Mirena 0.02 mg per 24 hours intrauterine system
Spain
Table of Contents
Patient Information Leaflet
Introduction
Patient Information Leaflet
Mirena 0.02 mg per 24 hours intrauterine system
Levonorgestrel
Read the entire leaflet carefully before you start using this medicine, as it contains important information for you.
|
Package leaflet contents
- What Mirena is and what it is used for
- What you need to know before using Mirena
- How to use Mirena
- Possible side effects
- Storage of Mirena
- Contents of the pack and other information
1. What Mirena is and what it is used for
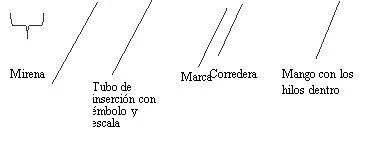
Mirena is a T-shaped intrauterine drug delivery system (IUS) which, after insertion, releases the hormone levonorgestrel into the uterus. The T-shaped design is intended to conform to the shape of the uterus. The vertical arm of the white T-shaped body contains a drug reservoir holding levonorgestrel. At the lower end of the vertical arm there is a loop to which two brown removal threads are attached.
Mirena is used for the prevention of pregnancy (contraception) and for the treatment of excessive menstrual bleeding (idiopathic menorrhagia).
Children and adolescents
Mirena is not indicated for use before the first menstruation (menarche).
2. What you need to know before starting to use Mirena
General information Before you start using Mirena, your doctor will ask you some questions about your personal and family medical history. This leaflet describes several situations in which Mirena should be removed, or in which the effectiveness of Mirena may decrease. In such situations, you should avoid sexual intercourse or use additional non-hormonal contraceptive precautions, for example, a condom or another barrier method. Do not use the rhythm method or the temperature method. These methods may not be reliable because Mirena alters the monthly changes in body temperature and cervical mucus. Like other hormonal contraceptives, Mirena does not protect against HIV infection (AIDS) or any other sexually transmitted disease. |
Do not use Mirena if you have any of the following conditions:
- Pregnancy or suspected pregnancy
- Hormone-sensitive tumors that may grow, e.g., breast cancer
- Current or recurrent pelvic inflammatory disease (infection of the female reproductive organs)
- Cervical infection (cervix or neck of the uterus)
- Lower genital tract infection
- Uterine infection following childbirth
- Uterine infection following abortion within the last 3 months
- Conditions associated with increased susceptibility to infections
- Abnormalities of the cervical cells
- Uterine or cervical cancer, or suspected cancer
- Unexplained abnormal uterine bleeding
- Abnormalities of the cervix or uterus, including fibroids if they distort the uterine cavity
- Acute liver disease or liver tumor
- Hypersensitivity to levonorgestrel or to any of the other components of this medicine (listed in section 6)
Warnings and precautions
Consult your doctor before starting to use Mirena.
If you have any of the conditions listed below, or if any of them develop for the first time while using Mirena, consult a specialist to determine whether you should continue using Mirena or have the system removed:
- Migraine, asymmetric vision loss, or other symptoms that may indicate transient cerebral ischemia (temporary blockage of blood flow to the brain)
- Exceptionally severe headache
- Jaundice (yellowing of the skin, whites of the eyes, and/or nails)
- Marked increase in blood pressure
- Serious arterial diseases such as stroke or heart attack
- Acute blood clots in the veins
Mirena should be used with caution in women with congenital heart disease or valvular heart disease at risk of infectious inflammation of the heart muscle.
In diabetic women using Mirena, blood glucose levels should be monitored.
Irregular bleeding may mask symptoms and signs of endometrial polyps or cancer; in such cases, diagnostic testing should be considered.
Medical examination/consultation
The examination before insertion may include a cervical cytology test (Pap smear), breast examination, and other tests, for example for infections, including sexually transmitted infections, and a pregnancy test if necessary. A gynecological examination should be performed to determine the position and size of the uterus.
Mirena must not be used as emergency contraception (postcoital contraception).
