Novoseven
Ukraine
Table of Contents
INSTRUCTION FOR MEDICAL USE OF THE MEDICINAL PRODUCT NOVOSEVEN® (NOVOSEVEN®)
Composition:
Active substance: eptacog alfa (activated) (rFVIIa);
One vial contains 2 mg (100 IU) or 5 mg (250 IU) of eptacog alfa (activated);
Excipients: sodium chloride; calcium chloride, dihydrate; glycylglycine; polysorbate 80; methionine; sucrose; mannitol (E421).
After reconstitution, the product contains 1 mg/mL of eptacog alfa (activated) when reconstituted with the solvent.
Solvent: histidine, water for injections.
Pharmaceutical form. Lyophilized powder for solution for injection.
Main physicochemical properties: white lyophilized powder.
Pharmacotherapeutic group. Haemostatics. Coagulation factors.
ATC code B02B D08.
Pharmacological Properties
Pharmacodynamics
NovoSeven® contains activated recombinant coagulation factor VII with a molecular weight of approximately 50,000 daltons, produced by genetic engineering using newborn hamster kidney cells (BHK cells) as host cells.
Mechanism of action
The mechanism of action involves binding of factor VIIa to tissue factor. This complex converts factors IX and X into their active forms—IXa and Xa—leading to the conversion of small amounts of prothrombin into thrombin. Thrombin at the site of injury activates platelets and factors V and VIII, resulting in conversion of fibrinogen to fibrin and formation of a hemostatic clot. In pharmacological doses, NovoSeven® independently of tissue factor directly activates factor X on the surface of activated platelets located at the site of injury. This leads to the conversion of large amounts of prothrombin into thrombin without involvement of tissue factor.
Pharmacodynamic effect
Accordingly, the pharmacodynamic effect of factor VIIa consists in local increase in the formation of factor Xa, thrombin, and fibrin.
Time to maximum coagulant activity after administration of NovoSeven® was approximately 10 minutes in healthy volunteers and in patients with hemophilia.
Theoretically, generalized activation of the blood coagulation system cannot be completely excluded in patients with conditions predisposing to development of disseminated intravascular coagulation (DIC).
Clinical efficacy and safety
Congenital FVII deficiency
In an observational registry (F7HAEM-3578), the mean dose for long-term prophylaxis of bleeding in 22 children (under 12 years of age) with factor VII deficiency and severe clinical phenotype was 30 mcg/kg (range: 17–200 mcg/kg; in 10 patients the most frequently used dose was 30 mcg/kg), with a mean frequency of administration of 3 doses per week (range: 1–7; in 13 patients the most frequently reported frequency was 3 times per week).
In the same registry, thromboembolic events were observed in 3 out of 91 patients after surgical intervention.
Glanzmann's thrombasthenia
The observational registry (F7HAEM-3521) includes data from 133 patients with Glanzmann's thrombasthenia treated with NovoSeven®. The mean dose per administration for treatment of 333 bleeding episodes was 90 mcg/kg (range: 28–450 mcg/kg). NovoSeven® was used in 157 surgical procedures at a mean dose of 92 mcg/kg (up to 270 mcg/kg). Treatment with NovoSeven®, alone or in combination with antifibrinolytics and/or platelets, was considered effective if bleeding was controlled for at least 6 hours. The efficacy rate was 81% and 82%, respectively, in patients with positive or negative results for platelet transfusion resistance, and 77% and 85%, respectively, in patients with positive or negative results for platelet antibodies. A positive status indicates the presence of at least one positive test result during treatment.
Severe postpartum hemorrhage
The efficacy and safety of NovoSeven® were evaluated in 84 women with severe postpartum hemorrhage in a multicenter, open-label clinical trial. Patients were randomized and assigned to two groups: one group received a single dose of 60 mcg/kg of NovoSeven® (in addition to standard therapy; N = 42), while the other group received comparator therapy (standard therapy only; N = 42) after ineffective use of uterotonics (sulprostone). The treatment groups were well balanced with respect to demographic characteristics and prior treatment history for postpartum hemorrhage before randomization. Standard therapy included fibrinogen and tranexamic acid. Information on the use of fibrinogen/tranexamic acid was available for approximately 57% of patients in the NovoSeven® group and 43% in the comparator group. Among these, about 40% of patients in both groups received fibrinogen and/or tranexamic acid. Bleeding was considered stopped (i.e., treatment was deemed successful) if the calculated blood loss decreased to less than 50 mL over 10 minutes within 30 minutes after randomization. If bleeding became uncontrollable or refractory, invasive procedures were considered.
