Moxifloxacin-darnitsa
Ukraine
Table of Contents
INSTRUCTIONS FOR MEDICAL USE OF THE MEDICINAL PRODUCT MOXIFLOXACIN-DARNYTSIA MOXIFLOXACIN-DARNYTSIA
Composition:
Active substance: moxifloxacin;
One vial (250 ml of solution) contains 436 mg of moxifloxacin hydrochloride, equivalent to 400 mg of moxifloxacin;
Excipients: sodium chloride, hydrochloric acid, sodium hydroxide, water for injections.
Pharmaceutical form. Infusion solution.
Main physicochemical properties: clear yellow liquid.
Theoretical osmolarity: 278 mOsmol/L; pH 4.1 – 4.6.
Pharmacotherapeutic group. Antimicrobial agents for systemic use. Antibacterials of the quinolone group. ATC code J01MA14.
Pharmacological properties.
Pharmacodynamics.
Mechanism of action
Moxifloxacin inhibits bacterial type II topoisomerases (DNA gyrase and topoisomerase IV), which are essential for replication, transcription, and repair of bacterial DNA.
Pharmacokinetics/pharmacodynamics
The ability of fluoroquinolones to kill bacteria is directly concentration-dependent. Pharmacodynamic studies of fluoroquinolones in animal models of infectious-inflammatory diseases and in humans indicate that the primary determinant of efficacy is the ratio between the area under the pharmacokinetic curve (AUC24) and the minimum inhibitory concentration (MIC).
Mechanism of resistance
Resistance to fluoroquinolones may arise due to mutations in DNA gyrase and topoisomerase IV. Other mechanisms include overexpression of efflux pumps, impermeability, and protein-mediated protection of DNA gyrase. Cross-resistance may be expected between moxifloxacin and other fluoroquinolones.
Resistance mechanisms characteristic of antibacterial agents belonging to other classes do not affect the antibacterial efficacy of moxifloxacin.
Breakpoint values
Clinical MIC and disk diffusion breakpoint values for moxifloxacin according to EUCAST (European Committee on Antimicrobial Susceptibility Testing) (01.01.2012):
Table 1
| Microorganism |
Susceptible |
Resistant |
| Staphylococcus spp. |
≤ 0.5 mg/l ≥ 24 mm |
> 1 mg/l < 21 mm |
| S. pneumoniae |
≤ 0.5 mg/l ≥ 22 mm |
> 0.5 mg/l < 22 mm |
| Streptococcus groups A, B, C, G |
≤ 0.5 mg/l ≥ 18 mm |
> 1 mg/l < 15 mm |
| H. influenzae |
≤ 0.5 mg/l ≥ 25 mm |
> 0.5 mg/l < 25 mm |
| M. catarrhalis |
≤ 0.5 mg/l ≥ 23 mm |
> 0.5 mg/l < 23 mm |
| Enterobacteriaceae |
≤ 0.5 mg/l ≥ 20 mm |
> 1 mg/l < 17 mm |
| Intermediate values, not species-related* |
≤ 0.5 mg/l |
> 1 mg/l |
*Non-species-related breakpoints were primarily established based on the relationship between pharmacokinetic and pharmacodynamic data and do not depend on the MIC for individual species. These data are used for species that do not have individually defined breakpoints and do not apply to species for which interpretive criteria are subject to determination.
Microbiological susceptibility
The prevalence of acquired resistance among isolated species may vary depending on geographical location and time; therefore, local information on resistance patterns is necessary, especially when treating severe infections. If necessary, consultation with specialists should be sought when local resistance prevalence has reached a level at which the benefit of using the medicinal product, at least for certain types of infections, is questionable.
| Commonly susceptible microorganisms |
| Aerobic Gram-positive microorganisms Staphylococcus aureus *+ Streptococcus agalactiae (Group B) Streptococcus milleri group* (S. anginosus, S. constellatus and S. intermedius) Streptococcus pneumoniae * Streptococcus pyogenes * (Group A) Streptococcus viridans group (S. viridans, S. mutans, S. mitis, S. sanguinis, S. salivarius, S. thermophilus) |
| Aerobic Gram-negative microorganisms Acinetobacter baumannii Haemophilus influenzae * Legionella pneumophila Moraxella (Branhamella) catarrhalis * |
| Anaerobic microorganisms Prevotella spp. |
| Other microorganisms Chlamydophila (Chlamydia) pneumoniae * Coxiella burnetii Mycoplasma pneumoniae * |
| Microorganisms with potential for resistance development |
| Aerobic Gram-positive microorganisms Enterococcus faecalis* Enterococcus faecium* |
| Aerobic Gram-negative microorganisms Enterobacter cloacae * Escherichia coli *# Klebsiella pneumoniae *# Klebsiella oxytoca Proteus mirabilis * |
| Anaerobic microorganisms Bacteroides fragilis* |
| Resistant microorganisms |
| Aerobic Gram-negative microorganisms Pseudomonas aeruginosa |
| *Clinical efficacy has been sufficiently demonstrated in clinical studies. +Methicillin-resistant S. aureus is very often simultaneously resistant to fluoroquinolones. In methicillin-resistant S. aureus, resistance rates to moxifloxacin exceed 50%. #Strains producing extended-spectrum beta-lactamases (ESBL) are also resistant to fluoroquinolones. |
Pharmacokinetics.