Infections
The insertion tube helps prevent contamination of Mirena by microorganisms during insertion, and the Mirena inserter has been designed to minimize the risk of infections. Nevertheless, in users of copper intrauterine devices (IUDs), there is an increased risk of pelvic infection immediately after insertion and during the following month. Pelvic infections in users of intrauterine systems (IUS) are often related to sexually transmitted infections. The risk of infection increases if the woman or her partner has multiple sexual partners simultaneously. Pelvic infections must be treated promptly. A pelvic infection may impair fertility and increase the risk of future ectopic pregnancy (pregnancy outside the uterus).
In extremely rare cases, a severe infection or septicemia (a very serious infection that may be fatal) may occur shortly after insertion.
Mirena must be removed if recurrent pelvic infections, endometrial infections, or a severe acute infection that does not respond to treatment within a few days occur.
Seek immediate medical advice if you experience persistent lower abdominal pain, fever, pain during sexual intercourse, or abnormal bleeding.
Expulsion
Uterine muscle contractions during menstruation may sometimes push the IUS out of place or expel it completely. This is more likely to occur if you are overweight at the time of IUS insertion or have a history of heavy menstrual bleeding. If the IUS moves out of place, it may not work properly, and the risk of pregnancy increases. If the IUS is expelled, you are no longer protected against pregnancy.
Possible signs of expulsion include pain and abnormal bleeding, but Mirena may also be expelled without your awareness. Because Mirena reduces menstrual flow, an increase in bleeding may indicate expulsion.
It is recommended that you check the threads with your finger, for example while showering. See also section 3 “How to use Mirena – How can I tell if Mirena is correctly positioned?”. If you notice signs suggesting expulsion or are unable to feel the threads, you should use an additional contraceptive method (such as condoms) and consult your healthcare provider.
Perforation
Perforation or penetration of the uterine wall may occur more frequently during insertion, although it may not be detected until later. A Mirena device displaced outside the uterine cavity will not prevent pregnancy and must be removed as soon as possible. Surgical intervention may be required to remove Mirena. The risk of perforation is increased in women who are breastfeeding, in women who have given birth within 36 weeks prior to insertion, and may be increased in women with a fixed and retroverted uterus (fixed backward-tilted uterus). If you suspect perforation has occurred, consult your doctor immediately and inform them that you have Mirena inserted, especially if they were not the person who inserted it.
Possible signs and symptoms of perforation may include:
- Severe pain (similar to menstrual cramps) or unusually strong pain
- Heavy bleeding (after insertion)
- Pain or bleeding that persists for more than a few weeks
- Sudden change in your periods
- Pain during sexual intercourse
- You can no longer locate the Mirena threads (see section 3 “How to use Mirena – How can I tell if Mirena is correctly positioned?”)
Breast cancer
Women who take oral contraceptives have a slightly increased risk of breast cancer. This risk returns to the baseline level appropriate for age 10 years after stopping the pill.
Some scientific studies have suggested a slightly increased risk of breast cancer with the use of the levonorgestrel-releasing IUD such as Mirena, while other studies have not indicated an increased risk. Discuss any concerns with your doctor.
Ectopic pregnancy
It is very unlikely that you will become pregnant while using Mirena. However, if you do become pregnant while using Mirena, the risk that the fetus develops outside the uterus (ectopic pregnancy) is relatively increased. Approximately 1 in 1,000 women per year who use Mirena correctly experience an ectopic pregnancy. This is lower than in women who use no contraceptive method (approximately 3 to 5 per 1,000 women per year). Women who have previously had an ectopic pregnancy, tubal surgery, or pelvic infection have a higher risk. An ectopic pregnancy is a serious condition requiring immediate medical attention. The following symptoms may indicate an ectopic pregnancy; if so, you must see your doctor immediately:
- Your period has stopped, but you then develop persistent bleeding or pain
- You experience diffuse or severe pain in the lower abdomen
- You have normal signs of pregnancy but continue to bleed and feel dizzy.
Dizziness
Some women feel dizzy after Mirena insertion. This is a normal physical response. Your doctor will advise you to rest for a while after Mirena insertion.
Enlarged ovarian follicles (cells surrounding a mature egg in the ovary)
Because the contraceptive effect of Mirena is primarily local, ovulatory cycles with follicular rupture are common in women of reproductive age. Occasionally, follicular degeneration is delayed and development may continue. Most of these follicles do not cause symptoms, although some may be associated with pelvic pain or pain during sexual intercourse. Enlarged follicles may require medical attention but usually resolve spontaneously.
