Relvar ellipta
Ukraine
Table of Contents
INSTRUCTIONS FOR MEDICAL USE OF THE MEDICINAL PRODUCT RELVAR ELLIPTA (RELVARELLIPTA)
Composition:
Active substances: fluticasone furoate, vilanterol;
One delivered dose contains 92 mcg of fluticasone furoate and 22 mcg of vilanterol (as trifenatate);
this corresponds to a pre-metered dose of 100 mcg fluticasone furoate and 25 mcg vilanterol (as trifenatate);
Excipients: lactose monohydrate; magnesium stearate.
Pharmaceutical form. Powder for inhalation.
Main physicochemical properties: white powder in a light grey inhaler with a pale blue spray cap and dose counter.
Pharmacotherapeutic group. Medicinal products used in obstructive respiratory diseases. Adrenergic drugs for inhalation use. Adrenergic agents in combination with corticosteroids and others, including anticholinergics. Vilanterol and fluticasone furoate. ATC code R03AK10.
Pharmacological Properties.
Pharmacodynamics.
Mechanism of action
Fluticasone furoate and vilanterol are representatives of two classes of medicinal products (a synthetic corticosteroid and a long-acting selective beta2-receptor agonist).
Pharmacodynamic effects
Fluticasone furoate
Fluticasone furoate is a synthetic trifluorinated corticosteroid with potent anti-inflammatory activity. The precise mechanism by which fluticasone furoate affects symptoms of asthma and COPD is unknown. Corticosteroids have demonstrated a broad range of actions on various cell types (including eosinophils, macrophages, and lymphocytes) and mediators (e.g., cytokines and chemokines involved in inflammation).
Vilanterol trifenatate
Vilanterol trifenatate is a selective long-acting beta2-adrenergic receptor agonist (LABA).
The pharmacological effects of beta2-adrenergic receptor agonists, including vilanterol trifenatate, are at least partially related to stimulation of intracellular adenylate cyclase, an enzyme that catalyzes the conversion of adenosine triphosphate (ATP) to cyclic 3',5'-adenosine monophosphate (cyclic AMP). Increased levels of cyclic AMP lead to relaxation of bronchial smooth muscle and inhibition of mediator release from cells involved in immediate hypersensitivity reactions, particularly mast cells.
Molecular interactions occur between corticosteroids and LABAs, whereby corticosteroids activate the beta2-receptor gene, increasing receptor number and sensitivity, while LABAs prime glucocorticoid receptors for steroid-dependent activation and enhance cellular nuclear translocation. These synergistic interactions are reflected in enhanced anti-inflammatory activity, demonstrated in vitro and in vivo in several inflammatory cells associated with the pathophysiology of asthma and COPD. Bronchial biopsy studies using fluticasone furoate and vilanterol at clinical doses have also demonstrated synergy between corticosteroids and LABAs in patients with COPD.
Pharmacokinetics.
Absorption. The absolute bioavailability of fluticasone furoate and vilanterol following inhalation as fluticasone furoate/vilanterol averaged 15.2% and 27.3%, respectively. Oral bioavailability of fluticasone furoate and vilanterol was low, averaging 1.26% and < 2%, respectively. Due to this low oral bioavailability, systemic exposure to fluticasone furoate and vilanterol after inhalation is predominantly related to absorption of the inhaled fraction of the dose deposited in the lungs.
Distribution. Following intravenous administration, fluticasone furoate and vilanterol are widely distributed, with mean volumes of distribution at steady state of 661 L and 165 L, respectively.
Fluticasone furoate and vilanterol exhibit minimal binding to erythrocytes. In vitro plasma protein binding of fluticasone furoate and vilanterol in human blood plasma is high, averaging > 99.6% and 93.9%, respectively. In vitro plasma protein binding in patients with renal or hepatic impairment is not reduced.
