Ozempic
Ukraine
Table of Contents
- INSTRUCTIONS for medical use of the medicinal product OZEMPIC® (OZEMPIC®)
- Composition:
- Pharmacological Properties
- Clinical characteristics
- Special precautions for use
- Method of Administration and Dosage
- Adverse Reactions
- Adverse Reactions
- Composition:
- Pharmacological Properties
- Clinical characteristics
- Special precautions for use
- Method of Administration and Dosage
- Adverse Reactions
- Adverse Reactions
INSTRUCTIONS for medical use of the medicinal product OZEMPIC® (OZEMPIC®)
Composition:
Active substance: semaglutide;
1 ml of solution contains 1.34 mg of semaglutide – a human glucagon-like peptide-1 (GLP-1) analogue, produced in Saccharomyces cerevisiae using recombinant DNA technology;
one pre-filled pen injector contains 2 mg of semaglutide in 1.5 ml of solution;
Excipients: sodium phosphate dihydrate; propylene glycol; phenol; hydrochloric acid (for pH adjustment); sodium hydroxide (for pH adjustment); water for injections.
Pharmaceutical form. Solution for injection.
Main physicochemical properties: clear, colourless or almost colourless isotonic solution; pH = 7.4.
Pharmacotherapeutic group. Antidiabetic agents, glucagon-like peptide-1 (GLP-1) analogues. ATC code A10BJ06.
Pharmacological Properties
Pharmacodynamics
Mechanism of Action
Semaglutide is a GLP-1 analog with 94% homology to human GLP-1. Semaglutide acts as a GLP-1 receptor agonist, selectively binding to and activating GLP-1 receptors, which are the target for native GLP-1.
GLP-1 is a physiological hormone that affects glucose concentration regulation, appetite, and the cardiovascular system through multiple pathways. The effects on glucose concentration and appetite are specifically mediated by GLP-1 receptors located in the pancreas and the brain.
Semaglutide reduces blood glucose levels in a glucose-dependent manner by stimulating insulin secretion and suppressing glucagon secretion under conditions of elevated blood glucose. The mechanism of glucose reduction is also associated with a slight delay in gastric emptying during the early postprandial phase. During hypoglycemia, semaglutide reduces insulin secretion and does not interfere with glucagon secretion.
Semaglutide use leads to reduction in body weight and fat mass by decreasing caloric intake and reducing appetite. Additionally, semaglutide reduces the craving for high-fat foods.
GLP-1 receptors are also expressed in the heart, vascular system, immune system, and kidneys.
In clinical studies, semaglutide positively influenced plasma lipid levels, reduced systolic blood pressure, and decreased inflammation. In animal trials, semaglutide inhibited the development of atherosclerosis by preventing progression of aortic plaques and reducing plaque inflammation.
Pharmacodynamic Effects
All pharmacodynamic trials were conducted after 12 weeks of treatment (including dose escalation) at steady state with semaglutide 1 mg administered once weekly.
Fasting and Postprandial Glucose Levels
Semaglutide reduces fasting and postprandial glucose concentrations. In patients with type 2 diabetes, treatment with semaglutide 1 mg led to reductions in glucose concentration in terms of absolute change from baseline (mmol/L) and relative reduction compared to placebo (%) for fasting glucose concentration (1.6 mmol/L; 22%), 2-hour postprandial glucose concentration (4.1 mmol/L; 37%), mean daily glucose concentration (1.7 mmol/L; 22%), and postprandial glucose fluctuation across three meals (0.6–1.1 mmol/L) compared to placebo. Semaglutide reduced fasting glucose levels after the first administration.
Beta-cell Function and Insulin Secretion
Semaglutide improves beta-cell function. Compared to placebo, semaglutide enhanced both first and second phase insulin response, with threefold and twofold increases, respectively, and increased maximal secretory capacity of beta cells in patients with type 2 diabetes. Additionally, compared to placebo, semaglutide treatment led to increased fasting insulin concentrations.
Glucagon Secretion
Semaglutide reduces fasting and postprandial glucagon concentrations. In patients with type 2 diabetes, semaglutide use resulted in relative reductions in glucagon concentration compared to placebo: fasting glucagon concentration (8–21%), postprandial glucagon response (14–15%), and mean daily glucagon concentration (12%).
Glucose-Dependent Insulin and Glucagon Secretion
Semaglutide lowers high blood glucose levels by stimulating insulin secretion and reducing glucagon secretion in a glucose-dependent manner. The rate of insulin secretion after semaglutide administration in patients with type 2 diabetes is comparable to that in healthy individuals.
During induced hypoglycemia, semaglutide, compared to placebo, did not alter the counter-regulatory response of glucagon elevation and did not exacerbate the decline in C-peptide concentration in patients with type 2 diabetes.
Gastric Emptying
Semaglutide causes a slight delay in early postprandial gastric emptying, thereby reducing the rate of glucose entry into the bloodstream during the postprandial period.
Appetite, Calorie Intake, and Food Choice
Compared to placebo, semaglutide reduced calorie intake by 18–35% during three consecutive ad libitum meals. This was facilitated by semaglutide-induced suppression of appetite both in the fasting and postprandial states, improved control over food intake, reduced urge to snack, and relatively lower craving for high-fat foods.
Fasting and Postprandial Lipids
Compared to placebo, semaglutide reduced fasting triglyceride and very-low-density lipoprotein cholesterol (VLDL-C) concentrations by 12% and 21%, respectively. The postprandial triglyceride response and the postprandial VLDL-C response to a high-fat meal were reduced by more than 40%.
Cardiac Electrophysiology (QTc)
The effect of semaglutide on cardiac repolarization was evaluated in a thorough QTc study. Semaglutide did not prolong QTc intervals at doses up to 1.5 mg at steady state.
Clinical Efficacy and Safety
Both improved glycemic control and reduced cardiovascular morbidity and mortality are essential components of treatment for type 2 diabetes.
The efficacy and safety of semaglutide at doses of 0.5 mg and 1 mg once weekly were evaluated in six randomized, controlled phase 3a clinical trials involving 7,215 patients with type 2 diabetes (4,107 patients received semaglutide). The primary objective of five clinical trials (SUSTAIN 1–5) was to assess glycemic control efficacy, and one trial (SUSTAIN 6) focused on cardiovascular outcomes.
An additional phase 3b clinical trial (SUSTAIN 7) involving 1,201 patients was conducted to compare the efficacy and safety of semaglutide 0.5 mg and 1 mg once weekly with dulaglutide 0.75 mg and 1.5 mg, respectively, administered once weekly. A phase 3b trial (SUSTAIN 9) was conducted to investigate the efficacy and safety of semaglutide as an add-on to treatment with a sodium-glucose cotransporter-2 inhibitor (SGLT-2 inhibitor).
Treatment with semaglutide demonstrated sustained, statistically significant, and clinically meaningful reductions in HbA1c and body weight over a period of up to two years compared to placebo and active comparator treatments (sitagliptin, insulin glargine, exenatide ER, and dulaglutide).
The efficacy of semaglutide was independent of age, sex, race, ethnicity, baseline BMI, baseline body weight (kg), duration of diabetes, and degree of renal impairment.
Target outcomes were achieved across all randomized patient groups (analyses based on mixed models for repeated measurements or multiple imputation).
Additionally, a phase 3b study (SUSTAIN 11) was conducted to investigate the effect of semaglutide compared to insulin aspart as an add-on to metformin and optimized insulin glargine (100 U).
More detailed information is provided below.
SUSTAIN 1 Trial: Monotherapy
In a double-blind, placebo-controlled clinical trial lasting 30 weeks, 388 patients with inadequate disease control on diet and exercise were randomized to receive once-weekly semaglutide 0.5 mg or 1 mg, or placebo.
Table 1
SUSTAIN 1 Study: Results at Week 30
| Parameter |
Semaglutide 0.5 mg |
Semaglutide 1 mg |
Placebo |
| Number of patients |
128 |
130 |
129 |
| HbA1c (%) |
|||
| At baseline (mean value) |
8.1 |
8.1 |
8.0 |
| Change from baseline to week 30 |
-1.5 |
-1.6 |
0 |
| Difference vs placebo (95% CI) |
-1.4 [-1.7, -1.1]a |
-1.5 [-1.8, -1.2]a |
- |
| Patients (%) achieving HbA1c < 7% |
74 |
72 |
25 |
| Fasting plasma glucose (mmol/L) |
|||
| At baseline (mean value) |
9.7 |
9.9 |
9.7 |
| Change from baseline to week 30 |
-2.5 |
-2.3 |
-0.6 |
| Body weight (kg) |
|||
| At baseline (mean value) |
89.8 |
96.9 |
89.1 |
| Change from baseline to week 30 |
-3.7 |
-4.5 |
-1.0 |
| Difference vs placebo (95% CI) |
-2.7 [-3.9, -1.6]a |
-3.6 [-4.7, -2.4]a |
- |
a p < 0.0001 (two-sided) for superiority.
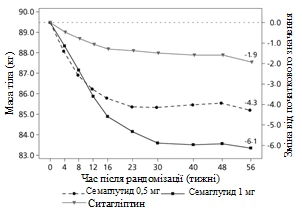
SUSTAIN 2 clinical trial. Semaglutide compared with sitagliptin, both in combination with one or two oral antidiabetic medicinal products (metformin and/or thiazolidinediones)
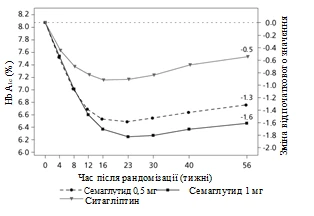
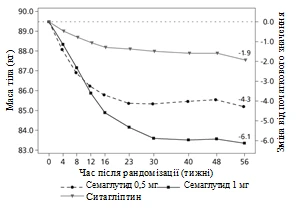
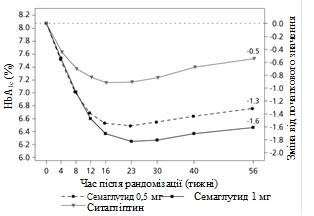
In a double-blind, active-controlled study of 56 weeks' duration, 1231 patients were randomized to receive either semaglutide 0.5 mg once weekly or 1 mg once weekly, or sitagliptin 100 mg once daily; all in combination with metformin (94%) and/or thiazolidinediones (6%).
Table 2
SUSTAIN 2 study: results at week 56
| Parameter |
Semaglutide 0.5 mg |
Semaglutide 1 mg |
Sitagliptin 100 mg |
| Number of patients |
409 |
409 |
407 |
| HbA1c (%) |
|||
| At baseline (mean value) |
8.0 |
8.0 |
8.2 |
| Change from baseline to week 56 |
-1.3 |
-1.6 |
-0.5 |
| Difference compared to sitagliptin (95% CI) |
-0.8 [-0.9, -0.6]a |
-1.1 [-1.2, -0.9]a |
- |
| Patients (%) achieving HbA1c < 7% |
69 |
78 |
36 |
| Fasting plasma glucose (mmol/L) |
|||
| At baseline (mean value) |
9.3 |
9.3 |
9.6 |
| Change from baseline to week 56 |
-2.1 |
-2.6 |
-1.1 |
| Body weight (kg) |
|||
| At baseline (mean value) |
89.9 |
89.2 |
89.3 |
| Change from baseline to week 56 |
-4.3 |
-6.1 |
-1.9 |
| Difference compared to sitagliptin (95% CI) |
-2.3 [-3.1, -1.6]a |
-4.2 [-4.9, -3.5]a |
- |
a p < 0.0001 (two-sided) for superiority.
**
**
Figure 1. Mean change in HbA1c (%) and body weight (kg) from baseline to week 56
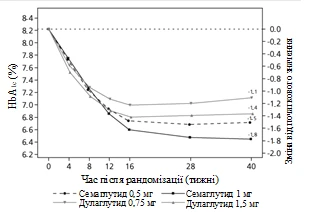
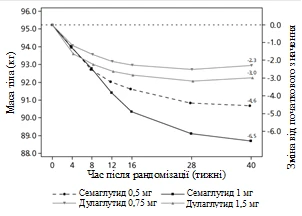
SUSTAIN 7 clinical trial. Semaglutide compared with dulaglutide, both in combination with metformin
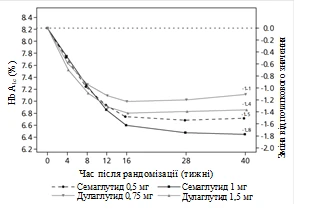
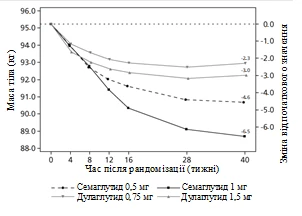
Patients in a 40-week open-label clinical trial (1,201 patients) receiving metformin were randomized in a 1:1:1:1 ratio to receive once-weekly semaglutide 0.5 mg or dulaglutide 0.75 mg, or semaglutide 1 mg, or dulaglutide 1.5 mg.
The trial compared outcomes of semaglutide 0.5 mg versus dulaglutide 0.75 mg and semaglutide 1 mg versus dulaglutide 1.5 mg.
Gastrointestinal disorders were the most common adverse reactions, occurring in a similar proportion of patients receiving semaglutide 0.5 mg (129 patients [43%]), semaglutide 1 mg (133 [44%]), and dulaglutide 1.5 mg (143 [48%]); fewer patients experienced gastrointestinal disorders with dulaglutide 0.75 mg (100 [33%]).
By week 40, the increase in pulse rate with semaglutide (0.5 mg and 1 mg) and dulaglutide (0.75 mg and 1.5 mg) was 2.4 and 4.0, and 1.6 and 2.1 beats per minute, respectively.
