Polaring
Ukraine
Table of Contents
INSTRUCTIONS for medical use of the medicinal product PolaRing (PolaRing)
Composition:
Active substances: etonogestrel, ethinylestradiol;
1 vaginal delivery system contains 11.0 mg etonogestrel and 3.474 mg ethinylestradiol;
Excipients: ethylene vinyl acetate copolymer (28% vinyl acetate), polyurethane.
Dosage form. Vaginal delivery system.
Main physicochemical characteristics: flexible, transparent, colorless or almost colorless ring with an outer diameter of 54 mm. The diameter of the cross-section of the vaginal delivery system is 4 mm.
Pharmacotherapeutic group. Local contraceptives. Vaginal ring containing a progestogen and an estrogen.
ATC code G02BB01.
Pharmacological Properties
Pharmacodynamics
Mechanism of Action
NuvaRing contains etonogestrel and ethinyl estradiol.
Etonogestrel is a progestogen derived from 19-nortestosterone that binds with high affinity to progesterone receptors in target organs.
Ethinyl estradiol is an estrogen widely used in contraceptive preparations. The contraceptive effect of the vaginal delivery system is based on several mechanisms, the most important of which is inhibition of ovulation.
Efficacy and Safety
Clinical studies were conducted in various countries worldwide (the United States, European Union countries, and Brazil) involving women aged 18 to 40 years. The contraceptive efficacy was at least comparable to that of combined oral contraceptives.
Table 1 shows the Pearl Index (number of pregnancies per 100 woman-years of use) obtained during clinical studies of the vaginal delivery system.
Table 1
| Method of analysis |
Pearl Index |
95% CI [confidence interval] |
Number of cycles |
| ITT (users + method failure cases) |
0.96 |
0.64 – 1.39 |
37,977 |
| PP (method failure only) |
0.64 |
0.35 – 1.07 |
28,723 |
When higher doses of COCs (combined oral contraceptives) (0.05 mg ethinyl estradiol) are used, the risk of developing endometrial and ovarian cancer is reduced. It remains to be determined whether these benefits also apply to such low-dose hormonal contraceptives as vaginal delivery systems.
Bleeding pattern
According to data from a comparative clinical study on the effect of the vaginal delivery system (n = 512) on menstrual bleeding pattern over 13 cycles, the frequency of spotting or breakthrough bleeding in the vaginal delivery system group (2.0–6.4%) was significantly lower than with combined oral contraceptives (COCs) containing 150/30 µg levonorgestrel/ethinyl estradiol (n = 518). In most women (58.8–72.8%), vaginal bleeding was limited to the period when the vaginal delivery system was not in use.
Effect on bone mineral density
The effect of the vaginal delivery system (n = 76) on bone mineral density was studied in comparison with a non-hormonal intrauterine device (n = 31) in women over two years. No adverse effect on bone tissue with use of the medicinal product PolaRing was observed.
Children
The safety and efficacy of the vaginal delivery system in adolescent girls (under 18 years of age) have not been studied.
Pharmacokinetics
Etonogestrel
Absorption. Etonogestrel released from the vaginal delivery system ring is rapidly absorbed through the vaginal mucosa. Maximum plasma concentration of etonogestrel (approximately 1700 pg/mL) is reached about one week after insertion of the ring. This serum concentration fluctuates slightly and slowly decreases to 1600 pg/mL after 1 week, 1500 pg/mL after 2 weeks, and 1400 pg/mL after 3 weeks. Absolute bioavailability is approximately 100%, which is higher than with oral contraceptives. Etonogestrel levels in the cervix and within the uterus during use of the vaginal delivery system were similar to etonogestrel levels observed with an oral contraceptive containing 0.150 mg desogestrel and 0.020 mg ethinyl estradiol.
Distribution. Etonogestrel binds to serum albumin and sex hormone-binding globulin. The volume of distribution of etonogestrel is 2.3 L/kg.
Metabolism. Etonogestrel is metabolized via known steroid metabolic pathways. The elimination rate of metabolites from plasma is approximately 3.5 L/h. No interaction between etonogestrel and co-administered ethinyl estradiol has been observed.
Elimination. Plasma concentration of etonogestrel decreases in two phases. The terminal elimination phase is characterized by a half-life of approximately 29 hours. Etonogestrel and its metabolites are excreted in urine and bile in a ratio of approximately 1.7:1. The half-life of metabolites is approximately 6 days.
Ethinyl estradiol
Absorption. Ethinyl estradiol released from the vaginal delivery system ring is rapidly absorbed through the vaginal mucosa. Maximum serum concentration (approximately 35 pg/mL) is reached within about 3 days after ring insertion and decreases to 19 pg/mL after 1 week, 18 pg/mL after 2 weeks, and 18 pg/mL after 3 weeks of use. Monthly systemic exposure to ethinyl estradiol (AUC0–∞) from the vaginal delivery system is 10.9 ng×h/mL. Absolute bioavailability is approximately 56%, corresponding to the bioavailability observed with oral administration of ethinyl estradiol. Ethinyl estradiol levels in the cervix and within the uterus during use of the vaginal delivery system were similar to ethinyl estradiol levels observed with an oral contraceptive containing 0.150 mg desogestrel and 0.020 mg ethinyl estradiol.
Distribution. Ethinyl estradiol binds non-specifically to serum albumin. The volume of distribution is approximately 15 L/kg.
Metabolism. Ethinyl estradiol is primarily metabolized via aromatic hydroxylation, forming various hydroxylated and methylated metabolites. These metabolites are present both in free form and as glucuronide and sulfate conjugates. Effective clearance is approximately 35 L/h.
Elimination. Plasma levels of ethinyl estradiol decrease in two phases. The terminal elimination phase shows considerable inter-individual variation in half-life; the mean elimination half-life is approximately 34 hours. Ethinyl estradiol is not excreted unchanged; elimination of ethinyl estradiol metabolites occurs via urine and bile in a ratio of 1.3:1. The half-life of metabolites is approximately 1.5 days.