Primary analysis results showed that the number of women undergoing at least one embolization and/or ligation procedure was lower in the NovoSeven® group than in the comparator group (21 vs. 35), corresponding to a statistically significant 40% relative risk reduction in the NovoSeven® group compared to the control group (relative risk = 0.60 (95% confidence interval: 0.43–0.84, p = 0.0012)).
In the comparator group, 8 out of 42 patients later received NovoSeven® as rescue treatment on compassionate grounds in an attempt to avoid life-saving hysterectomy, which was successful in 2 cases.
Pharmacokinetics
Healthy volunteers
Distribution, excretion, and linearity
The pharmacokinetics of NovoSeven® were studied in 35 healthy Caucasian and Japanese volunteers in a dose-escalation study using a coagulation FVII assay. Participants were stratified by sex and ethnicity and received doses of 40, 80, and 160 mcg of NovoSeven® per kg body weight and/or placebo (3 doses). Pharmacokinetics were independent of sex and ethnic group. Mean volume of distribution at steady state ranged from 130 to 165 mL/kg, mean clearance values ranged from 33.3 to 37.2 mL/hour × kg. Mean terminal half-life ranged from 3.9 to 6 hours.
Pharmacokinetic profiles were dose-proportional.
Hemophilia A and B with inhibitors
Distribution, elimination, and linearity
Pharmacokinetic properties of NovoSeven® were studied using FVII assay in 12 children (2–12 years) and 5 adult patients in the absence of bleeding. Mean volume of distribution at steady state was 196 mL/kg in children compared to 159 mL/kg in adults. Mean clearance was approximately 50% higher in children than in adults (78 vs. 53 mL/hour × kg), while mean terminal half-life was 2.3 hours in both groups. Clearance appears to be age-related, and may increase by more than 50% in younger patients.
Dose proportionality was studied in children at doses of 90 and 180 mcg/kg body weight, based on previously obtained data from lower doses (17.5–70 mcg/kg rFVIIa).
Factor VII deficiency
Distribution and elimination
Pharmacokinetics of a single dose of NovoSeven® administered at 15 and 30 mcg/kg body weight did not differ significantly in terms of dose-independent parameters: total clearance – 70.8–79.1 mL/hour × kg, volume of distribution at steady state – 280–290 mL/kg, mean residence time in blood – 3.75–3.80 hours, elimination half-life – 2.82–3.11 hours. The mean in vivo plasma content was approximately 20% of the administered dose.
Glanzmann's thrombasthenia
The pharmacokinetics of NovoSeven® in patients with Glanzmann's thrombasthenia have not been studied, but it may be assumed that they do not differ significantly from those in hemophilia A and B.
Severe postpartum hemorrhage
The pharmacokinetics of NovoSeven® in women with severe postpartum hemorrhage have not been studied.
Preclinical safety data
All data obtained during preclinical safety studies were related to the pharmacological effect of rFVIIa.
A potential synergistic effect with combined treatment using rFXIII and rFVIIa was demonstrated in an experimental cardiovascular model in macaques, resulting in a significant pharmacological effect (thrombosis and death) at lower doses than when either agent was administered alone.
Clinical characteristics.
Indications.
Treatment and prevention of bleeding during surgical interventions or other invasive procedures in patients with the following conditions:
- Congenital hemophilia with inhibitor levels against coagulation factor VIII or IX > 5 BU (Bethesda units);
- Congenital hemophilia with a history of severe reaction to administration of factors VIII or IX;
- Acquired hemophilia;
- Congenital factor VII deficiency;
- Glanzmann's thrombasthenia with a history or current evidence of resistance to platelet transfusions or with thrombocytopenia.
Severe postpartum hemorrhage
The medicinal product NovoSeven® is indicated for the treatment of severe postpartum hemorrhage when uterotonics are insufficient to achieve hemostasis.
Contraindications.
Hypersensitivity to the active substance or to any of the excipients, as well as to mouse, hamster, or bovine proteins.
Interaction with other medicinal products and other forms of interactions.
The risk of interaction between NovoSeven® and coagulation factor concentrates is unknown. Concomitant use of activated or non-activated prothrombin complex concentrates should be avoided.
Administration of antifibrinolytic agents to hemophilia patients reduces blood loss during surgical procedures, particularly orthopedic surgeries or procedures in areas with high fibrinolytic activity, such as the oral cavity. Antifibrinolytic agents are also used to reduce bleeding in women with postpartum hemorrhage. However, experience with concomitant administration of antifibrinolytic agents and NovoSeven® is limited.
According to preclinical study data (see section "Preclinical safety data"), concomitant use of factor VIIa and factor XIII is not recommended.
Clinical data on the interaction between factor VIIa and factor XIII are lacking.
Special precautions for use.
Traceability
To improve traceability of biological medicinal products, the name and batch number of the administered product must be clearly documented.