Table 3
SUSTAIN 7 study: results at week 40
| Parameter |
Semaglutide 0.5 mg |
Semaglutide 1 mg |
Dulaglutide 0.75 mg |
Dulaglutide 1.5 mg |
| Number of patients |
301 |
300 |
299 |
299 |
| HbA1c (%) |
||||
| At baseline (mean value) |
8.3 |
8.2 |
8.2 |
8.2 |
| Change from baseline to week 40 |
-1.5 |
-1.8 |
-1.1 |
-1.4 |
| Difference compared to dulaglutide (95% CI) |
-0.4b [-0.6, -0.2)a |
-0.4c [-0.6, -0.3]a |
- |
- |
| Patients (%) achieving HbA1c < 7% |
68 |
79 |
52 |
67 |
| Fasting plasma glucose (mmol/L) |
||||
| At baseline (mean value) |
9.8 |
9.8 |
9.7 |
9.6 |
| Change from baseline to week 40 |
-2.2 |
-2.8 |
-1.9 |
-2.2 |
| Body weight (kg) |
||||
| At baseline (mean value) |
96.4 |
95.5 |
95.6 |
93.4 |
| Change from baseline to week 40 |
-4.6 |
-6.5 |
-2.3 |
-3.0 |
| Difference compared to dulaglutide (95% CI) |
-2.3b [-3.0, -1.5)a |
-3.6c [-4.3, -2.8]a |
- |
- |
a p < 0.0001 (two-sided) for superiority.
b Semaglutide 0.5 mg compared to dulaglutide 0.75 mg.
c Semaglutide 1 mg compared to dulaglutide 1.5 mg.
**
**
Figure 2. Mean change in HbA1c (%) and body weight (kg) from baseline to week 40
Clinical trial SUSTAIN 3. Semaglutide versus exenatide ER, both in combination with metformin or metformin plus sulfonylurea
In an open-label 56-week trial, 813 patients who were on metformin only (49%), metformin plus sulfonylurea (45%), or other antidiabetic medications (6%) were randomized to receive either semaglutide 1 mg or exenatide ER 2 mg once weekly.
Table 4
SUSTAIN 3 trial: Results at week 56
| Parameter |
Semaglutide 1 mg |
Exenatide ER 2 mg |
| Number of patients |
404 |
405 |
| HbA1c (%) |
||
| At baseline (mean value) |
8.4 |
8.3 |
| Change from baseline to week 56 |
-1.5 |
-0.9 |
| Difference compared to exenatide (95 % CI) |
-0.6 [-0.8, -0.4]a |
- |
| Patients (%) achieving HbA1c < 7 % |
67 |
40 |
| Fasting plasma glucose (mmol/l) |
||
| At baseline (mean value) |
10.6 |
10.4 |
| Change from baseline to week 56 |
-2.8 |
-2.0 |
| Body weight (kg) |
||
| At baseline (mean value) |
96.2 |
95.4 |
| Change from baseline to week 56 |
-5.6 |
-1.9 |
| Difference compared to exenatide (95 % CI) |
-3.8 [-4.6, -3.0]a |
- |
a p < 0.0001 (two-sided) for superiority.
SUSTAIN 4 clinical trial. Semaglutide compared with insulin glargine, both in combination with one or two oral antidiabetic agents (metformin or metformin with sulfonylurea)
In an open-label comparator trial of 30 weeks' duration, 1089 patients were randomized to receive either semaglutide 0.5 mg once weekly, semaglutide 1 mg once weekly, or insulin glargine once daily, with concomitant use of metformin (48%) or metformin with sulfonylurea (51%).
Table 5
SUSTAIN 4 study: Results at Week 30
| Parameter |
Semaglutide 0.5 mg |
Semaglutide 1 mg |
Insulin glargine |
| Number of patients |
362 |
360 |
360 |
| HbA1c (%) |
|||
| At baseline (mean value) |
8.1 |
8.2 |
8.1 |
| Change from baseline to Week 30 |
-1.2 |
-1.6 |
-0.8 |
| Difference vs insulin glargine (95% CI) |
-0.4 [-0.5, -0.2]a |
-0.8 [-1.0, -0.7]a |
- |
| Patients (%) achieving HbA1c < 7% |
57 |
73 |
38 |
| Fasting plasma glucose (mmol/L) |
|||
| At baseline (mean value) |
9.6 |
9.9 |
9.7 |
| Change from baseline to Week 30 |
-2.0 |
-2.7 |
-2.1 |
| Body weight (kg) |
|||
| At baseline (mean value) |
93.7 |
94.0 |
92.6 |
| Change from baseline to Week 30 |
-3.5 |
-5.2 |
+1.2 |
| Difference vs insulin glargine (95% CI) |
-4.6 [-5.3, -4.0]a |
-6.34 [-7.0, -5.7]a |
- |
a p < 0.0001 (two-sided) for superiority.
SUSTAIN 5 clinical trial. Semaglutide compared with placebo, both in combination with basal insulin
In a double-blind, placebo-controlled trial lasting 30 weeks, 397 patients with inadequate control on basal insulin therapy, with or without metformin, were randomized to receive either semaglutide 0.5 mg once weekly, semaglutide 1 mg once weekly, or placebo.
Table 6
SUSTAIN 5 study: Results at Week 30
| Parameter |
Semaglutide 0.5 mg |
Semaglutide 1 mg |
Placebo |
| Number of patients |
132 |
131 |
133 |
| HbA1c (%) |
|||
| At baseline (mean value) |
8.4 |
8.3 |
8.4 |
| Change from baseline to week 30 |
-1.4 |
-1.8 |
-0.1 |
| Difference vs placebo (95% CI) |
-1.4 [-1.6, -1.1]a |
-1.8 [-2.0, -1.5]a |
- |
| Patients (%) achieving HbA1c < 7% |
61 |
79 |
11 |
| Fasting plasma glucose (mmol/L) |
|||
| At baseline (mean value) |
8.9 |
8.5 |
8.6 |
| Change from baseline to week 30 |
-1.6 |
-2.4 |
-0.5 |
| Body weight (kg) |
|||
| At baseline (mean value) |
92.7 |
92.5 |
89.9 |
| Change from baseline to week 30 |
-3.7 |
-6.4 |
-1.4 |
| Difference vs placebo (95% CI) |
-2.3 [-3.3, -1.3]a |
-5.1 [-6.1, -4.0]a |
- |
a p < 0.0001 (two-sided) for superiority.
SUSTAIN 9 clinical trial. Semaglutide compared with placebo, both as add-on to SGLT2 inhibitor ± metformin or sulphonylurea
In a double-blind, placebo-controlled trial of 30 weeks' duration, 302 patients with inadequate control on SGLT2 inhibitor with or without metformin or sulphonylurea were randomized to receive either once-weekly semaglutide 1.0 mg or placebo.
Table 7
SUSTAIN 9: Results at Week 30
| Parameter |
Semaglutide 1 mg |
Placebo |
| Number of patients |
151 |
151 |
| HbA1c (%) |
||
| At baseline (mean value) |
8.0 |
8.1 |
| Change from baseline to week 30 |
-1.5 |
-0.1 |
| Difference vs placebo (95% CI) |
-1.4 [-1.6, -1.2]a |
- |
| Patients (%) achieving HbA1c < 7% |
78.7 |
18.7 |
| Fasting plasma glucose (mmol/L) |
||
| At baseline (mean value) |
9.1 |
8.9 |
| Change from baseline to week 30 |
-2.2 |
0.0 |
| Body weight (kg) |
||
| At baseline (mean value) |
89.6 |
93.8 |
| Change from baseline to week 30 |
-4.7 |
-0.9 |
| Difference vs placebo (95% CI) |
-3.8 [-4.7, -2.9]a |
- |
a p < 0.0001 (two-sided) for superiority, adjusted for multiplicity based on hierarchical testing of HbA1c and body weight.
Clinical trial SUSTAIN 11 – Semaglutide versus insulin aspart as add-on to insulin glargine + metformin
In a 52-week open-label trial, 1748 patients with inadequately controlled type 2 diabetes after a 12-week run-in period with insulin glargine and metformin were randomized 1:1 to receive once-weekly semaglutide (0.5 mg or 1.0 mg) or insulin aspart three times daily. The enrolled population had a mean diabetes duration of 13.4 years and a mean HbA1c of 8.6%, with a target HbA1c of 6.5–7.5%.
Treatment with semaglutide resulted in a reduction in HbA1c at week 52 (-1.5% for semaglutide versus -1.2% for insulin aspart).
The number of episodes of severe hypoglycemia was low in both treatment groups (4 episodes with semaglutide versus 7 episodes with insulin aspart).
Mean baseline body weight decreased with semaglutide (-4.1 kg) and increased with insulin aspart (+2.8 kg), with a treatment-dependent estimated difference of -6.99 kg (95% CI: -7.41 to -6.57) at week 52.
Combination with sulfonylurea monotherapy
In the SUSTAIN 6 clinical trial (see section "Cardiovascular disease"), 123 patients were initially on sulfonylurea monotherapy. Baseline HbA1c was 8.2%, 8.4%, and 8.4% with semaglutide 0.5 mg, semaglutide 1 mg, and placebo, respectively. After 30 weeks, HbA1c decreased by 1.6% and 1.5% with semaglutide 0.5 mg and 1 mg, respectively, and increased by 0.1% with placebo.
Combination with premixed insulin ± one or two oral glucose-lowering agents (OGLAs)
In the SUSTAIN 6 trial (see section "Cardiovascular disease"), 867 patients were on premixed insulin (at baseline with or without OGLAs). Baseline HbA1c was 8.8%, 8.9%, and 8.9% with semaglutide 0.5 mg, semaglutide 1 mg, and placebo, respectively. After 30 weeks, HbA1c decreased by 1.3%, 1.8%, and 0.4% with semaglutide 0.5 mg, semaglutide 1 mg, and placebo, respectively.
Cardiovascular disease
In a double-blind, 104-week clinical trial (SUSTAIN 6), 3297 patients with type 2 diabetes and high cardiovascular risk were randomized to receive once-weekly semaglutide 0.5 mg or 1 mg or placebo, in addition to standard of care, over the next 2 years. Overall, 98% of patients completed the trial, and vital signs data were available at endpoint for 99.6% of them.
The study population was distributed by age as follows: 1598 patients (48.5%) aged ≥65 years, 321 (9.7%) aged ≥75 years, and 20 (0.6%) aged ≥85 years. Renal function was normal or mildly impaired in 2358 patients, moderately impaired in 832 patients, and severely impaired or at end-stage renal disease in 107 patients. The population included 61% men, with a mean age of 65 years and a mean BMI of 33 kg/m². The mean duration of diabetes was 13.9 years.
The primary endpoint was time from randomization to first occurrence of a major adverse cardiovascular event (MACE): cardiovascular death, non-fatal myocardial infarction, or non-fatal stroke.
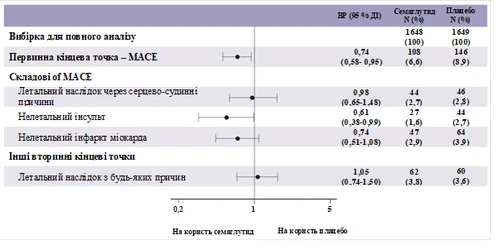
The composite rate for the components of the primary MACE endpoint was 254, including 108 (6.6%) with semaglutide and 146 (8.9%) with placebo. See Figure 4 for results on primary and secondary cardiovascular endpoints. Treatment with semaglutide resulted in a 26% reduction in the risk of the composite primary endpoint of cardiovascular death, non-fatal myocardial infarction, and non-fatal stroke. The total number of cardiovascular deaths, non-fatal myocardial infarctions, and non-fatal strokes was 90, 111, and 71, respectively, including 44 (2.7%), 47 (2.9%), and 27 (1.6%) cases, respectively, with semaglutide (Figure 4). The risk reduction in the primary composite endpoint was primarily driven by reductions in non-fatal stroke (39%) and non-fatal myocardial infarction (26%) (Figure 3).
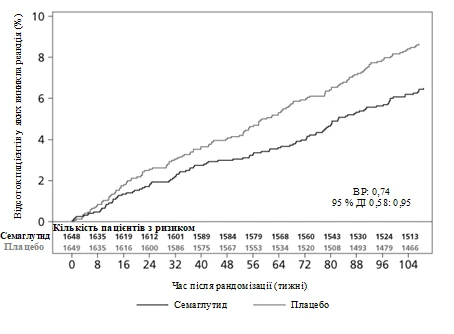
Figure 3. Kaplan-Meier curve for time to first occurrence of the composite event: cardiovascular death, non-fatal myocardial infarction, and non-fatal stroke (SUSTAIN 6 clinical trial).
**
**
Figure 4. Forest plot: time-to-first-event analysis for the composite endpoint, its components, and all-cause mortality (SUSTAIN 6 trial)
A total of 158 cases of new or worsening nephropathy were recorded. The HR [95% CI] for time to nephropathy, defined by persistent macroalbuminuria (first occurrence of persistent macroalbuminuria, sustained doubling of serum creatinine, need for continuous renal replacement therapy, or death due to kidney disease), was 0.64 [0.46; 0.88].
Body weight
After one year of treatment, body weight loss of ≥5% and ≥10% was observed in a higher proportion of patients receiving semaglutide 0.5 mg (46% and 13%) and 1 mg (52–62% and 21–24%) compared to those receiving the active comparators sitagliptin (18% and 3%) and exenatide ER (17% and 4%).
In a 40-week head-to-head trial versus dulaglutide, a higher proportion of patients achieved body weight loss of ≥5% and ≥10% with semaglutide 0.5 mg (44% and 14%) versus dulaglutide 0.75 mg (23% and 3%), and with semaglutide 1 mg (up to 63% and 27%) versus dulaglutide 1.5 mg (30% and 8%).
In the SUSTAIN 6 trial, significant and sustained reductions in body weight from baseline to week 104 were observed with semaglutide 0.5 mg and 1 mg compared to placebo 0.5 mg and 1 mg, as add-on to standard of care (-3.6 kg and -4.9 kg versus -0.7 kg and -0.5 kg, respectively).
Blood pressure
Significant reductions in mean systolic blood pressure were observed with semaglutide 0.5 mg (3.5–5.1 mmHg) and 1 mg (5.4–7.3 mmHg) when used in combination with oral antidiabetic agents or basal insulin. No significant difference was observed in diastolic blood pressure between semaglutide treatment and comparator agents.