Psychiatric disorders
Some women using hormonal contraceptives such as Mirena have reported depression or depressed mood. Depression can be severe and may sometimes lead to suicidal thoughts. If you experience mood changes or depressive symptoms, contact your doctor for further medical advice as soon as possible.
Other medicines and Mirena
The mechanism of action of Mirena is primarily local; therefore, taking other medicines is not expected to increase the risk of pregnancy during Mirena use. However, consult your doctor if you are taking or have recently taken any other medicines, including over-the-counter medicines.
Pregnancy, breastfeeding, and fertility
Pregnancy
Mirena must not be used during pregnancy or suspected pregnancy.
It is very rare for a woman to become pregnant with Mirena in place. However, if Mirena is expelled, you will no longer be protected and should use another contraceptive method until you see your doctor.
In some women, periods may stop while using Mirena. Absence of periods is not necessarily a sign of pregnancy. If you do not have periods and also experience other signs of pregnancy (e.g., nausea, fatigue, breast tenderness), visit your doctor for an examination and a pregnancy test.
If you become pregnant with Mirena in place, you must see your healthcare provider immediately to have Mirena removed. Removal may cause miscarriage. However, if Mirena is left in place during pregnancy, not only is the risk of spontaneous miscarriage increased, but also the risk of premature delivery. If Mirena cannot be removed, consult your healthcare provider about the benefits and risks of continuing the pregnancy. If the pregnancy continues, you will be closely monitored, and you must contact your doctor immediately if you experience stomach cramps, stomach pain, or fever.
Mirena contains a hormone called levonorgestrel, and isolated cases of effects on the genitalia of female infants have been reported when exposed to levonorgestrel-releasing intrauterine devices while in the uterus.
Breastfeeding
Mirena can be used during breastfeeding. Levonorgestrel has been detected in small amounts in the milk of breastfeeding women (0.1% of the dose is transferred to the infant). When Mirena is used starting six weeks after childbirth, it appears to have no negative effects on the child's growth or development. Progestogen-only hormonal contraceptives do not appear to affect the quantity or quality of breast milk.
Hormonal contraceptives are not recommended as the first-choice contraceptive method during breastfeeding; only non-hormonal methods are considered first-line, followed by progestogen-only contraceptives such as Mirena. The daily dose and blood concentrations of levonorgestrel with Mirena are lower than with any other hormonal contraceptive method.
Fertility
After removal of Mirena, women regain normal fertility.
If you are pregnant or breastfeeding, think you may be pregnant, or plan to become pregnant, consult your doctor or pharmacist before using this medicine.
Driving and use of machines
No effects have been observed.
Mirena contains barium sulfate
The T-shaped structure of Mirena contains barium sulfate, which makes it visible during X-ray examination.
3. How to use Mirena
What is the effectiveness of Mirena?
In contraception, Mirena is as effective as the most modern and effective copper IUDs. Studies (clinical trials) showed approximately two pregnancies per 1,000 women using Mirena during the first year.
In the treatment of idiopathic menorrhagia, Mirena causes a marked reduction in menstrual bleeding after three months of use. Some users may stop having periods altogether.
When should Mirena be inserted?
Starting to use Mirena
- Before inserting Mirena, it must be confirmed that you are not pregnant.
- Mirena should be inserted within 7 days from the start of menstruation. When inserted during this time, Mirena is effective immediately and will prevent pregnancy from the moment of insertion.
- If Mirena cannot be inserted within 7 days from the start of menstruation, or if your menstrual cycle is irregular, Mirena may be inserted on any other day. In this case, you must not have had unprotected sexual intercourse since your last menstrual period, and you must have a negative pregnancy test before insertion. Additionally, Mirena may not reliably prevent pregnancy immediately after insertion. Therefore, you must use a barrier contraceptive method (such as a condom) or abstain from vaginal intercourse for the first 7 days following Mirena insertion.
- Mirena is not indicated for use as emergency contraception (postcoital contraception).
Starting to use Mirena after childbirth
- Mirena may be inserted after childbirth once the uterus has returned to its normal size, and not earlier than 6 weeks after delivery (see section 2 “What you need to know before starting to use Mirena – Perforation”).