In pathological conditions where tissue factor is expressed more intensely than normal, administration of NovoSeven® carries a risk of thrombosis or disseminated intravascular coagulation (DIC). Such a situation may occur in patients with severe atherosclerosis, crush syndrome, sepsis, or DIC.
Due to the risk of thromboembolic complications, NovoSeven® should be used with caution in patients with a history of ischemic heart disease, liver disease, patients after surgical procedures, pregnant women or women prior to delivery, neonates, or patients at risk of thromboembolic events or DIC. In each of these situations, the potential benefit of treatment with NovoSeven® must be weighed against the risk of such complications.
It is known that severe postpartum hemorrhage and pregnancy, as well as clinical conditions (delivery, severe hemorrhage, blood transfusion, DIC, surgical intervention/invasive procedures, and coagulopathy) may trigger thromboembolic risk, and particularly the risk of venous thromboembolism, which may be associated with NovoSeven® administration (see section "Adverse reactions").
Since the recombinant coagulation factor VIIa medicinal product NovoSeven® may contain traces of mouse and bovine immunoglobulins G, as well as other culture proteins (hamster and bovine serum proteins), patients receiving this product may develop hypersensitivity to these proteins over time. In such cases, the appropriateness of intravenous antihistamine treatment should be considered.
If allergic or anaphylactic reactions occur, administration of the product must be stopped immediately. In case of shock, standard medical treatment for this condition should be initiated. Patients should be informed about early signs of hypersensitivity reactions. If such symptoms occur, patients should be advised to stop using the medicinal product immediately and seek medical advice.
In cases of severe bleeding, this product should be administered in medical institutions specialized in treating hemophilia patients with inhibitors to factor VIII or IX, or, if such facilities are unavailable, in close collaboration with a physician experienced in the treatment of hemophilia.
If bleeding cannot be controlled, the patient must be hospitalized immediately. Patients or caregivers should inform healthcare professionals as quickly as possible about all injections of NovoSeven®. In patients with factor VII deficiency, prothrombin time and factor VII coagulation activity should be determined before and after administration of NovoSeven®. If factor VIIa activity does not reach the expected level, or bleeding cannot be controlled with the recommended doses, antibody formation may be suspected. In such cases, antibody levels should be determined.
Cases of thrombosis have been reported in patients with factor VII deficiency receiving NovoSeven® during surgical procedures; however, the degree of risk for such events remains unclear (see section "Pharmacodynamics").
Sodium content
NovoSeven® contains less than 1 mmol of sodium (23 mg); therefore, the medicinal product can be considered essentially "sodium-free".
Use during pregnancy or breastfeeding.
Pregnancy
As a precautionary measure, use of NovoSeven® during pregnancy is not recommended. Limited data on the use of the medicinal product during pregnancy for approved indications suggest no adverse effects of rFVIIa on pregnancy or fetal/neonatal health. Currently, no other relevant epidemiological data are available. Animal studies have shown no direct or indirect adverse effects on pregnancy, embryonic/fetal development, parturition, or postnatal development.
Breastfeeding
It is unknown whether rFVIIa is excreted in human breast milk. Excretion of rFVIIa into animal breast milk has not been studied. The decision to continue or discontinue breastfeeding or treatment with NovoSeven® should be made by considering the benefits of breastfeeding for the child and the benefits of NovoSeven® therapy for the woman.
Fertility
Preclinical and post-marketing data do not indicate any negative effect of rFVIIa on fertility in men or women.
Ability to affect reaction speed when driving or operating machinery.
No studies on the effect of the medicinal product on the ability to drive or operate machinery have been conducted.
Administration and Dosage
Treatment should be initiated under the supervision of a physician experienced in the management of hemophilia and/or bleeding disorders.
The management of severe postpartum hemorrhage should be performed by a multidisciplinary team. In addition to obstetricians, this team should include anesthesiologists, intensivists, and/or hematologists. Standard treatment methods should be continued according to the individual patient's needs. Adequate fibrinogen concentration and platelet count should be maintained to optimize the therapeutic benefit of NovoSeven®.
Dosage Regimen
Hemophilia A or B with inhibitors or acquired hemophilia
NovoSeven® should be administered as soon as possible after the onset of bleeding. The initial recommended dose is given intravenously (as a bolus) at a dose of 90 mcg (4.5 IU) per kg body weight.
After administration of the initial dose, repeated doses may be required. The duration of treatment and intervals between doses vary depending on the severity of bleeding, type of invasive procedure, or surgical intervention.
Available clinical experience indicates no overall difference in dosing between adults and children, although children have a faster clearance than adults. Therefore, higher doses of rFVIIa may be required in children to achieve plasma concentrations similar to those in adult patients (see section "Pharmacokinetics").
Dosing Intervals
Initially, to achieve hemostasis, the drug should be re-administered every 2–3 hours.