Children
The European Medicines Agency has deferred the obligation to submit results of studies with Ozempic® in one or more pediatric subgroups for the treatment of type 2 diabetes (see section "Dosage and administration").
Pharmacokinetics
Compared to native GLP-1, semaglutide has a prolonged elimination half-life of approximately 1 week, enabling once-weekly subcutaneous administration. The main mechanism behind this prolonged action is albumin binding, which reduces renal clearance and protects against metabolic degradation. Additionally, semaglutide is stabilized against degradation by the enzyme DPP-4.
Absorption
Maximum concentration is reached within 1–3 days after administration. Steady-state concentration is achieved after 4–5 weeks of once-weekly dosing. In patients with type 2 diabetes, the mean steady-state concentrations after subcutaneous administration of 0.5 mg and 1 mg semaglutide were approximately 16 nmol/L and 30 nmol/L, respectively. Exposure to semaglutide increased in a dose-proportional manner with doses of 0.5 mg and 1 mg. Similar exposure was achieved following subcutaneous administration in the abdomen, thigh, or upper arm. The absolute bioavailability of semaglutide after subcutaneous administration is 89%.
Distribution
The mean volume of distribution of semaglutide after subcutaneous administration in patients with type 2 diabetes is approximately 12.5 L. Semaglutide is highly bound to plasma albumin (>99%).
Metabolism
Prior to excretion, semaglutide is actively metabolized via proteolytic cleavage of the peptide backbone and subsequent beta-oxidation of the fatty acid side chain. Neutral endopeptidase (NEP) is believed to be involved in the metabolism of semaglutide.
Excretion
In a study with subcutaneous administration of a single radiolabeled dose of semaglutide, semaglutide-related material was excreted mainly via urine and feces; approximately 2/3 of the semaglutide-related material was excreted in urine and approximately 1/3 in feces. Approximately 3% of the administered dose was excreted unchanged in urine. In patients with type 2 diabetes, the clearance of semaglutide is approximately 0.05 L/h. With its elimination half-life of approximately 1 week, semaglutide remains in circulation for about 5 weeks after the last dose.
Special patient groups
Geriatric patients
Based on data from phase 3a trials involving patients aged 20–86 years, age does not influence the pharmacokinetics of semaglutide.
Sex, race, and ethnicity
Sex, race (Caucasian, African, or Asian), and ethnicity (Hispanic or Latino, non-Hispanic or non-Latino) do not influence the pharmacokinetics of semaglutide.
Body weight
Body weight influences semaglutide exposure. Higher body weight leads to lower exposure; a 20% difference in individual body weight results in nearly a 16% difference in exposure. Semaglutide doses of 0.5 mg and 1 mg provide adequate systemic exposure across a body weight range of 40–198 kg.
Renal impairment
Renal impairment does not have a clinically significant effect on the pharmacokinetics of semaglutide. This was demonstrated after administration of a single 0.5 mg dose of semaglutide in patients with mild, moderate, severe renal impairment, or on dialysis, compared to patients with normal renal function. This was also confirmed by data from phase 3a clinical trials in patients with type 2 diabetes and renal impairment, although experience in patients with end-stage renal disease is limited.
Hepatic impairment
Hepatic impairment does not affect semaglutide exposure. Pharmacokinetics of semaglutide after a single 0.5 mg dose were evaluated in patients with mild, moderate, or severe hepatic impairment compared to patients with normal liver function.
Children
Studies of semaglutide in pediatric patients have not been conducted.
Preclinical safety data
Preclinical data based on studies of pharmacological safety, repeated-dose toxicity, and genotoxicity revealed no risk to humans.
Non-lethal tumors originating from C-cells of the thyroid gland observed in rodents are effects typical of the class of GLP-1 receptor agonists. In a 2-year carcinogenicity study in rats and mice, semaglutide caused thyroid C-cell tumors at clinically relevant exposure levels. No other tumors related to treatment were observed. The tumors in rodents are attributed to a non-genotoxic, GLP-1 receptor-mediated mechanism to which rodents are partially sensitive. The relevance of this mechanism to humans is considered low but cannot be fully excluded.
In fertility studies in rats, semaglutide did not affect mating performance or fertility in males. In female rats, prolonged estrous cycle duration and a slight reduction in corpora lutea (ovulation) were observed at doses associated with body weight loss.
In embryo-fetal development studies in rats, semaglutide caused embryotoxic effects at exposures below clinically relevant levels. Semaglutide caused marked body weight loss in females and reduced embryo survival and growth. Fetal skeletal and visceral malformations were observed, including changes in long bones, ribs, spine, tail bones, blood vessels, and brain ventricles. Mechanistic evaluation indicated that the embryotoxic effect involves GLP-1 receptor-mediated disruption of nutrient supply to the embryo via the yolk sac in rats. Due to anatomical and functional differences in the yolk sac across species and the lack of GLP-1 receptor expression in the yolk sac of non-human primates, this mechanism is considered unlikely in humans. However, a direct effect of semaglutide on the fetus cannot be ruled out.
In developmental toxicity studies in rabbits and cynomolgus monkeys at clinically relevant exposure levels, increased pregnancy loss and a slight increase in fetal abnormalities were observed. These findings coincided with marked body weight loss in females, reaching up to 16%. It is unknown whether these effects are related to reduced food intake due to direct GLP-1 effects.
Postnatal growth and development were evaluated in cynomolgus monkeys. Offspring were slightly smaller at birth, but body weight normalized during the lactation period.
In young rats, semaglutide caused delayed sexual maturation in both males and females. This delay did not affect fertility, reproductive capacity, or the ability of females to maintain pregnancy.
Clinical characteristics
Indications
Ozempic® should be used in inadequately controlled type 2 diabetes mellitus as an adjunct to diet and exercise:
- as monotherapy when metformin is considered inappropriate due to intolerance or contraindications;
- as an adjunct to other antidiabetic medicinal products.
For information on study results of combination therapies, effects on glycemic control and cardiovascular outcomes, as well as patient populations studied, see sections "Special warnings and precautions for use", "Interaction with other medicinal products and other forms of interaction", and "Pharmacodynamics".
Contraindications
Hypersensitivity to the active substance or to any of the excipients (see section "Composition").
Interaction with other medicinal products and other forms of interaction
Semaglutide delays gastric emptying and may affect the rate of absorption of concomitantly administered oral medicinal products. Semaglutide should be used with caution in patients receiving oral medicinal products requiring rapid absorption in the gastrointestinal tract.
Paracetamol
Based on pharmacokinetic assessment of paracetamol during a standardized meal test, semaglutide delays gastric emptying. Following concomitant administration of paracetamol with semaglutide 1 mg, AUC0–60min and Cmax of paracetamol were reduced by 27% and 23%, respectively. Total exposure to paracetamol (AUC0–5h) was unchanged. Dose adjustment of paracetamol is not required when administered concomitantly with semaglutide.
Oral contraceptives
A reduction in efficacy of oral contraceptives is not expected with semaglutide. When administered concomitantly with a combined oral contraceptive medicinal product (ethinylestradiol 0.03 mg / levonorgestrel 0.15 mg), semaglutide did not clinically significantly affect the total exposure of ethinylestradiol and levonorgestrel. Exposure to ethinylestradiol was unaffected; exposure to levonorgestrel increased by 20% at steady state. Cmax of either component was unchanged.
Atorvastatin
Semaglutide did not alter total exposure of atorvastatin following a single 40 mg dose of atorvastatin. Cmax of atorvastatin was reduced by 38%. This was considered clinically insignificant.
Digoxin
Semaglutide did not alter total exposure or Cmax of digoxin following a single 0.5 mg dose of digoxin.
Metformin
Semaglutide did not alter total exposure or Cmax of metformin following administration of metformin 500 mg twice daily for 3.5 days.
Warfarin and other coumarin derivatives
Semaglutide did not alter total exposure or Cmax of R- and S-warfarin following a single 25 mg dose of warfarin, and pharmacodynamic parameters of warfarin measured by international normalized ratio (INR) were not clinically significantly altered. However, cases of decreased INR have been reported with concomitant use of acenocoumarol and semaglutide. Frequent INR monitoring is recommended at the initiation of semaglutide treatment in patients taking warfarin or other coumarin derivatives.
Special precautions for use
Traceability
In order to improve the traceability of biological medicinal products, the name and batch number of the administered product should be clearly documented on the packaging.
Aspiration in combination with general anaesthesia or deep sedation
Cases of pulmonary aspiration have been reported in patients receiving GLP-1 receptor agonists who were under general anaesthesia or deep sedation. Therefore, before performing procedures involving general anaesthesia or deep sedation, the increased risk of residual gastric content due to delayed gastric emptying should be considered (see section "Adverse reactions").
General information
Semaglutide should not be used in patients with type 1 diabetes or for the treatment of diabetic ketoacidosis. Semaglutide is not an insulin replacement. Cases of diabetic ketoacidosis have been reported in insulin-dependent patients who initiated treatment with a GLP-1 receptor agonist and rapidly discontinued or substantially reduced their insulin dose (see section "Dosage and administration").
There is no clinical experience in treating patients with NYHA class IV heart failure; therefore, semaglutide is not recommended for use in these patients.
Gastrointestinal effects
Use of GLP-1 receptor agonists may be associated with gastrointestinal adverse reactions. This should be considered when treating patients with renal impairment, as nausea, vomiting, and diarrhoea may lead to dehydration, which could worsen renal function (see section "Adverse reactions").
Acute pancreatitis
Cases of acute pancreatitis have been observed during treatment with GLP-1 receptor agonists.
Patients should be informed about the typical symptoms of acute pancreatitis. If pancreatitis is suspected, semaglutide should be discontinued; if pancreatitis is confirmed, treatment with semaglutide must not be resumed. Semaglutide should be used with caution in patients with a history of pancreatitis.
Hypoglycaemia
The risk of hypoglycaemia may be increased in patients receiving semaglutide in combination with sulphonylureas or insulin. The risk of hypoglycaemia can be reduced by reducing the dose of sulphonylurea or insulin at the initiation of semaglutide treatment (see section "Adverse reactions").
Diabetic retinopathy
An increased risk of complications of diabetic retinopathy has been observed in patients with diabetic retinopathy receiving insulin and semaglutide (see section "Adverse reactions"). Semaglutide should be used with caution in patients with diabetic retinopathy who are receiving insulin. These patients should be closely monitored and managed according to clinical guidelines. Rapid improvement in glucose control has been associated with a transient worsening of diabetic retinopathy; however, the possibility of other mechanisms cannot be excluded.
Sodium content
This medicinal product contains less than 1 mmol sodium (23 mg) per dose and is therefore considered essentially "sodium-free".
Use during pregnancy or breastfeeding
Women of reproductive potential
Women of reproductive potential are advised to use contraception during treatment with semaglutide.
Pregnancy
Animal studies have shown reproductive toxicity (see section "Non-clinical safety data"). Data on the use of semaglutide in pregnant women are limited. Therefore, semaglutide should not be used during pregnancy. Semaglutide treatment should be discontinued in patients planning to become pregnant or who are pregnant. Due to the long elimination half-life of semaglutide, treatment should be discontinued at least 2 months before planned pregnancy (see section "Pharmacokinetics").
Breastfeeding
Semaglutide passes into milk during lactation in rats. Since a risk to the breastfed infant cannot be excluded, semaglutide should not be used during breastfeeding.
Fertility
The effect of semaglutide on fertility in humans is unknown. Semaglutide did not affect fertility in male rats. In female rats, prolongation of the oestrous cycle and reduced number of ovulations were observed at doses associated with body weight loss (see section "Non-clinical safety data").
Ability to affect the capacity to drive and use machines
Semaglutide has no or negligible influence on the ability to drive or operate machinery. However, when used in combination with sulphonylureas or insulin, patients should be advised to take precautions to avoid hypoglycaemia while driving or operating machinery (see section "Special precautions for use").
Method of Administration and Dosage
Dosage
The initial dose is 0.25 mg of semaglutide once weekly. After 4 weeks, the dose should be increased to 0.5 mg once weekly. To further improve glycemic control after at least 4 weeks of treatment with the 0.5 mg dose, the dose may be increased to 1 mg once weekly.
The 0.25 mg dose of semaglutide is not a maintenance dose. Weekly doses exceeding 1 mg are not recommended.
When Ozempic® is added to ongoing treatment with metformin and/or thiazolidinedione or a sodium-glucose cotransporter-2 inhibitor (SGLT2 inhibitor), the current dose of metformin and/or thiazolidinedione or SGLT2 inhibitor may remain unchanged.
When Ozempic® is added to ongoing treatment with a sulfonylurea or insulin, consider reducing the dose of sulfonylurea or insulin to reduce the risk of hypoglycemia (see sections "Adverse Reactions" and "Ability to Affect Driving and Use of Machines").
Dose adjustments of Ozempic® do not require self-monitoring of blood glucose levels. Self-monitoring of blood glucose levels is required for dose adjustments of sulfonylurea and insulin, especially when initiating Ozempic® treatment and when reducing insulin dose. A stepwise insulin dose reduction regimen is recommended.
Missed Dose
If a dose is missed, it should be administered as soon as possible within 5 days of the missed dose. If more than 5 days have passed, the missed dose should be skipped and the next dose administered on the regularly scheduled day. In this way, patients can resume their regular once-weekly dosing schedule.
If necessary, the day of weekly administration may be changed, provided that the interval between two doses is at least 3 days (>72 hours). After selecting a new administration day, continue treatment according to the once-weekly schedule.
Special Patient Populations
Elderly Patients
Dose adjustment based on age is not required. Experience in patients aged ≥75 years is limited (see section "Pharmacokinetics").
Renal Impairment
Dose adjustment is not required in patients with mild, moderate, or severe renal impairment. Experience with semaglutide in patients with severe renal impairment is limited. Semaglutide is not recommended in patients with end-stage renal disease (see section "Pharmacokinetics").
Hepatic Impairment
Dose adjustment is not required in patients with hepatic impairment. Experience with semaglutide in patients with severe hepatic impairment is limited. Semaglutide should be used with caution in such patients (see section "Pharmacokinetics").
Children
The safety and efficacy of semaglutide in children (under 18 years of age) have not been established. No data are available.