Fluticasone furoate and vilanterol are substrates for P-glycoprotein (P-gp); however, co-administration of fluticasone furoate/vilanterol with P-gp inhibitors is unlikely to alter systemic exposure to fluticasone furoate/vilanterol due to their good absorption.
Biological transformation. In vitro data indicate that the primary metabolic pathways for fluticasone furoate and vilanterol in humans are predominantly mediated by CYP3A4.
Fluticasone furoate is primarily metabolized via hydrolysis of the S-fluoromethyl-carbothioate group to metabolites with substantially reduced corticosteroid activity. Vilanterol is primarily metabolized via O-dealkylation to metabolites with substantially reduced β1- and β2-agonist activity.
Elimination. After oral administration, fluticasone furoate is eliminated in humans primarily through metabolism, with metabolites excreted almost entirely in feces, and < 1% of the recovered radioactive dose excreted in urine.
After oral administration, vilanterol is eliminated primarily via metabolism, with subsequent excretion of metabolites in urine and feces at approximately 70% and 30% of the radioactive dose, respectively, in a human study using radiolabeled compounds. The expected elimination half-life of vilanterol in plasma after a single inhalation of fluticasone furoate/vilanterol averaged 2.5 hours. The effective half-life of accumulated vilanterol, determined after repeated inhalation of 25 mcg doses of vilanterol, is 16 hours in patients with asthma and 21.3 hours in patients with COPD.
Children. No dosage adjustment recommendations are available for adolescents (aged 12 years and older).
The pharmacokinetics of fluticasone furoate/vilanterol have not been studied in patients under 12 years of age. The safety and efficacy of fluticasone furoate/vilanterol in children under 12 years of age have not been established.
Special patient groups
Elderly patients (> 65 years)
The effect of age on the pharmacokinetics of fluticasone furoate and vilanterol was evaluated in Phase III studies in patients with COPD and asthma. There was no evidence of age (12–84 years) affecting the pharmacokinetics of fluticasone furoate and vilanterol in patients with asthma.
There was no evidence of age affecting the pharmacokinetics of fluticasone furoate and vilanterol in patients with COPD, although an increase (37%) in AUC(0–24) of vilanterol was observed across the studied age range (41–84 years). For elderly patients (84 years) with low body weight (35 kg), AUC(0–24) of vilanterol is predicted to be more than 35% higher compared to the reference population (COPD patients aged 60 years with body weight 70 kg), while Cmax remains unchanged. These differences are unlikely to be of clinical significance.
No dosage adjustment is recommended for elderly patients with asthma or COPD.
Renal impairment. Clinical pharmacology studies of fluticasone furoate/vilanterol showed that severe renal impairment (creatinine clearance < 30 mL/min) does not result in substantially increased exposure to fluticasone furoate or vilanterol, or in more pronounced systemic corticosteroid or beta2-agonist effects compared to those with normal renal function.
No dose adjustment is necessary for patients with renal impairment.
The effect of hemodialysis has not been studied.
Hepatic impairment. After 7 days of repeated dosing with fluticasone furoate/vilanterol, systemic exposure to fluticasone furoate increased (up to threefold, as measured by AUC(0–24)) in patients with hepatic impairment (Child–Pugh class A, B, or C) compared to healthy volunteers. This increased systemic exposure to fluticasone furoate in patients with moderate hepatic impairment (Child–Pugh class B; fluticasone furoate/vilanterol 184/22 mcg) was associated with a mean 34% reduction in serum cortisol compared to healthy volunteers. Dose-normalized systemic exposure to fluticasone furoate was similar in patients with moderate and severe hepatic impairment (Child–Pugh class B or C).
After 7 days of repeated dosing with fluticasone furoate/vilanterol, no clinically significant increase in systemic exposure to vilanterol (Cmax and AUC) was observed in patients with mild, moderate, or severe hepatic impairment (Child–Pugh class A, B, or C).