If continued treatment is necessary after achieving effective hemostasis, administration should be repeated every 4, 6, 8, or 12 hours, as required for treatment.
Minor or moderate bleeding (including outpatient treatment)
Early administration of the drug in an outpatient setting has proven effective in treating mild or moderate bleeds into joints, muscles, skin, and mucous membranes. Two administration regimens may be recommended:
- administration of two to three doses of the drug at 90 mcg/kg body weight every 3 hours, followed by one additional dose to maintain hemostasis;
- single administration of the drug at a dose of 270 mcg/kg body weight.
The duration of outpatient treatment should not exceed 24 hours. Home treatment continuation may only be considered after consultation with a hemophilia treatment center.
There is no clinical experience with a single dose of 270 mcg/kg body weight in elderly patients.
Severe bleeding
It is recommended to administer the initial dose of 90 mcg/kg body weight during patient transport to the hospital where they are usually treated. The dose of subsequent administrations depends on the type and severity of bleeding. Initially, the drug should be administered every 2 hours until clinical improvement is observed. If continued treatment is necessary, the interval between doses may be extended to every 3 hours for 1–2 days. Thereafter, during the subsequent treatment period, the dosing interval should be progressively extended to every 4, 6, 8, or 12 hours. Severe bleeding episodes may require treatment for 2–3 weeks or longer (depending on the patient's clinical condition).
Invasive procedures/surgery
The initial dose of 90 mcg/kg body weight should be administered immediately before the procedure. This dose should be repeated 2 hours later, and then every 2–3 hours during the first 24–48 hours (depending on the extent of the procedure and the patient's clinical condition). For major surgical procedures, the drug should be administered every 2–4 hours for 6–7 days. Thereafter, during the next 2 weeks, the dosing interval should be increased to every 6–8 hours. Patients undergoing major surgery should receive the drug for 2–3 weeks until wound healing is complete.
Acquired hemophilia
Dose and administration intervals
NovoSeven® should be administered as soon as possible after the onset of bleeding. The initial recommended dose is given intravenously (as a bolus) at a dose of 90 mcg (4.5 IU) per kg body weight.
After administration of the initial dose, repeated doses may be required. The duration of treatment and intervals between doses vary depending on the severity of bleeding, type of invasive procedure, or surgical intervention.
Initially, the drug should be re-administered every 2–3 hours. If continued treatment is necessary after achieving effective hemostasis, administration should be repeated every 4, 6, 8, or 12 hours, as required for treatment.
Factor VII deficiency
Dose range and administration intervals
The recommended dose range for children and adults for the treatment and prevention of bleeding in patients undergoing surgery or invasive procedures is 15–30 mcg/kg body weight every 4–6 hours until hemostasis is achieved. The dose and administration interval should be individually adjusted.
Children
Results from limited clinical experience with long-term prophylaxis in children up to 12 years of age with a severe clinical phenotype have been combined (see section "Pharmacodynamics").
The dose and frequency of injections for prophylaxis should be based on the clinical response to treatment and individually adjusted.
Glanzmann's thrombasthenia
Dose range and administration intervals
The recommended dose for the treatment and prevention of bleeding in patients undergoing surgery or invasive procedures is 90 mcg (range 80–120 mcg)/kg body weight every 2 hours (1.5–2.5 hours). At least three doses should be administered to maintain effective hemostasis. Bolus injections are recommended, as slow infusion may be ineffective. For the treatment of Glanzmann's thrombasthenia, platelet transfusions should be administered first in patients without resistance.
Severe postpartum hemorrhage
Dose range and dosing interval
The recommended dose range for the treatment of bleeding is 60–90 mcg per kg body weight administered intravenously as a bolus. Peak coagulant activity is expected within 10 minutes after administration. A second dose may be administered depending on the individual patient's clinical response.
If hemostatic response is insufficient, a second dose should be administered within 30 minutes.
Administration method
Instructions for reconstitution of the drug before administration can be found on the reverse side of the NovoSeven® medical instructions leaflet. The solution should be administered as an intravenous bolus injection over 2–5 minutes.
Treatment monitoring — laboratory tests
Monitoring of treatment is not mandatory, as the severity of bleeding and the clinical response to NovoSeven® administration determine the need for further dosing.
After administration of NovoSeven®, a reduction in prothrombin time and activated partial thromboplastin time has been observed; however, no correlation with the clinical efficacy of the drug has been demonstrated.
Handling and disposal precautions
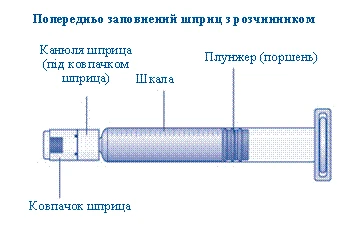
The diluent for NovoSeven® is supplied in a pre-filled syringe.
