Onbryz brezhailler
Ukraine
Table of Contents
INSTRUCTION FOR MEDICAL USE OF THE MEDICINAL PRODUCT. ONBREZ BREEZHALER® (ONBREZ® BREEZHALER®)
Composition:
Active substance: indacaterol maleate;
1 capsule contains indacaterol maleate equivalent to 150 mcg or 300 mcg of indacaterol, corresponding to a delivered dose of 120 mcg or 240 mcg, respectively;
Excipients: lactose monohydrate, gelatin.
Pharmaceutical form. Powder for inhalation, hard capsules.
Main physicochemical properties:
Yellowish-transparent (colorless) size 3 capsules with a black mark «» printed under a black band on the cap and the black inscription «IDL 150» printed above a black band on the body, containing a white to practically white powder;
Yellowish-transparent (colorless) size 3 capsules with a blue mark «» printed under a blue band on the cap and the blue inscription «IDL 300» printed above a blue band on the body, containing a white to practically white powder.
Pharmacotherapeutic group. Adrenergic drugs for inhalation use. Selective beta2-adrenoreceptor agonists.
ATC code R03AC18.
Pharmacological properties.
Pharmacodynamics.
Mechanism of action
The pharmacological effects of beta2-adrenergic receptor agonists are at least partially due to stimulation of intracellular adenylate cyclase, an enzyme that catalyzes the conversion of adenosine triphosphate (ATP) to cyclic-3',5'-adenosine monophosphate (cyclic AMP). Increased levels of cyclic AMP lead to relaxation of bronchial smooth muscle. In vitro studies have shown that indacaterol has long-acting beta2-receptor agonist activity, with 24-fold greater selectivity for beta2-receptors than for beta1-receptors and 20-fold greater selectivity than for beta3-receptors. After inhalation, indacaterol acts locally in the lungs as a bronchodilator. Indacaterol is a partial agonist of human beta2-adrenergic receptors with nanomolar potency. In isolated human bronchus, indacaterol demonstrates rapid onset of action and long duration of effect.
Although beta2-receptors predominate among adrenergic receptors in bronchial smooth muscle, and beta1-receptors predominate in the human heart, beta2-adrenergic receptors are also present in the human heart, accounting for 10–50% of total adrenergic receptors. The precise function of beta2-adrenergic receptors in the human heart is unknown, but their presence increases the likelihood of effects of highly selective beta2-adrenergic agonists on cardiac function.
Pharmacodynamic effects
Onbrez Breezhaler, administered once daily at doses of 150 mcg and 300 mcg, provided consistent and significant improvement in lung function (FEV1) over 24 hours in multiple clinical pharmacodynamic and efficacy studies. A rapid onset of action was observed within 5 minutes after inhalation of Onbrez Breezhaler, with an increase in FEV1 from baseline of 110–160 mL compared to the fast-acting beta2-adrenergic agonist salbutamol 200 mcg, and a statistically significantly faster onset of action compared to salmeterol/fluticasone 50/500 mcg. Mean peak improvement in FEV1 from baseline was 250–330 mL at steady state. The bronchodilator effect was independent of the time of dosing (morning or evening).
Onbrez Breezhaler reduced lung hyperinflation, both dynamic and at rest, leading to an increase in inspiratory capacity compared to placebo.
Effects on cardiac electrophysiology
Results from a double-blind, placebo- and active (moxifloxacin)-controlled 2-week study in 404 healthy volunteers demonstrated a maximum mean (90% confidence intervals) QTcF interval prolongation (in ms) of 2.66 (0.55, 4.77), 2.98 (1.02, 4.93), and 3.34 (0.86, 5.82) following multiple doses of the drug (150 mcg, 300 mcg, and 600 mcg, respectively). These findings indicate no risk of proarrhythmic potential related to QT interval prolongation at recommended therapeutic doses or at doses twice the maximum recommended dose. No data on the concentration-effect relationship for delta QTc across the evaluated dose range were obtained.
As demonstrated in a 26-week, double-blind, placebo-controlled Phase III study involving 605 patients with COPD, there was no clinically significant difference in the incidence of arrhythmias during 24-hour monitoring at baseline and at three time points during 26 weeks of treatment between patients receiving recommended doses of Onbrez Breezhaler and those receiving placebo or tiotropium.