- See also “Starting to use Mirena” above for additional information regarding timing of insertion.
Starting to use Mirena after an abortion
Mirena may be inserted immediately after an abortion if the pregnancy lasted less than 3 months, provided there are no genital infections. Mirena will be effective from the moment of insertion.
Replacing Mirena
Mirena may be replaced at any time during your menstrual cycle with a new Mirena device. The new Mirena will be effective immediately upon insertion.
Switching from another contraceptive method (such as combined hormonal contraceptives, implants)
- Mirena may be inserted immediately if it can be confirmed that you are not pregnant.
- If more than 7 days have passed since the start of menstrual bleeding, you should abstain from vaginal intercourse or use additional contraceptive protection for the following 7 days.
How is Mirena inserted?
Mirena must be inserted by a healthcare professional experienced in Mirena insertion.
After a gynecological examination, a speculum is inserted into the vagina and the cervix is cleaned with an antiseptic solution. The IUD is then inserted into the uterus using a thin, flexible plastic tube (the inserter). Local anesthesia may be applied to the cervix before insertion if necessary.
Some women may experience pain and dizziness after insertion. If these symptoms do not resolve within half an hour of rest, it may indicate that the IUD is not correctly positioned. An examination should be performed, and removal of the IUD may be necessary.
After Mirena placement, your doctor should provide you with a patient reminder card for follow-up visits. Bring this card to every visit.
When should I see my doctor?
You should have your IUD checked 4–12 weeks after insertion, and then regularly, at least once a year. Your doctor will determine the frequency and type of check-ups appropriate for your individual case. Bring the patient reminder card provided by your doctor to every visit.
Additionally, you should consult your doctor if any of the following occur:
- You can no longer feel the removal threads in your vagina
- You can feel the lower part of the device
- You think you might be pregnant
- You experience prolonged abdominal pain, fever, or abnormal vaginal discharge
- You or your partner feel pain or discomfort during sexual intercourse
- You experience sudden changes in your menstruation (for example: if you previously had light or no bleeding and suddenly begin continuous bleeding, or experience pain or start bleeding heavily)
- You develop other medical problems such as migraine-type headaches or recurrent severe headaches, sudden vision problems, jaundice, or increased blood pressure
- You develop any of the conditions mentioned in section 2 “What you need to know before starting to use Mirena”.
Always remind your doctor that you have Mirena inserted, especially if it is not the same doctor who inserted it.
How long can Mirena be used?
Mirena is effective for 8 years when used for pregnancy prevention (contraception). Are you using Mirena for this reason? If so, your Mirena must be removed or replaced no later than after 8 years.
Mirena is effective for 5 years for heavy menstrual bleeding (idiopathic menorrhagia). Are you using Mirena for this reason? If so, your Mirena must be removed or replaced when heavy menstrual bleeding returns or no later than after 8 years.
If desired, a new Mirena may be inserted when the old one is removed.
What happens if I want to become pregnant or remove Mirena for any other reason?
The IUD can be easily removed by your doctor at any time, after which pregnancy becomes possible. Removal is usually a painless procedure. Fertility returns to normal after Mirena removal.
Continuation of contraception after removal
If you do not wish to become pregnant, Mirena should not be removed after the seventh day of the menstrual cycle (menstrual period) unless contraception is ensured with another method (e.g., condoms) for at least seven days prior to removal. If you have irregular periods or no periods, you should use barrier contraceptive methods starting seven days before removal and continuing until your menstruation returns. Alternatively, a new Mirena may be inserted immediately after removal; in this case, additional protection is not needed. If you do not wish to continue with the same contraceptive method, consult your doctor about other reliable contraceptive options.
Can I become pregnant after stopping Mirena?
Yes. After Mirena is removed, it will not interfere with your normal fertility. You may become pregnant during the first menstrual cycle after Mirena removal.
Can Mirena affect my menstrual periods?
Mirena affects your menstrual cycle. It may cause changes such as spotting (light bleeding), shorter or longer periods, light or heavy bleeding, or absence of bleeding.
