Menopur
Ukraine
Table of Contents
- INSTRUCTION for medical use of the medicinal product MENOPUR® (MENOPUR®)
- Composition
- Pharmaceutical form
- Main physicochemical properties
- Pharmacotherapeutic group
- Pharmacological properties
- Pharmacodynamics
- Pharmacokinetics
- Clinical characteristics
- Indications
- Contraindications
- Interaction with other medicinal products and other forms of interaction
- Special precautions for use
- Ovarian Hyperstimulation Syndrome (OHSS)
- Multiple pregnancies
- Pregnancy loss
- Ectopic pregnancy
- Reproductive system neoplasms
- Congenital malformations
- Thromboembolic complications
- Important information about excipients
- Use during pregnancy or breastfeeding
- Effects on ability to drive and use machines
- Method of administration and dosage
- Women with anovulation (including PCOS)
- Women undergoing controlled ovarian hyperstimulation for multiple follicular development in assisted reproductive technologies (ART)
- Preparation of Menopur 600 IU and 1200 IU solution
- For this, it is necessary:
- Remove the syringe and the reconstitution needle.
- The vial with powder dissolved using one pre-filled syringe of solvent is ready for use. If the solution is not clear or contains particles, it should not be used.
- REMEMBER: since this vial contains medication sufficient for several days of therapy, you must ensure that you draw up no more than the dose prescribed by your doctor. If you have been prescribed Bravelle together with Menopur, you may mix these two medicinal products by reconstituting Menopur and then injecting the prescribed dose of Menopur into the reconstituted Bravelle solution. Draw up the mixed solution: you may then administer both medicinal products together, instead of injecting each separately.
- Your doctor or nurse will instruct you where to administer the injection (e.g., the front of the thigh, abdomen, etc.). Before injecting, disinfect the injection site using the alcohol swabs provided in the package.
- After removing the syringe, apply pressure to the injection site to stop bleeding. Gently massaging the injection site may help spread the solution under the skin. Do not dispose of used materials in household waste; they must be properly discarded.
- Menopur 1200 IU
- This should be done as follows:
- Remove the protective cap from the second pre-filled syringe containing the solvent and firmly attach the syringe to the needle secured in the vial. Slowly inject all the solvent, avoiding the formation of bubbles (Figure 5).
- Remove the reconstitution syringe and needle.
- The vial containing the powder dissolved using two pre-filled syringes with solvent is ready for use. Do not use the solution if it is not clear or contains particles.
- REMEMBER: since this vial contains medication sufficient for several days of treatment, you must ensure that you draw up no more than the dose prescribed by your doctor. If Bravelle has been prescribed together with Menopur, you may mix these two medications by reconstituting Menopur and injecting the prescribed dose of Menopur into the reconstituted Bravelle solution. Draw up the mixed solution: you may administer both medications together, instead of injecting each separately.
- Your doctor or nurse will tell you where to administer the injection (e.g., the front of the thigh, abdomen, etc.). Before injecting, disinfect the injection site using the alcohol swabs provided in the pack.
- After removing the injection syringe, apply gentle pressure to the injection site to stop bleeding. Gentle massage of the injection site will help distribute the solution under the skin. Do not dispose of used materials in regular household waste; they must be properly discarded.
- If you have administered more Menopur than prescribed, please inform your nurse or doctor. If you forget to inject Menopur, do not administer a double dose to compensate for the missed dose. Please inform your nurse or doctor.
INSTRUCTION for medical use of the medicinal product MENOPUR® (MENOPUR®)
Composition
Menopur 600 IU:
Active substance: highly purified menotropin;
1 vial of powder contains highly purified menotropin (highly purified human menopausal gonadotropin, hMG) equivalent to 600 IU of FSH (follicle-stimulating hormone) and 600 IU of LH (luteinizing hormone).
Menopur 1200 IU:
Active substance: highly purified menotropin;
1 vial of powder contains highly purified menotropin (highly purified human menopausal gonadotropin, hMG) equivalent to 1200 IU of FSH (follicle-stimulating hormone) and 1200 IU of LH (luteinizing hormone).
Excipients:
lactose monohydrate;
disodium hydrogen phosphate heptahydrate;
polysorbate 20;
1 M solution of phosphoric acid;
0.5 M solution of disodium hydrogen phosphate heptahydrate;
1 syringe of solvent contains: m-cresol, water for injections.
Pharmaceutical form
Lyophilized powder for solution for injection.
Main physicochemical properties
Powder: white or almost white lyophilisate in the form of a cake;
Solvent: clear, colourless solution.
Pharmacotherapeutic group
Gonadotropins and other ovulation stimulants.
Human menopausal gonadotropin.
ATC code: G03GA02.