Clinical efficacy and safety
The clinical trial program included one 12-week study, two 6-month studies (one of which was extended to one year to assess safety and tolerability), and one one-year randomized controlled study in patients with a clinical diagnosis of COPD. Outcome measures for lung function and health status in the studies included dyspnea, exacerbations, and health-related quality of life.
Lung function
Treatment with Onbrez Breezhaler at doses of 150 mcg and 300 mcg once daily resulted in clinically significant improvement in lung function. In the 12-week primary endpoint (24-hour trough FEV1), treatment with 150 mcg led to an increase of 130–180 mL compared to placebo (p<0.001) and an increase of 60 mL compared to salmeterol 50 mcg twice daily (p<0.001). Treatment with 300 mcg led to an increase of 170–180 mL compared to placebo (p<0.001) and an increase of 100 mL compared to formoterol 12 mcg twice daily (p<0.001). Both doses resulted in an increase of 40–50 mL compared to unblinded tiotropium 18 mcg once daily (150 mcg, p=0.004; 300 mcg, p=0.01).
The 24-hour bronchodilator effect of Onbrez Breezhaler was maintained after the first dose throughout one year of treatment, with no evidence of loss of efficacy (tachyphylaxis).
Symptomatic benefits
Both doses demonstrated statistically significant improvement in disease symptoms compared to placebo—dyspnea and health status assessed by the Transition Dyspnea Index (TDI) and the St. George's Respiratory Questionnaire (SGRQ), respectively. The magnitude of response was generally greater than that observed with active comparator treatments (see Table 1). Additionally, patients receiving Onbrez Breezhaler required significantly less use of rescue medication, had significantly more days without the need for rescue medication, and had a significantly higher percentage of days without daytime symptoms compared to the placebo group.
A combined analysis of 6-month efficacy data showed that the rate of COPD exacerbations was statistically significantly lower than in the placebo group. Compared to placebo, the rate ratios for treatment with Onbrez Breezhaler at doses of 150 mcg and 300 mcg were 0.68 (95% CI [0.47, 0.98]; p-value 0.036) and 0.74 (95% CI [0.56, 0.96]; p-value 0.026), respectively. Experience with the drug in patients of African descent is limited.
Table 1. Symptom relief during 6 months of treatment
| Drug dose (mcg) |
Indacaterol 150 once daily |
Indacaterol 300 once daily |
Tiotropium 18 once daily |
Salmeterol 50 twice daily |
Formoterol 12 twice daily |
Placebo |
| Percentage of patients achieving MCID TDI† |
57a 62b |
71b 59c |
57b |
54a |
54c |
45a 47b 41c |
| Percentage of patients achieving MCID SGRQ† |
53a 58b |
53b 55c |
47b |
49a |
51c |
38a 46b 40c |
| Reduction in number of daily inhalations of rescue medication compared to baseline |
1.3a 1.5b |
1.6b |
1.0b |
1.2a |
NA |
0.3a 0.4b |
| Percentage of days without use of rescue medication |
60a 57b |
58b |
46b |
55a |
NA |
42a 42b |
Study design using:
a indacaterol 150 mcg, salmeterol, and placebo;
b indacaterol 150 and 300 mcg, tiotropium, and placebo;
c indacaterol 300 mcg, formoterol, and placebo.
†MCID – minimal clinically important difference (change in TDI ≥ 1 unit, change in SGRQ ≥ 4 units).
n/a – not assessed over six months.
Pediatric population
The European Medicines Agency has waived the obligation to submit the results of studies with Onbrez Breezhaler in all subgroups of the pediatric population for chronic obstructive pulmonary disease (COPD).
Pharmacokinetics.
Indacaterol is a chiral molecule with R-configuration.
Pharmacokinetic data were obtained from a series of clinical studies conducted in healthy volunteers and patients with COPD.
Absorption
The median time to reach maximum indacaterol serum concentration was approximately 15 minutes after single or repeated inhalation doses. Systemic exposure to indacaterol increased proportionally with dose escalation (from 150 mcg to 600 mcg). The absolute bioavailability of indacaterol after inhalation dosing averaged 43%. Systemic exposure results from a combination of indacaterol absorption in the lungs (approximately 75%) and in the intestine (approximately 25%).
Serum indacaterol concentrations increase with repeated once-daily administration of indacaterol. Steady state is achieved within 12–14 days. The mean accumulation ratio of indacaterol, i.e., AUC over the 24-hour dosing interval on Day 14 compared to Day 1, ranged from 2.9 to 3.5 for inhaled doses of 150 mcg to 600 mcg once daily.