Special populations
Children. The pharmacokinetics of the vaginal delivery system in healthy adolescent girls under 18 years of age who have reached menarche have not been studied.
Renal impairment. Studies on the effect of renal disease on the pharmacokinetics of the vaginal delivery system have not been conducted.
Hepatic impairment. Studies on the effect of liver disease on the pharmacokinetics of the vaginal delivery system have not been conducted. However, it should be considered that metabolism of steroid hormones may be altered in hepatic impairment.
Ethnic groups. Formal studies to evaluate pharmacokinetics in ethnic groups have not been conducted.
Clinical characteristics
Indications
Prevention of pregnancy (contraception).
The medicinal product PolaRing is indicated for use in women of reproductive age. Safety and efficacy have been established in women aged 18 to 40 years.
When considering the prescription of PolaRing, individual risks in each woman should be taken into account, especially the risk of venous thromboembolism (VTE), as well as the risk of VTE associated with the use of PolaRing and other combined hormonal contraceptives (see sections "Contraindications" and "Special precautions").
Contraindications
Combined hormonal contraceptives (CHCs) must not be used if any of the conditions listed below are present.
Presence or risk of venous thromboembolism (VTE).
- Venous thromboembolism — current VTE (under anticoagulant treatment) or history of VTE [e.g., deep vein thrombosis (DVT) or pulmonary embolism (PE)].
- Known acquired or hereditary predisposition to venous thromboembolism, such as activated protein C resistance (including factor V Leiden), antithrombin III deficiency, protein C deficiency, protein S deficiency.
- Major surgery with prolonged immobilization (see section "Special precautions").
- High risk of venous thromboembolism due to the presence of multiple risk factors (see section "Special precautions").
Presence or risk of arterial thromboembolism (ATE).
-
Arterial thromboembolism — current or past history of arterial thromboembolism (e.g., myocardial infarction) or prodromal conditions (e.g., angina pectoris).
-
Cerebrovascular disease — history of stroke, past stroke, or prodromal conditions (e.g., transient ischemic attack).
-
Hereditary or acquired predisposition to arterial thromboembolism, e.g., hyperhomocysteinemia and antiphospholipid antibodies (anticardiolipin antibodies, lupus anticoagulant).
-
History of migraine with focal neurological symptoms.
-
High risk of arterial thromboembolism due to the presence of multiple risk factors or one serious risk factor (see section "Special precautions"):
-
diabetes mellitus with vascular complications;
-
severe arterial hypertension;
-
severe dyslipoproteinemia.
-
Pancreatitis or history of pancreatitis associated with severe hypertriglyceridemia.
-
Severe liver disease (until liver function tests return to normal values).
-
Current or past history of benign or malignant liver tumors.
-
Confirmed or suspected hormonally-dependent malignant tumors of the genital organs or breasts.
-
Vaginal bleeding of unknown etiology.
-
Hypersensitivity to the active substances or to any component of the medicinal product PolaRing (see section "Composition").
PolaRing is contraindicated for use with the combined hepatitis C virus (HCV) treatment regimen containing ombitasvir/paritaprevir/ritonavir, with or without dasabuvir, or with products containing glecaprevir/pibrentasvir (see sections "Special precautions" and "Interaction with other medicinal products and other forms of interaction").
Interaction with other medicinal products and other forms of interaction
Note: The package leaflet of the concomitant medicinal product should be carefully reviewed to identify potential interactions. Interactions between contraceptives and other medicinal products that induce microsomal enzymes may lead to increased clearance of sex hormones and breakthrough bleeding or contraceptive failure.
Course monitoring
Enzyme induction may occur within a few days of treatment. Maximum enzyme induction is usually observed within several weeks. After discontinuation of the medicinal product, enzyme induction may persist for approximately 4 weeks.
Short-term treatment
Women taking any medicinal or herbal products that induce liver enzymes should be aware that the effectiveness of PolaRing may be reduced. Note: PolaRing must not be used together with a diaphragm, cervical cap, or female condom.
A barrier method of contraception should be used in addition to PolaRing during concomitant use of liver enzyme-inducing agents, and for 28 days after discontinuation of such treatment. If the duration of concomitant treatment extends beyond 3 weeks of ring use, the next ring should be inserted without the usual break.
Long-term treatment
Women undergoing long-term treatment with substances that induce liver enzymes are recommended to use another reliable non-hormonal method of contraception.
The following interactions have been reported in scientific publications.
Substances that increase the elimination of combined hormonal contraceptives
Interactions may occur with medicinal products or herbal preparations that induce microsomal enzymes, particularly CYP450 (CYP) enzymes, leading to increased clearance of sex hormones and potentially reducing the effectiveness of combined oral contraceptives, including PolaRing. Such agents include phenytoin, phenobarbital, primidone, bosentan, carbamazepine, rifampicin, and possibly oxcarbazepine, topiramate, felbamate, griseofulvin, certain HIV protease inhibitors (e.g., ritonavir), non-nucleoside reverse transcriptase inhibitors (e.g., efavirenz), and herbal preparations containing St. John's wort (Hypericum perforatum).
Substances with variable effects on elimination of combined hormonal contraceptives
Concomitant use of hormonal contraceptives with many combinations of HIV protease inhibitors (e.g., nelfinavir) and non-nucleoside reverse transcriptase inhibitors (e.g., nevirapine) and/or combinations with hepatitis C virus (HCV) treatment agents (e.g., boceprevir, telaprevir) may increase or decrease plasma concentrations of progestins, including etonogestrel, or estrogens. The clinical significance of these changes may be relevant in some cases.
Substances that reduce the elimination of combined hormonal contraceptives
The clinical significance of potential interactions with enzyme inhibitors remains unknown.