Absorption and bioavailability
After a single 1-hour intravenous infusion of 400 mg, the maximum concentration (Cmax) of the drug is reached at the end of the infusion and is approximately 4.1 mg/l, which is about 26 % higher than this value after oral administration (3.1 mg/l). The AUC value is approximately 39 mg•h/l after intravenous administration, which slightly exceeds the parameter after oral administration (35 mg•h/l); absolute bioavailability is approximately 91 %. There is no need to adjust doses according to patient age or gender when moxifloxacin is administered intravenously. Pharmacokinetics are linear within the range of 50–200 mg for single oral doses, up to 600 mg for single intravenous doses, and up to 600 mg administered once daily for 10 days.
Distribution
Moxifloxacin rapidly distributes into the extravascular space. The volume of distribution at steady state (Vss) is approximately 2 l/kg. In vitro and ex vivo studies show that protein binding is approximately 40–42 %, independent of drug concentration. Moxifloxacin binds primarily to serum albumin.
Maximum concentrations of 5.4 mg/kg and 20.7 mg/l (geometric mean values) were observed in bronchial mucosa and epithelial lining fluid, respectively, 2.2 hours after oral dosing. The corresponding Cmax in alveolar macrophages was 56.7 mg/kg. A concentration of 1.75 mg/l was observed in blister fluid 10 hours after intravenous administration. The "free concentration – time" profile in interstitial fluid is similar to that in plasma, with peak free concentration reaching approximately 1.0 mg/l (geometric mean) about 1.8 hours after intravenous administration.
Metabolism
Moxifloxacin undergoes phase II biotransformation and is eliminated from the body via the kidneys (approximately 40 %) and feces/bile (approximately 60 %), both unchanged and as sulfated (M1) and glucuronide (M2) metabolites. M1 and M2 are metabolites relevant only in humans, and both are microbiologically inactive.
No metabolic pharmacokinetic interactions with other drugs involved in phase I biotransformation, including cytochrome P450 enzyme system, were observed during in vitro and phase I clinical studies. There is no evidence of oxidative metabolism.
Elimination
The elimination half-life of moxifloxacin in plasma is approximately 12 hours. Mean steady-state total clearance after administration of 400 mg ranges from 179 to 246 ml/min. After intravenous administration of 400 mg, urinary excretion of unchanged drug was approximately 22 % and fecal excretion approximately 26 %. Overall excretion (unchanged drug and metabolites) was approximately 98 % after intravenous administration. Renal clearance is approximately 24–53 ml/min, indicating partial tubular reabsorption of the drug in the kidneys. Concomitant administration of ranitidine and probenecid does not alter renal clearance of the parent drug.
Renal impairment
No significant changes in moxifloxacin pharmacokinetics have been observed in patients with renal dysfunction (including patients with creatinine clearance > 20 ml/min/1.73 m²). With decreasing renal function, plasma concentration of metabolite M2 (glucuronide) increases by almost 2.5-fold (with creatinine clearance < 30 ml/min/1.73 m²).
Hepatic impairment
Pharmacokinetic studies in patients with hepatic insufficiency (Child–Pugh classes A and B) do not allow definitive conclusions regarding differences in pharmacokinetic parameters between patients with hepatic impairment and healthy volunteers. Hepatic dysfunction was associated with higher plasma exposure to metabolite M1, while exposure to the parent drug was similar to that in healthy volunteers. There is insufficient clinical experience with moxifloxacin use in patients with hepatic impairment.
Preclinical safety data
In traditional repeated-dose toxicity studies in animals, hematological toxicity and hepatotoxicity were observed with moxifloxacin. Toxic effects on the central nervous system (CNS) were noted. These effects occurred after administration of high doses of moxifloxacin or prolonged treatment.
High oral doses in animals (≥ 60 mg/kg), resulting in plasma concentrations ≥ 20 mg/l, caused changes in electroretinogram parameters and, in some cases, retinal atrophy.
Systemic toxicity after intravenous administration was most pronounced when moxifloxacin was given as bolus injections (45 mg/kg) and was not observed when moxifloxacin (40 mg/kg) was administered via slow infusions over 50 minutes.
After intra-arterial administration, inflammatory changes spreading into perivascular soft tissues were observed, indicating that intra-arterial administration of moxifloxacin should be avoided.
Moxifloxacin was genotoxic in in vitro tests using bacteria or mammalian cells. However, genotoxicity was not observed in in vivo studies, even with very high doses of moxifloxacin. Moxifloxacin showed no carcinogenic effects in animal carcinogenicity studies.
In vitro, moxifloxacin at high concentrations affected cardiac electrophysiological parameters, potentially causing QT interval prolongation.
After intravenous administration of moxifloxacin to animals at a dose of 30 mg/kg via 15-, 30-, or 60-minute infusions, a relationship between the degree of QT interval prolongation and infusion rate was observed: the shorter the infusion time, the greater the QT prolongation. QT prolongation was not observed when the 30 mg/kg dose was administered via a 60-minute infusion.