Distribution
Following intravenous infusion, the volume of distribution of indacaterol during the terminal elimination phase was 2557 liters, indicating extensive distribution. In vitro binding of indacaterol to serum and plasma proteins was 94.1–95.3% and 95.1–96.2%, respectively.
Biotransformation
After oral administration of radiolabeled indacaterol in human ADME (absorption, distribution, metabolism, and excretion) studies, unchanged indacaterol was the main component detected in serum, accounting for approximately one-third of the total AUC over 24 hours. The hydroxylated metabolite was the most prominent in serum. The phenolic O-glucuronide of indacaterol and hydroxylated indacaterol were also significant metabolites. Other identified metabolites included the diastereomer of the hydroxylated derivative, N-glucuronide of indacaterol, and C- and N-dealkylated products.
In vitro studies showed that UGT1A1 is the only uridine diphosphate glucuronosyltransferase (UGT) isoform responsible for metabolizing indacaterol to its phenolic O-glucuronide. Oxidative metabolites were formed upon incubation with recombinant CYP1A1, CYP2D6, and CYP3A4. CYP3A4 is considered the predominant isoenzyme involved in the hydroxylation of indacaterol. In vitro studies also showed that indacaterol is a low-affinity substrate for the efflux pump P-gp.
Elimination
In clinical studies including urine analysis, the amount of unchanged indacaterol excreted in urine was generally less than 2% of the dose. Renal clearance of indacaterol averaged 0.46–1.20 L/h. Compared to the serum clearance of indacaterol – 23.3 L/hour – it is evident that renal clearance plays a minor role (approximately 2–5% of systemic clearance) in the elimination of systemically available indacaterol.
In the ADME study involving patients who received oral indacaterol, fecal excretion of indacaterol predominated over urinary excretion. Indacaterol was excreted in human feces mainly as unchanged parent compound (54% of dose) and to a lesser extent as hydroxylated metabolites of indacaterol (23% of dose). Mass balance was complete at ≥ 90% of the administered dose recovered in excreta.
Serum indacaterol concentrations decline in a multi-phasic manner, with a mean terminal half-life ranging from 45.5 to 126 hours. The effective half-life, derived from the accumulation ratio after repeated dosing, ranged from 40 to 52 hours, consistent with the time required to reach steady state (approximately 12–14 days).
Special patient populations
Population pharmacokinetic analysis of data revealed no clinically significant effect of age (adults up to 88 years), sex, body weight (32–168 kg), or race on the pharmacokinetics of indacaterol. This analysis showed no differences between ethnic subgroups within this population.
No relevant changes in Cmax or AUC of indacaterol were observed in patients with mild or moderate hepatic impairment, and no differences in indacaterol protein binding were observed in such patients compared to healthy subjects in control groups. Studies in patients with severe hepatic impairment have not been conducted.
Due to the very low percentage of indacaterol excreted in urine relative to total drug elimination, studies in patients with renal impairment have not been conducted.
Clinical characteristics.
Indications.
Maintenance bronchodilator therapy for airflow obstruction in adult patients with chronic obstructive pulmonary disease (COPD).
Contraindications.
Hypersensitivity to the active substance, lactose, or any of the other excipients.
Interaction with other medicinal products and other forms of interaction.
Sympathomimetic agents
Concomitant use of other sympathomimetic agents (either as monotherapy or as part of combination therapy) may potentiate the adverse effects of Onbrez Breezhaler.
Onbrez Breezhaler should not be used together with other long-acting beta2-adrenergic agonists or medicinal products containing long-acting beta2-adrenergic agonists.
Hypokalaemia
Concomitant treatment with methylxanthine derivatives, corticosteroids, or non-potassium-sparing diuretics may potentiate the possible hypokalaemic effect of beta2-adrenergic agonists and therefore requires caution.
beta-Adrenergic blockers
Beta-adrenergic blockers may attenuate or antagonize the effect of beta2-adrenergic agonists when used concomitantly. Therefore, indacaterol must not be used together with beta-adrenergic blockers (including eye drops), except in cases where their use is clinically justified and necessary. If required, cardioselective beta-blockers should be preferred, although they should still be used with caution.
Interaction with medicinal products that prolong the QT interval
Onbrez Breezhaler, like other beta2-adrenergic agonists, should be used with caution in patients receiving monoamine oxidase inhibitors, tricyclic antidepressants, or medicinal products that prolong the QT interval, due to the potential for increased effects on the QT interval.