Concomitant use with strong (e.g., ketoconazole, itraconazole, clarithromycin) or moderate (e.g., fluconazole, diltiazem, erythromycin) CYP3A4 inhibitors may lead to increased serum concentrations of estrogens and progestins, including etonogestrel.
There have been reports of ring rupture with concomitant use of intravaginal products, including antifungal agents, antibiotics, and lubricants (see section "Special precautions").
Based on pharmacokinetic data, intravaginally administered antifungal agents and spermicides are unlikely to affect the contraceptive efficacy and safety of PolaRing.
Hormonal contraceptives may affect the metabolism of other medicinal products. Consequently, plasma and tissue concentrations of such drugs may be increased (e.g., cyclosporine) or decreased (e.g., lamotrigine).
Pharmacodynamic interaction
Concomitant use with medicinal products containing ombitasvir/paritaprevir/ritonavir and dasabuvir, with or without ribavirin, or glecaprevir/pibrentasvir increases the risk of elevated alanine aminotransferase (ALT) levels (see sections "Contraindications" and "Special precautions"). Therefore, an alternative method of contraception (e.g., progestogen-only contraception or non-hormonal methods) should be considered prior to initiating such combination therapy. Resumption of PolaRing should occur approximately 2 weeks after completion of the combination treatment.
Laboratory tests
The use of contraceptive steroids may affect the results of certain laboratory tests, including biochemical parameters of liver, thyroid, adrenal, and kidney function, plasma protein levels (e.g., corticosteroid-binding globulin and sex hormone-binding globulin), lipid and lipoprotein fractions, carbohydrate metabolism, and coagulation and fibrinolysis parameters. These changes are usually within normal laboratory ranges.
Interaction with tampons
Pharmacokinetic data indicate that the use of tampons does not affect the systemic absorption of hormones released by PolaRing. In isolated cases, PolaRing may be expelled during tampon removal (see section "Special precautions").
Special precautions for use
If any of the conditions/factors listed below are present, the benefits and risks of prescribing the medicinal product PolaRing should be carefully weighed for each individual woman, and these should be discussed with her. In case of exacerbation, worsening, or new onset of any of these conditions, the woman should consult her physician. The physician will determine whether treatment with PolaRing should be discontinued.
Disorders of blood circulation
Risk of venous thromboembolism (VTE)
- Use of any combined oral contraceptive (COC) increases the risk of venous thromboembolism (compared to the risk when COCs are not used). Preparations containing levonorgestrel, norgestimate, or norethisterone are associated with the lowest risk of VTE. Other preparations, such as PolaRing, may increase the risk by up to 2 times. The decision to prescribe any contraceptive that is not a low-VTE-risk preparation should only be made after discussing with the woman and informing her about the risks of VTE associated with the use of PolaRing, how her individual risk factors may influence this risk, and that the risk of VTE is highest during the first year of use of the medicinal product. The risk also increases when restarting COC use after a break of 4 weeks or more.
- Among women who do not use COCs and are not pregnant, approximately 2 out of 10,000 will develop VTE within one year. However, for any individual woman, the risk may be significantly higher depending on underlying risk factors.
- Among 10,000 women using a low-dose COC containing levonorgestrel, approximately 6[1] will develop VTE within one year. Conflicting data exist regarding the incidence of VTE with PolaRing compared to COCs containing levonorgestrel (relative risk estimates range from no increase in risk, RR = 0.96, to a doubling of risk, RR = 1.90): from 6 to 12 cases of VTE per year per 10,000 women using PolaRing.
- In both of the above-mentioned cases, the number of annual VTE events is lower than the expected number in pregnant women and during the postpartum period.
- VTE can be fatal in 1–2% of cases.
Number of VTE cases per 10,000 women per year
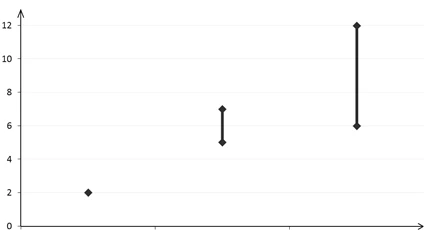
Patients not using COCs COCs containing levonorgestrel COCs containing etonogestrel
(2 cases) (5–7 cases) (6–12 cases)
- Very rarely, thrombosis has been reported in other blood vessels, such as hepatic, mesenteric, renal, cerebral, or retinal veins and arteries, in women using COCs.
Risk factors for VTE
- The risk of VTE complications with COC use is substantially increased in women with additional risk factors, especially when multiple risk factors are present (see Table 2).
- The medicinal product PolaRing is contraindicated in women with multiple risk factors for venous thrombosis (see section "Contraindications"). If a woman has several risk factors, the overall risk may be greater than the sum of individual risk factors. In such cases, the overall risk of VTE in the woman should be carefully evaluated. If the benefit-risk ratio is unfavorable, COCs should not be prescribed (see section "Contraindications").
Table 2
VTE risk factors
| Risk factor |
Comment |
| Obesity (body mass index (BMI) greater than 30 kg/m²). |
Risk increases significantly with increasing BMI. It is particularly important to consider the presence of other risk factors. |
| Long-term immobilization, major surgery, any surgery on legs or pelvic organs, neurosurgery, major trauma. Note: temporary immobilization, particularly air travel lasting more than 4 hours, may also be a risk factor for VTE, especially in women with other risk factors. |
In such situations, it is recommended to discontinue use of the ring (in case of elective surgery — at least 4 weeks prior) and not resume earlier than 2 weeks after full restoration of mobility. Alternative contraceptive methods should be used to prevent pregnancy. Antithrombotic therapy should be considered if use of the medicinal product PolaRing was not discontinued in advance. |
| Family history (venous thromboembolism in siblings or parents, especially at a relatively young age, i.e., before 50 years). |
If inherited predisposition is suspected, the woman should be referred to a specialist prior to deciding on use of COCs. |
| Other medical conditions associated with VTE. |
Cancer, systemic lupus erythematosus, hemolytic uremic syndrome, chronic inflammatory bowel disease (Crohn's disease or ulcerative colitis), and sickle cell anemia. |
| Age |
Especially after age 35. |
-
There is no consensus regarding the possible role of varicose veins and superficial thrombophlebitis in the development or progression of venous thrombosis.