There were no clinically significant effects of the fluticasone furoate/vilanterol combination on systemic beta-adrenergic effects (heart rate or serum potassium levels) in patients with mild or moderate hepatic impairment (vilanterol 22 mcg) or severe hepatic impairment (vilanterol 12.5 mcg) compared to healthy volunteers.
Other special groups
In asthma, AUC(0–24) of fluticasone furoate in patients of East Asian, Japanese, and Southeast Asian origin (12–13% of patients) was on average 33–53% higher compared to other patient groups. However, there was no evidence of greater systemic exposure in this population associated with greater effects on urinary cortisol excretion. On average, Cmax of vilanterol is predicted to be 220–287% higher, while AUC(0–24) is comparable between Asian and non-Asian patients. There was no evidence that this higher Cmax of vilanterol led to clinically significant effects on heart rate.
In COPD, AUC(0–24) of fluticasone furoate in patients of East Asian, Japanese, and Southeast Asian origin (13–14% of patients) was on average 23–30% higher compared to Caucasian patients. However, there was no evidence of greater systemic exposure in this population associated with greater effects on urinary cortisol excretion. Race did not influence the pharmacokinetic parameters of vilanterol in patients with COPD.
Sex, body weight, and BMI
There was no evidence of influence of sex, body weight, or body mass index (BMI) on the pharmacokinetics of fluticasone furoate based on pharmacokinetic analysis data from Phase III studies in 1213 patients with asthma (712 women) and 1225 patients with COPD (392 women).
There was no evidence of influence of sex, body weight, or BMI on the pharmacokinetics of vilanterol based on population pharmacokinetic analysis data in 856 patients with asthma (500 women) and 1091 patients with COPD (340 women).
No dose adjustment is necessary based on sex, body weight, or BMI.
Clinical characteristics.
Indications.
Asthma
Regular treatment of asthma in adults and children aged 12 years and older who require combination therapy (long-acting beta2-agonist and inhaled corticosteroid):
- patients whose disease is not adequately controlled with inhaled corticosteroids and as-needed inhaled short-acting beta2-agonists;
- patients who have already achieved adequate disease control with an inhaled corticosteroid and a long-acting inhaled beta2-agonist.
COPD (chronic obstructive pulmonary disease)
Symptomatic treatment of adults with COPD with FEV1 < 70% of predicted values (post-bronchodilator) and a history of exacerbations despite regular bronchodilator therapy.
Contraindications.
Hypersensitivity to the active substances or to any of the excipients of the medicinal product.
Interaction with other medicinal products and other forms of interactions.
Clinically significant interactions mediated by fluticasone furoate/vilanterol at clinical doses are considered unlikely due to low plasma concentrations achieved after inhalation.
Beta-blockers
Beta2-adrenergic receptor blockers may attenuate or antagonize the effects of beta2-adrenergic receptor agonists. Concomitant use of non-selective and selective beta2-adrenergic receptor blockers should be avoided unless there are compelling reasons for their use.
Inhibitors of CYP3A4
Fluticasone furoate and vilanterol are rapidly eliminated due to extensive first-pass metabolism mediated by the hepatic enzyme CYP3A4.
Caution is required when co-administering with strong CYP3A4 inhibitors (e.g., ketoconazole, ritonavir), as there is a potential for increased systemic exposure to fluticasone furoate and vilanterol; therefore, concomitant use should be avoided. A drug interaction study with repeated doses of a CYP3A4 inhibitor was conducted in healthy volunteers using a combination of fluticasone furoate/vilanterol (184/22 mcg) and the strong CYP3A4 inhibitor ketoconazole (400 mg). Concomitant administration increased the mean AUC(0–24) and Cmax of fluticasone furoate by 36% and 33%, respectively. The increased exposure to fluticasone furoate was associated with a 27% reduction in the weighted mean serum cortisol over 0–24 hours. Concomitant administration increased the mean AUC(0–t) and Cmax of vilanterol by 65% and 22%, respectively. The increased exposure to vilanterol was not associated with increased systemic effects on heart rate, blood potassium levels, or QTcF interval prolongation related to beta2-agonist activity.