Medicinal products that prolong the QT interval may increase the risk of ventricular arrhythmias.
Metabolism and transporters involved in drug interactions
Inhibition of the main clearance pathways of indacaterol—CYP3A4 and P-glycoprotein (P-gp)—does not affect the safety of Onbrez Breezhaler at therapeutic doses. Drug interaction studies have been conducted using potent and specific inhibitors of CYP3A4 and P-glycoprotein (P-gp) (e.g., ketoconazole, erythromycin, verapamil, ritonavir). Administration of verapamil, as a prototype P-glycoprotein (P-gp) inhibitor, resulted in a 1.4- to 2-fold increase in systemic exposure (AUC) of indacaterol and a 1.5-fold increase in Cmax. Concomitant use of Onbrez Breezhaler with erythromycin led to a 1.6-fold increase in systemic exposure and a 1.2-fold increase in Cmax. Administration of ketoconazole, a potent dual inhibitor of P-glycoprotein (P-gp) and CYP3A4, resulted in a doubling of systemic exposure and a 1.4-fold increase in Cmax. Concomitant use with ritonavir, another dual inhibitor of CYP3A4 and P-glycoprotein (P-gp), led to a 1.6- to 1.8-fold increase in systemic exposure and had no effect on Cmax.
The available data collectively indicate that changes in the activity of both P-glycoprotein (P-gp) and CYP3A4 affect systemic clearance. The twofold increase in systemic exposure caused by the potent dual inhibitor ketoconazole reflects the combined inhibitory effect.
The increased exposure due to drug interactions does not compromise the safety of Onbrez Breezhaler, as demonstrated by the clinical experience with Onbrez Breezhaler in clinical trials of up to one year in duration, using doses twice the maximum recommended therapeutic dose.
Indacaterol has not been shown to cause drug interactions with concomitant medications. In vitro studies have shown that indacaterol has a low potential to cause metabolic drug interactions at the systemic level, consistent with clinical experience.
Special precautions for use.
Bronchial asthma
Onbrez Breezhaler is a long-acting beta2-adrenergic agonist indicated only for use in COPD. Onbrez Breezhaler should not be used in bronchial asthma due to lack of data on the long-term outcomes of its use in this condition. Long-acting beta2-adrenergic agonists (LABA) may increase the risk of serious asthma-related adverse events, including death, when used for asthma treatment.
Hypersensitivity
Immediate-type hypersensitivity reactions have been reported after administration of Onbrez Breezhaler. If symptoms suggestive of allergic reactions occur (e.g., difficulty in breathing or swallowing, swelling of the tongue, lips, or face, urticaria, skin rash), Onbrez Breezhaler should be discontinued immediately and alternative therapy initiated.
Paradoxical bronchospasm
As with other inhaled therapies, Onbrez Breezhaler may cause paradoxical bronchospasm, which may be life-threatening. In such cases, Onbrez Breezhaler should be discontinued immediately and alternative therapy initiated.
Worsening of disease
Onbrez Breezhaler is not indicated for the initial treatment of acute episodes of bronchospasm, i.e., as rescue therapy. If COPD worsens during treatment with Onbrez Breezhaler, the patient's condition and COPD treatment regimen should be reassessed. The daily dose of Onbrez Breezhaler should not be increased above the maximum recommended dose of 300 mcg.
Systemic effects
Although clinically significant cardiovascular effects are not usually observed after administration of Onbrez Breezhaler at recommended doses, as with other beta2-adrenergic agonists, indacaterol should be used with caution in patients with cardiovascular disorders, particularly coronary insufficiency, acute myocardial infarction, cardiac arrhythmias, and arterial hypertension, as well as in patients with seizure disorders or thyrotoxicosis, and in patients who respond inadequately to beta2-adrenergic agonists.
Cardiovascular effects
Like other beta2-adrenergic agonists, indacaterol may produce clinically significant cardiovascular effects in some patients, such as increased heart rate, elevated blood pressure, and/or other symptoms. In such cases, discontinuation of the drug may be necessary. Additionally, beta2-adrenergic agonists have been reported to cause ECG changes, including flattening of the T wave, QT interval prolongation, and ST segment depression. The clinical significance of these findings is unknown. Therefore, long-acting beta2-adrenergic agonists (LABA), or medicinal products containing LABA such as Onbrez Breezhaler, should be used with caution in patients with known or suspected QT interval prolongation and in patients receiving medicinal products that affect the QT interval.