-
The increased risk of thromboembolism during pregnancy should be taken into account, especially within the first 6 weeks postpartum (see section "Use during pregnancy or breastfeeding").
Symptoms of VTE (deep vein thrombosis and pulmonary embolism)
If any symptoms occur, women should seek immediate medical attention and inform their doctor that they are taking COCs.
Symptoms of deep vein thrombosis (DVT) include:
- Unilateral swelling of the leg and/or foot or swelling along the vein;
- Pain or tenderness in the leg, which may only be felt while standing or walking;
- Increased warmth in the affected limb;
- Redness or discoloration of the skin on the leg.
Symptoms of pulmonary embolism (PE) include:
- Sudden shortness of breath or rapid breathing;
- Sudden cough, which may be accompanied by hemoptysis (coughing up blood);
- Acute chest pain;
- Severe dizziness or vertigo;
- Rapid or irregular heartbeat.
Some of these symptoms (e.g., shortness of breath, cough) are non-specific and may be misinterpreted as common or less serious conditions (e.g., respiratory tract infection).
Other signs of vascular occlusion may include: sudden pain, swelling, and a slightly bluish discoloration of the skin of a limb.
If occlusion of ocular vessels occurs, symptoms may range from painful blurred vision to sudden vision loss. In some cases, vision loss may occur almost immediately.
Arterial thromboembolism (ATE) risk
Epidemiological studies have shown an association between the use of COCs and an increased risk of arterial thromboembolism (myocardial infarction) or cerebrovascular events (e.g., transient ischemic attack, stroke). Arterial thromboembolic events can be fatal.
ATE risk factors
The risk of developing arterial thromboembolic complications or cerebrovascular events while using COCs is increased in women with risk factors (see Table 3). The medicinal product PolaRing is contraindicated in women with one major or multiple risk factors that lead to a high risk of arterial thrombosis (see section "Contraindications"). If a woman has multiple risk factors, the overall risk may be greater than the sum of the individual risk factors. In such cases, the overall risk for the individual woman should be carefully considered. If the benefit-risk balance is considered unfavorable, COCs should not be prescribed (see section "Contraindications").
Table 3
ATE risk factors
| Risk factor |
Comment |
| Age |
Especially after 35 years of age. |
| Smoking |
Women are advised to stop smoking while using COCs. Women over 35 years of age who continue to smoke are strongly advised to use another method of contraception. |
| Arterial hypertension. |
|
| Obesity (body mass index greater than 30 kg/m²). |
Risk increases significantly with increasing BMI. It is especially important to consider the presence of other risk factors. |
| Family history (arterial thromboembolism in a brother/sister or parents, especially at a relatively young age, i.e. before 50 years). |
If inherited predisposition is suspected, the woman should be referred for consultation with a specialist before deciding on the use of COCs. |
| Migraine |
Increased frequency or severity of migraine during COC use (which may be a prodromal symptom of cerebrovascular disorder) may require immediate discontinuation of the medicinal product. |
| Other medical conditions associated with vascular side effects. |
Diabetes mellitus, hyperhomocysteinemia, heart valve disorders, atrial fibrillation, dyslipoproteinemia, and systemic lupus erythematosus. |
ATE Symptoms
If ATE symptoms occur, a woman should seek immediate medical attention and inform her doctor that she is taking COCs.
Symptoms of cerebrovascular disorders may include:
- sudden numbness or weakness of the face, arm, or leg, especially on one side of the body;
- sudden difficulty walking, dizziness, loss of balance or coordination;
- sudden confusion, trouble speaking or understanding speech;
- sudden vision problems in one or both eyes;
- sudden severe or prolonged headache with no known cause;
- loss of consciousness or fainting, with or without seizures.
Transient symptoms may indicate a transient ischemic attack (TIA).
Symptoms of myocardial infarction may include:
- chest pain, discomfort, pressure, heaviness, squeezing, or fullness in the chest, arm, or below the sternum;
- discomfort radiating to the back, jaw, throat, arm, or stomach;
- feeling of stomach fullness, indigestion, or constipation;
- sweating, nausea, vomiting, or dizziness;
- unusual weakness, anxiety, or shortness of breath;
- rapid or irregular heartbeat.
If VTE or ATE is suspected or confirmed, COC use should be discontinued. An appropriate contraceptive method should be prescribed, considering the teratogenicity of anticoagulant therapy (coumarins).
Tumors
Epidemiological studies have shown that long-term use of COCs increases the risk of cervical cancer in women infected with human papillomavirus (HPV). However, uncertainty remains regarding the extent to which this disease is influenced by confounding factors such as the number of sexual partners or use of barrier contraceptives. Epidemiological data on the risk of cervical cancer in women using PolaRing are lacking (see below, "Medical examination/consultation").
A meta-analysis of 54 epidemiological studies revealed a slightly increased relative risk (RR = 1.24) of breast cancer diagnosed in women using COCs. This risk gradually disappears within 10 years after discontinuation of COCs. Since breast cancer is rare in women under 40 years of age, the increase in the incidence of diagnosed breast cancer among women currently or recently using COCs is small compared to the overall risk of developing breast cancer. Breast cancers diagnosed in women who have ever used COCs are generally less advanced than clinically diagnosed cases in women who have never used COCs.