P-glycoprotein inhibitors
Fluticasone furoate and vilanterol are substrates of P-glycoprotein (P-gp). A clinical pharmacology study in healthy volunteers with concomitant administration of vilanterol and a potent P-gp inhibitor as well as a moderate CYP3A4 inhibitor, verapamil, showed no significant effect on the pharmacokinetics of vilanterol. A clinical pharmacology study with a specific P-gp inhibitor and fluticasone furoate has not been conducted.
Sympathomimetics
Concomitant use with other sympathomimetics (either as monotherapy or as part of combination therapy) may increase the risk of adverse reactions to fluticasone furoate/vilanterol. Relvar Ellipta must not be used concomitantly with other long-acting beta2-adrenergic receptor agonists or medicinal products containing long-acting beta2-adrenergic receptor agonists.
Paediatric population
Interactions have only been studied in adult patients.
Special precautions for use.
Worsening of disease
Fluticasone furoate/vilanterol must not be used for the treatment of acute asthma symptoms or acute exacerbations of COPD requiring short-acting bronchodilators. An increased frequency of using short-acting bronchodilators to relieve symptoms indicates worsening control, and in such cases, the patient should be evaluated by a physician.
Patients must not discontinue treatment with fluticasone furoate/vilanterol for asthma or COPD without consulting a physician, as symptoms may recur after stopping therapy.
During treatment with fluticasone furoate/vilanterol, adverse events and exacerbations related to asthma may occur. Patients should be advised to continue treatment but to seek medical advice if asthma symptoms are not controlled or worsen after inhalation of Relvar™ Ellipta.
Paradoxical bronchospasm
Paradoxical bronchospasm may occur, characterized by a sudden and rapid increase in wheezing immediately after dosing. This requires urgent treatment with short-acting inhaled bronchodilators. Relvar Ellipta must be discontinued immediately, the patient evaluated, and alternative therapy initiated if necessary.
Cardiovascular effects
Cardiovascular effects such as cardiac arrhythmias, including supraventricular tachycardia and extrasystoles, may occur with sympathomimetics, including Relvar Ellipta. In a placebo-controlled trial involving patients with moderate COPD or a history of increased cardiovascular risk, no increase in the risk of cardiovascular events was observed with fluticasone furoate/vilanterol compared to placebo. However, fluticasone furoate/vilanterol should be used with caution in patients with severe cardiovascular disorders or cardiac rhythm disturbances, thyrotoxicosis, uncorrected hypokalemia, or in patients predisposed to low serum potassium levels.
Patients with hepatic impairment
Patients with moderate to severe hepatic impairment should receive the 92/22 mcg dose, with careful monitoring for systemic corticosteroid-related adverse reactions (see section "Pharmacokinetics").
Systemic effects of corticosteroids
Systemic effects may occur with any inhaled corticosteroid, particularly at high doses used over prolonged periods. These effects are much less likely than with oral corticosteroids. Possible systemic effects include Cushing's syndrome, Cushingoid features, adrenal suppression, decreased bone mineral density, growth retardation in children and adolescents, cataract, glaucoma, and less frequently, various physiological and behavioral reactions including psychomotor hyperactivity, sleep disturbances, anxiety, depression, or aggression (particularly in children).
Fluticasone furoate/vilanterol should be used with caution in patients with pulmonary tuberculosis and in patients with chronic or untreated infections.
Visual disturbances
Visual disturbances have been reported with both systemic and local administration of corticosteroids. If symptoms such as blurred vision or other visual disturbances occur, the patient should be referred to an ophthalmologist to evaluate possible causes, which may include cataract, glaucoma, or rare conditions such as central serous chorioretinopathy (CSCR), reported after both systemic and local corticosteroid use.
Hyperglycemia
Elevated blood glucose levels have been reported in patients with diabetes mellitus and should be considered when prescribing the drug to patients with a history of diabetes.