Clinically significant effects on QT interval prolongation were not observed in clinical trials of Onbrez Breezhaler when recommended therapeutic doses were used.
Hypokalemia
Beta2-adrenergic agonists may cause marked hypokalemia in some patients, which may lead to adverse cardiovascular effects. Serum potassium reduction is usually transient and does not require supplementation. In patients with severe COPD, hypokalemia may be exacerbated by hypoxia and concomitant therapy, potentially increasing susceptibility to cardiac arrhythmias.
Hyperglycemia
Inhalation of high doses of beta2-adrenergic receptor agonists may increase plasma glucose levels. Plasma glucose levels should be monitored more closely in patients with diabetes mellitus after initiation of Onbrez Breezhaler therapy.
During clinical trials, clinically significant changes in plasma glucose levels occurred more frequently (by 1–2%) in patients treated with Onbrez Breezhaler at recommended doses compared to those receiving placebo. The effect of Onbrez Breezhaler has not been studied in patients with poorly controlled diabetes mellitus.
Excipients
The capsules contain lactose. Patients with rare hereditary problems of galactose intolerance, Lapp lactase deficiency, or glucose-galactose malabsorption should not take this medicinal product.
Use during pregnancy or breastfeeding.
Pregnancy
There are no data on the use of Onbrez Breezhaler during pregnancy. Animal studies do not indicate a direct or indirect harmful effect on reproductive performance. Like other beta2-adrenergic agonists, indacaterol may inhibit labor due to its relaxing effect on uterine smooth muscle. Indacaterol should be used during pregnancy only if the expected benefit to the pregnant woman outweighs the potential risk to the fetus.
Breastfeeding
It is unknown whether indacaterol/metabolites are excreted in human breast milk. Available pharmacokinetic/toxicological data show excretion of indacaterol/metabolites into animal milk. A risk to the breastfed infant cannot be excluded. A decision on whether to discontinue breastfeeding or to discontinue therapy with Onbrez Breezhaler should be made, taking into account the benefit of breastfeeding for the infant and the benefit of therapy for the woman.
Fertility
A reduced pregnancy rate was observed in rats. However, it is considered unlikely that indacaterol will affect reproductive function and fertility following inhalation of the maximum recommended dose.
Ability to influence reaction speed when driving or operating machinery.
Onbrez Breezhaler usually has no effect or has a negligible effect on the ability to drive or operate machinery. However, the possibility of nervous system-related adverse reactions should be considered (see section "Adverse reactions").
Dosage and Administration.
For use in adults.
The recommended dose is inhalation of the contents of 1 capsule of Onbrez Breezhaler 150 mcg using the Onbrez Breezhaler inhaler once daily. The dose may be increased only upon physician's recommendation.
Inhalation of the contents of 1 capsule of Onbrez Breezhaler 300 mcg once daily using the Onbrez Breezhaler inhaler has demonstrated additional clinical benefit in alleviating (relieving) dyspnea in patients with severe COPD. The maximum dose is 300 mcg once daily.
Onbrez Breezhaler should be used at the same time each day.
If a dose is missed, the next dose should be taken at the usual time the following day.
Elderly patients
Maximum plasma concentration and overall systemic exposure increase with age; however, dose adjustment in elderly patients is not required.
Hepatic or renal impairment
Dose adjustment is not required for patients with mild or moderate hepatic impairment. There are no data available on the use of the medicinal product in patients with severe hepatic impairment. Dose adjustment is not required for patients with renal impairment.
Administration instructions
Onbrez Breezhaler capsules must be used only by oral inhalation and exclusively with the Onbrez Breezhaler inhaler.
Onbrez Breezhaler capsules must not be swallowed.
Capsules should be removed from the blister pack only immediately before use.
Onbrez Breezhaler capsules from each new package should be used with a new inhaler. The inhaler from a previous package should not be used.
Patients should be instructed on the correct way to take the medicine. Patients who do not feel improvement in breathing should be asked whether they are swallowing instead of inhaling the medicine.
Instructions for using the inhaler.