Another epidemiological study among 1.8 million Danish women, followed for a mean of 10.9 years, reported that the relative risk (RR) of diagnosed breast cancer increases with longer duration of COC use compared to women who have never used COCs (overall RR = 1.19; RR ranged from 1.17 for 1–5 years of COC use to 1.46 for more than 10 years of COC use). The known absolute difference in RR (number of breast cancer cases in women who have never used COCs compared to those currently using or who recently discontinued COCs) was small: 13 per 100,000 woman-years.
Epidemiological studies do not provide evidence of a causal relationship for these observations. The observed pattern of increased risk may be related to earlier diagnosis of breast cancer in COC users, the biological effects of COCs, or a combination of both factors.
In rare cases, benign liver tumors and even more rarely, malignant liver tumors, have been reported in COC users. In individual cases, these tumors have led to life-threatening intra-abdominal hemorrhage. Therefore, liver tumor should be considered in the differential diagnosis if women using PolaRing report severe upper abdominal pain, have hepatomegaly, or signs of intra-abdominal bleeding.
Hypersensitivity reactions
Hypersensitivity reactions, including angioedema and anaphylaxis, have been reported during use of PolaRing. If angioedema and/or anaphylaxis is suspected, PolaRing should be discontinued and appropriate treatment initiated.
Elevated ALT levels
During clinical trials of a combined hepatitis C virus treatment regimen including ombitasvir/paritaprevir/ritonavir, with or without dasabuvir, ALT elevations greater than 5 times the upper limit of normal (ULN) were significantly more frequent in women using ethinylestradiol-containing products (COCs). ALT elevations have also been observed in women using ethinylestradiol (COCs) when co-administered with glecaprevir/pibrentasvir.
Other conditions
- Women with hypertriglyceridemia or a family history of hypertriglyceridemia have an increased risk of pancreatitis when using hormonal contraceptives.
- Although a slight increase in blood pressure has been observed in many women using hormonal contraceptives, clinically significant increases are rare. A definitive link between hormonal contraceptive use and clinical hypertension has not been established. However, if persistent clinically significant hypertension occurs during use of PolaRing, the physician should discontinue the use of the ring and initiate antihypertensive therapy. If appropriate, PolaRing use may be resumed once blood pressure has normalized with antihypertensive treatment.
- The following conditions have been reported to occur or worsen during pregnancy or with use of hormonal contraceptives, but convincing evidence of a causal link with hormonal contraceptives is lacking: cholestasis-related jaundice and/or pruritus; gallbladder stone formation; porphyria; systemic lupus erythematosus; hemolytic uremic syndrome; Sydenham's chorea; herpes gestationis; hearing loss associated with otosclerosis.
- Exogenous estrogens may induce or exacerbate symptoms of hereditary or acquired angioedema.
- Acute or chronic liver dysfunction may require discontinuation of PolaRing until liver function tests normalize. Recurrence of cholestatic jaundice and/or cholestasis-related pruritus, first observed during pregnancy or prior use of sex hormones, necessitates discontinuation of the ring.
- Although estrogens and progestogens may affect peripheral insulin resistance and glucose tolerance, there is no evidence that the therapeutic regimen needs to be changed in diabetics using hormonal contraception. However, women with diabetes should be closely monitored during use of PolaRing, especially during the first months.
- Crohn's disease and ulcerative colitis have been reported in association with use of hormonal contraceptives.
- Chloasma may occasionally occur, particularly in women with a history of chloasma of pregnancy. Women prone to chloasma should avoid sun exposure or ultraviolet radiation during use of PolaRing.
- Women with any of the following conditions may be unable to properly insert PolaRing or may actually lose the ring: uterine prolapse, cystocele and/or rectocele, severe or chronic constipation.
Very rarely, accidental insertion of PolaRing into the urethra and possibly into the bladder has been reported. Therefore, incorrect placement of the ring should be considered in the differential diagnosis of cystitis symptoms.
- Vaginitis may occur occasionally during use of PolaRing. There is no evidence that treatment of vaginitis affects the efficacy of PolaRing or that PolaRing affects the treatment of vaginitis (see section "Interaction with other medicinal products and other forms of interaction").
- Occasionally, adhesion of the ring to vaginal tissue has been reported, requiring medical intervention. In some cases where the ring became embedded in vaginal tissue, it could be removed by cutting the ring without tissue incision.
- Amenorrhea or oligomenorrhea may occur in some women after discontinuation of COCs, especially if the condition existed previously.
- Some women using PolaRing have reported developing toxic shock syndrome (TSS). TSS is associated with tampon use and certain barrier contraceptives. In particular, some women using PolaRing also used tampons. A causal relationship between PolaRing use and TSS has not been established. If a patient develops signs or symptoms of TSS, this diagnosis should be considered and appropriate medical evaluation and treatment initiated.
- Women with a history of depression should discontinue use of the medicinal product if depression worsens.
Medical examination/consultation
Before initiating or resuming use of PolaRing, the physician should carefully review the woman's medical and family history and exclude pregnancy. Blood pressure should be measured and a medical examination performed, considering contraindications and warnings (see sections "Contraindications" and "Special precautions for use"). The woman should be informed about venous and arterial thrombosis, including information on risks associated with PolaRing compared to other COCs, symptoms of VTE and ATE, known risk factors, and actions to take if thrombosis is suspected.
Women are advised to carefully read the instructions and follow the recommendations. The frequency and nature of follow-up examinations should be based on established clinical practice and individually adapted.
Women should be informed that PolaRing does not protect against HIV infection (AIDS) or other sexually transmitted diseases.
Reduced efficacy
The efficacy of PolaRing may be reduced if the recommended regimen is not followed (see section "Dosage and administration") or if used concomitantly with drugs that reduce plasma concentrations of ethinylestradiol and/or etonogestrel (see section "Interaction with other medicinal products and other forms of interaction").