Pneumonia in patients with COPD
An increased incidence of pneumonia has been observed in patients with COPD receiving fluticasone furoate/vilanterol. There was also an increased frequency of pneumonia leading to hospitalization. In some cases, these pneumonias were fatal (see section "Adverse reactions"). Physicians should consider the possibility of pneumonia in patients with COPD, as the clinical signs of such infections partially overlap with symptoms of COPD exacerbation. Risk factors for pneumonia in patients with COPD receiving fluticasone furoate/vilanterol include smoking, history of pneumonia, body mass index < 25 kg/m², and forced expiratory volume in 1 second (FEV1) < 50% of predicted. These factors should be considered when prescribing fluticasone furoate/vilanterol; treatment should be re-evaluated if pneumonia occurs.
Relvar Ellipta 184/22 mcg is not indicated for patients with COPD. There is no additional benefit of the 184/22 mcg dose compared to the 92/22 mcg dose, and there is a potentially increased risk of pneumonia and systemic corticosteroid-related adverse reactions (see section "Adverse reactions").
Pneumonia in patients with asthma occurred more frequently at higher doses. The incidence of pneumonia in asthma patients receiving fluticasone furoate/vilanterol 184/22 mcg was higher compared to those receiving fluticasone furoate/vilanterol 92/22 mcg or placebo (see section "Adverse reactions"). No specific risk factors have been identified.
Excipients
Patients with rare hereditary conditions such as galactose intolerance, lactase deficiency, or glucose-galactose malabsorption should not take this medicine.
Use during pregnancy or breastfeeding.
Pregnancy. Animal studies have shown reproductive toxicity at doses not considered clinically relevant. There are insufficient data on the use of fluticasone furoate and vilanterol trifenatate in pregnant women.
Fluticasone furoate/vilanterol may be used during pregnancy only if the expected benefit to the woman outweighs any potential risk to the fetus.
Breastfeeding. There is insufficient information on the excretion of fluticasone furoate or vilanterol trifenatate and/or their metabolites in human milk. However, other corticosteroids and beta2-agonists have been detected in human breast milk. Risk to breastfed infants cannot be excluded.
A decision should be made whether to discontinue breastfeeding or to discontinue therapy with fluticasone furoate/vilanterol, taking into account the benefit of breastfeeding for the child and the benefit of therapy for the woman.
Fertility. There are no data on the effect of the drug on human fertility. Animal studies did not show any effect of fluticasone furoate/vilanterol trifenatate on reproductive function.
Ability to drive and use machines.
Fluticasone furoate and vilanterol have no influence on the ability to drive or operate machinery.
Method of Administration and Dosage.
Dosage
-
Asthma *
-
Adults and children aged 12 years and older *
One inhalation of Relvar Ellipta 92/22 mcg once daily.
Patients usually experience improvement in lung function within 15 minutes after inhalation.
Patients should be informed that regular daily use is necessary to maintain control of asthma symptoms and that treatment should be continued even in the absence of symptoms.
If symptoms occur between inhalations, a short-acting beta2-agonist should be used for immediate relief.
The initial dose of Relvar Ellipta 92/22 mcg should be considered for adults and children aged 12 years and older who require low or medium doses of inhaled corticosteroids in combination with long-acting beta2-agonists. If the patient's condition is not adequately controlled with Relvar Ellipta 92/22 mcg, the dose may be increased to 184/22 mcg, which may provide additional improvement in asthma control.
Patients should undergo regular medical evaluations to ensure that the dose of fluticasone furoate/vilanterol they are receiving remains optimal and should only be changed upon a physician's recommendation. The dose should be adjusted to the lowest dose at which effective symptom control is maintained.
Patients with asthma should receive a dose of Relvar Ellipta containing a fluticasone furoate (FF) dose appropriate to the severity of their disease. Prescribing healthcare professionals should be aware that for asthma patients, fluticasone furoate (FF) 100 mcg once daily is approximately equivalent to fluticasone propionate (FP) 250 mcg twice daily, and FF 200 mcg once daily is approximately equivalent to FP 500 mcg twice daily.