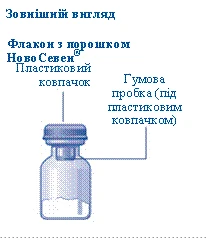
Lyophilized powder in vial and diluent in pre-filled syringe
Always follow aseptic procedures.
Reconstitution
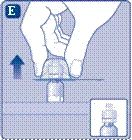
- The vial containing NovoSeven® powder and the pre-filled syringe with diluent should be at room temperature before reconstitution. Remove the plastic cap from the vial. Do not use the vial if the cap is loose or missing. Wipe the rubber stopper of the vial with a sterile alcohol swab and allow it to dry for several seconds before use. Do not touch the rubber stopper after wiping.
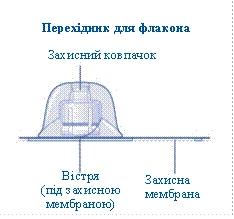
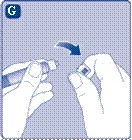
- Remove the protective membrane from the vial adapter. Do not remove the vial adapter from its protective cap. Do not use the vial adapter if the protective membrane is incompletely sealed or damaged. Twist off the protective cap and attach the vial adapter. Gently press the protective cap with thumb and index finger. Remove the protective cap from the vial adapter.
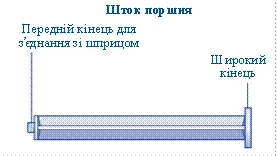
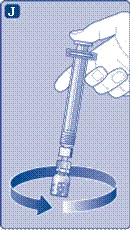
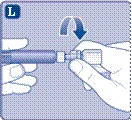
- Screw the plunger rod of the syringe into the plunger inside the pre-filled syringe clockwise until firmly seated. Remove the cap from the syringe by twisting it until the perforation breaks. Do not touch the tip of the syringe under the cap. Do not use the pre-filled syringe if the cap is loose or missing.
- Attach the pre-filled syringe with diluent to the vial adapter by turning the syringe clockwise until firmly seated. Hold the syringe slightly tilted with the vial downward. Press the plunger to transfer all the diluent into the vial. Keep the plunger depressed and gently rotate the vial until the powder is completely dissolved. Do not shake the vial, as this may cause foaming.
If a higher dose is required, repeat this procedure with additional vials, diluent-filled syringes, and vial adapters.
The reconstituted NovoSeven® solution is colorless. Before administration, visually inspect the solution for the presence of foreign particles and discoloration.
NovoSeven® is recommended for immediate use after reconstitution. Storage conditions for the reconstituted solution are described in the "Storage" section.
Administration
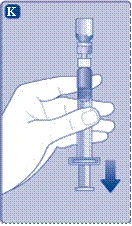
- Keep the plunger fully inserted into the syringe barrel. Invert the syringe with the vial upward. Release pressure on the plunger and wait for the reconstituted solution to fill the syringe. Gently pull the plunger downward to draw all the solution into the syringe.
- Holding the vial upward, gently tap the syringe to allow all air bubbles to rise to the top. Slowly press the plunger until all air bubbles are expelled.
If the full dose is not required, use the scale on the syringe to determine how much reconstituted solution has been withdrawn.
- Detach the syringe from the vial adapter by turning it counterclockwise.
- NovoSeven® is now ready for injection. Select the injection site and slowly administer NovoSeven® intravenously over 2–5 minutes, without removing the needle from the injection site.
Dispose of used materials following necessary safety precautions. All unused medicinal products and waste materials should be disposed of according to local requirements.
Procedure for combining vials (only possible in hospital settings)
In vitro studies have demonstrated that the drug remains chemically and physically stable when stored in a 50 ml polypropylene syringe for 24 hours at 25°C. Compatibility has been demonstrated with a system consisting of a 50 ml polypropylene syringe, a 2 m polyethylene infusion tube, and an integrated 5-micron filter.
Combining vials (only in hospital settings)
- All steps must be performed by qualified personnel under controlled and certified aseptic conditions.
- If reconstitution, mixing, or use of the drug by the user does not follow the instructions for medical use, responsibility for storage duration and conditions lies with the user.
- Ensure that a vial adapter is used.
- Perform reconstitution of the drug as described above in the "Reconstitution" section. Detach the empty syringe from the vial adapter by turning it counterclockwise, ensuring that the vial adapter remains attached to the vial containing the reconstituted drug.
- Repeat this procedure with the required number of additional vials, diluent vials / pre-filled syringes, and vial adapters.