Worsening menstrual cycle control
Irregular bleeding (spotting or breakthrough bleeding) may occur during use of PolaRing. If irregular bleeding occurs after previously regular cycles while using PolaRing according to the recommended regimen, non-hormonal causes should be considered and appropriate diagnostic measures taken to exclude pregnancy or malignant tumors, which may include curettage.
In some women, bleeding may not occur during the ring-free interval. If PolaRing has been used according to the recommendations in section "Dosage and administration," the likelihood of pregnancy is low. However, if PolaRing was not used according to these recommendations before the first absence of bleeding during the ring-free interval, or if bleeding is absent for two consecutive cycles, pregnancy should be excluded before continuing use of PolaRing.
Effect of ethinylestradiol and etonogestrel on men
The extent and possible pharmacological effect of ethinylestradiol and etonogestrel on male partners via absorption through the mucous membrane of the male genital organ have not been studied.
Ring damage
In very rare cases, breakage of PolaRing during use has been reported (see section "Interaction with other medicinal products and other forms of interaction"). Women are advised to remove the broken ring, insert a new ring as soon as possible, and additionally use a barrier method—male condom—for the next 7 days. Vaginal injury due to ring breakage has been reported. Pregnancy should be considered, and medical consultation sought if necessary.
Ring expulsion
Occasionally, expulsion of PolaRing from the vagina has been reported, for example due to incorrect insertion, tampon removal, during sexual intercourse, or in the context of severe or chronic constipation. If a prolonged period has passed since expulsion, this may lead to contraceptive failure and/or breakthrough bleeding. Therefore, women are advised to regularly check for the presence of PolaRing in the vagina (e.g., before and after sexual intercourse).
If the ring has been accidentally removed and remained outside the vagina for less than 3 hours, contraceptive efficacy is not reduced. In this case, the ring should be rinsed with cold or lukewarm water (not hot) and reinserted as soon as possible, but no later than 3 hours.
If the ring has been outside the vagina for more than 3 hours or if there is suspicion of this, its contraceptive efficacy may be reduced. In such cases, the instructions provided in the section "Dosage and administration. What to do if the ring has been temporarily outside the vagina?" should be followed.
Use during pregnancy or breastfeeding
Fertility
PolaRing is indicated for prevention of pregnancy. If a woman wishes to discontinue use of PolaRing to become pregnant, she is advised to wait until the onset of a normal menstrual period before attempting conception, as this will help calculate the expected date of delivery.
Pregnancy
Pregnancy is a contraindication for the use of PolaRing. If a woman becomes pregnant while the ring is in place, the ring should be removed. Extensive epidemiological studies have not shown an increased risk of congenital malformations in newborns of women who used COCs before pregnancy, nor a teratogenic effect when COCs were used accidentally during early pregnancy.
A clinical study involving a small number of women showed that, despite intravaginal administration of PolaRing, intrauterine concentrations of contraceptive steroids in women using the vaginal ring are similar to levels observed in women taking COCs (see subsection "Pharmacodynamics"). There are no clinical data on adverse outcomes of pregnancy in women who used PolaRing.
The increased risk of VTE in the postpartum period should be considered when resuming use of PolaRing (see sections "Dosage and administration" and "Special precautions for use").
Breastfeeding
Estrogens may affect lactation, as they may reduce the quantity and alter the composition of breast milk. Therefore, PolaRing is not recommended during breastfeeding until complete weaning. Small amounts of contraceptive steroids and/or their metabolites may pass into breast milk, but there is no evidence of negative effects on infant health.
Ability to affect reaction speed when driving or operating machinery. Given the pharmacodynamic properties of PolaRing, it is unlikely to affect reaction speed when driving or operating machinery.
Method of Administration and Dosage
A woman can insert the PolaRing into the vagina by herself. A healthcare provider should instruct the woman on how to insert and remove the PolaRing. To insert the ring, the woman should choose a comfortable position—such as standing with one leg raised, squatting, or lying down. The PolaRing should be squeezed and inserted into the vagina so that it settles comfortably. The exact position of the ring within the vagina is not critical for the contraceptive effectiveness of the medicinal product (see Figures 1–4).
From the moment of insertion, the ring must remain in the vagina continuously for 3 weeks. The woman is advised to regularly check the presence of the ring in the vagina (e.g., before and after sexual intercourse). If the ring is accidentally removed, see below "What to do if the ring has been out of the vagina temporarily?"
The PolaRing must be removed after 3 weeks, on the same day of the week it was inserted. After a 7-day break, a new ring should be inserted (for example: if the ring was inserted on Wednesday at 10 p.m., it should be removed on Wednesday three weeks later at 10 p.m. A new ring should be inserted one week later, the following Wednesday). The PolaRing can be removed by hooking it with the index finger or by grasping the ring between the index and middle fingers (see Figure 5). The used ring should be placed in the provided pouch (which should be stored out of reach of children and pets) and discarded with regular household waste to prevent accidental contact with others. The PolaRing must not be flushed down the toilet. Withdrawal bleeding typically begins 2–3 days after removal of the PolaRing and may continue until the next ring is inserted.
Use of the medicinal product PolaRing with other vaginal products
PolaRing may interfere with the proper placement of certain female barrier methods, such as a diaphragm, cervical cap, or female condom. These methods should not be used as additional contraceptive methods together with the medicinal product PolaRing.
Figure 1

Remove the PolaRing from the sachet
Figure 2
Squeeze the ring

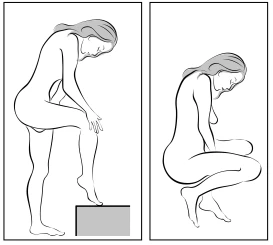
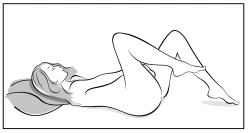
Figure 4A Figure 4B Figure 4C



With one hand, insert the ring into the vagina (Figure 4A); if necessary, use the other hand to separate the labia. Push the ring into the vagina until it is comfortably positioned (Figure 4B). Leave the ring in the vagina for 3 weeks (Figure 4C).