- Children under 12 years of age *
Safety and efficacy of Relvar Ellipta in children under 12 years of age for the treatment of bronchial asthma have not been established.
Data are lacking.
- COPD *
One inhalation of Relvar Ellipta 92/22 mcg once daily.
Relvar Ellipta 184/22 mcg is not indicated for patients with COPD. There is no additional benefit from the 184/22 mcg dose compared to the 92/22 mcg dose, and there is a potential increased risk of pneumonia and systemic corticosteroid-related adverse reactions (see sections "Special Warnings and Precautions" and "Adverse Reactions").
Patients usually experience improvement in lung function within 16–17 minutes after inhalation of Relvar Ellipta.
- Children *
There are no adequate data on the use of Relvar Ellipta in children for the treatment of COPD.
Special Patient Groups
- Elderly patients (>65 years) *
No dose adjustment is necessary for this population (see section "Pharmacokinetics").
- Patients with renal impairment *
No dose adjustment is necessary for this population (see section "Pharmacokinetics").
- Patients with hepatic impairment *
Studies in patients with mild, moderate, and severe hepatic impairment showed increased systemic exposure to fluticasone furoate (Cmax and AUC) (see section "Pharmacokinetics").
The drug should be used with caution in patients with hepatic impairment, as they may be at greater risk of systemic adverse reactions associated with corticosteroids.
For patients with moderate or severe hepatic impairment, the maximum dose is 92/22 mcg (see section "Special Warnings and Precautions").
Method of Administration
Relvar Ellipta is intended for inhalation only.
It should be used at the same time each day.
The final decision regarding evening or morning administration should be left to the physician’s discretion.
If a dose is missed, the next dose should be taken at the usual time the following day.
If the medication has been stored in the refrigerator, the inhaler should be allowed to reach room temperature for at least one hour before use.
After inhalation, patients should rinse their mouth with water without swallowing it.
If the inhaler is used for the first time, there is no need to test its function or prepare it in any special way. The step-by-step instructions should be followed.
The Ellipta inhaler is packaged in a tray containing a desiccant sachet to reduce moisture content. After opening, the desiccant sachet should be discarded.
When the inhaler is removed from the tray, it will be in the closed position. Patients should be informed not to open the tray containing the inhaler until they are ready to inhale a dose.
The patient must enter the end-use date in the designated space marked “Do not use after:”. The end-use date is 6 weeks from the date the tray is opened. The inhaler must not be used after the end-use date. The tray may be discarded after first opening.
The step-by-step instructions below for the Ellipta inhaler containing 30 doses also apply to the Ellipta inhaler containing 14 doses.
Instructions for Use of the Inhaler (Fig. 1)
- Read before first use
If the inhaler cap is opened and closed without inhaling the medication, the dose will be lost. The lost dose will remain securely in the inhaler but will no longer be available for inhalation.
Accidental administration of an excessive or double dose in a single inhalation is not possible.
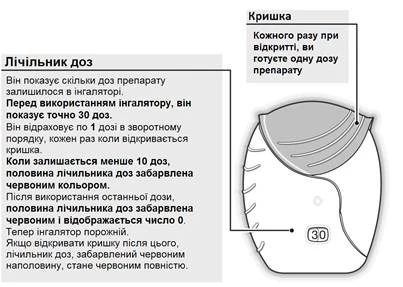
Fig. 1
- How to prepare a dose
Open the cap when ready to take a dose. Do not shake the inhaler.
Pull the cap down until you hear a click (Fig. 2).
The medication is now ready for inhalation. The dose counter will count down by one to confirm use.
If the dose counter does not count down after you hear the click, the inhaler is not working. Return it to the pharmacist for advice.