- Draw approximately 5 ml of sterile air into a 50 ml polypropylene syringe. Attach the syringe to the vial adapter by turning it clockwise until firmly seated. Hold the syringe slightly tilted with the vial downward. Carefully press the plunger to inject a small amount of air into the vial. Invert the syringe with the vial upward and draw the vial contents into the syringe. Repeat the above procedure with other vials containing reconstituted drug to obtain the required solution volume in the syringe.
- An integrated 5-micron filter must be used for administration. Before starting administration, ensure that the syringe, infusion tubing, and integrated filter are filled with solution and free of air bubbles.
- The syringe containing properly reconstituted drug is ready for use with a CE-marked infusion pump (compatible with a 50 ml syringe).
- The infusion pump should only be operated by qualified medical personnel.
NovoSeven®, user instructions
Before using NovoSeven®, read these instructions carefully.
NovoSeven® is supplied as a powder. Before injection (administration), it must be reconstituted with the diluent provided in the syringe. The diluent is a histidine solution. The reconstituted NovoSeven® preparation is administered intravenously (intravenous injection). The contents of this package are intended for reconstitution and administration of NovoSeven®.
For intravenous administration, an infusion set (tubing and butterfly needle), alcohol swabs, gauze pads, and adhesive tape are also required. These medical devices are not included in the NovoSeven® package.
Do not use equipment without proper training from a physician or nurse.
Always wash your hands before use and ensure that your surroundings are clean.
During preparation and direct intravenous administration of the drug, it is very important to follow aseptic and antiseptic procedures. Improper injection technique may lead to blood infection.
Do not open the equipment until you are ready to use it.
Do not use equipment if it has been dropped or damaged. Take a new package.
Do not use equipment after its expiration date. Take a new package. The expiration date is printed after "Exp." on the carton box, vial, vial adapter, and pre-filled syringe.
Do not use equipment if you suspect it is contaminated. Take a new package.
Do not discard any part of the kit until you have administered the prepared solution.
The equipment is intended for single use only.
Package contents:
- 1 vial with NovoSeven® powder
- 1 vial adapter
- 1 pre-filled syringe with diluent
- 1 plunger rod (located under the syringe)
ensure it contains the required medication.
prefilled syringe from the box. Leave the syringe plunger in the box.
room temperature (not exceeding 37°C). You can do this by holding them in your hands until they feel as warm as your hands.
|
|
If the plastic cap is loose or missing, do not use the vial.
Do not touch the rubber stopper with fingers, as this may transfer microorganisms. |
|
If the seal of the protective membrane is broken or damaged, do not use the vial adapter. Do not remove the vial adapter from its packaging with fingers. If you touch the tip of the vial adapter, it may lead to transfer of microorganisms from your fingers. |
|
|
|
and index finger, as shown in the picture. Remove the protective cap from the adapter, but without removing the adapter from the vial. |
|
Take the syringe plunger by the wide end and remove it from the box. Do not touch the sides or front end of the plunger rod. If you touch the sides or front end of the plunger rod, it may transfer microorganisms from your fingers. Immediately attach the plunger rod to the piston inside the prefilled syringe by turning it clockwise until it stops. |
|
| Remove the syringe cap from the prefilled syringe, bending it downward until it breaks off at the perforation. Do not touch the syringe cannula under the cap. If you touch the syringe cannula, it may transfer microorganisms from your fingers. If the cap on the syringe is loose or missing, do not use this prefilled syringe. |
|
|
|
|
|
Do not shake the vial – this will cause foaming.
|
|
| Use the reconstituted NovoSeven® medication solution immediately to avoid contamination. If you do not use the solution immediately, refer to the "Storage conditions" section on the back of the leaflet. Do not store the reconstituted solution without consulting your doctor or nurse. If a dose greater than 1 vial is required, repeat steps 1–4 (Fig. A–J) with additional vials, vial adapters, and prefilled syringes until the required dose is obtained. |
|
|
|
If you touch the syringe cannula, it may transfer microorganisms from your fingers. |
|
| Administration of NovoSeven® medication from the prefilled syringe via a needle-free connector for intravenous catheters. Warning. The prefilled syringe is made of glass and is compatible with standard "Luer-Lock" connections. Some needle-free connectors with internal needles are incompatible with the prefilled syringe. This incompatibility may prevent administration of the drug and/or damage the needle-free connector. Follow the instructions for use of needle-free connectors. When administering medication via needle-free connectors, it may be necessary to transfer the reconstituted solution into a standard 10 ml disposable plastic "Luer-Lock" syringe. This must be done immediately after step 4 (Fig. J). |
|
The NovoSeven® medication is now ready for administration as an intravenous injection.
Injection of the solution via a central venous catheter or subcutaneous port:
|
|
| Disposal
|
|
| Do not disassemble equipment before disposal. Do not reuse equipment. |
|








Children.