Pharmacological properties
Pharmacodynamics
Menopur contains human chorionic gonadotropin (hCG), a natural hormone found in the urine of postmenopausal women, which primarily provides LH activity. Menotropin, possessing both FSH and LH activity, induces follicular growth and development, as well as gonadal steroid secretion in women who do not suffer from primary ovarian insufficiency. FSH initially initiates the resumption of follicular growth at the early folliculogenesis stage, while LH is essential for ovarian steroidogenesis and participates in physiological processes leading to the development of a suitable preovulatory follicle.
Follicular growth can be stimulated by FSH even in the complete absence of LH; however, the resulting follicles develop abnormally. Additionally, such stimulation is associated with low estradiol levels, leading to inadequate luteinization.
In line with the LH-driven enhancement of steroidogenesis, in IVF/ICSI cycles with pituitary desensitization, estradiol levels during Menopur treatment are higher than with recombinant FSH preparations. This should be considered when monitoring patient response via estradiol level measurements. No differences in achieved estradiol levels were observed when using low-dose ovulation induction protocols in anovulatory patients.
Pharmacokinetics
The pharmacokinetic profile of FSH in Menopur has been studied. After 7 days of administration of 150 IU Menopur to healthy female volunteers with desensitized pituitary glands, maximum plasma concentrations of FSH (baseline-corrected) (mean ± SD) were 8.9 ± 3.5 IU/L and 8.9 ± 3.5 IU/L following subcutaneous and intramuscular administration, respectively. Maximum FSH concentrations were reached within 7 hours for both routes of administration. After repeated dosing, the elimination half-life of FSH was 30 ± 11 hours and 27 ± 9 hours following subcutaneous and intramuscular administration, respectively (mean ± SD).
Although individual LH concentrations increase over time after Menopur administration, available data are insufficient for pharmacokinetic analysis. Menotropin is primarily eliminated by the kidneys. Pharmacokinetics of Menopur in patients with impaired renal or hepatic function have not been studied.
Clinical characteristics
Indications
Treatment of infertility in the following clinical conditions:
- Anovulation, including polycystic ovary syndrome (PCOS), in women who are unresponsive to clomiphene citrate treatment;
- Controlled ovarian hyperstimulation to induce the development of multiple follicles in the context of assisted reproductive technologies (ART) (e.g., in vitro fertilization/embryo transfer (IVF/ET), gamete intrafallopian transfer (GIFT), and intracytoplasmic sperm injection (ICSI));
- Stimulation of follicular growth in women with hypogonadotropic hypogonadism.
Contraindications
Menopur is contraindicated in women:
- with hypersensitivity to the active substance or to any of the excipients;
- with pituitary or hypothalamic tumours;
- with ovarian, uterine, or breast carcinoma;
- with gynecological bleeding of unknown origin;
- with premature menopause;
- with ovarian cysts or enlarged ovaries not related to polycystic ovary syndrome (PCOS);
- during pregnancy or breastfeeding.
Menopur should not be administered when a favourable treatment outcome is unlikely:
- in cases of primary ovarian insufficiency;
- in congenital malformations of the reproductive organs incompatible with pregnancy;
- in uterine fibroids incompatible with pregnancy.
Interaction with other medicinal products and other forms of interaction
Drug interactions of Menopur in humans have not been studied. Despite the lack of clinical experience, concomitant use of Menopur and clomiphene citrate is expected to enhance follicular response. When using GnRH agonists for pituitary desensitization, higher doses of Menopur may be required to achieve adequate follicular response.
Special precautions for use
Due to its potent gonadotropic activity, which may cause mild to moderate adverse effects, Menopur should be administered under the supervision of physicians specialized in infertility treatment and experienced in such therapy. Gonadotropin treatment requires careful medical monitoring and regular assessment of ovarian response, including ultrasound examinations, possibly combined with serum estradiol level measurements.
Ovarian response to menotropin administration varies significantly among patients, with some showing poor response. The lowest effective dose corresponding to the treatment goal should be used. The first Menopur injection should be administered under direct medical supervision.
Before initiating treatment, the diagnosis of infertility in the couple should be confirmed, and contraindications to pregnancy should be ruled out. In particular, patients should be evaluated for hypothyroidism, adrenal insufficiency, hyperprolactinemia, and pituitary or hypothalamic tumours, and appropriate treatment initiated if necessary.
In patients undergoing follicular growth stimulation for anovulatory infertility or ART procedures, ovarian enlargement or hyperstimulation may occur. These risks can be minimized by strictly adhering to recommended dosing and administration regimens and careful therapy monitoring. Assessment of follicular development and maturation must be performed by a physician experienced in interpreting relevant tests.