Figure 5

The PolaRing can be removed by hooking it with the index finger or by grasping the ring between the index and middle fingers.
How to start using the medicinal product PolaRing
If hormonal contraceptives have not been used during the previous menstrual cycle
PolaRing should ideally be inserted on the first day of the woman's natural menstrual cycle (i.e., the first day of menstrual bleeding). PolaRing may be inserted on days 2–5 of the menstrual cycle. If PolaRing is used within the first 7 days of the cycle, it is recommended to additionally use barrier contraceptive methods.
Switching from combined hormonal contraceptives (CHCs)
PolaRing should be inserted no later than the day after the tablet-free interval, patch-free interval, or placebo tablet period of the previous combined hormonal contraceptive.
If the woman has used the previous contraceptive method continuously and correctly, and if she is certain she is not pregnant, she may switch from the previous combined hormonal contraceptive on any day of the cycle.
The hormone-free interval of the previous contraceptive method should not be extended beyond the recommended duration.
Switching from progestogen-only contraceptives (mini-pill, implant, or injection) or from a progestogen-releasing intrauterine system (IUS)
A woman currently taking a mini-pill may switch to PolaRing at any time. For those using an implant or IUS, the switch should occur on the day of removal. For injectable contraception, the switch should occur on the day the next injection would have been due. However, in all these cases, the woman must use an additional barrier contraceptive method for the first 7 days.
After first-trimester abortion
A woman may start using the ring immediately after an abortion. In this case, no additional contraceptive methods are needed. If immediate use of PolaRing after abortion is not desired, the woman should follow the instructions provided in this leaflet (see above "If hormonal contraceptives have not been used during the previous menstrual cycle"). In the meantime, the woman is advised to use an alternative contraceptive method.
After childbirth or second-trimester abortion
Information for breastfeeding women is provided in the section "Use during pregnancy or breastfeeding." Women are advised to start using the ring within the fourth week after childbirth or second-trimester abortion. If starting later, it is recommended to additionally use a barrier contraceptive method for the first 7 days of PolaRing use. In any case, if sexual intercourse has already occurred during this period, pregnancy should first be ruled out or the woman should wait for the first menstruation before inserting PolaRing.
It should be remembered that there is an increased risk of venous thromboembolism (VTE) in the postpartum period when resuming use of PolaRing (see sections "Method of Administration and Dosage" and "Special Warnings and Precautions for Use").
Deviations from the recommended regimen
Contraceptive effectiveness and menstrual cycle control may be compromised if the woman does not follow the recommended regimen. To prevent reduced contraceptive efficacy in case of regimen deviations, the following instructions should be followed.
- What to do in case of a prolonged (more than 7 days) break in ring use?
The woman may insert a new ring as soon as she remembers. Additionally, a barrier contraceptive method (e.g., male condom) must be used for the first 7 days. If sexual intercourse occurred during the break in ring use, the possibility of pregnancy should be considered. The longer the break, the higher the risk of pregnancy.
- What to do if the ring has been temporarily out of the vagina?
The PolaRing must remain in the vagina continuously for 3 weeks. If the ring is accidentally removed, it can be rinsed with cold or warm (not hot) water and immediately reinserted into the vagina.
If the ring has been out of the vagina for less than 3 hours, contraceptive effectiveness is not reduced. The woman should reinsert the ring as soon as possible, but no later than 3 hours.
If the ring has been out of the vagina or there is suspicion it has been out for more than 3 hours during the first or second week of use, contraceptive effectiveness may be reduced. The woman should reinsert the ring as soon as she remembers.
A barrier contraceptive method (e.g., male condom) should be used until the PolaRing has been in the vagina continuously for 7 days. The longer the PolaRing is out of the vagina and the closer this period is to the time of ring removal, the higher the risk of pregnancy.
If the ring has been out of the vagina or there is suspicion it has been out for more than 3 hours during the third week of the 3-week use period, contraceptive effectiveness may be reduced. The woman should discard the current ring and choose one of the following two options:
- Insert a new ring immediately.
This starts the next 3-week use period. The woman may not experience the expected withdrawal bleeding from her previous cycle. However, she may experience light spotting or breakthrough bleeding.
- Allow withdrawal bleeding to occur and insert a new ring no later than 7 days (7 × 24 hours) after removal of the previous ring.
This option should only be chosen if the ring has been used continuously during the preceding 7 days.
If the ring has been out of the vagina for an unknown duration, pregnancy may have occurred. A pregnancy test should be performed before inserting a new ring.
- What to do if PolaRing has been used longer than recommended?
If PolaRing is used for up to 4 weeks maximum, its contraceptive effectiveness remains adequate. The woman may take a one-week break from ring use and then insert a new ring. If PolaRing remains in the vagina longer than 4 weeks, contraceptive efficacy may be reduced, and pregnancy should be ruled out before inserting a new ring.
If the woman does not follow the recommended regimen and does not experience bleeding during the next ring-free interval, pregnancy should be ruled out before inserting a new ring.
How to change the timing of menstruation or delay menstruation
In exceptional cases, to delay menstruation, the woman may insert a new ring without a weekly break. The new ring should also be used for 3 weeks. During this time, the woman may experience light spotting or breakthrough bleeding. Afterward, following a regular one-week break from ring use, the woman resumes regular use of PolaRing.
To change the timing of menstruation—i.e., shift its onset to a different day of the week than would occur with the usual ring insertion schedule—the woman may be advised to shorten the next ring-free interval by as many days as needed. The shorter the break, the higher the likelihood of absence of withdrawal bleeding and the occurrence of breakthrough bleeding or light spotting during use of the next ring.
Children.