The inhaler should be disposed of after all capsules from the pack have been used.
|
|
|||||||
| Insert |
Pierce and release |
Breathe in deeply |
Check that the capsule is empty |
||||
|
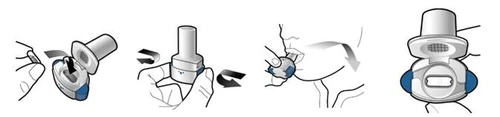
Step 1a: Remove the cap. |
Step 2a: Pierce the capsule once. Hold the inhaler vertically. Pierce the capsule by pressing both side buttons simultaneously. You should hear a click when the capsule is pierced. Pierce the capsule only once. |
Step 3a: Breathe out fully. Do not breathe into the inhaler. |
Check that the capsule is empty. Open the inhaler to see if any powder remains in the capsule. If powder remains in the capsule:
|
||||
|
Step 1b: Open the inhaler. |
Step 2b: Release the side buttons. |
Inhale the medication deeply. Hold the inhaler as shown in the picture. Place the mouthpiece in your mouth and close your lips tightly around it. Do not press the side buttons. |
|
||||
|
Step 1c: Remove the capsule. Peel off one blister from the blister pack. Do not swallow the capsule. |
Inhale as quickly and deeply as possible. During inhalation, you will hear a buzzing sound. You may taste the medicine during inhalation.
Step 3c: Hold your breath. Hold your breath for at least 5 seconds. |
Remove the empty capsule. Place the empty capsule in the trash. Close the inhaler and replace the cap. |
|||||
|
Step 1d: Insert the capsule. Never place the capsule directly into the mouthpiece.
Step 1e: Close the inhaler. |
Important information
|
||||||
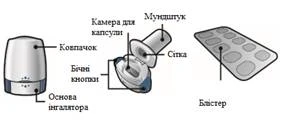
| The Onbrez Breezhaler inhaler pack contains:
Inhaler Base of inhaler Blister |
Frequently asked questions Why did I not hear a sound during inhalation? The capsule may be stuck in the capsule chamber. If this happens, gently dislodge the capsule by tapping the base of the inhaler. Inhale the medicine again by repeating steps 3a–3c. What should I do if there is still powder left in the capsule? You have not received a full dose of the medicine. Close the inhaler and repeat steps 3a–3c. I coughed after inhalation. Does this matter? This may happen. If the capsule is empty, you have received the full dose of the medicine. I felt small pieces of the capsule on my tongue. Does this matter? This may happen. It is not harmful. The likelihood of the capsule breaking into pieces increases if the capsule is punctured more than once. |
Cleaning the inhaler Wipe the mouthpiece inside and outside with a clean, dry, lint-free cloth to remove any powder residue. Keep the inhaler dry. Never wash the inhaler with water. |
|||||
| Disposal of the inhaler after use Each inhaler should be disposed of after all capsules in the pack have been used. Ask your pharmacist how to properly dispose of unused medicines and inhalers. |
|||||||






 Step 3b:
Step 3b:





Children.
There are no data on the appropriate use of Onbrez Breezhaler in children (under 18 years of age).
Overdose.
In patients with COPD, single doses exceeding the maximum recommended therapeutic dose by 10 times were associated with moderate increases in pulse rate, systolic blood pressure, and QTc interval.
Overdose of indacaterol may lead to intensification of effects typical of beta2-adrenergic agonists, i.e., tachycardia, tremor, palpitations, headache, nausea, vomiting, drowsiness, ventricular arrhythmia, metabolic acidosis, hypokalemia, and hyperglycemia.
In case of indacaterol overdose, supportive and symptomatic treatment is indicated. In severe cases, hospitalization of the patient is required. Cardioselective beta-blockers may be used, but only under physician supervision and with extreme caution, as their use may provoke bronchospasm.
Adverse reactions.
Safety profile
The most common adverse reactions with the use of the recommended doses of the medicinal product were nasopharyngitis (14.3%), upper respiratory tract infections (14.2%), cough (8.2%), headache (3.7%), and muscle spasms (3.5%). These adverse reactions were mainly mild or moderate in severity, and their frequency decreased with continued treatment.
At the recommended doses, the adverse reaction profile of Onbrez Breezhaler in patients with COPD shows clinically insignificant systemic effects of beta2-adrenoceptor stimulation. Changes in mean heart rate were less than 1 beat per minute; tachycardia occurred rarely and with the same frequency as in the placebo group. No relevant QTcF interval prolongation was observed compared to the placebo group. The incidence of clinically significant QTcF intervals [i.e., >450 ms (in males) and >470 ms (in females)] and hypokalaemia was similar to that in the placebo group. The mean value of maximum changes in blood glucose levels was similar in the Onbrez Breezhaler and placebo groups.