Administration Method
Administer subcutaneously.
Ozempic® is administered subcutaneously in the abdominal area, thigh, or upper arm. Injection site may be rotated without dose adjustment. Ozempic® must not be administered intravenously or intramuscularly.
Ozempic® should be administered once weekly at any time of day, independent of meals.
For further information on administration, see section "Handling and Disposal Instructions".
Handling and Disposal Instructions
Patients should be advised to dispose of the needle after each injection and to store the pen without an attached needle. This may prevent needle clogging, contamination, infection, leakage of solution, and inaccurate dosing. Needles and other waste materials should be disposed of according to local requirements. The pen is intended for individual use only. Ozempic® should not be used if the solution does not appear clear, colorless, or almost colorless. Do not use after freezing. The pen is designed for use with NovoFine® or NovoTwist® disposable needles up to 8 mm in length. NovoFine® Plus needles are included in the product packaging.
| Instructions for Use of the Ozempic® Pen 0.25 mg, 0.5 mg (solution for injection in a pre-filled pen) |
|
| For detailed information, see the package leaflet before using the Ozempic® pen. Speak with your doctor, nurse, or pharmacist about how to properly inject Ozempic®. Before using the pen, check it to make sure it contains Ozempic® in the dose of 0.25 mg or 0.5 mg. Then review the illustrations below to learn about the different parts of the pen and the needle. If the patient cannot see at all or has poor vision and is unable to read the dose counter on the pen, the pen must not be used without assistance. Assistance must be provided by a person with good vision who knows how to use the pre-filled Ozempic® pen. The pen is pre-filled and has a dose selection mechanism. It contains 2 mg of semaglutide. You will be able to select doses of 0.25 mg or 0.5 mg. One new, unused pen contains:
Use the table on the carton lid to track how many injections you have given and when: You should indicate the day of the week chosen for administration
|
|
|
|
0.5 mg per dose. This is especially important if you use different injectable medicines. Using the wrong medicine may be harmful to your health.
|
|
|
|
Check whether the paper membrane or the outer needle cap is damaged, as this may indicate loss of sterility. If there is any damage, use a new needle.
|
|
| Ensure the needle is properly attached.
|
|
| The needle is covered by two caps. Both caps must be removed. If you forget to remove both caps, you will not deliver the solution injection.
|
|
A drop of solution may appear at the needle tip. This is normal. However, you must check medicine flow when using a new pen for the first time. See step 2, “Checking solution flow with each new pen.” Do not attach a new needle until you are ready to inject. |
|
| Always use a new needle for each injection. This helps prevent needle blockage, contamination, infection, and incorrect dosing. |
|
| Never use a needle if it is bent or damaged. |
|
|
|
|
|
Press and hold the dose button until the dose counter returns to “0”. The “0” should align with the dose pointer. A drop of solution should appear at the needle tip. |
|
| A small drop may remain at the needle tip, but it will not be injected. If no drop appears, repeat step 2 “Checking solution flow with a new pen” up to 6 times. If still no drop appears, change the needle and repeat the steps in step 2 “Checking solution flow with a new pen” once more. If no drop still appears, dispose of the pen and use a new one. |
|
| You must always ensure a drop appears at the needle tip before first using a new pen. This ensures the solution will be delivered. If no drop appears, do not use the pen, even if the dose counter changes. This may indicate a blocked or damaged needle. If you do not check flow before the first injection of a new pen, you may not receive the required dose of solution needed for the desired effect of Ozempic®. |
|
|
|
If you select the wrong dose, you can turn the dose selector forward or backward to the correct dose. The maximum dose the pen can deliver is 0.5 mg. |
|
| The dose selector allows you to adjust the dose. Only the dose counter and dose pointer show how many milligrams you have selected for injection. You can only select 0.5 mg of medicine per dose. If the pen contains less than 0.5 mg of medicine, the dose counter will stop before reaching 0.5. When turning the selector forward, backward, or beyond the selected dose indicator, the pen clicks differently. Do not count the number of clicks. |
|
| Always use the dose counter and dose pointer to verify the selected dose before injecting. Do not count the number of clicks of the pen. Only doses of 0.25 mg or 0.5 mg can be selected using the dose selector. The selected dose must exactly align with the dose pointer to ensure correct dosing. |
|
| Remaining solution in the pen |
|
|
|
| If there is not enough solution for a full dose, do not use the pen. Use a new Ozempic® pen. |
|
|
|
|
|
“0” should align with the dose pointer. You may then hear or feel a click.
|
|
|
|
If a drop of blood appears at the injection site, press gently on the area. |
|
| You may see a drop of solution at the needle tip after injection. This is normal and does not affect the volume of the injected dose. |
|
| Always look at the dose pointer to confirm how many milligrams of solution you have injected. Keep the injection button pressed until the dose pointer returns to “0”. How to detect a blocked or damaged needle.
What to do with a blocked needle. Remove the needle as described in step 5 “After injection” and repeat all steps starting from step 1 “Preparing the pen with a new needle for use.” Make sure you select the correct dose. Never touch the dose counter during injection. This may interrupt the injection. |
|
|
|
| Always dispose of the needle after each injection to ensure ease of future injections and prevent using a blocked needle. If the needle is blocked, you cannot inject the medicine.
|
|
|
|
|
|
| When the pen is empty, dispose of it without the needle according to instructions from your doctor, nurse, pharmacist, or local regulations. |
|
| Never try to reattach the inner needle cap to the needle. You may injure yourself with the needle. Always remove the needle from the pen after each injection. This helps prevent needle blockage, contamination, infection, leakage, and inaccurate dosing. |
|
| Additional important information. |
|
|
|
| Caring for the pen. |
|
| Handle your pen carefully. Rough handling or improper use may result in incorrect dosing. If this occurs, you may not achieve the desired effect of the medicine. |
|
|
|

















Children
The safety and efficacy of semaglutide in children (under 18 years of age) have not been established. Data are lacking.
The European Medicines Agency has deferred the obligation to submit the results of studies with semaglutide in one or more paediatric subgroups for the treatment of type 2 diabetes (see section "Posology and method of administration").
Overdose
During clinical trials, overdose was reported up to 4 mg following single administration and up to 4 mg when administered over one week. Nausea was the most frequently reported event. All patients recovered without complications.
There is no specific antidote for the treatment of semaglutide overdose. In case of overdose, supportive treatment should be administered according to the clinical signs and symptoms present in the patient. Due to the long elimination half-life of semaglutide of approximately one week, prolonged treatment of symptoms may be necessary (see section "Pharmacokinetics").
Adverse Reactions
Summary of safety profile
In eight phase 3 clinical trials, 4792 patients received semaglutide at doses up to 1 mg. During clinical trials, the most frequently reported adverse reactions were gastrointestinal in nature, including nausea (very common), diarrhea (very common), and vomiting (common). Overall, these reactions were of mild or moderate severity and transient.
Adverse Reactions
Below is a list of adverse reactions identified in all Phase 3a trials in patients with type 2 diabetes (described in more detail in the "Pharmacodynamics" section). The frequency of adverse reactions is based on pooled data from Phase 3a clinical trials, except for cardiovascular outcomes trials (see additional information below).
Adverse reactions are classified by system organ class and frequency of occurrence. Frequency is defined according to the following scale: very common: (≥ 1/10), common: (≥ 1/100 to < 1/10), uncommon: (≥ 1/1000 to < 1/100), rare: (≥ 1/10,000 to < 1/1000), very rare: (< 1/10,000), not known: (cannot be estimated from available data). Within each category, adverse reactions are listed in order of decreasing severity.
Immune system disorders: uncommon – hypersensitivityc; rare – anaphylactic reaction.
Metabolism and nutrition disorders: very common – hypoglycaemiaa when used concomitantly with insulin or sulphonylureas; common – hypoglycaemiaa when used concomitantly with other antidiabetic medicinal products, decreased appetite.
Nervous system disorders: common – dizziness; uncommon – dysgeusia.
Eye disorders: common – complications of diabetic retinopathyb.
Cardiac disorders: uncommon – increased heart rate.
Gastrointestinal disorders: very common – nausea, diarrhoea; common – vomiting, abdominal pain, abdominal distension, constipation, dyspepsia, gastritis, gastroesophageal reflux disease, eructation, flatulence; uncommon – acute pancreatitis, delayed gastric emptying; not known – intestinal obstructiond.
Hepatobiliary disorders: common – cholelithiasis.
Skin and subcutaneous tissue disorders: not known – angioedemad.
General disorders and administration site conditions: common – fatigue; uncommon – injection site reactions.
Investigations: common – increased lipase levels, increased amylase levels, decreased body weight.
a Hypoglycaemia was defined as severe (requiring assistance from another person) or symptomatic event with a concurrent blood glucose measurement < 3.1 mmol/L.
b Complications of diabetic retinopathy include the following: retinal photocoagulation, treatment with intravitreal injection agents, vitreous haemorrhage, blindness due to diabetes (uncommon). Frequency was determined based on data from the cardiovascular outcomes trial.
c General term including also hypersensitivity-related adverse events such as rash and urticaria.
d Post-marketing reports.
Cardiovascular outcomes trial and 2-year safety trial
In patients at high risk of cardiovascular disease, the adverse reaction profile was similar to that observed in other Phase 3a trials (described in the "Pharmacodynamics" section).
Description of selected adverse reactions
Hypoglycaemia
Severe hypoglycaemic episodes were not observed when semaglutide was used as monotherapy. Severe hypoglycaemia was mainly observed when semaglutide was used in combination with sulphonylureas (1.2% of patients; 0.03 events per patient-year) or insulin (1.5% of patients; 0.02 events per patient-year). A few episodes (0.1% of patients; 0.001 events per patient-year) occurred when semaglutide was used in combination with other oral antidiabetic agents, excluding sulphonylureas.
The American Diabetes Association classified hypoglycaemia in 11.3% of patients (0.3 events per patient-year) receiving semaglutide 1.0 mg in combination with DPP-4 inhibitors in the SUSTAIN 9 trial, compared to 2.0% of patients (0.04 events per patient-year) receiving placebo. Severe hypoglycaemia was reported in 0.7% (0.01 events per patient-year) and 0% of patients, respectively.
Gastrointestinal adverse reactions
Nausea was observed in 17.0% and 19.9% of patients receiving semaglutide 0.5 mg and 1 mg, respectively; diarrhoea in 12.2% and 13.3%, and vomiting in 6.4% and 8.4%. Most cases were mild to moderate in severity and transient. These reactions led to discontinuation of treatment in 3.9% and 5% of patients, respectively. Reactions were most frequently reported during the first months of treatment. The number of gastrointestinal disorders may be higher in patients with low body weight receiving semaglutide. In the SUSTAIN 9 trial, constipation and gastroesophageal reflux disease were observed in 6.7% and 4% of patients, respectively, receiving semaglutide 1.0 mg in combination with DPP-4 inhibitors, compared to no events in patients receiving placebo. The incidence of these events did not decrease over time.
Acute pancreatitis
The incidence of confirmed acute pancreatitis reported in Phase 3a clinical trials was 0.3% with semaglutide and 0.2% with comparator. In the cardiovascular outcomes trial lasting
2 years, the incidence of expert-adjudicated acute pancreatitis was 0.5% with semaglutide and 0.6% with placebo (see section "Special precautions for use").
Complications of diabetic retinopathy
A 2-year clinical trial included 3297 patients with type 2 diabetes, high cardiovascular risk, long duration of diabetes, and inadequate glycaemic control. In this trial, confirmed events of diabetic retinopathy complications occurred in more patients receiving semaglutide (3.0%) than in those receiving placebo (1.8%). This was observed in patients with confirmed diabetic retinopathy who were receiving insulin. The difference between treatment groups emerged early and persisted throughout the trial. Systematic assessment of diabetic retinopathy complications was performed only in the cardiovascular outcomes trial. In a 1-year clinical trial involving 4807 patients with type 2 diabetes, the proportion of patients with adverse events related to diabetic retinopathy was similar in the semaglutide group (1.7%) and the comparator group (2.0%).
Discontinuation of treatment due to adverse reactions
The frequency of treatment discontinuation due to adverse events was 6.1% and 8.7% in patients receiving semaglutide 0.5 mg and 1 mg, respectively, compared to 1.5% in those receiving placebo. The most common adverse reactions leading to treatment discontinuation were gastrointestinal disorders.
Injection site reactions
Injection site reactions (such as rash, erythema at injection site) were reported in 0.6% and 0.5% of patients receiving semaglutide 0.5 mg and 1 mg, respectively. These reactions were generally mild.
Immunogenicity
Due to the potential immunogenic properties of medicinal products containing proteins or peptides, there is a possibility of antibody formation in patients during treatment with semaglutide. The percentage of patients with positive test results for anti-semaglutide antibodies at any time after initiation of treatment was low (1–2%), and no patient had neutralising antibodies to semaglutide or antibodies with neutralising GLP-1 effect at the end of clinical trials.
Increased heart rate
An increase in heart rate has been observed with GLP-1 receptor agonists. In Phase 3a clinical trials, patients receiving Ozempic® experienced a mean increase in heart rate of 1 to 6 beats per minute (bpm) from a baseline of 72–76 bpm. In a long-term trial involving patients with risk factors for cardiovascular disease, after 2 years of treatment, 16% of patients receiving Ozempic® had an increase in heart rate of > 10 bpm compared to 11% of patients receiving placebo.
Reporting of suspected adverse reactions
After marketing authorization, it is important to report suspected adverse reactions. This allows continued monitoring of the benefit-risk balance of the medicinal product. Healthcare professionals are encouraged to report suspected adverse reactions via the national reporting system.
Shelf life
Before first use – 3 years.
After first use – 6 weeks.
After first use, store below 30 °C or in the refrigerator (at 2–8 °C). Do not freeze.
Store the pen with the cap attached to protect from light.
Storage conditions
Before first use: store in the refrigerator (2–8 °C), not too close to the freezer compartment. Do not freeze. Do not use after freezing.
Store the pen with the cap attached to protect from light.
Storage conditions after first use are described in the "Shelf life" section.