Studies on the effect of moxifloxacin on animal reproductive function have demonstrated that moxifloxacin crosses the placenta. Animal studies did not reveal teratogenic effects or impaired fertility after moxifloxacin administration. In animals, a slight increase in the frequency of spinal and rib malformations was observed, but only at a dose (20 mg/kg intravenously) associated with severe maternal toxicity. An increased incidence of pregnancy loss was observed in animals at plasma concentrations corresponding to therapeutic levels expected in humans.
It is known that quinolones, including moxifloxacin, cause damage to cartilage in large diarthrodial joints in immature animals.
Clinical Characteristics.
Indications.
Community-acquired pneumonia.
Complicated skin and skin structure infections.
Moxifloxacin should be used only when other antibacterial agents typically recommended for initial treatment of these infections are inappropriate.
Official guidelines for appropriate use of antibacterial agents should be taken into account.
Contraindications.
- Hypersensitivity to moxifloxacin, other quinolone antibiotics, or to any of the excipients of the medicinal product.
- Pregnancy or breastfeeding (see section "Use in Pregnancy or Breastfeeding").
- Pediatric age (under 18 years).
- History of tendon disorders related to prior quinolone use.
During preclinical and clinical studies, administration of moxifloxacin was associated with changes in cardiac electrophysiological parameters, manifested by QT interval prolongation. For this reason, moxifloxacin is contraindicated in patients with:
- Congenital or acquired QT prolongation;
- Electrolyte imbalance, particularly uncorrected hypokalemia;
- Clinically significant bradycardia;
- Clinically significant heart failure with reduced left ventricular ejection fraction;
- History of symptomatic arrhythmias.
Moxifloxacin must not be administered concomitantly with drugs known to prolong the QT interval (see also section "Interaction with Other Medicinal Products and Other Forms of Interaction").
Due to insufficient clinical experience, moxifloxacin is contraindicated in patients with hepatic impairment (Child–Pugh class C) and in those with transaminase elevations five times or more above the upper limit of normal.
Special Precautions.
Each vial is intended for single use only. Any unused solution must be discarded.
The following diluents have been shown to be compatible with the 400 mg moxifloxacin infusion solution: water for injection; 0.9% sodium chloride solution; 5%, 10%, and 40% glucose solutions; Ringer's solution; complex sodium lactate solutions (Hartmann's solution, lactated Ringer's solution).
Moxifloxacin infusion solution must not be administered simultaneously with other medicinal products.
The product must not be used if visible particulate matter or cloudiness is present in the solution.
Precipitation may occur during storage at cold temperatures, but the precipitate dissolves at room temperature. Therefore, storage of the infusion solution below 15°C is not recommended.
Interaction with Other Medicinal Products and Other Forms of Interaction.
Interaction with Medicinal Products
An additive effect of moxifloxacin and other medicinal products capable of inducing QTc interval prolongation cannot be excluded. This effect may lead to the development of ventricular arrhythmias, including polymorphic ventricular tachycardia of the torsades de pointes type. Therefore, the concomitant use of moxifloxacin with any of the following medicinal products is contraindicated (see also section "Contraindications"):
- Class IA antiarrhythmics (e.g., quinidine, hydroquinidine, disopyramide);
- Class III antiarrhythmics (e.g., amiodarone, sotalol, dofetilide, ibutilide);
- Antipsychotics (e.g., phenothiazines, pimozide, sertindole, haloperidol, sultopride);
- Tricyclic antidepressants;
- Certain antimicrobial agents (saquinavir, sparfloxacin, intravenous erythromycin, pentamidine, antimalarials such as halofantrine);
- Certain antihistamines (terfenadine, astemizole, mizolastine);
- Other medicinal products (cisapride, intravenous vincamine, bepridil, difemanil).
Moxifloxacin should be administered with caution to patients receiving medicinal products that may reduce potassium levels (e.g., loop and thiazide diuretics, laxatives and enemas (in high doses), corticosteroids, amphotericin B), or medicinal products associated with clinically significant bradycardia.
Following repeated administration of moxifloxacin in healthy volunteers, an increase in digoxin Cmax of approximately 30% was observed, without affecting AUC or the shape of the concentration-time curve.
In studies involving healthy volunteers and diabetic patients, concomitant oral administration of moxifloxacin and glyburide resulted in a reduction of glyburide plasma Cmax by approximately 21%. The combination of glyburide with moxifloxacin could theoretically provoke mild, short-term hyperglycemia. However, the observed pharmacokinetic changes in glyburide did not result in changes in pharmacodynamic parameters (blood glucose levels, insulin levels). Therefore, there is no clinically significant interaction between moxifloxacin and glyburide.
Change in International Normalized Ratio (INR).
Numerous cases of increased activity of oral anticoagulants have been reported in patients receiving antimicrobial agents, particularly fluoroquinolones, macrolides, tetracyclines, co-trimoxazole, and certain cephalosporins. Risk factors include infectious diseases and inflammatory processes, age, and the patient's general condition. Therefore, it is difficult to determine whether changes in INR are caused by the infection or by treatment. As a precautionary measure, INR should be monitored more frequently. Dose adjustment of the oral anticoagulant should be performed as needed.