List of adverse reactions in the table
In the phase III clinical trial program of Onbrez Breezhaler, patients with a clinical diagnosis of moderate to severe COPD were enrolled. A total of 4764 patients received indacaterol for up to one year at doses up to twice the maximum recommended dose. Of these patients, 2611 received the medicinal product at a dose of 150 mcg once daily and 1157 at 300 mcg once daily. Approximately 41% of patients had severe COPD. The mean age of patients was 64 years, with 48% of patients aged over 65 years. The majority of patients (80%) were of Caucasian race.
The adverse reactions listed in Table 2 are classified by system organ classes according to MedDRA and are arranged in order of decreasing frequency as follows: very common (≥ 1/10); common (≥ 1/100, < 1/10); uncommon (≥ 1/1000, < 1/100); rare (≥ 1/10,000, < 1/1000); very rare (< 1/10,000); not known (cannot be estimated from available data).
Table 2. Adverse reactions
Adverse Reactions |
Frequency category when using dose of 150 mcg |
Frequency category when using dose of 300 mcg |
| Infections and infestations Upper respiratory tract infections Nasopharyngitis Sinusitis |
Common Common Common |
Very common Very common Common |
| Immune system disorders Increased sensitivity1 |
Uncommon |
Uncommon |
| Metabolism and nutrition disorders Diabetes and hyperglycemia |
Uncommon |
Common |
| Nervous system disorders Headache Dizziness Paresthesia |
Common Common Uncommon |
Common Common Uncommon |
| Cardiac disorders Ischemic heart disease Atrial fibrillation Palpitations Tachycardia |
Uncommon Uncommon Uncommon Uncommon |
Common Uncommon Common Uncommon |
| Respiratory, thoracic and mediastinal disorders Cough Oropharyngeal pain, including throat irritation Rhinorrhea Paradoxical bronchospasm |
Common Common Common Uncommon |
Common Common Common Uncommon |
| Skin and subcutaneous tissue disorders Pruritus/rash |
Uncommon |
Common |
| Musculoskeletal and connective tissue disorders Muscle spasm Myalgia Musculoskeletal pain |
Common Uncommon Uncommon |
Common Uncommon Common |
| General disorders and administration site conditions Chest pain Peripheral edema |
Common Common |
Common Common |
1Cases of hypersensitivity have been reported during the post-marketing experience with Onbrez Breezhaler. These reports were received on a voluntary basis from a population of unknown size, therefore, it is not always possible to reliably estimate frequency or establish a causal relationship to drug exposure. Hence, the frequency was calculated based on clinical trial experience.
When the dose of 600 mcg once daily was used, the safety profile of Onbrez Breezhaler was generally similar to that observed with the recommended doses. Additional adverse reactions include tremor (common).
Individual adverse reactions
During phase III clinical trials, sporadic cough was observed in an average of 17–20% of patients, starting within 15 seconds after inhalation and usually lasting 5 seconds (approximately 10 seconds in smokers). Cough occurred more frequently in women than in men and in smokers. This cough was generally well tolerated and did not lead to discontinuation of participation in the studies when the recommended doses were used (cough is a symptom of COPD, and only 8.2% of patients reported cough as an adverse reaction). There is no evidence that post-inhalation cough is associated with bronchospasm, complications, worsening of disease, or reduced treatment efficacy.
Reporting of possible adverse reactions
Reporting of possible adverse reactions after marketing authorization of the medicinal product is important. It allows continuous monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are requested to report any suspected adverse reactions via the national reporting system.
Shelf life. 2.5 years.
Storage conditions. Store below 30°C in the original packaging to protect from moisture. Keep out of reach of children.
Packaging. 10 capsules in a blister; 1 or 3 blisters with an inhaler in a cardboard box.
Prescription status. Prescription only.
Manufacturer.
Novartis Pharma Stein AG, Switzerland / Novartis Pharma Stein AG, Switzerland.
Novartis Farmaceutica S.A., Spain / Novartis Farmaceutica S.A., Spain.
Manufacturer's address and place of business.
Schaffhauserstrasse, 4332 Stein, Switzerland / Schaffhauserstrasse, 4332 Stein, Switzerland.
Ronda de Santa Maria 158, 08210 Barbera del Valles, Barcelona, Spain / Ronda de Santa Maria 158, 08210 Barbera del Valles, Barcelona, Spain.
Date of last review.