Keep out of the reach of children.
Incompatibilities
Since compatibility studies have not been conducted, this medicinal product must not be mixed with other medicinal products.
Packaging
Pre-filled multi-dose disposable pen made of polypropylene, polyoxymethylene, polycarbonate and acrylonitrile butadiene styrene, containing a cartridge (type I glass) sealed on one side with a rubber (chlorobutyl) plunger and on the other side with an aluminium cap with a laminated rubber seal (bromobutyl / polyisoprene).
The pen contains 1.5 mL of solution, allowing administration of doses of 0.25 mg or 0.5 mg. The package contains 1 pre-filled pen and 6 disposable NovoFine® Plus needles in a cardboard box.
Prescription category. Prescription only.
Manufacturer
A/T Novo Nordisk.
Manufacturer's address and place of business
Novo Allé
2880, Bagsværd
Denmark.
Marketing authorization holder
A/T Novo Nordisk.
Address of the marketing authorization holder
Novo Allé
2880, Bagsværd
Denmark.
INSTRUCTION
for medical use of the medicinal product
OZEMPIC®
(OZEMPIC®)
Composition:
active substance: semaglutide;
1 ml of solution contains 1.34 mg of semaglutide – a human glucagon-like peptide-1 (GLP-1) analogue produced in Saccharomyces cerevisiae using recombinant DNA technology;
one pre-filled pen injector contains 4 mg of semaglutide in 3.0 ml of solution. Each dose contains 1 mg of semaglutide in 0.74 ml of solution;
excipients: sodium phosphate dihydrate; propylene glycol; phenol; hydrochloric acid (for pH adjustment); sodium hydroxide (for pH adjustment); water for injections.
Pharmaceutical form. Solution for injection.
Main physicochemical properties: clear, colourless or almost colourless isotonic solution; pH = 7.4.
Pharmacotherapeutic group. Antidiabetic drugs, glucagon-like peptide-1 (GLP-1) analogues. ATC code A10B J06.
Pharmacological Properties
Pharmacodynamics
Mechanism of Action
Semaglutide is a GLP-1 analogue with 94% homology to human GLP-1. Semaglutide acts as a GLP-1 receptor agonist, selectively binding to and activating GLP-1 receptors, which are the target for native GLP-1.
GLP-1 is a physiological hormone that affects glucose regulation, appetite, and the cardiovascular system through multiple pathways. The effects on glucose concentration and appetite are specifically mediated by GLP-1 receptors located in the pancreas and the brain.
Semaglutide reduces blood glucose levels in a glucose-dependent manner by stimulating insulin secretion and suppressing glucagon secretion under conditions of elevated blood glucose. The glucose-lowering mechanism is also accompanied by a slight delay in gastric emptying during the early postprandial phase. During hypoglycemia, semaglutide reduces insulin secretion and does not interfere with glucagon secretion.
Administration of semaglutide leads to reduction in body weight and fat mass by decreasing caloric intake and reducing appetite. Additionally, semaglutide reduces the craving for high-fat foods.
GLP-1 receptors are also expressed in the heart, vascular system, immune system, and kidneys.
In clinical studies, semaglutide positively influenced plasma lipid levels, reduced systolic blood pressure, and decreased inflammation. In animal trials, semaglutide inhibited the development of atherosclerosis by preventing the progression of aortic plaques and reducing plaque inflammation.
Pharmacodynamic Effects
All pharmacodynamic trials were conducted after 12 weeks of treatment (including dose escalation) at steady state with semaglutide 1 mg administered once weekly.
Fasting and Postprandial Glucose Levels
Semaglutide reduces fasting and postprandial glucose concentrations. In patients with type 2 diabetes, treatment with semaglutide 1 mg led to reductions in glucose concentration in terms of absolute change from baseline (mmol/L) and relative reduction compared to placebo (%) for the following parameters: fasting glucose concentration (1.6 mmol/L; 22%), 2-hour postprandial glucose concentration (4.1 mmol/L; 37%), mean daily glucose concentration (1.7 mmol/L; 22%), and postprandial glucose fluctuation across three meals (0.6–1.1 mmol/L) compared to placebo. Semaglutide reduced fasting glucose levels after the first administration.
Beta-cell Function and Insulin Secretion
Semaglutide improves beta-cell function. Compared to placebo, semaglutide enhanced both first- and second-phase insulin response, with threefold and twofold increases, respectively, and increased maximal secretory capacity of beta cells in patients with type 2 diabetes. Additionally, compared to placebo, treatment with semaglutide led to increased fasting insulin concentration.
Glucagon Secretion
Semaglutide reduces fasting and postprandial glucagon concentrations. In patients with type 2 diabetes, semaglutide treatment resulted in relative reductions in glucagon concentration compared to placebo: fasting glucagon concentration (8–21%), postprandial glucagon response (14–15%), and mean daily glucagon concentration (12%).
Glucose-Dependent Insulin and Glucagon Secretion
Semaglutide reduces high blood glucose levels by stimulating insulin secretion and suppressing glucagon secretion in a glucose-dependent manner. The rate of insulin secretion after semaglutide administration in patients with type 2 diabetes is comparable to that in healthy individuals.
During induced hypoglycemia, semaglutide, compared to placebo, did not alter the counter-regulatory glucagon response and did not enhance the reduction in C-peptide concentration in patients with type 2 diabetes.
Gastric Emptying
Semaglutide causes a slight delay in early postprandial gastric emptying, thereby reducing the rate of glucose entry into the bloodstream during the postprandial period.
Appetite, Caloric Intake, and Food Choice
Compared to placebo, semaglutide reduced caloric intake by 18–35% during three consecutive ad libitum meals. This effect was supported by semaglutide-induced suppression of appetite both in the fasting and postprandial states, improved control over food intake, reduced urge to snack, and relatively lower craving for high-fat foods.
Fasting and Postprandial Lipids
Compared to placebo, semaglutide reduced fasting triglyceride and very-low-density lipoprotein cholesterol (VLDL-C) concentrations by 12% and 21%, respectively. The postprandial triglyceride response and the postprandial VLDL-C response to a high-fat meal were reduced by more than 40%.
Cardiac Electrophysiology (QTc)
The effect of semaglutide on cardiac repolarization was evaluated in a thorough QTc study. Semaglutide did not prolong QTc intervals at doses up to 1.5 mg at steady state.
Clinical Efficacy and Safety
Both improved glycemic control and reduced cardiovascular morbidity and mortality are essential components of type 2 diabetes therapy.
The efficacy and safety of semaglutide at doses of 0.5 mg and 1 mg once weekly were evaluated in six phase 3a randomized, controlled clinical trials involving 7,215 patients with type 2 diabetes (4,107 patients received semaglutide). The primary objective of five clinical trials (SUSTAIN 1–5) was to assess glycemic control efficacy, while one trial (SUSTAIN 6) focused on cardiovascular outcomes.
An additional phase 3b clinical trial (SUSTAIN 7) involving 1,201 patients was conducted to compare the efficacy and safety of semaglutide 0.5 mg and 1 mg once weekly with dulaglutide 0.75 mg and 1.5 mg, respectively, administered once weekly. A phase 3b trial (SUSTAIN 9) was conducted to investigate the efficacy and safety of semaglutide as an add-on to treatment with a sodium-glucose cotransporter-2 inhibitor (SGLT-2i).
Treatment with semaglutide demonstrated sustained, statistically significant, and clinically meaningful reductions in HbA1c and body weight over a period of up to two years compared to placebo and active comparator treatments (sitagliptin, insulin glargine, exenatide ER, and dulaglutide).
The efficacy of semaglutide was independent of age, sex, race, ethnicity, baseline BMI, baseline body weight (kg), duration of diabetes, and degree of renal impairment.
Target outcomes were achieved across all randomized patient groups (analyses based on mixed models for repeated measures or multiple imputation).
Additionally, a phase 3b study (SUSTAIN 11) was conducted to evaluate the effect of semaglutide compared to insulin aspart as an add-on to metformin and optimized insulin glargine (100 U).
More detailed information is provided below.
SUSTAIN Trials 1. Monotherapy
In a double-blind, placebo-controlled clinical trial lasting 30 weeks, 388 patients with inadequate disease control on diet and exercise were randomized to receive once-weekly semaglutide 0.5 mg or 1 mg, or placebo.
Table 1
SUSTAIN Study 1: Results at Week 30
| Parameter |
Semaglutide 0.5 mg |
Semaglutide 1 mg |
Placebo |
| Number of patients |
128 |
130 |
129 |
| HbA1c (%) |
|||
| At baseline (mean value) |
8.1 |
8.1 |
8.0 |
| Change from baseline to week 30 |
-1.5 |
-1.6 |
0 |
| Difference vs placebo (95 % CI) |
-1.4 [-1.7, -1.1]a |
-1.5 [-1.8, -1.2]a |
- |
| Patients (%) achieving HbA1c < 7 % |
74 |
72 |
25 |
| Fasting plasma glucose (mmol/L) |
|||
| At baseline (mean value) |
9.7 |
9.9 |
9.7 |
| Change from baseline to week 30 |
-2.5 |
-2.3 |
-0.6 |
| Body weight (kg) |
|||
| At baseline (mean value) |
89.8 |
96.9 |
89.1 |
| Change from baseline to week 30 |
-3.7 |
-4.5 |
-1.0 |
| Difference vs placebo (95 % CI) |
-2.7 [-3.9, -1.6]a |
-3.6 [-4.7, -2.4]a |
- |
a p < 0.0001 (two-sided) for superiority.
SUSTAIN 2 Clinical Trial. Semaglutide compared with sitagliptin, both in combination with one or two oral antidiabetic medicinal products (metformin and/or thiazolidinediones)
In a double-blind, active-controlled study lasting 56 weeks, 1231 patients were randomized to receive either semaglutide 0.5 mg once weekly or 1 mg once weekly, or sitagliptin 100 mg once daily; all in combination with metformin (94%) and/or thiazolidinediones (6%).
Table 2
SUSTAIN 2 Study: Results at Week 56
| Parameter |
Semaglutide 0.5 mg |
Semaglutide 1 mg |
Sitagliptin 100 mg |
| Number of patients |
409 |
409 |
407 |
| HbA1c (%) |
|||
| Baseline (mean value) |
8.0 |
8.0 |
8.2 |
| Change from baseline to week 56 |
-1.3 |
-1.6 |
-0.5 |
| Difference compared to sitagliptin (95 % CI) |
-0.8 [-0.9, -0.6]a |
-1.1 [-1.2, -0.9]a |
- |
| Patients (%) achieving HbA1c < 7 % |
69 |
78 |
36 |
| Fasting plasma glucose (mmol/L) |
|||
| Baseline (mean value) |
9.3 |
9.3 |
9.6 |
| Change from baseline to week 56 |
-2.1 |
-2.6 |
-1.1 |
| Body weight (kg) |
|||
| Baseline (mean value) |
89.9 |
89.2 |
89.3 |
| Change from baseline to week 56 |
-4.3 |
-6.1 |
-1.9 |
| Difference compared to sitagliptin (95 % CI) |
-2.3 [-3.1, -1.6]a |
-4.2 [-4.9, -3.5]a |
- |
p < 0.0001 (two-sided) for superiority.
**
**
Figure 1. Mean change in HbA1c (%) and body weight (kg) from baseline to week 56
SUSTAIN7 clinical trial. Semaglutide compared with dulaglutide, both in combination with metformin
Patients in a 40-week, open-label, randomized clinical trial (1,201 patients) receiving metformin were randomized in a 1:1:1:1 ratio to receive once-weekly semaglutide 0.5 mg or dulaglutide 0.75 mg, or semaglutide 1 mg, or dulaglutide 1.5 mg.
The trial compared outcomes of semaglutide 0.5 mg versus dulaglutide 0.75 mg, and semaglutide 1 mg versus dulaglutide 1.5 mg.
Gastrointestinal disorders were the most common adverse reactions, occurring in a similar proportion of patients receiving semaglutide 0.5 mg (129 patients [43%]), semaglutide 1 mg (133 [44%]), and dulaglutide 1.5 mg (143 [48%]); fewer patients experienced gastrointestinal disorders with dulaglutide 0.75 mg (100 [33%]).
At week 40, increases in pulse rate with semaglutide (0.5 mg and 1 mg) and dulaglutide (0.75 mg and 1.5 mg) were 2.4 and 4.0, and 1.6 and 2.1 beats per minute, respectively.
Table 3
SUSTAIN 7 study: results at week 40
| Parameter |
Semaglutide 0.5 mg |
Semaglutide 1 mg |
Dulaglutide 0.75 mg |
Dulaglutide 1.5 mg |
| Number of patients |
301 |
300 |
299 |
299 |
| HbA1c (%) |
||||
| At baseline (mean value) |
8.3 |
8.2 |
8.2 |
8.2 |
| Change from baseline to week 40 |
-1.5 |
-1.8 |
-1.1 |
-1.4 |
| Difference compared to dulaglutide (95% CI) |
-0.4b [-0.6, -0.2)a |
-0.4c [-0.6, -0.3]a |
- |
- |
| Patients (%) achieving HbA1c < 7% |
68 |
79 |
52 |
67 |
| Fasting plasma glucose (mmol/L) |
||||
| At baseline (mean value) |
9.8 |
9.8 |
9.7 |
9.6 |
| Change from baseline to week 40 |
-2.2 |
-2.8 |
-1.9 |
-2.2 |
| Body weight (kg) |
||||
| At baseline (mean value) |
96.4 |
95.5 |
95.6 |
93.4 |
| Change from baseline to week 40 |
-4.6 |
-6.5 |
-2.3 |
-3.0 |
| Difference compared to dulaglutide (95% CI) |
-2.3b [-3.0, -1.5)a |
-3.6c [-4.3, -2.8]a |
- |
- |
a p < 0.0001 (two-sided) for superiority.
b Semaglutide 0.5 mg compared to dulaglutide 0.75 mg.
c Semaglutide 1 mg compared to dulaglutide 1.5 mg.