The medicinal product is administered to children (see section "Dosage and administration").
Overdose.
The dose-limiting toxicity of NovoSeven® has not been studied during clinical trials.
Four cases of overdose have been reported in patients with haemophilia over the last 16 years. The only complication reported in connection with overdose was a slight transient increase in blood pressure in a 6-year-old patient who received 24 mg of rFVIIa instead of 5.5 mg.
No cases of overdose have been reported in patients with acquired haemophilia or Glanzmann's thrombasthenia.
In patients with factor VII deficiency, at the recommended dose of 15–30 mcg/kg rFVIIa, one case of overdose was associated with a thrombotic event (occipital stroke) in an elderly male patient (>80 years of age) who exceeded the recommended dose by 10–20 times. In addition, development of antibodies against NovoSeven® and factor VII has been associated with overdose in one patient with factor VII deficiency.
Doses administered should not exceed the recommended doses due to the lack of information on potential additional risks.
Adverse Reactions
The most commonly reported adverse reactions were reduced therapeutic response, fever, rash, venous thromboembolic events, pruritus, and urticaria. These reactions occurred at a rare frequency (≥ 1/1000, < 1/100).
Adverse reactions reported during clinical trials and in the post-marketing period are listed below. Within each frequency group, reactions are listed in order of decreasing severity. The frequency of adverse reactions reported only in the post-marketing period (not during clinical trials) is unknown.
In clinical studies involving 484 patients (4297 treatment episodes) with hemophilia A and B, acquired hemophilia, factor VII deficiency, or Glanzmann's thrombasthenia, adverse reactions to the medicinal product were shown to be common (≥ 1/100 to < 1/10). Since the total number of treatment episodes in clinical trials did not exceed 10,000, the lowest possible frequency of adverse reactions that can be identified is rare (≥ 1/10,000 to < 1/1000).
The most frequent adverse reactions to the medicinal product are fever and rash (uncommon: ≥ 1/1000 to < 1/100), while the most serious adverse reactions are venous thromboembolic events (uncommon: ≥ 1/1000 to < 1/100) and arterial thromboembolic events (rare: ≥ 1/10,000 to < 1/1000).
Blood and lymphatic system disorders
Rare (≥ 1/10,000, < 1/1000) – disseminated intravascular coagulation (DIC) and associated laboratory abnormalities, including elevated D-dimer levels and decreased AT-III levels (see section "Special precautions for use"), coagulopathy.
Gastrointestinal disorders
Rare (≥ 1/10,000, < 1/1000) – nausea.
General disorders and administration site conditions
Uncommon (≥ 1/1000, < 1/100) – reduced therapeutic response, fever.
Rare (≥ 1/10,000, < 1/1000) – injection site reactions, including injection site pain.
Immune system disorders
Rare (≥ 1/10,000, < 1/1000) – hypersensitivity (see sections "Contraindications" and "Special precautions for use").
Frequency unknown – anaphylactic reactions.
Investigations
Rare (≥ 1/10,000, < 1/1000) – increased levels of fibrin degradation products, increased levels of alanine aminotransferase, alkaline phosphatase, lactate dehydrogenase, and prothrombin.
Nervous system disorders
Rare (≥ 1/10,000, < 1/1000) – headache.
Skin and subcutaneous tissue disorders
Uncommon (≥ 1/1000, < 1/100) – rash (including allergic dermatitis and erythematous rashes), pruritus, and urticaria.
Frequency unknown – flushing, angioedema.
Vascular disorders
Uncommon (≥ 1/1000, < 1/100) – venous thromboembolic events (deep vein thrombosis, thrombosis at the site of intravenous administration, pulmonary embolism, hepatic thromboembolic events including portal vein thrombosis, renal vein thrombosis, thrombophlebitis, superficial venous thrombophlebitis, and intestinal ischemia).
Rare (≥ 1/10,000, < 1/1000) – arterial thromboembolic events (myocardial infarction, cerebral infarction, cerebral ischemia, occlusion of cerebral vessels, stroke, renal artery thrombosis, peripheral vascular ischemia, peripheral ischemic thrombosis, and intestinal ischemia), angina pectoris.
Frequency unknown – cardiac chamber thrombosis.
Reduced efficacy (decreased therapeutic response) has been reported. It is very important that the dosing regimen of NovoSeven® complies with the recommendations provided in the section "Dosage and administration".
Description of selected adverse reactions
Development of inhibitory antibodies
During post-marketing use, no cases of inhibitory antibodies to NovoSeven® or FVII have been reported in patients with hemophilia A or B. Cases of development of inhibitory antibodies to NovoSeven® have been reported in a post-marketing observational registry of patients with congenital factor VII deficiency.