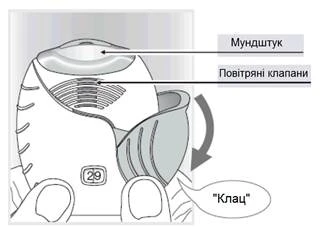
Fig. 2
- How to inhale the medication
Hold the inhaler away from the mouth and breathe out gently.
Do not breathe out into the inhaler.
Place the mouthpiece between the lips and close the lips tightly around it (Fig. 3).
Do not block the air vents with fingers.
Take one long, steady, deep breath in. Hold the breath as long as possible (at least 3–4 seconds).
- Remove the inhaler from the mouth.
- Breathe out slowly and gently.
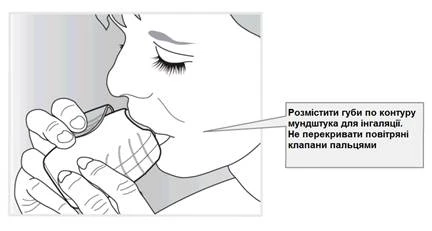
Fig. 3
You may not taste or feel the medication, even when the inhaler is used correctly.
- Close the inhaler and rinse the mouth
If cleaning of the mouthpiece is needed, use a dry cloth before closing the cap.
Pull the cap up until it stops to close the mouthpiece (Fig. 4).
Rinse the mouth with water after using the inhaler. This will reduce the likelihood of oral and throat discomfort as side effects.
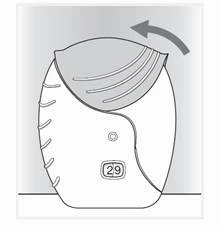
Fig. 4
- Children *
Safety and efficacy of Relvar Ellipta in children under 12 years of age for the treatment of bronchial asthma have not been established. Data are lacking.
The medication is not intended for use in children (under 18 years of age) for the treatment of COPD.
Overdose.
Symptoms and Signs
Overdose of fluticasone furoate/vilanterol may cause symptoms related to the effects of individual components, including those observed with beta2-agonist overdose and consistent with the known effects of the class of inhaled medications (see section "Special Warnings and Precautions").
Treatment
There is no specific antidote for overdose with fluticasone furoate/vilanterol. In case of overdose, supportive therapy with appropriate monitoring should be administered as necessary.
Cardioselective beta-blockade should be considered only in cases of severe vilanterol overdose causing clinical concern and unresponsive to supportive measures. Cardioselective beta-blockers should be used with caution in patients with a history of bronchospasm.
Further management should be based on clinical indications.
Adverse Reactions
Overview of Safety Profile
Data from large clinical trials in asthma and COPD were used to determine the frequency of adverse reactions associated with fluticasone furoate/vilanterol. A total of 7034 patients were included in the integrated safety assessment program for clinical studies in asthma. A total of 6237 patients were included in the integrated safety assessment program for clinical studies in COPD.
The most commonly reported adverse reactions with fluticasone furoate and vilanterol were headache and nasopharyngitis. With the exception of pneumonia and fractures, the safety profile was similar in patients with asthma and COPD. During clinical trials, pneumonia and fractures were observed more frequently in patients with COPD.
The table below lists adverse reactions by system organ class and frequency.
Classification of frequency of adverse reactions:
very common ≥ 1/10;
common ≥ 1/100 to < 1/10;
uncommon ≥ 1/1000 to < 1/100;
rare ≥ 1/10000 to < 1/1000;
very rare < 1/10000.