In clinical studies, the absence of clinically significant interactions with moxifloxacin has been demonstrated for the following agents: ranitidine, probenecid, oral contraceptives, calcium supplements, parenterally administered morphine, theophylline, cyclosporine, or itraconazole.
In vitro studies using human cytochrome P450 enzymes have confirmed these results. Thus, metabolic interaction via cytochrome P450 enzymes is unlikely.
Interaction with Food
Moxifloxacin does not exhibit clinically significant interaction with food, including dairy products.
Special precautions for use.
Avoid using moxifloxacin in patients with a history of serious adverse reactions after taking drugs containing quinolones or fluoroquinolones (see section "Adverse reactions"). Treatment with moxifloxacin should be initiated in such patients only if no alternative therapy is available and after careful assessment of the benefit-risk ratio (see also section "Contraindications").
The benefits of moxifloxacin therapy, especially in mild infections, should be evaluated considering the information contained in this section.
QTc interval prolongation and clinical conditions associated with QTc interval prolongation
Moxifloxacin has been shown to prolong the QTc interval on the electrocardiogram (ECG) in some patients. The degree of QT interval prolongation may increase with higher plasma concentrations of the drug during rapid intravenous infusion. Therefore, it is essential to follow the recommended infusion duration of at least 60 minutes and not exceed the intravenous dose of 400 mg once daily. See sections "Contraindications" and "Interaction with other medicinal products and other forms of interaction" for further details.
Moxifloxacin therapy should be discontinued immediately upon the appearance of symptoms that may be related to cardiac arrhythmia, regardless of whether this is confirmed by ECG findings.
Moxifloxacin should be used with caution in patients with conditions predisposing to arrhythmia (e.g., acute myocardial ischemia), as such patients have an increased risk of ventricular arrhythmias (including polymorphic ventricular tachycardia of the torsades de pointes type) and cardiac arrest (see also sections "Contraindications" and "Interaction with other medicinal products and other forms of interaction"). Caution is also required when administering moxifloxacin to patients taking medicinal products that may reduce potassium levels (see also sections "Contraindications" and "Interaction with other medicinal products and other forms of interaction").
Moxifloxacin should be prescribed with caution to patients receiving medicinal products associated with clinically significant bradycardia (see also section "Contraindications").
Women and elderly patients may exhibit increased sensitivity to the effects of drugs that cause QTc interval prolongation, such as moxifloxacin; therefore, these patients require special attention.
Hypersensitivity/allergic reactions
Cases of hypersensitivity and allergic reactions have been reported after the first administration of fluoroquinolones, including moxifloxacin. Anaphylactic reactions may manifest as life-threatening shock even after the first dose. In case of clinical manifestations of severe hypersensitivity reactions, moxifloxacin should be discontinued immediately and appropriate treatment initiated (e.g., shock therapy).
Severe hepatic impairment
Cases of fulminant hepatitis, which may lead to liver failure (including fatal cases), have been reported during moxifloxacin therapy (see section "Adverse reactions"). If symptoms of fulminant hepatitis develop, such as rapidly progressing fatigue accompanied by jaundice, dark urine, bleeding tendency, or hepatic encephalopathy, patients should consult a physician before continuing treatment.
Liver function tests should be performed if signs of hepatic dysfunction occur.
Severe skin reactions
During moxifloxacin therapy (see section "Adverse reactions"), cases of severe skin reactions have been reported, including toxic epidermal necrolysis (also known as Lyell's syndrome), Stevens-Johnson syndrome, acute generalized exanthematous pustulosis, and drug reaction with eosinophilia and systemic symptoms (DRESS), which may be life-threatening or fatal. Patients should be informed about the signs and symptoms of severe skin reactions and closely monitored. Upon appearance of signs or symptoms suggestive of such reactions, moxifloxacin should be discontinued immediately and alternative therapy considered. If a patient develops severe skin reactions such as Stevens-Johnson syndrome, toxic epidermal necrolysis, acute generalized exanthematous pustulosis, or drug reaction with eosinophilia and systemic symptoms during moxifloxacin therapy, re-administration of moxifloxacin is absolutely contraindicated.
Patients predisposed to seizures
Quinolones are known to induce seizures. They should be prescribed with caution in patients with CNS disorders or other risk factors that may provoke seizures or lower the seizure threshold. If seizures occur, moxifloxacin should be discontinued and appropriate measures taken.
Prolonged, disabling, and potentially irreversible serious adverse reactions
Rare cases of prolonged (lasting months or years), disabling, and potentially irreversible serious adverse reactions affecting various organ systems (musculoskeletal, nervous, psychiatric, and sensory organs), sometimes multiple systems simultaneously, have been reported in patients receiving quinolones and fluoroquinolones, regardless of patient age or existing risk factors. Moxifloxacin should be discontinued immediately upon the first symptoms of any serious adverse reaction, and patients should be advised to consult a physician.