Ovarian Hyperstimulation Syndrome (OHSS)
OHSS is a distinct clinical condition differing from uncomplicated ovarian enlargement. OHSS is a syndrome with varying degrees of severity. Signs include ovarian enlargement, high serum sex hormone levels, and increased vascular permeability, potentially leading to fluid accumulation in the peritoneal, pleural, and, rarely, pericardial cavities.
Severe OHSS may present with abdominal pain, abdominal distension, marked ovarian enlargement, weight gain, dyspnea, oliguria, and gastrointestinal symptoms such as nausea, vomiting, and diarrhea. Clinical examination may reveal hypovolemia, hemoconcentration, electrolyte imbalance, ascites, hemoperitoneum, pleural effusion, hydrothorax, acute respiratory distress, and thromboembolism.
Excessive ovarian response to gonadotropin treatment rarely leads to OHSS until hCG is administered to trigger ovulation. Therefore, hCG should not be administered in cases of ovarian hyperstimulation; patients should be advised to abstain from sexual intercourse or use barrier contraception for at least 4 days.
OHSS can progress rapidly (within 24 hours to several days) and become severe; thus, patients should remain under medical supervision for at least 2 weeks after hCG administration. The risk of ovarian hyperstimulation and multiple pregnancy can be minimized by adhering to recommended dosing and administration regimens and careful treatment monitoring.
In ART procedures, the risk of hyperstimulation can be reduced by aspirating all follicles before ovulation. OHSS may become more severe and prolonged if pregnancy occurs. OHSS most commonly develops after completion of hormonal therapy, peaking approximately 7–10 days after treatment ends. OHSS usually resolves spontaneously with the onset of menstruation. In cases of severe OHSS, gonadotropin treatment should be discontinued. If symptoms persist, hospitalization and specific OHSS treatment are required. OHSS is more frequently observed in women with polycystic ovary syndrome (PCOS).
Multiple pregnancies
Multiple pregnancies, especially higher-order multiples, increase the risk of complications for both mother and child. The frequency of multiple pregnancies is higher in patients undergoing gonadotropin-induced ovulation compared to natural conception. Most multiple pregnancies are twin pregnancies. Careful monitoring of ovarian response is recommended to reduce the risk of multiple pregnancies. In ART procedures, the risk of multiple pregnancies primarily depends on the number of embryos transferred, embryo quality, and patient age. Patients should be informed about the potential risk of multiple pregnancies before treatment initiation.
Pregnancy loss
The frequency of pregnancy loss—preterm delivery and spontaneous abortion—is higher in patients undergoing follicular stimulation as part of ART procedures compared to the general patient population.
Ectopic pregnancy
Women with a history of tubal disease are at risk of ectopic pregnancy, regardless of whether conception occurs spontaneously or following infertility treatment. Following IVF, the reported incidence of ectopic pregnancy is 2–5%, compared to 1–1.5% in the general population.
Reproductive system neoplasms
Cases of benign and malignant neoplasms of the ovaries and other reproductive organs have been reported in women treated with multiple drugs for infertility. It has not yet been established whether gonadotropin treatment increases the baseline risk of such tumours in infertile women.
Congenital malformations
The prevalence of congenital malformations following ART may be slightly higher than after spontaneous conception. This is believed to result from differences in parental characteristics (e.g., maternal age, sperm parameters) and multiple pregnancies.
Thromboembolic complications
Women with established risk factors for thromboembolic complications—such as a history of thromboembolic disease, familial thromboembolic disorders, severe obesity (BMI > 30 kg/m²), or thrombophilia—are at increased risk of venous or arterial thromboembolism during or after gonadotropin treatment. In such patients, the benefits of gonadotropin use should be weighed against potential risks. However, it should be noted that pregnancy itself is also a risk factor for thromboembolic complications.
Important information about excipients
This medicinal product contains less than 1 mmol (23 mg) of sodium per dose, i.e., essentially sodium-free.
Use during pregnancy or breastfeeding
Menopur is contraindicated in pregnant women. Data on the use of menotropin in pregnant women are lacking or limited. Animal studies on the effects of Menopur during pregnancy have not been conducted. Menopur is contraindicated in breastfeeding women.
Effects on ability to drive and use machines
Appropriate studies have not been conducted. However, it is unlikely that Menopur affects the ability of patients to drive or perform tasks requiring high attention and rapid reaction.
Method of administration and dosage
Treatment with Menopur should be initiated under the supervision of a physician experienced in infertility treatment. Menopur 600 IU and Menopur 1200 IU are intended for subcutaneous administration after reconstitution with solvent, as the syringe provided in the package is designed only for subcutaneous injection. The powder must be reconstituted before use. The prepared solution is for multiple-dose use and can be stored for up to 28 days. Vigorous shaking should be avoided during reconstitution. The solution should not be used if it is cloudy or contains particles.