During the first 3–6 months after Mirena insertion, many women experience frequent spotting or light bleeding in addition to their regular periods. Some women may have heavy or prolonged bleeding during this time. Please inform your doctor, especially if this persists.
In general, you will likely experience a gradual reduction in both the number of bleeding days and the amount of blood lost each month. Over time, some women notice that their periods stop completely. Since menstrual blood loss typically decreases with Mirena use, most women experience an increase in their blood hemoglobin levels.
When the device is removed, menstrual periods return to normal.
Is it abnormal not to have periods?
No, when using Mirena. If you do not have periods while using Mirena, it is due to the hormone’s effect on the uterine lining. Monthly thickening of the lining does not occur, so there is nothing to be shed as a period. This does not necessarily mean you have reached menopause or that you are pregnant. Your own hormone levels remain normal.
In fact, the absence of periods can be a significant health benefit for women.
How can I know if I am pregnant?
Pregnancy is unlikely in women using Mirena, even if they do not have periods.
If you have not had a period for six weeks and are concerned, consider taking a pregnancy test. If the test is negative, there is no need to repeat it unless you develop other signs of pregnancy, such as nausea, fatigue, or breast tenderness.
Can Mirena cause pain or discomfort?
Some women experience pain (similar to menstrual cramps) during the first few weeks after insertion. You should return to your doctor or clinic if you have severe pain or if the pain lasts longer than three weeks after Mirena insertion.
Can Mirena interfere with sexual intercourse?
Neither you nor your partner should feel the IUD during sexual intercourse. If you do, you should avoid sexual intercourse until your doctor confirms that the IUD is correctly positioned.
How long should I wait after Mirena insertion before having sexual intercourse?
To allow your body to rest, it is best to wait 24 hours after Mirena insertion before having sexual intercourse. Depending on when in your menstrual cycle Mirena was inserted, you may need to use a barrier method (such as a condom) or abstain from sexual intercourse for the first 7 days after insertion (see section 3 “How to use Mirena – When should Mirena be inserted?”).
Can tampons or menstrual cups be used?
The use of sanitary pads is recommended. If tampons or menstrual cups are used, they should be changed carefully to avoid pulling on the Mirena removal threads. If you suspect that Mirena has been displaced (see “When should I see my doctor?” for possible signs), avoid sexual intercourse or use a barrier method (such as condoms), and contact your doctor.
What happens if Mirena comes out?
It is rare but possible that Mirena may be expelled during your period without you noticing. An unusually heavy flow during your period may indicate that Mirena has completely passed out through the vagina. It is also possible that part of Mirena may be expelled from the uterus (you or your partner may notice this during sexual intercourse). If Mirena is completely or partially expelled, you will not be protected against pregnancy.
How can I tell if Mirena is correctly positioned?
You can check whether the removal threads are in place. Gently insert a finger into your vagina and feel for the removal threads at the end of your vagina, near the opening of your uterus (cervix).
Do not pull on the removal threads, as you could accidentally dislodge Mirena. If you cannot feel the removal threads, this may indicate expulsion or perforation. In this case, use a barrier contraceptive method (such as condoms) and consult your doctor immediately.
4. Possible adverse effects
Like all medicines, this medicine can cause adverse effects, although not everyone will experience them.