Peripheral neuropathy
Cases of sensory or sensorimotor polyneuropathy leading to paresthesia, hypaesthesia, dysesthesia, or weakness have been reported in patients receiving quinolones and fluoroquinolones. Patients taking moxifloxacin should be advised to inform their physician about the development of neuropathic symptoms such as pain, burning, tingling, numbness, or weakness before continuing treatment to prevent potentially irreversible conditions (see section "Adverse reactions").
Psychiatric reactions
Psychiatric reactions may occur even after the first dose of fluoroquinolones, including moxifloxacin. In rare cases, depression or psychiatric reactions may progress to suicidal thoughts and self-harming behaviors such as suicide attempts (see section "Adverse reactions"). If such reactions occur, moxifloxacin therapy should be discontinued and appropriate measures taken. Caution is required when prescribing moxifloxacin to patients with psychiatric disorders, including those in their medical history.
Diarrhea associated with antibiotic use, including colitis
Cases of antibiotic-associated diarrhea (AAD) and antibiotic-associated colitis (AAC), including pseudomembranous colitis and Clostridium difficile-associated diarrhea, have been observed with broad-spectrum antibiotics, including moxifloxacin. The severity of these events may range from mild diarrhea to fatal colitis. Therefore, it is important to consider this diagnosis in patients who develop severe diarrhea during or after moxifloxacin therapy. If suspected or confirmed AAD or AAC occurs, antimicrobial therapy, including moxifloxacin, should be discontinued immediately and appropriate therapeutic measures initiated. Additionally, appropriate infection control measures should be implemented to reduce transmission risk. Antimotility agents are contraindicated in patients who develop severe diarrhea.
Patients with severe myasthenia gravis
Moxifloxacin should be used with caution in patients with severe myasthenia gravis, as symptoms may be exacerbated.
Tendon inflammation and tendon rupture
Tendon inflammation and ruptures (particularly, but not limited to, Achilles tendon), sometimes bilateral, may occur during therapy with quinolones and fluoroquinolones, developing as early as 48 hours after initiation of treatment and persisting for several months after discontinuation (see sections "Contraindications" and "Adverse reactions"). The risk of tendinitis and tendon rupture is increased in elderly patients, patients with renal impairment, solid organ transplant recipients, and patients receiving concomitant corticosteroid therapy. Therefore, concurrent use of this medicinal product with corticosteroids should be avoided.
If initial symptoms of tendinitis (e.g., painful swelling or inflammation) occur, moxifloxacin should be discontinued and alternative therapy considered. Appropriate treatment (e.g., immobilization) should be initiated for the affected limb(s). Corticosteroids should not be used if symptoms of tendinopathy develop.
Aortic aneurysm and dissection, and cardiac valve regurgitation/insufficiency
Epidemiological studies report an increased risk of aortic aneurysm and dissection, particularly in elderly patients, and regurgitation of aortic and mitral valves following fluoroquinolone use. Cases of aortic aneurysm and dissection, sometimes complicated by rupture (including fatal cases), and regurgitation/insufficiency of any cardiac valve have been reported in patients receiving fluoroquinolones (see section "Adverse reactions").
Therefore, fluoroquinolones should be used only after careful benefit-risk assessment and consideration of alternative therapeutic options in patients with a positive family history of aneurysm or congenital heart valve defects, or in patients with an existing diagnosis of aneurysm and/or aortic dissection, or heart valve disease, or in the presence of other risk factors or predisposing conditions:
- both for aortic aneurysm and dissection and for cardiac valve regurgitation/insufficiency (e.g., connective tissue disorders such as Marfan syndrome or Ehlers-Danlos syndrome, Turner syndrome, Behçet’s disease, hypertension, rheumatoid arthritis, and infective endocarditis) or additionally.
- for aortic aneurysm and dissection (e.g., vascular disorders such as Takayasu arteritis or giant cell arteritis, or known atherosclerosis, or Sjögren’s syndrome) or additionally.
- for cardiac valve regurgitation/insufficiency (e.g., infective endocarditis). The risk of aortic aneurysm, dissection, and their rupture may be increased in patients receiving systemic corticosteroids concomitantly.
In case of sudden abdominal pain, chest pain, or back pain, patients should seek immediate medical attention.
Patients should be advised to seek immediate medical help if acute dyspnea, new-onset palpitations, or development of abdominal or lower limb edema occurs.
Patients with renal impairment
Moxifloxacin should be used with caution in elderly patients with renal disorders who are unable to maintain adequate fluid volume, as dehydration increases the risk of renal failure.
Visual disturbances
In case of visual deterioration or any effect on the eyes, immediate consultation with an ophthalmologist is required (see sections "Ability to affect reaction speed when driving or operating machinery" and "Adverse reactions").
Dysglycemia
As with all fluoroquinolones, deviations in blood glucose levels, both hypoglycemia and hyperglycemia, have been reported during moxifloxacin therapy (see section "Adverse reactions"). Dysglycemia occurred predominantly in elderly patients and diabetic patients receiving concomitant oral hypoglycemic agents (e.g., sulfonylureas) or insulin. Cases of hypoglycemic coma have been reported. Diabetic patients should be advised to closely monitor blood glucose levels.
