 to receive sham intervention. A total of 73 patients (95%) randomized and treated with OZURDEX completed the 26-week trial.
The adverse reactions reported most frequently in the study eye in patients who received OZURDEX were conjunctival hemorrhage (30.3%), increased intraocular pressure (25.0%), and cataracts (11.8%).
Reporting suspected adverse reactions
It is important to report suspected adverse reactions to the medicinal product after authorization. This enables continued monitoring of the benefit-risk balance of the medicinal product. Healthcare professionals are encouraged to report suspected adverse reactions via the national reporting system included in Appendix V.
4.9 Overdose
In the event of overdose, intraocular pressure should be monitored and treated if deemed necessary by the physician.
5.3 Preclinical safety data
Reactions were observed only in preclinical studies at exposures considered higher than the maximum human exposure, indicating limited relevance for clinical use.
No data are available regarding mutagenicity, carcinogenic potential, or reproductive and developmental toxicity of OZURDEX. Dexamethasone has been shown to be teratogenic in mice and rabbits following topical ophthalmic administration.
Exposure to dexamethasone in the healthy or untreated eye via contralateral diffusion has been observed in rabbits following implant administration in the posterior segment of the eye.
6. PHARMACEUTICAL DATA
6.4 Special precautions for storage
This medicinal product does not require special storage conditions.
6.6 Special precautions for disposal and other handling
OZURDEX is for single use only.
Each applicator must be used only for the treatment of one single eye.
If the seal of the laminated pouch containing the applicator is damaged, the applicator must not be used. Once the laminated pouch is opened, the applicator should be used immediately.
Administration of OZURDEX
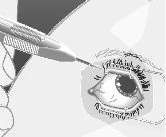
1) | Hold the long axis of the applicator parallel to the limbus. |
|
2) | Position the applicator obliquely against the sclera with the needle bevel facing upward and away from the sclera. Advance the needle tip approximately 1 mm into the sclera, keeping it parallel to the limbus. |
|
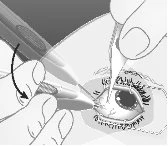
3) | Redirect the needle toward the center of the eye into the vitreous cavity. This will create an angled scleral track. |
|
4) | Slowly press the activation button until an audible and/or palpable click is detected. Before removing the applicator from the eye, ensure that the activation button is fully depressed and locked flush with the applicator surface. |
|
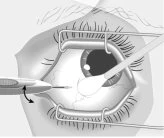
5) | Remove the applicator in the same direction used to enter the vitreous. |
|
6) | Dispose of the applicator safely immediately after treatment. |


Disposal of unused medicine and all materials that have been in contact with it must be carried out in accordance with local regulations.
Date of the most recent revision of this leaflet
This page has been machine-translated and may contain inaccuracies. The original data is available in the manufacturing country's language.
Last data check: May 18, 2026 · Data source: CIMA — AEMPS