**
**
Figure 2. Mean change in HbA1c (%) and body weight (kg) from baseline to week 40
SUSTAIN 3 clinical trial. Semaglutide compared to exenatide ER, both in combination with metformin or metformin with sulfonylurea
In an open-label 56-week trial, 813 patients receiving either metformin only (49%), metformin with sulfonylurea (45%), or other antidiabetic medications (6%) were randomized to receive either semaglutide 1 mg or exenatide ER 2 mg once weekly.
Table 4
SUSTAIN 3 trial: results at week 56
| Parameter |
Semaglutide 1 mg |
Exenatide ER 2 mg |
| Number of patients |
404 |
405 |
| HbA1c (%) |
||
| At baseline (mean value) |
8.4 |
8.3 |
| Change from baseline to Week 56 |
-1.5 |
-0.9 |
| Difference vs exenatide (95% CI) |
-0.6 [-0.8, -0.4]a |
- |
| Patients (%) achieving HbA1c < 7% |
67 |
40 |
| Fasting plasma glucose (mmol/L) |
||
| At baseline (mean value) |
10.6 |
10.4 |
| Change from baseline to Week 56 |
-2.8 |
-2.0 |
| Body weight (kg) |
||
| At baseline (mean value) |
96.2 |
95.4 |
| Change from baseline to Week 56 |
-5.6 |
-1.9 |
| Difference vs exenatide (95% CI) |
-3.8 [-4.6, -3.0]a |
- |
a p < 0.0001 (two-sided) for superiority.
SUSTAIN4 clinical trial. Semaglutide compared with insulin glargine, both in combination with one or two oral antidiabetic agents (metformin or metformine with sulfonylurea)
In a 30-week open-label trial with an active comparator, 1089 patients were randomized to receive either once-weekly semaglutide 0.5 mg, once-weekly semaglutide 1 mg, or once-daily insulin glargine, all in combination with metformin (48%) or metformin plus sulfonylurea (51%).
Table 5
SUSTAIN 4 study: results at week 30
| Parameter |
Semaglutide 0.5 mg |
Semaglutide 1 mg |
Insulin glargine |
| Number of patients |
362 |
360 |
360 |
| HbA1c (%) |
|||
| At baseline (mean value) |
8.1 |
8.2 |
8.1 |
| Change from baseline to week 30 |
-1.2 |
-1.6 |
-0.8 |
| Difference vs. insulin glargine (95% CI) |
-0.4 [-0.5, -0.2]a |
-0.8 [-1.0, -0.7]a |
- |
| Patients (%) achieving HbA1c < 7% |
57 |
73 |
38 |
| Fasting plasma glucose (mmol/L) |
|||
| At baseline (mean value) |
9.6 |
9.9 |
9.7 |
| Change from baseline to week 30 |
-2.0 |
-2.7 |
-2.1 |
| Body weight (kg) |
|||
| At baseline (mean value) |
93.7 |
94.0 |
92.6 |
| Change from baseline to week 30 |
-3.5 |
-5.2 |
+1.2 |
| Difference vs. insulin glargine (95% CI) |
-4.6 [-5.3, -4.0]a |
-6.34 [-7.0, -5.7]a |
- |
a p < 0.0001 (two-sided) for superiority.
SUSTAIN5 clinical trial. Semaglutide compared to placebo, both in combination with basal insulin
In a double-blind, placebo-controlled trial lasting 30 weeks, 397 patients with inadequate glycemic control on basal insulin, with or without metformin, were randomized to receive either semaglutide 0.5 mg once weekly, semaglutide 1 mg once weekly, or placebo.
Table 6
SUSTAIN 5 trial: results at week 30
| Parameter |
Semaglutide 0.5 mg |
Semaglutide 1 mg |
Placebo |
| Number of patients |
132 |
131 |
133 |
| HbA1c (%) |
|||
| At baseline (mean value) |
8.4 |
8.3 |
8.4 |
| Change from baseline to week 30 |
-1.4 |
-1.8 |
-0.1 |
| Difference vs placebo (95% CI) |
-1.4 [-1.6, -1.1]a |
-1.8 [-2.0, -1.5]a |
- |
| Patients (%) achieving HbA1c < 7% |
61 |
79 |
11 |
| Fasting plasma glucose (mmol/L) |
|||
| At baseline (mean value) |
8.9 |
8.5 |
8.6 |
| Change from baseline to week 30 |
-1.6 |
-2.4 |
-0.5 |
| Body weight (kg) |
|||
| At baseline (mean value) |
92.7 |
92.5 |
89.9 |
| Change from baseline to week 30 |
-3.7 |
-6.4 |
-1.4 |
| Difference vs placebo (95% CI) |
-2.3 [-3.3, -1.3]a |
-5.1 [-6.1, -4.0]a |
- |
a p < 0.0001 (two-sided) for superiority.
SUSTAIN9 clinical trial. Semaglutide compared with placebo, both as add-on to SGLT2 inhibitor ± metformin or sulphonylurea
In a double-blind, placebo-controlled trial of 30 weeks’ duration, 302 patients with inadequate glycaemic control on an SGLT2 inhibitor with or without metformin or sulphonylurea were randomized to receive either once-weekly semaglutide 1.0 mg or placebo.
Table 7
SUSTAIN 9 trial: results at week 30
| Parameter |
Semaglutide 1 mg |
Placebo |
| Number of patients |
151 |
151 |
| HbA1c (%) |
||
| At baseline (mean value) |
8.0 |
8.1 |
| Change from baseline to Week 30 |
-1.5 |
-0.1 |
| Difference vs placebo (95% CI) |
-1.4 [-1.6, -1.2]a |
- |
| Patients (%) achieving HbA1c < 7% |
|
|
| Fasting plasma glucose (mmol/L) |
||
| At baseline (mean value) |
9.1 |
8.9 |
| Change from baseline to Week 30 |
-2.2 |
|
| Body weight (kg) |
||
| At baseline (mean value) |
89.6 |
93.8 |
| Change from baseline to Week 30 |
-4.7 |
-0.9 |
| Difference vs placebo (95% CI) |
-3.8 [-4.7, -2.9]a |
- |
a p < 0.0001 (two-sided) for superiority, adjusted for multiplicity based on hierarchical testing of HbA1c and body weight.
Clinical Study SUSTAIN11 – Semaglutide compared to insulin aspart as add-on to insulin glargine + metformin
In a 52-week open-label study, 1748 patients with inadequately controlled type 2 diabetes after a 12-week period of insulin glargine and metformin were randomized in a 1:1 ratio to receive once-weekly semaglutide (0.5 mg or 1.0 mg) or insulin aspart three times daily. The enrolled population had a mean diabetes duration of 13.4 years and a mean HbA1c of 8.6%, with a target HbA1c of 6.5–7.5%.
Treatment with semaglutide led to a reduction in HbA1c at week 52 (-1.5% for semaglutide compared to -1.2% for insulin aspart).
The number of severe hypoglycemic episodes was low in both treatment groups (4 episodes with semaglutide compared to 7 episodes with insulin aspart).
Mean baseline body weight decreased with semaglutide (-4.1 kg) and increased with insulin aspart (+2.8 kg), with a treatment-dependent difference of -6.99 kg (95% CI: -7.41 to -6.57) at week 52.
Combination use with sulfonylurea monotherapy
In the SUSTAIN 6 clinical trial (see section "Cardiovascular disease"), 123 patients were initially on sulfonylurea monotherapy. Baseline HbA1c was 8.2%, 8.4%, and 8.4% in the semaglutide 0.5 mg, semaglutide 1 mg, and placebo groups, respectively. After 30 weeks, HbA1c decreased by 1.6% and 1.5% with semaglutide 0.5 mg and 1 mg, respectively, and increased by 0.1% with placebo.
Combination use with premixed insulin ± one or two oral glucose-lowering agents (OGLAs)
In the SUSTAIN 6 study (see section "Cardiovascular disease"), 867 patients were on premixed insulin (at baseline with or without OGLAs). Baseline HbA1c was 8.8%, 8.9%, and 8.9% in the semaglutide 0.5 mg, semaglutide 1 mg, and placebo groups, respectively. After 30 weeks, HbA1c decreased by 1.3%, 1.8%, and 0.4% with semaglutide 0.5 mg, semaglutide 1 mg, and placebo, respectively.
Cardiovascular disease
In a double-blind, 104-week clinical trial (SUSTAIN 6), 3297 patients with type 2 diabetes and high cardiovascular risk were randomized to receive once-weekly semaglutide 0.5 mg or 1 mg or placebo, in addition to standard therapy, over the following 2 years. Overall, 98% of patients completed the trial, and vital signs data were available for 99.6% at the end.
The study population was distributed by age as follows: 1598 patients (48.5%) aged ≥65 years, 321 (9.7%) aged ≥75 years, and 20 (0.6%) aged ≥85 years. Renal function was normal or mildly impaired in 2358 patients, moderately impaired in 832 patients, and severely impaired or at end-stage renal disease in 107 patients. The population included 61% men, with a mean age of 65 years and a mean BMI of 33 kg/m². Mean duration of diabetes was 13.9 years.
The primary endpoint was time from randomization to first occurrence of a major adverse cardiovascular event (MACE): cardiovascular death, non-fatal myocardial infarction, or non-fatal stroke.
The total number of events for the composite primary endpoint MACE was 254, including 108 (6.6%) with semaglutide and 146 (8.9%) with placebo. See Figure 4 for results on primary and secondary cardiovascular endpoints. Treatment with semaglutide resulted in a 26% reduction in the risk of the composite primary endpoint of cardiovascular death, non-fatal myocardial infarction, and non-fatal stroke. The total number of cardiovascular deaths, non-fatal myocardial infarctions, and non-fatal strokes were 90, 111, and 71, respectively, including 44 (2.7%), 47 (2.9%), and 27 (1.6%) events, respectively, with semaglutide (Figure 4). The risk reduction in the primary composite endpoint was primarily driven by a reduction in non-fatal stroke (39%) and non-fatal myocardial infarction (26%) (Figure 3).
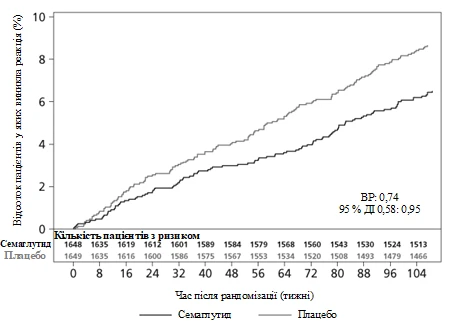
Figure 3. Kaplan-Meier curve for time to first occurrence of the composite event: cardiovascular death, non-fatal myocardial infarction, and non-fatal stroke (SUSTAIN 6 clinical trial).
**
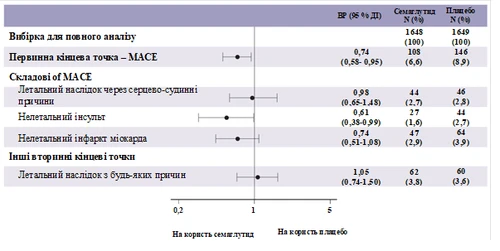
**
Figure 4. Forest plot: time to first occurrence of the composite event, its components, and all-cause mortality (SUSTAIN 6 study)
A total of 158 cases of new-onset or worsening nephropathy were recorded. The HR [95% CI] for time to nephropathy, defined as persistent macroalbuminuria (first occurrence of persistent macroalbuminuria, persistent doubling of serum creatinine, need for continuous renal replacement therapy, or death due to kidney disease), was 0.64 [0.46; 0.88].
Body weight
After one year of treatment, body weight loss of ≥5% and ≥10% was observed in a higher proportion of patients receiving semaglutide 0.5 mg (46% and 13%) and 1 mg (52–62% and 21–24%) compared to those receiving the active comparators sitagliptin (18% and 3%) and exenatide ER (17% and 4%).
In a 40-week head-to-head study versus dulaglutide, a higher proportion of patients achieved body weight loss of ≥5% and ≥10% with semaglutide 0.5 mg (44% and 14%) compared to dulaglutide 0.75 mg (23% and 3%), and with semaglutide 1 mg (up to 63% and 27%) compared to dulaglutide 1.5 mg (30% and 8%).
In the SUSTAIN 6 clinical trial, significant and sustained reductions in body weight from baseline to week 104 were observed with semaglutide 0.5 mg and 1 mg compared to placebo, when added to standard therapy (-3.6 kg and -4.9 kg vs. -0.7 kg and -0.5 kg, respectively).
Arterial blood pressure
A significant reduction in mean systolic blood pressure was observed with semaglutide 0.5 mg (3.5–5.1 mmHg) and 1 mg (5.4–7.3 mmHg) when used in combination with oral antidiabetic agents or basal insulin. No significant difference in diastolic blood pressure was observed between semaglutide treatment and comparator agents.
Children
The European Medicines Agency has deferred the obligation to submit the results of studies with the medicinal product Ozempic® in one or more pediatric subgroups for the treatment of type 2 diabetes (see section "Dosage and administration").
Pharmacokinetics
Compared to native GLP-1, semaglutide has a prolonged elimination half-life of approximately 1 week, enabling once-weekly subcutaneous administration. The primary mechanism behind this prolonged action is albumin binding, which reduces renal clearance and protects against metabolic degradation. Additionally, semaglutide is stabilized against degradation by the enzyme DPP-4.
Absorption
Maximum concentration is reached within 1–3 days after administration. Steady-state concentration is achieved after 4–5 weeks of once-weekly dosing. In patients with type 2 diabetes, mean steady-state concentrations after subcutaneous administration of 0.5 mg and 1 mg semaglutide were approximately 16 nmol/L and 30 nmol/L, respectively. Exposure increased in a dose-dependent manner with doses of 0.5 mg and 1 mg. Similar exposure was achieved with subcutaneous administration in the abdomen, thigh, or upper arm. Absolute bioavailability after subcutaneous administration was 89%.
Distribution
Mean volume of distribution after subcutaneous administration in patients with type 2 diabetes was approximately 12.5 L. Semaglutide is highly bound to plasma albumin (>99%).