Prevention of photosensitivity reactions
Photosensitivity reactions have been reported in patients receiving quinolones. However, clinical studies indicate a lower risk of photosensitivity reactions with moxifloxacin. Nevertheless, patients should avoid exposure to ultraviolet radiation or prolonged and/or intense sunlight during moxifloxacin therapy (see section "Adverse reactions").
Patients with glucose-6-phosphate dehydrogenase deficiency
Patients with glucose-6-phosphate dehydrogenase (G6PD) deficiency or a family history of this condition are prone to hemolytic reactions during quinolone therapy. Therefore, moxifloxacin should be used with caution in such patients.
Periarterial tissue inflammation
Moxifloxacin infusion solution is intended for intravenous use only. Intraarterial administration should be avoided, as periarterial tissue inflammation has been observed in preclinical studies with this route of administration.
Patients with specific complicated skin and soft tissue infections
The clinical efficacy of moxifloxacin in the treatment of severe infections associated with burns, fasciitis, and infected diabetic foot complicated by osteomyelitis has not been established.
Effect on biological tests
Moxifloxacin may affect test results for Mycobacterium spp. by inhibiting mycobacterial growth, potentially leading to false-negative results in patients taking moxifloxacin.
Patients with infections caused by methicillin-resistant Staphylococcus aureus (MRSA)
Moxifloxacin is not recommended for the treatment of infections caused by methicillin-resistant Staphylococcus aureus (MRSA). If MRSA infection is suspected or confirmed, appropriate antibacterial therapy should be initiated (see section "Pharmacodynamics").
Important information about excipients.
This medicinal product contains 787 mg (approximately 34 mmol) of sodium in one 250 ml infusion vial, equivalent to 39.35% of the maximum daily sodium intake (2 g) recommended by WHO for adults. Therefore, caution is advised when administering this product to patients on a sodium-restricted diet.
Use during pregnancy or breastfeeding.
Pregnancy
The safety of moxifloxacin use during human pregnancy has not been established. Animal studies indicate reproductive toxicity (see section "Pharmacological properties"). The potential risk in humans is unknown. Given the experimentally established risk of harmful effects of fluoroquinolones on weight-bearing cartilage in immature animals and considering the occurrence of reversible joint lesions in children treated with certain fluoroquinolones, moxifloxacin should not be administered to pregnant women (see section "Contraindications").
Breastfeeding period
There are no data on the use of moxifloxacin during breastfeeding in women. Preclinical studies show that a small amount of moxifloxacin passes into breast milk. Due to the lack of data on effects in breastfed infants and considering the experimental risk of harmful effects of fluoroquinolones on weight-bearing cartilage in immature animals, breastfeeding is contraindicated during moxifloxacin therapy (see section "Contraindications").
Fertility
Animal studies have not shown any effect on fertility (see section "Pharmacological properties").
Ability to affect reaction speed when driving or operating machinery.
Studies on the effect of moxifloxacin on the ability to drive or operate machinery have not been conducted. However, fluoroquinolones, including moxifloxacin, may affect reaction speed due to central nervous system effects (e.g., dizziness, acute transient visual loss) or acute, short-term loss of consciousness (see section "Adverse reactions"). Patients are advised to assess their individual response to moxifloxacin before driving or operating machinery.
Method of Administration and Dosage
Dosage
The recommended dosage regimen is 400 mg of moxifloxacin administered as an infusion once daily.
Initial intravenous therapy may be continued with oral administration of 400 mg moxifloxacin tablets, provided there are clinical indications for such a switch.
In clinical trials, most patients switched to oral moxifloxacin within 4 days (for community-acquired pneumonia) or 6 days (for complicated skin and soft tissue infections). The recommended total duration of intravenous and oral treatment is 7–14 days for community-acquired pneumonia and 7–21 days for complicated skin and soft tissue infections.
Method of Administration
The drug should be administered intravenously as a continuous infusion lasting at least
60 minutes (see also section "Special Instructions").
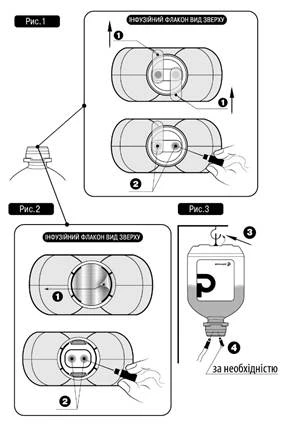
Do not insert needles into any areas of the polymer bottle other than the designated ports—only into sterile ports!
The following procedure should be followed for infusion administration:
- Remove the tamper-evident plastic cap (if present).
- Remove protective seal(s) No. 1 as shown in Fig. 1 and Fig. 2 (the manufacturer may use different types and materials for protective seals).
- Remove the needle cap and insert the needle into either of the designated ports No. 2 of the infusion vial (see Fig. 1 and Fig. 2).
- The other sterile port may be used to introduce other medicinal products into the infusion vial (No. 4, see Fig. 3), or, if necessary, to improve flow rate with an air-vent needle (No. 4, see Fig. 3).
- Hang the vial using the special ring No. 3 located at the bottom of the vial (see Fig. 3).
If clinically indicated, the infusion solution may be administered via a Y-site catheter together with compatible infusion solutions (see section "Special Safety Precautions").