In addition to the possible adverse effects described in other sections (e.g., section 2 “What you need to know before starting to use Mirena”), the following are possible adverse effects listed according to the body systems affected and their frequency:
Very common adverse effects: may affect more than 1 in 10 people:
Disorders of the reproductive system and breast
- Uterine or vaginal bleeding, including spotting, infrequent periods (oligomenorrhea), and absence of bleeding (amenorrhea)
- Benign ovarian cysts (see section 2 “Enlarged ovarian follicles”)
Common adverse effects: may affect up to 1 in 10 people:
Psychiatric disorders
- Depressed mood or depression
- Nervousness
- Decreased libido
Nervous system disorders
- Headache
Vascular disorders
- Dizziness
Gastrointestinal disorders
- Abdominal pain
- Nausea (feeling sick)
Skin and subcutaneous tissue disorders
- Acne
Musculoskeletal, connective tissue and bone disorders
- Back pain
Reproductive system and breast disorders
- Pelvic pain
- Dysmenorrhea (painful menstruation)
- Vaginal discharge
- Vulvovaginitis (inflammation of the external genital organs or vagina)
- Breast tenderness
- Breast pain
- Expulsion of the intrauterine contraceptive device
Investigations
- Weight gain
Uncommon adverse effects: may affect up to 1 in 100 people:
Nervous system disorders
- Migraine
Gastrointestinal disorders
- Abdominal distension
Skin and subcutaneous tissue disorders
- Hirsutism (excessive body hair)
- Hair loss (alopecia)
- Pruritus (intense itching)
- Eczema (skin inflammation)
- Chloasma (golden-brown skin patches) or skin hyperpigmentation
Reproductive system and breast disorders
- Uterine perforation
- Pelvic inflammatory disease (infection of the upper female genital tract, affecting female structures above the cervix)
- Endometritis
- Cervicitis/Pap smear normal, class II (inflammation of the cervix)
General disorders and administration site conditions
- Edema (swelling)
Rare adverse effects: may affect up to 1 in 1,000 people:
Skin and connective tissue disorders
- Rash
- Urticaria (hives)
If you become pregnant while using Mirena, there is a possibility that the pregnancy may develop outside the uterus (see section 2 “Ectopic pregnancy”).
Cases of sepsis (a severe systemic infection that may be life-threatening) have been reported following IUD insertion.
Reporting of adverse effects
If you experience any type of adverse effect, consult your doctor, pharmacist, or nurse, even if it is a possible adverse effect not listed in this leaflet. You can also report them directly through the Spanish Pharmacovigilance System for Human Medicines: https://www.notificaram.es. By reporting adverse effects, you can help provide more information on the safety of this medicine.
5. Storage of Mirena
Keep this medicine out of the sight and reach of children.
No special storage conditions are required.
Do not use this medicine after the expiry date stated on the packaging. The expiry date refers to the last day of the month indicated.
Medicines must not be disposed of via wastewater or household waste. Unused containers and medicines should be taken to the SIGRE collection point at your pharmacy. If you have any doubts, ask your pharmacist how to dispose of unused containers and medicines. This will help protect the environment.
6. Package contents and other information
Composition of Mirena
- The active substance is levonorgestrel. The intrauterine delivery system contains 52 mg of levonorgestrel.
- The other components are polydimethylsiloxane elastomer, anhydrous colloidal silica, polyethylene, barium sulfate, and iron oxide.
Appearance of the product and contents of the pack
Pack contents: one sterile intrauterine delivery system for intrauterine use.
Marketing Authorisation Holder
Bayer Hispania, S.L.
Av. Baix Llobregat 3-5
08970 Sant Joan Despí (Barcelona)
Spain
Manufacturer
Bayer Oy
Pansiontie 47
20210 Turku
Finland
For any information about this medicinal product, please contact the Marketing Authorisation Holder:
Bayer Hispania, S.L.
Av. Baix Llobregat 3-5
08970 Sant Joan Despí (Barcelona)
Spain
IF YOU HAVE ANY FURTHER QUESTIONS, PLEASE CONSULT YOUR DOCTOR OR PHARMACIST.
Date of most recent review of this leaflet: November 2025
Detailed information on this medicinal product is available on the website of the Spanish Agency for Medicines and Health Products (AEMPS) (http://www.aemps.gob.es/).
Other sources of information
You can access detailed and up-to-date information on this medicinal product by scanning with your mobile phone (smartphone) the QR code included in the package leaflet, packaging, and patient reminder card. You can also access the same information at the following internet address: https://cima.aemps.es/info/63158
The following information is intended for healthcare professionals only:
INSERTION INSTRUCTIONS
Mirena 0.02 mg per 24 hours intrauterine delivery system
Must be inserted by a healthcare professional using an aseptic technique.
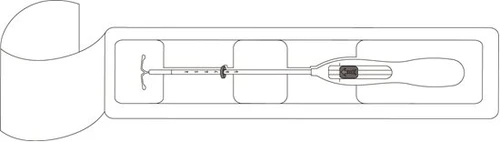
Mirena is supplied within an inserter, in a sterile pack which should not be opened until immediately before use. Do not re-sterilize. As supplied, Mirena is for single use only. Do not use if the inner pack is damaged or open. Do not insert after the expiry month and year stated on the label.