Metabolism
Prior to excretion, semaglutide is actively metabolized via proteolytic cleavage of the peptide backbone and subsequent beta-oxidation of the fatty acid side chain. Neutral endopeptidase (NEP) is believed to be involved in semaglutide metabolism.
Excretion
In a study with subcutaneous administration of a single radiolabeled dose of semaglutide, semaglutide-related material was excreted primarily via urine and feces; approximately 2/3 was excreted in urine and approximately 1/3 in feces. Approximately 3% of the administered dose was excreted unchanged in urine. In patients with type 2 diabetes, semaglutide clearance was approximately 0.05 L/h. With an elimination half-life of approximately 1 week, semaglutide remains in circulation for about 5 weeks after the last dose.
Special patient populations
Elderly patients
Based on data from phase 3a trials involving patients aged 20–86 years, age does not influence the pharmacokinetics of semaglutide.
Gender, race, and ethnicity
Gender, race (Caucasian, African, or Asian), and ethnicity (Hispanic or Latino, non-Hispanic or non-Latino) do not influence the pharmacokinetics of semaglutide.
Body weight
Body weight influences semaglutide exposure. Higher body weight leads to lower exposure; a 20% difference in individual body weight results in nearly a 16% difference in exposure. Semaglutide doses of 0.5 mg and 1 mg provide adequate systemic exposure across a body weight range of 40–198 kg.
Renal impairment
Renal impairment does not clinically significantly affect the pharmacokinetics of semaglutide. This was demonstrated after a single 0.5 mg dose of semaglutide in patients with mild, moderate, severe renal impairment, or on dialysis, compared to patients with normal renal function. This was also confirmed by phase 3a clinical trial data in patients with type 2 diabetes and renal impairment, although experience in patients with end-stage renal disease is limited.
Hepatic impairment
Hepatic impairment does not affect semaglutide exposure. Pharmacokinetics of semaglutide were evaluated after a single 0.5 mg dose in patients with mild, moderate, or severe hepatic impairment compared to patients with normal liver function.
Children
Studies of semaglutide in pediatric patients have not been conducted.
Non-clinical safety data
Non-clinical data based on studies of pharmacological safety, repeat-dose toxicity, and genotoxicity revealed no risk for humans.
Non-lethal tumors derived from C-cells of the thyroid gland observed in rodents are effects typical of the class of GLP-1 receptor agonists. In a 2-year carcinogenicity study in rats and mice, semaglutide caused C-cell thyroid tumors at clinically relevant exposure levels. No other treatment-related tumors were observed. The tumors in rodents are caused by a non-genotoxic, GLP-1 receptor-mediated mechanism to which rodents are partially sensitive. The relevance of this mechanism to humans is considered low but cannot be entirely excluded.
In fertility studies in rats, semaglutide did not affect mating performance or fertility in males. In female rats, prolonged estrous cycle duration and a slight reduction in corpora lutea (ovulation) were observed at doses associated with body weight loss.
In embryo-fetal development studies in rats, semaglutide caused embryotoxic effects at exposures below clinically relevant levels. Semaglutide caused marked body weight loss in females and reduced embryonic survival and growth. Fetal skeletal and visceral malformations were observed, including changes in long bones, ribs, spine, tail bones, blood vessels, and brain ventricles. Mechanistic evaluation indicated that the embryotoxic effect involves GLP-1 receptor-mediated impairment of nutrient supply to the embryo via the yolk sac in rats. Due to anatomical and functional differences in the yolk sac across species and lack of GLP-1 receptor expression in the yolk sac of non-human primates, this mechanism is considered unlikely in humans. However, a direct effect of semaglutide on the fetus cannot be ruled out.
In developmental toxicity studies in rabbits and cynomolgus monkeys at clinically relevant exposure levels, increased rates of pregnancy loss and some increase in fetal abnormalities were observed. These effects coincided with marked body weight loss in females, reaching up to 16%. It is unknown whether these effects are related to reduced food intake in females due to direct GLP-1 effects.
Postnatal growth and development were evaluated in cynomolgus monkeys. Offspring were slightly smaller at birth, but body weight normalized during the lactation period.
In young rats, semaglutide caused delayed sexual maturation in both males and females. This delay did not affect fertility or reproductive capacity in either sex, nor the ability of females to maintain pregnancy.
Clinical characteristics
Indications
The medicinal product Ozempic® is indicated for use in inadequately controlled type 2 diabetes mellitus as an adjunct to diet and exercise:
- as monotherapy when metformin is considered inappropriate due to intolerance or contraindications;
- as an adjunct to other antidiabetic medicinal products.
For information on study results of combination therapies, effects on glycemic control and cardiovascular outcomes, as well as patient populations studied, see sections "Special instructions for use", "Interaction with other medicinal products and other forms of interaction", and "Pharmacodynamics".
Contraindications
Hypersensitivity to the active substance or to any of the excipients of the medicinal product (see section "Composition").
Interaction with other medicinal products and other forms of interaction
Semaglutide delays gastric emptying and may affect the rate of absorption of concomitantly administered oral medicinal products. Semaglutide should be used with caution in patients receiving oral medicinal products requiring rapid absorption in the gastrointestinal tract.
Paracetamol
Pharmacokinetic assessment of paracetamol during a standardized meal test showed that semaglutide delays gastric emptying rate. Following concomitant administration of paracetamol with semaglutide 1 mg, AUC0-60min and Cmax of paracetamol decreased by 27% and 23%, respectively. Total exposure to paracetamol (AUC0–5h) remained unchanged. Dose adjustment of paracetamol is not required when administered concomitantly with semaglutide.
Oral contraceptives
A clinically relevant reduction in the efficacy of oral contraceptives is not expected with semaglutide. When administered concomitantly with a combined oral contraceptive medicinal product (ethinylestradiol 0.03 mg / levonorgestrel 0.15 mg), semaglutide did not clinically significantly affect the total exposure to ethinylestradiol and levonorgestrel. Exposure to ethinylestradiol was unaffected; exposure to levonorgestrel increased by 20% at steady state. Cmax of either component was unchanged.
Atorvastatin
Semaglutide did not alter total exposure to atorvastatin following a single 40 mg dose of atorvastatin. Cmax of atorvastatin decreased by 38%. This was considered clinically insignificant.
Digoxin
Semaglutide did not alter total exposure or Cmax of digoxin following administration of a single 0.5 mg dose of digoxin.
Metformin
Semaglutide did not alter total exposure or Cmax of metformin following administration of 500 mg metformin twice daily for 3.5 days.
Warfarin and other coumarin derivatives
Semaglutide did not alter total exposure or Cmax of R- and S-warfarin following administration of a single 25 mg dose of warfarin, and pharmacodynamic parameters of warfarin measured by the international normalized ratio (INR) were not clinically significantly altered. However, cases of decreased INR have been reported during concomitant use of acenocoumarol and semaglutide. Frequent monitoring of INR is recommended at the initiation of semaglutide treatment in patients taking warfarin or other coumarin derivatives.
Special precautions for use
Traceability
In order to improve the traceability of biological medicinal products, the name and batch number of the administered product should be clearly recorded.
Aspiration in combination with general anaesthesia or deep sedation
Cases of pulmonary aspiration have been reported in patients receiving GLP-1 receptor agonists who were under general anaesthesia or deep sedation. Therefore, before undergoing procedures involving general anaesthesia or deep sedation, the increased risk of residual gastric content due to delayed gastric emptying should be considered (see section "Adverse reactions").
General information
Semaglutide should not be used in patients with type 1 diabetes or for the treatment of diabetic ketoacidosis. Semaglutide is not a substitute for insulin. Cases of diabetic ketoacidosis have been reported in insulin-dependent patients who initiated treatment with a GLP-1 receptor agonist and rapidly discontinued or rapidly reduced their insulin dose (see section "Dosage and administration").
There is no clinical experience in treating patients with NYHA class IV heart failure; therefore, semaglutide is not recommended for use in these patients.
Gastrointestinal effects
Treatment with GLP-1 receptor agonists may be associated with gastrointestinal adverse reactions. This should be considered when treating patients with renal impairment, as nausea, vomiting, and diarrhoea may lead to dehydration, which could worsen renal function (see section "Adverse reactions").
Acute pancreatitis
Cases of acute pancreatitis have been observed during treatment with GLP-1 receptor agonists.
Patients should be informed about the typical symptoms of acute pancreatitis. If pancreatitis is suspected, semaglutide should be discontinued; if pancreatitis is confirmed, semaglutide must not be restarted. Semaglutide should be used with caution in patients with a history of pancreatitis.
Hypoglycaemia
The risk of hypoglycaemia may be increased in patients receiving semaglutide in combination with sulphonylureas or insulin. The risk of hypoglycaemia may be reduced by reducing the dose of sulphonylurea or insulin at the initiation of semaglutide treatment (see section "Adverse reactions").
Diabetic retinopathy
An increased risk of complications of diabetic retinopathy has been observed in patients with diabetic retinopathy receiving insulin and semaglutide (see section "Adverse reactions"). Semaglutide should be used with caution in patients with diabetic retinopathy who are receiving insulin. These patients should be closely monitored and managed according to clinical guidelines. Rapid improvement in glucose control has been associated with transient worsening of diabetic retinopathy; however, the possibility of other mechanisms cannot be excluded.
Sodium content
This medicinal product contains less than 1 mmol sodium (23 mg) per dose; therefore, this product can be considered essentially "sodium-free".
Use during pregnancy or breastfeeding
Women of childbearing potential
Women of childbearing potential are advised to use contraception during treatment with semaglutide.
Pregnancy
Animal studies have shown reproductive toxicity (see section "Non-clinical safety data"). Data on the use of semaglutide in pregnant women are limited. Therefore, semaglutide should not be used during pregnancy. If a patient is planning pregnancy or becomes pregnant, semaglutide should be discontinued. Due to the long elimination half-life of semaglutide, treatment should be discontinued at least 2 months prior to planned pregnancy (see section "Pharmacokinetics").
Breastfeeding
Semaglutide passes into milk during lactation in rats. As a potential risk to the breastfed infant cannot be excluded, semaglutide should not be used during breastfeeding.
Fertility
The effect of semaglutide on fertility in humans is unknown. Treatment with semaglutide in male rats did not affect fertility. In female rats, prolonged oestrous cycle and reduced number of ovulations were observed at doses associated with body weight loss (see section "Non-clinical safety data").
Ability to affect the ability to drive and use machines
Semaglutide has no or negligible influence on the ability to drive or use machines. However, when used in combination with sulphonylureas or insulin, patients should be advised to take precautions to avoid hypoglycaemia while driving or operating machinery (see section "Special precautions for use").
Method of Administration and Dosage
Dosage
The initial dose is 0.25 mg of semaglutide once weekly. After 4 weeks, the dose should be increased to 0.5 mg once weekly. For further improvement of glycemic control after at least 4 weeks of treatment with 0.5 mg once weekly, the dose may be increased to 1 mg once weekly.
The 0.25 mg dose of semaglutide is not a maintenance dose. Weekly doses exceeding 1 mg are not recommended.
When Ozempic® is added to ongoing treatment with metformin and/or thiazolidinedione or a sodium-glucose cotransporter-2 inhibitor (SGLT2 inhibitor), the current dose of metformin and/or thiazolidinedione or SGLT2 inhibitor may remain unchanged.
When Ozempic® is added to ongoing treatment with a sulfonylurea or insulin, consideration should be given to reducing the dose of sulfonylurea or insulin to reduce the risk of hypoglycemia (see sections "Side Effects" and "Ability to Influence Reaction Rate When Driving or Operating Machinery").
Dose adjustment of Ozempic® does not require self-monitoring of blood glucose levels. Self-monitoring of blood glucose levels is required for dose adjustment of sulfonylurea and insulin, especially when starting treatment with Ozempic® and when reducing insulin dose. A stepwise insulin dose reduction regimen is recommended.
Missed Dose
If a dose is missed, it should be administered as soon as possible within 5 days of the missed dose. If more than 5 days have passed, the missed dose should be skipped and the next dose administered on the regularly scheduled day. In this way, patients can resume their regular once-weekly dosing schedule.
If necessary, the day of weekly administration may be changed, provided that the interval between two doses is at least 3 days (>72 hours). After selecting a new administration day, continue treatment according to the once-weekly schedule.
Special Patient Populations
Elderly Patients
Dose adjustment based on age is not required. Experience with treatment in patients aged ≥75 years is limited (see section "Pharmacokinetics").
Renal Impairment
Dose adjustment is not required in patients with mild, moderate, or severe renal impairment. Experience with semaglutide in patients with severe renal impairment is limited. Semaglutide is not recommended in patients with end-stage renal disease (see section "Pharmacokinetics").
Hepatic Impairment
Dose adjustment is not required in patients with hepatic impairment. Experience with semaglutide in patients with severe hepatic impairment is limited. Semaglutide should be used with caution in such patients (see section "Pharmacokinetics").
Children
The safety and efficacy of semaglutide in children (under 18 years of age) have not been established. No data are available.
Route of Administration
For subcutaneous use only.
Ozempic® is administered subcutaneously in the abdominal area, thigh, or upper arm. The injection site may be rotated without dose adjustment. Ozempic® must not be administered intravenously or intramuscularly.
Ozempic® should be administered once weekly at any time of day, independent of meals.
For further information on administration, see section "Handling and Disposal Precautions".