In clinical studies involving patients with factor VII deficiency, the development of antibodies to NovoSeven® and factor VII (common: ≥ 1/100, < 1/10) was the only reported adverse reaction. In some cases, these antibodies caused an inhibitory effect in vitro. Risk factors for antibody development include prior treatment with human plasma and/or plasma-derived factor VII, severe factor VII gene mutations, and overdosing of NovoSeven®. Patients with factor VII deficiency treated with NovoSeven® should be continuously monitored for the presence of antibodies to factor VII (see section "Special precautions for use").
Thromboembolic events: arterial and venous
When NovoSeven® is used for unapproved indications, arterial thromboembolic events are common (≥ 1/100, < 1/10). A higher risk of arterial thromboembolic adverse events (see above "Vascular disorders") (5.6% in patients treated with NovoSeven® compared to 3.0% in placebo-treated patients) was identified in a meta-analysis of pooled data from placebo-controlled studies when the medicinal product was used for unapproved indications.
Thromboembolic events may lead to cardiac arrest.
Special patient populations
Patients with acquired hemophilia
In clinical studies involving 61 patients with acquired hemophilia (including 100 treatment episodes), the most frequently reported adverse reactions (1% of all treatment episodes) were arterial thromboembolic events (occlusion of cerebral vessels, stroke), venous thromboembolic events (pulmonary embolism and deep vein thrombosis), angina pectoris, nausea, fever, erythematous rashes, and increased levels of fibrin degradation products.
Women with severe postpartum hemorrhage
In an open-label randomized clinical trial, venous thromboembolic events were reported in 2 out of 51 women who received a single dose of NovoSeven® (mean dose 58 mcg/kg); such events were not observed in any of the 33 women who did not receive NovoSeven®; arterial thromboembolic events were not observed in either group.
In 4 non-interventional studies, venous thromboembolic events were observed in 3 out of 358 women (0.8%) who received NovoSeven® (mean dose range 63–105 mcg/kg), and arterial thromboembolic events were observed in 1 woman (0.3%) who received NovoSeven®.
For information on known factors contributing to increased thromboembolic risk associated with pregnancy and severe postpartum hemorrhage, see section "Special precautions for use".
Reporting of adverse reactions and lack of efficacy
Reporting adverse reactions after marketing authorization of the medicinal product is of great importance. It enables ongoing monitoring of the benefit-risk balance of the medicinal product. Healthcare professionals, pharmacists, patients, and their legal representatives should report all suspected adverse reactions and lack of efficacy via the Automated Pharmacovigilance Information System at https://aisf.dec.gov.ua/.
Shelf life. The shelf life of the commercially packaged product is 3 years when stored below 25 °C.
In the vial
Chemical and physical stability of the reconstituted medicinal product has been demonstrated for 6 hours at 25 °C or 24 hours at 5 °C.
From a microbiological standpoint, the reconstituted product should be used immediately. The user is responsible for the storage conditions and duration. If reconstitution was not performed under controlled and validated aseptic conditions, the storage time of the reconstituted medicinal product should not exceed 24 hours at 2–8 °C. The reconstituted solution should be stored in the vial.
In the syringe (50 mL polypropylene syringe) only in hospital settings
Reconstitution should be performed by trained personnel under controlled and certified aseptic conditions. The medicinal product remains chemically and physically stable when stored in a 50 mL polypropylene syringe for up to 24 hours at 25 °C. If the product is not used immediately, the user is responsible for ensuring proper storage conditions. The storage time after opening the packaging should not exceed 24 hours.
Storage conditions.
Store out of reach and sight of children, protected from light, at a temperature not exceeding 25 °C.
Do not freeze.
For storage conditions of the reconstituted medicinal product, see section "Shelf life".
Incompatibilities. NovoSeven® must not be mixed with infusion solutions or administered by infusion.
Packaging.
1 cardboard box contains 1 glass vial of 2 mL or 12 mL capacity with white powder for solution for injection, closed with a chlorobutyl rubber stopper and sealed with an aluminum cap with a protective removable polypropylene cap, and 1 pre-filled glass syringe (type 1) of 3 mL or 10 mL capacity containing 2 mL or 5 mL of solvent (histidine, water for injections).
The syringe is closed on one side with a bromobutyl rubber cap and polypropylene cap, and on the other side with a bromobutyl rubber plunger and polypropylene stopper. A polypropylene plunger rod is also included with the syringe. A vial adapter with a 25 µm filter for fine filtration, individually packaged, is also included.
Prescription status. Prescription only.
Manufacturer/Marketing Authorization Holder.
A/T Novo Nordisk / Novo Nordisk A/S.
Manufacturer's address and place of business.
Novo Allé, Bagsværd, 2880, Denmark / Novo Alle, Bagsvaerd, 2880, Denmark.