Renal or Hepatic Impairment
Patients with mild to severe renal impairment, as well as patients undergoing chronic dialysis (e.g., hemodialysis or long-term ambulatory peritoneal dialysis), do not require dosage adjustment (see section "Pharmacological Properties" for further details).
There is insufficient information regarding patients with hepatic impairment (see section "Contraindications").
Other Special Patient Groups
Elderly patients and patients with low body weight do not require dosage adjustment.
Children
Due to the negative effects on cartilage in young animals (see section "Pharmacological Properties"), moxifloxacin is contraindicated in children (under 18 years of age) (see section "Contraindications").
The efficacy and safety of moxifloxacin in children and adolescents have not been established (see section "Contraindications").
Overdose
No specific interventions are recommended following accidental overdose. Symptomatic treatment should be administered in case of overdose. Since QT interval prolongation may occur, ECG monitoring is required. Concomitant administration of activated charcoal with a 400 mg dose of moxifloxacin given orally or intravenously reduces systemic bioavailability by more than 80% or 20%, respectively. Administration of activated charcoal in the early phase of absorption may effectively prevent excessive systemic exposure to moxifloxacin in cases of oral overdose.
Adverse Reactions
The adverse reactions listed below were observed during clinical trials and in the post-marketing period of moxifloxacin use at a dose of 400 mg once daily (intravenous therapy only, sequential [intravenous/oral], and oral). Adverse reactions are classified according to their frequency.
All adverse reactions, except nausea and diarrhea, occurred with a frequency of less than 3%.
All adverse reactions are listed by system organ class and frequency: very common (≥ 1/10), common (≥ 1/100 to < 1/10), uncommon (≥ 1/1,000 to < 1/100), rare (≥ 1/10,000 to < 1/1,000), very rare (< 1/10,000), frequency not known (cannot be estimated from available data).
Eye disorders*: uncommon – visual disturbances, including diplopia and blurred vision (especially during CNS-related reactions) (see section "Special Warnings and Precautions for Use"); rare – photophobia; very rare – transient visual loss (especially during CNS-related reactions) (see sections "Special Warnings and Precautions for Use" and "Effects on Ability to Drive and Use Machines"), uveitis, and bilateral acute iris transillumination (see section "Special Warnings and Precautions for Use").
Ear and labyrinth disorders*: rare – tinnitus, hearing disturbances including deafness (usually reversible).
Respiratory, thoracic and mediastinal disorders: uncommon – dyspnea (including asthmatic attacks).
Gastrointestinal disorders: common – nausea, vomiting, abdominal pain and discomfort, diarrhea; uncommon – decreased appetite and reduced food intake, constipation, dyspepsia, flatulence, gastritis, increased amylase levels; rare – dysphagia, stomatitis, antibiotic-associated colitis (including pseudomembranous colitis, which in rare cases may be associated with life-threatening complications) (see section "Special Warnings and Precautions for Use").
Hepatobiliary disorders: common – increased transaminase levels; uncommon – hepatic function abnormalities [including increased LDH (lactate dehydrogenase)], increased bilirubin, GGT (gamma-glutamyl transferase), alkaline phosphatase; rare – jaundice, hepatitis (predominantly cholestatic); very rare – fulminant hepatitis, which may lead to life-threatening hepatic failure (see section "Special Warnings and Precautions for Use").
Renal and urinary disorders: uncommon – dehydration; rare – renal function impairment (including increased blood urea nitrogen and creatinine levels), renal failure (see section "Special Warnings and Precautions for Use").
Endocrine disorders: very rare – syndrome of inappropriate antidiuretic hormone secretion (SIADH).
Metabolism and nutrition disorders: uncommon – hyperlipidemia; rare – hyperglycemia, hyperuricemia; very rare – hypoglycemia, hypoglycemic coma.
Nervous system disorders*: common – headache, dizziness; uncommon – paresthesia/dysesthesia, taste disturbances (including ageusia in rare cases), confusion and disorientation, sleep disorders (mainly insomnia), tremor, vertigo, somnolence; rare – hypoesthesia, olfactory disturbances (including loss of smell), abnormal dreams, coordination disorders (including gait disturbances due to dizziness or vertigo), seizures (including grand mal seizures) (see section "Special Warnings and Precautions for Use"), attention disturbances, speech disorders, amnesia, peripheral neuropathy and polyneuropathy; very rare – hyperesthesia.
Psychiatric disorders*: uncommon – anxiety reactions, increased psychomotor activity/agitation; rare – mood lability, depression (in rare cases with possible self-harm, manifesting as suicidal thoughts/ideation or suicide attempts), hallucinations, delirium; very rare – depersonalization, psychotic reactions (with possible self-harm, manifesting as suicidal thoughts/ideation or suicide attempts) – (see section "Special Warnings and Precautions for Use").
Cardiac disorders**: common – QT interval prolongation in patients with hypokalemia (see sections "Contraindications" and "Special Warnings and Precautions for Use"); uncommon – QT interval prolongation (see section "Special Warnings and Precautions for Use"), palpitations, tachycardia, atrial fibrillation, angina pectoris, vasodilation; rare – ventricular tachyarrhythmias, syncope (e.g., acute and transient loss of consciousness), arterial hypertension, hypotension; very rare – non-specific arrhythmia, torsades de pointes (see section "Special Warnings and Precautions for Use"), cardiac arrest (see section "Special Warnings and Precautions for Use"), vasculitis.