For guidance on the timing of insertion, refer to the Summary of Product Characteristics of Mirena.
Mirena includes within the pack a patient reminder card. Complete the patient reminder card and give it to the patient after insertion.
Preparation for insertion
-
Examine the patient to rule out contraindications to Mirena insertion and to exclude pregnancy (see Summary of Product Characteristics, section 4.3 and section 4.4 under Medical examination/consultation).
-
Insert a speculum, visualize the cervix, and then thoroughly clean the cervix and vagina with an appropriate antiseptic solution.
-
Assist with an assistant if necessary.
-
Grasp the anterior lip of the cervix with a tenaculum or other cervical forceps to stabilize the uterus. If the uterus is retroverted, grasping the posterior lip of the cervix may be more appropriate. Gentle traction may be applied with the forceps to straighten the cervical canal. The forceps should remain in place, and gentle traction on the cervix should be maintained throughout the entire insertion procedure.
-
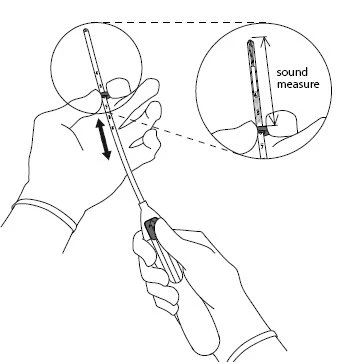
Insert a uterine sound through the cervical canal to the fundus to measure uterine depth and confirm uterine cavity direction, and to rule out any intrauterine abnormalities (e.g., septum, submucosal fibroids) or the presence of a previously inserted intrauterine contraceptive device not yet removed. If difficulties are encountered, consider cervical dilation. If cervical dilation is required, consider the use of analgesics and/or paracervical block.
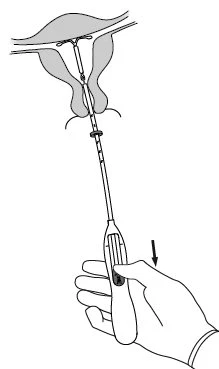
Insertion
| |
| |
|
|
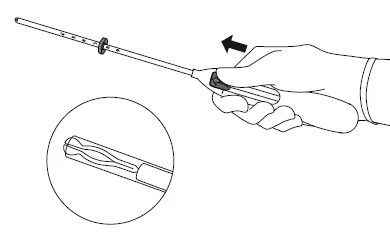
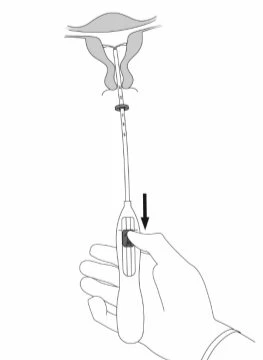
IMPORTANT! Do not pull the slider downward, as this may prematurely release Mirena. Once released, Mirena cannot be reloaded.
| |
|
|
|
|
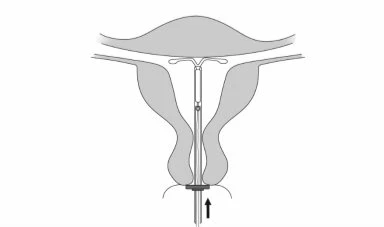
IMPORTANT! Do not force the inserter. Dilate the cervical canal if necessary.
| |
|
|
|
|
|
|









IMPORTANT!
If incorrect positioning of the system is suspected, check its location (e.g., by ultrasound). Remove the system if it is not correctly placed within the uterine cavity. A removed system must not be reinserted.
Removal/reinsertion
For removal/replacement, refer to the Mirena product information.

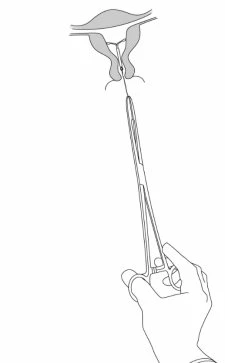
Mirena is removed by gently pulling on the threads with forceps (Figure 8). A new Mirena can be inserted immediately after removal. After Mirena removal, the system should be examined to ensure it is intact and has been completely removed. |