Within each frequency group, adverse reactions are listed in order of decreasing severity.
| System organ classes |
Adverse reaction |
Frequency |
| Infections and infestations |
Pneumonia*, upper respiratory tract infection, bronchitis, influenza, oral and pharyngeal candidiasis |
Common |
| Immune system disorders |
Hypersensitivity reactions, including anaphylaxis, angioedema, rash, urticaria |
Uncommon |
| Metabolism and nutrition disorders |
Hyperglycemia |
Uncommon |
| Psychiatric disorders |
Anxiety |
Uncommon |
| Nervous system disorders |
Headache Tremor |
Very common Uncommon |
| Eye disorders |
Blurred vision |
Uncommon |
| Cardiac disorders |
Extrasystoles Palpitations Tachycardia |
Uncommon Uncommon Uncommon |
| Respiratory, thoracic and mediastinal disorders |
Nasopharyngitis Paradoxical bronchospasm Oropharyngeal pain, sinusitis, pharyngitis, rhinitis, cough, dysphonia |
Very common Uncommon Common |
| Gastrointestinal disorders |
Abdominal pain |
Common |
| Musculoskeletal and connective tissue disorders |
Joint pain, back pain, fractures**, muscle spasms |
Common |
| General disorders and administration site conditions |
Pyrexia |
Common |
*, ** See below «Specific adverse reactions»
Specific adverse reactions
Pneumonia
In an integrated analysis of two replicate one-year studies in patients with COPD and a history of exacerbation in the previous year (n = 3255), the rate of pneumonia per 1000 patient-years was 97.9 with fluticasone furoate/vilanterol 184/22, 85.7 with fluticasone furoate/vilanterol 92/22, and 42.3 with vilanterol 22. The rate of severe pneumonia per 1000 patient-years was 33.6, 35.5, and 7.6, respectively, while the rate of serious pneumonia per 1000 patient-years was 35.1 with fluticasone furoate/vilanterol 184/22, 42.9 with fluticasone furoate/vilanterol 92/22, and 12.1 with vilanterol 22. The exposure-adjusted rate of fatal pneumonia cases was 8.8 with fluticasone furoate/vilanterol 184/22 compared to 1.5 with fluticasone furoate/vilanterol 92/22 and 0 with vilanterol 22.
In an integrated analysis of 11 studies in patients with asthma (7034 patients), the incidence rate of pneumonia per 1000 patient-years was 18.4 with fluticasone furoate/vilanterol 184/22 compared to 9.6 with fluticasone furoate/vilanterol 92/22 and 8.0 in the placebo group.
Fractures
In two replicate 12-month studies involving a total of 3255 patients with COPD, the overall incidence of bone fractures was low in all treatment groups, with a higher incidence in the Relvar Ellipta treatment groups (2%) compared to the vilanterol 22 mcg group (< 1%). Although there were more fractures in the Relvar™ Ellipta groups compared to the vilanterol 22 mcg group, fractures typically associated with corticosteroid use (e.g., spinal compression fractures/thoracolumbar spine fractures, femoral fractures, and acetabular fractures) occurred in < 1% of patients in both the Relvar Ellipta and vilanterol treatment groups.
In an integrated analysis of 11 studies in patients with asthma (7034 patients), the incidence of fractures was < 1% and these were generally associated with trauma.
Reporting of suspected adverse reactions
Reporting suspected adverse reactions after marketing authorization is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals and patients can report suspected adverse reactions to GlaxoSmithKline Pharmaceuticals Ukraine LLC via the 24-hour hotline (044) 585-51-85 or by email at [email protected].
Shelf life. 2 years.
Shelf life after opening the tray – 6 weeks.
Storage conditions.
Store at temperatures not exceeding 25°C. Keep out of the reach of children.
Store in the original packaging to protect from moisture.
Use within 6 weeks after opening the tray.
The patient must record the final date on the designated space provided, after which the inhaler should be discarded. The date should be recorded immediately after removing the inhaler from the tray.
Packaging.
14 or 30 doses in a powder inhaler, 1 inhaler per cardboard box.
Prescription status. Prescription only.
Manufacturer.
Glaxo Operations UK Ltd, United Kingdom / Glaxo Operations UK Ltd, United Kingdom.
Manufacturer's address and place of business.
Glaxo Operations UK Ltd, Priory Street, Ware, SG12 0DJ, United Kingdom / Glaxo Operations UK Ltd, Priory Street, Ware, SG12 0DJ, United Kingdom.