Blood and lymphatic system disorders: uncommon – anemia, leukopenia, neutropenia, thrombocytopenia, thrombocytosis, eosinophilia, prolonged prothrombin time/increased INR; very rare – elevated prothrombin levels/decreased INR, agranulocytosis, pancytopenia.
Immune system disorders: uncommon – allergic reactions (see section "Special Warnings and Precautions for Use"); rare – anaphylaxis, including life-threatening shock in rare cases (see section "Special Warnings and Precautions for Use"), allergic edema/angioedema (including potentially life-threatening laryngeal edema) (see section "Special Warnings and Precautions for Use").
Infections and infestations: common – superinfections associated with resistant bacteria or fungi, e.g., oral and vaginal candidiasis.
Skin and subcutaneous tissue disorders: uncommon – pruritus, rash, urticaria, dry skin; very rare – bullous skin reactions such as Stevens-Johnson syndrome or toxic epidermal necrolysis (potentially life-threatening) – (see section "Special Warnings and Precautions for Use"); frequency not known – acute generalized exanthematous pustulosis (AGEP), drug reaction with eosinophilia and systemic symptoms (DRESS) (see section "Special Warnings and Precautions for Use"), fixed drug eruption, photosensitivity reactions (see section "Special Warnings and Precautions for Use").
Musculoskeletal and connective tissue disorders*: uncommon – arthralgia, myalgia; rare – tendinitis (see section "Special Warnings and Precautions for Use"), increased muscle tone, muscle cramps, muscle weakness; very rare – tendon rupture (see section "Special Warnings and Precautions for Use"), arthritis, increased muscle rigidity as a symptom of myasthenia gravis (see section "Special Warnings and Precautions for Use"); frequency not known – rhabdomyolysis.
General disorders and administration site conditions*: common – injection and infusion site reactions; uncommon – malaise (mainly asthenia or fatigue), pain (including back, chest, pelvic, and limb pain), increased sweating, thrombophlebitis at infusion site; rare – edema.
Investigations:
* Rare cases of prolonged (months or years), disabling, and potentially irreversible serious adverse reactions have been reported in patients treated with quinolones and fluoroquinolones, regardless of age or known risk factors, affecting various systems and sensory organs, sometimes multiple (including reactions such as tendon inflammation, tendon rupture, arthralgia, limb pain, gait disturbances, neuropathy associated with paresthesia, depression, fatigue, memory impairment, sleep disorders, and disturbances of hearing, vision, taste, and smell) (see section "Special Warnings and Precautions for Use").
** Cases of aortic aneurysm and dissection, sometimes complicated by rupture (including fatal cases), and regurgitation/insufficiency of any cardiac valve have been reported in patients receiving fluoroquinolones (see section "Special Warnings and Precautions for Use").
The frequency of the following effects is higher when the drug is administered intravenously followed by oral therapy or without such transition.
Common: increased gamma-glutamyl transferase levels.
Uncommon: ventricular tachyarrhythmia, arterial hypotension, edema, antibiotic-associated colitis (including pseudomembranous colitis, which in rare cases may be associated with life-threatening complications, see section "Special Warnings and Precautions for Use"), seizures (including grand mal seizures) – (see section "Special Warnings and Precautions for Use"), hallucinations, renal function impairment (including increased blood urea nitrogen and creatinine levels), renal failure (see section "Special Warnings and Precautions for Use").
In rare cases following treatment with other fluoroquinolones, adverse effects have been reported that may also likely occur during moxifloxacin therapy: increased intracranial pressure (including idiopathic intracranial hypertension), hypernatremia, hypercalcemia, hemolytic anemia, photosensitivity reactions (see section "Special Warnings and Precautions for Use").
Reporting of suspected adverse reactions.
Reporting suspected adverse reactions after medicine authorization is important. It allows ongoing monitoring of the benefit-risk balance of the medicine. Healthcare professionals and patients or their legal representatives should report all suspected adverse reactions and/or lack of efficacy via the Automated Pharmacovigilance Information System at: https://aisf.dec.gov.ua.
Shelf life. 2 years.
Storage conditions.
Store in the original packaging at a temperature not below 15 °C and not above 25 °C. Do not freeze. Keep out of reach of children.
Incompatibilities. Moxifloxacin infusion solution must not be administered simultaneously with other incompatible solutions, including: 10% sodium chloride solution; 20% sodium chloride solution; 4.2% sodium bicarbonate solution; 8.4% sodium bicarbonate solution.
This medicinal product should not be mixed with other medicinal products except those specified in the section "Special Precautions for Handling and Disposal".
Packaging. 250 ml in a vial; 1 vial in a carton.
Prescription status. Prescription only.
Manufacturer. JSC "Pharmaceutical Company "Darnytsia".
Manufacturer's address and location of operations.
13 Borispilska Street, Kyiv, 02093, Ukraine.