Handling and Disposal Precautions
Patients should be advised to dispose of the needle after each injection and to store the pen without an attached needle. This may prevent needle clogging, contamination, infection, leakage of solution, and inaccurate dosing. Needles and other waste should be disposed of according to local requirements. The pen is intended for individual use only. Ozempic® should not be used if it is not clear and colorless or almost colorless. Do not use after freezing. The pen is designed to be used with NovoFine® or NovoTwist® disposable needles up to 8 mm in length. NovoFine® Plus needles are included in the product packaging.
| Instructions for using the Ozempic® pen device 1 mg (injectable solution in a pre-filled pen). |
||
| For detailed information, refer to the package leaflet before using the Ozempic® pen. Discuss with your doctor, nurse, or pharmacist how to properly administer Ozempic®. Begin using the medicine by checking the pen device to ensure it contains Ozempic® at a strength of 1 mg. Then review the illustrations below to learn about the different parts of the pen and the needle. If the patient cannot see at all or has poor vision and is unable to read the dose counter on the pen device, the pen must not be used without assistance from another person. Assistance must be provided by someone with good vision who knows how to use the pre-filled Ozempic® pen device. The pen device is pre-filled and has a dose selection mechanism. It contains 4 mg of semaglutide; you can only select a dose of 1 mg. One new pen device contains four doses of 1 mg each. Use the table inside the lid of the carton to track how many injections you have administered and when they were given: You should indicate the day of the week chosen for administration Important information Pay special attention to these notes, as they are important for the safe use of the pen. Also: Open here Lift here |
|
|
|
||
|
|
|
Look through the cartridge scale window. If the solution is cloudy or discolored, the pen must not be used. |
|
|
Check whether the paper seal or the outer needle cap is damaged, as this may indicate loss of sterility. If there is any damage, use a new needle.
|
|
|
| Ensure the needle is properly attached.
|
|
|
| The needle is covered by two caps. Both caps must be removed. If you forget to remove both caps, you will not administer the solution.
|
|
|
A drop of solution may appear at the tip of the needle. This is normal, but you must check medicine flow when using a new pen for the first time. See step 2, "Checking solution flow with each new pen device." Do not attach a new needle until you are ready to administer the injection. |
|
|
| Always use a new needle for each injection. This helps prevent needle blockage, contamination, infection, and incorrect dosing. |
||
| Never use a needle if it is bent or damaged. |
||
|
||
|
|
|
Press and hold the dose button until the dose counter returns to "0". "0" should align with the dose pointer. A drop of solution should appear at the needle tip. |
|
|
| A small drop may remain at the needle tip, but it will not be injected. If no drop appears, repeat step 2 "Checking solution flow with a new pen device" up to 6 times. If still no drop appears, change the needle and repeat the steps described in step 2 "Checking solution flow with a new pen device" once more. If no drop appears after that, dispose of the pen and use a new one. |
||
| You must always ensure a drop appears at the needle tip before first use of a new pen. This ensures the solution will be delivered. If no drop appears, do not use the pen, even if the dose counter changes value. This may indicate a blocked or damaged needle. If you do not check flow before the first injection of a new pen, you may not receive the required dose of solution needed for the desired effect of Ozempic®. |
||
|
||
Turn the dose selector until the dose counter stops and displays 1 mg. |
|
|
| Only the dose counter and dose pointer will show that you have selected 1 mg for injection. You can only select 1 mg of medicine per dose. If this pen contains less than 1 mg of medicine, the dose counter will stop before reaching 1. When turning the selector forward, backward, or beyond the selected 1 mg dose indicator, the pen clicks differently. Do not count the number of clicks. |
||
| Always use the dose counter and dose pointer to confirm you have selected 1 mg before administering the medicine. Do not count the number of pen clicks. The 1 mg dose must exactly align with the dose pointer to ensure correct dosing. |
||
| Remaining solution in the pen device |
||
|
|
|
| If there is insufficient solution for a full dose, do not use the pen. Use a new Ozempic® pen. |
||
|
||
|
|
|
Observe until the dose counter returns to "0". "0" should align with the dose pointer. You may then hear or feel a click.
|
|
|
|
|
|
If a drop of blood appears at the injection site, gently press the area. |
|
|
| A drop of solution may be visible at the needle tip after injection. This is normal and does not affect the volume of dose administered. |
||
| Always look at the dose pointer to see how many milligrams of solution you have administered. Keep the injection button pressed until the dose pointer returns to "0". How to identify a blocked or damaged needle.
What to do with a blocked needle. Remove the needle as described in step 5 "After injection" and repeat all steps starting from step 1 "Preparing the pen device with a new needle for use". Never touch the dose counter during medicine administration. This may interrupt the injection. |
||
|
||
| Always dispose of the needle after each injection to ensure ease of use and prevent using a blocked needle. If the needle is blocked, you will not be able to administer the medicine.
|
|
|
|
|
|
|
|
|
| When the pen is empty, dispose of it without the needle according to instructions from your doctor, nurse, pharmacist, or local regulations. |
||
| Never attempt to reattach the inner needle cap to the needle. You may injure yourself with the needle. Always remove the needle from the pen after each injection. This helps prevent needle blockage, contamination, infection, leakage of solution, and inaccurate dosing. |
||
| Additional important information. |
||
|
||
| Caring for the pen device. |
||
| Handle your pen device carefully. Careless handling or incorrect use may result in incorrect dosing. If this occurs, you may not achieve the desired effect from this medicine. |
||
|
||





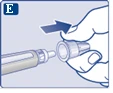




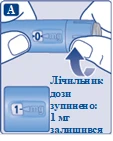





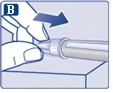

Children
The safety and efficacy of semaglutide in children (under 18 years of age) have not been established. Data are lacking.
The European Medicines Agency has deferred the obligation to submit the results of studies with semaglutide in one or more paediatric subgroups for the treatment of type 2 diabetes (see section "Posology and method of administration").
Overdose
During clinical trials, overdose was reported with doses up to 4 mg following a single administration and up to 4 mg administered over one week. The most commonly reported event was nausea. All patients recovered without complications.
There is no specific antidote for the treatment of semaglutide overdose. In case of overdose, supportive treatment should be administered based on the patient's clinical signs and symptoms. Due to the long elimination half-life of semaglutide of approximately one week, prolonged treatment of symptoms may be required (see section "Pharmacokinetics").
Adverse Reactions
Summary of safety profile
In eight phase 3a clinical trials, 4792 patients received semaglutide at doses up to 1 mg. During clinical trials, adverse reactions most commonly reported were gastrointestinal in nature, including nausea (very common), diarrhea (very common), and vomiting (common). Overall, these reactions were of mild or moderate severity and transient.
Adverse Reactions
The adverse reactions listed below were observed in all Phase 3a trials in patients with type 2 diabetes (described in more detail in the section “Pharmacodynamics”). The frequency of adverse reactions is based on pooled data from Phase 3a clinical trials, except for cardiovascular outcomes trials (see below for additional information).
Adverse reactions are classified by system organ class and frequency of occurrence. Frequency was assessed using the following scale: very common: (≥ 1/10), common: (≥ 1/100 to < 1/10), uncommon: (≥ 1/1,000 to < 1/100), rare: (≥ 1/10,000 to < 1/1,000), very rare: (< 1/10,000), not known: (cannot be estimated from available data). Within each group, adverse reactions are listed in decreasing order of severity.
Immune system disorders: uncommon – hypersensitivityc; rare – anaphylactic reaction.
Metabolism and nutrition disorders: very common – hypoglycaemiaa when used in combination with insulin or sulphonylureas; common – hypoglycaemiaa when used in combination with other oral antidiabetic medicinal products, decreased appetite.
Nervous system disorders: common – dizziness; uncommon – dysgeusia.
Eye disorders: common – complications of diabetic retinopathyb.
Cardiac disorders: uncommon – increased heart rate.
Gastrointestinal disorders: very common – nausea, diarrhoea; common – vomiting, abdominal pain, abdominal distension, constipation, dyspepsia, gastritis, gastroesophageal reflux disease, belching, flatulence; uncommon – acute pancreatitis, delayed gastric emptying; not known – intestinal obstructiond.
Hepatobiliary disorders: common – cholelithiasis.
Skin and subcutaneous tissue disorders: not known – angioedemad.
General disorders and administration site conditions: common – fatigue; uncommon – injection site reactions.
Investigations: common – increased lipase levels, increased amylase levels, decreased body weight.
a Hypoglycaemia was defined as severe (requiring assistance from another person) or symptomatic event with a concurrent blood glucose measurement < 3.1 mmol/L.
b Complications of diabetic retinopathy include the following composite: retinal photocoagulation, treatment with intravitreal injection agents, vitreous haemorrhage, blindness due to diabetes (uncommon). The frequency of events was determined based on data from the cardiovascular outcomes trial.
c General term including also adverse reactions related to hypersensitivity, such as rash and urticaria.
d Reports from the post-marketing period.
Cardiovascular outcomes and 2-year safety trial
In patients at high risk of cardiovascular disease, the adverse reaction profile was similar to that observed in other Phase 3a trials (described in the section “Pharmacodynamics”).
Description of selected adverse reactions
Hypoglycaemia
No episodes of severe hypoglycaemia were observed when semaglutide was used as monotherapy. Severe hypoglycaemia was mainly observed when semaglutide was used concomitantly with sulphonylureas (1.2% of patients; 0.03 events per patient-year) or insulin (1.5% of patients; 0.02 events per patient-year). A few episodes (0.1% of patients; 0.001 events per patient-year) were observed when semaglutide was used in combination with oral antidiabetic medicinal products other than sulphonylureas.
The American Diabetes Association classified hypoglycaemia in 11.3% of patients (0.3 events per patient-year) receiving semaglutide 1.0 mg in combination with DPP-4 inhibitors in the SUSTAIN 9 trial, compared to 2.0% of patients (0.04 events per patient-year) receiving placebo. Severe hypoglycaemia was reported in 0.7% (0.01 events per patient-year) and 0% of patients, respectively.
Gastrointestinal adverse reactions
Nausea was observed in 17.0% and 19.9% of patients receiving semaglutide 0.5 mg and 1 mg, respectively, diarrhoea in 12.2% and 13.3%, and vomiting in 6.4% and 8.4%. Most cases were mild to moderate in severity and transient. These reactions led to discontinuation of treatment in 3.9% and 5% of patients, respectively. Reactions were most frequently reported during the first months of treatment.
Patients with low body weight may experience a higher number of gastrointestinal disorders when treated with semaglutide.
In the SUSTAIN 9 trial, constipation and gastroesophageal reflux disease were observed in 6.7% and 4% of patients, respectively, receiving semaglutide 1.0 mg when used concomitantly with DPP-4 inhibitors, compared to no events in patients receiving placebo. The prevalence of these events did not decrease over time.
Acute pancreatitis
The incidence of confirmed acute pancreatitis observed during Phase 3a clinical trials was 0.3% with semaglutide and 0.2% with the comparator. In the 2-year cardiovascular outcomes trial, the incidence of expert-adjudicated acute pancreatitis was 0.5% with semaglutide and 0.6% with placebo (see section “Special warnings and precautions for use”).
Complications of diabetic retinopathy
A 2-year clinical trial included 3,297 patients with type 2 diabetes, high cardiovascular risk, long duration of diabetes, and inadequate glycaemic control. In this trial, confirmed events of complications of diabetic retinopathy occurred in more patients receiving semaglutide (3.0%) than in those receiving placebo (1.8%). This was observed in patients with confirmed diabetic retinopathy who were receiving insulin. The difference between treatment groups emerged early and persisted throughout the trial. Systematic assessment of complications of diabetic retinopathy was performed only in the cardiovascular outcomes trial. In a 1-year clinical trial involving 4,807 patients with type 2 diabetes, the proportion of patients with adverse reactions related to diabetic retinopathy was similar in the semaglutide group (1.7%) and the comparator group (2.0%).
Discontinuation of treatment due to adverse reactions
The frequency of treatment discontinuation due to adverse events was 6.1% and 8.7% in patients receiving semaglutide 0.5 mg and 1 mg, respectively, compared to 1.5% in those receiving placebo. The most common adverse reactions leading to treatment discontinuation were gastrointestinal disorders.
Injection site reactions
Injection site reactions (such as rash, erythema at injection site) were reported in 0.6% and 0.5% of patients receiving semaglutide 0.5 mg and 1 mg, respectively. These reactions were generally mild.
Immunogenicity
Due to the potential for immunogenic properties of medicinal products containing proteins or peptides, there is a possibility of antibody formation in patients during treatment with semaglutide. The percentage of patients with positive antibody test results for semaglutide at any time after initiation of treatment was low (1–2%), and no patients had neutralising antibodies to semaglutide or antibodies with neutralising GLP-1 effect by the end of clinical trials.
Increased heart rate
An increase in heart rate has been observed with GLP-1 receptor agonists. In Phase 3a clinical trials, patients receiving Ozempic® experienced a mean increase in heart rate of 1 to 6 beats per minute (bpm) from a baseline of 72–76 bpm. In a long-term trial involving patients with risk factors for cardiovascular disease, after 2 years of treatment, 16% of patients receiving Ozempic® had an increase in heart rate of > 10 bpm compared to 11% of patients receiving placebo.
Reporting of suspected adverse reactions
It is important to report suspected adverse reactions after marketing authorisation. This allows continued monitoring of the benefit-risk balance of the medicinal product. Healthcare professionals are encouraged to report suspected adverse reactions via the national reporting system.
Shelf life
Before first use – 3 years.
After first use – 6 weeks.
After first use, store below 30 °C or in a refrigerator (2–8 °C). Do not freeze.
Store the pen with the cap attached to protect from light.
Storage conditions
Before first use: store in a refrigerator (2–8 °C), not too close to the freezer compartment. Do not freeze. Do not use after freezing.
Store the pen with the cap attached to protect from light.
Storage conditions after first opening are described in the section “Shelf life”.
Keep out of the reach and sight of children.
Incompatibilities
As compatibility studies have not been conducted, this medicinal product must not be mixed with other medicinal products.
Packaging
Pre-filled multi-dose single-use pen, made of polypropylene, polyoxymethylene, polycarbonate and acrylonitrile butadiene styrene, containing a cartridge (type I glass), sealed on one side with a rubber (chlorobutyl) plunger and on the other side with an aluminium cap with laminated rubber seal (bromobutyl / polyisoprene).
The pen contains 3.0 mL of solution, allowing administration of doses of 1.0 mg. The pack contains 1 pre-filled pen and 4 NovoFine® Plus disposable needles in a cardboard box.
Prescription status. Prescription only.
Manufacturer
A/S Novo Nordisk.
Manufacturer’s address
Novo Allé
2880 Bagsværd
Denmark.
Marketing Authorisation Holder
A/S Novo Nordisk.
Marketing Authorisation Holder’s address
Novo Allé
2880 Bagsværd
Denmark.