The safety and efficacy of the medicinal product PolaRing in individuals under 18 years of age have not been established; therefore, PolaRing should not be used in this age group.
Overdose
No serious or life-threatening complications due to overdose of hormonal contraceptives have been reported. In case of overdose, adverse reactions such as nausea, vomiting, and vaginal bleeding in young women may occur. Treatment of overdose is symptomatic; there are no specific antidotes.
Adverse reactions
During studies, the most commonly reported adverse reactions were headache, vaginal infections, and vaginal discharge — each observed in 5–6% of women.
Use of COCs has been associated with an increased risk of arterial and venous thromboembolism, including myocardial infarction, stroke, transient ischemic attack, deep vein thrombosis, and pulmonary embolism; for more details, see section "Special precautions".
Other adverse reactions have also been reported with the use of COCs — more detailed information is provided in section "Special precautions".
The adverse reactions listed below were observed during clinical trials, observational studies, or in the post-marketing period of the medicinal product PolaRing (see Table 4). MedDRA (Medical Dictionary for Regulatory Activities) terms were used to describe adverse reactions. All adverse reactions are listed by system organ class and frequency: common (≥ 1/100, < 1/10), uncommon (≥ 1/1000, < 1/100), rare (≥ 1/10000, < 1/1000), and not known (cannot be estimated from available data).
Table 4
| System organ classes |
Common |
Uncommon |
Rare |
Not known1 |
| Infections and infestations |
Vaginal infection |
Cervicitis, cystitis, urinary tract infection |
||
| Immune system |
Hypersensitivity reactions, including angioedema and anaphylaxis Exacerbation of symptoms of hereditary and acquired angioedema |
|||
| Metabolism and nutrition disorders |
Increased appetite |
|||
| Psychiatric disorders |
Depression, decreased libido |
Mood alteration, mood swings, labile affect |
Anxiety |
|
| Nervous system |
Headache, migraine |
Dizziness, paraesthesia |
Stroke/cerebrovascular disorders |
|
| Vision |
Vision blurred |
|||
| Vascular |
Facial flushing |
Venous thromboembolism, arterial thromboembolism |
Thrombosis of large veins, exacerbation of varicose veins, myocardial infarction, vascular disorders |
|
| Gastrointestinal system |
Abdominal pain, nausea |
Abdominal distension, diarrhoea, vomiting, constipation |
Cholelithiasis, liver disease |
|
| Skin and subcutaneous tissue |
Acne |
Alopecia, eczema, pruritus, rash, urticaria |
Chloasma |
|
| Musculoskeletal and connective tissue |
Back pain, muscle cramps, limb pain |
|||
| Renal and urinary system |
Dysuria, urinary urgency, pollakiuria |
|||
| Reproductive system and breast |
Breast tenderness, genital pruritus in women, dysmenorrhoea, pelvic pain, vaginal discharge |
Amenorrhoea, breast discomfort, breast enlargement, breast mass, cervical polyp, coital bleeding, dyspareunia, ectropion of cervix, fibrocystic mastopathy, menorrhagia, metrorrhagia, pelvic discomfort, premenstrual syndrome, uterine contractions, burning sensation in vagina, unpleasant vaginal odour, vaginal pain, vulvovaginal discomfort, vulvovaginal dryness |
Galactorrhoea |
Penile reactions |
| General disorders and administration site conditions |
Fatigue, irritability, malaise, oedema, foreign body sensation |
Vaginal tissue overgrowth at site of vaginal ring |
||
| Investigations |
Weight increased |
Blood pressure increased |
||
| Injury and procedural complications |
Discomfort during ring use, expulsion of vaginal contraceptive ring |
Complications during use of contraceptive ring, damage to ring |
Vaginal injury as a result of ring rupture |
Some adverse reactions observed in women using combined hormonal contraceptives (these events are described in more detail in the section "Special Instructions"): pancreatitis, obstructive jaundice, hemolytic-uremic syndrome, decreased glucose tolerance, Sydenham's chorea, choreas, hearing loss associated with otosclerosis, jaundice and/or pruritus associated with cholestasis, Crohn's disease, ulcerative colitis, herpes gestationis, cervical cancer, changes in appetite, optic neuritis, changes in body weight, venous thromboembolic disorders; arterial thromboembolic disorders; arterial hypertension.
Cases of hormone-dependent tumors (e.g., liver tumor, breast cancer) have been reported during the use of combined hormonal contraceptives. See section "Special Instructions" for details.
Interactions
Interactions with other medicinal products (inducers of microsomal enzymes) may lead to breakthrough bleeding and/or reduced contraceptive efficacy (see section "Interaction with other medicinal products and other forms of interaction").
Reporting of suspected adverse reactions
Reporting of suspected adverse reactions after marketing authorization is of great importance. It allows ongoing monitoring of the benefit-risk balance of the medicinal product. Healthcare professionals and patients, as well as patients' legal representatives, are encouraged to report any suspected adverse reactions and lack of efficacy through the Automated Pharmacovigilance Information System at the following link: https://aisf.dec.gov.ua.
Shelf life.
2 years.
Storage conditions
No special storage conditions required. Store in the original packaging to protect from light. Keep out of reach and sight of children.
Packaging.
1 vaginal delivery system in a sachet; 1 sachet in a cardboard box with leaflet and stickers.
Prescription category.
Prescription only.
Manufacturer.
Laboratorios Leon Farma S.A., Spain / Laboratorios Leon Farma S.A., Spain.
Manufacturer's address.
Calle La Vallina s/n, Poligono Industrial Navatejera, Villaquilambre, 24193, Spain /
Calle La Vallina s/n, Poligono Industrial Navatejera, Villaquilambre, 24193, Spain.
[1] The average range of 5 to 7 per 10,000 woman-years is based on the relative risk associated with use of combined oral contraceptives containing levonorgestrel, compared to a range of 2.3 to 3.6 when no contraceptive is used.