The dosing regimens described below are applicable for both subcutaneous and intramuscular administration. Ovarian response to exogenous gonadotropins is highly individual, making it impossible to establish a single universal dosing regimen. Therefore, dosing should be individualized based on ovarian response. Menopur can be used as monotherapy or in combination with a gonadotropin-releasing hormone (GnRH) agonist or antagonist. Recommended doses and treatment duration depend on the treatment protocol used.
Women with anovulation (including PCOS)
The goal of Menopur therapy is the development of a single Graafian follicle, from which an oocyte is released after administration of human chorionic gonadotropin (hCG). Menopur therapy should begin within the first 7 days of the menstrual cycle. The recommended daily starting dose is 75–150 IU, maintained for at least 7 days. Subsequent treatment should be individualized based on ovarian response and clinical monitoring (including ultrasound, possibly combined with estradiol level measurements). Dose adjustments should not be made more frequently than every 7 days. Recommended incremental dose increases are 37.5 IU, not exceeding 75 IU. The maximum daily dose should not exceed 225 IU.
If an inadequate response is observed after 4 weeks of treatment, the therapeutic cycle should be discontinued, and a new cycle initiated with a higher dose than used in the previous cycle. Upon achieving optimal response, a single injection of hCG at a dose of 5000–10000 IU should be administered 1 day after the last Menopur injection. Patients are advised to have sexual intercourse on the day of hCG injection and the following day. Alternatively, intrauterine insemination (IUI) may be performed.
If excessive response to Menopur occurs, treatment should be discontinued and hCG administration withheld (see section "Special precautions for use"). Patients should use barrier contraception or abstain from sexual intercourse until the onset of the next menstrual bleeding.
Women undergoing controlled ovarian hyperstimulation for multiple follicular development in assisted reproductive technologies (ART)
Based on clinical trial results using Menopur with GnRH agonist desensitization, Menopur therapy should begin approximately 2 weeks after starting the agonist. During the first 5 days of treatment, a daily dose of 150–225 IU of Menopur is recommended. Subsequent dosing should be individualized based on clinical monitoring (including ultrasound, possibly combined with estradiol levels), with dose increments not exceeding 150 IU. The maximum daily dose should not exceed 450 IU. In most cases, treatment should not be continued beyond 20 days.
For protocols without GnRH agonist desensitization, Menopur therapy should begin on day 2 or 3 of the menstrual cycle. The same dosing and administration regimen as for desensitization protocols is recommended.
When a sufficient number of follicles of appropriate size are present, a single injection of hCG up to 10000 IU should be administered to induce final follicular maturation. Patients should remain under close medical observation for at least 2 weeks after hCG administration.
If excessive response to Menopur occurs, treatment should be discontinued and hCG administration withheld (see section "Special precautions for use"). Patients should use barrier contraception or abstain from sexual intercourse until the onset of the next menstrual bleeding.
Preparation of Menopur 600 IU and 1200 IU solution
If your clinic has instructed you to self-administer Menopur injections, you must follow all provided instructions. Menopur is intended for subcutaneous injection, preferably in the abdominal area. The first Menopur injection should be administered under medical or nursing supervision. Patients must be thoroughly familiar with the administration method. Only well-motivated and trained patients should self-administer the drug and should remain in contact with their physician.
Menopur 600 IU:
Menopur is supplied as a powder in a vial and must be reconstituted before injection using one syringe filled with solvent. The solvent to be used for reconstitution is provided in a pre-filled syringe in the package. Menopur 600 IU should be reconstituted using one pre-filled syringe of solvent. After reconstitution, the vial contains sufficient medication for several days of therapy. Ensure that you draw up only the amount prescribed by your physician. Your physician has prescribed a dose of Menopur in IU (units). To obtain the required dose, use one of the 9 provided administration syringes, graduated in IU (units) of FSH/LH.
| |

For this, it is necessary:
| |
|
|
|
|
|
1 |
2 |
3 |
4 |
||





-
Remove the protective cap from the vial containing the powder and the rubber cap from the pre-filled syringe containing the solvent (Figure 1).
-
Firmly attach the needle (reconstitution needle) to the pre-filled syringe containing the solvent and remove the protective cap from the needle (Figure 2).
-
Insert the needle vertically through the center of the rubber stopper on the vial containing the powder and slowly inject the entire amount of solvent, avoiding the formation of bubbles (Figure 3).
-
After adding the solvent, a slight overpressure may develop inside the vial. Therefore, release the syringe plunger and allow it to rise on its own for approximately 10 seconds. This will help relieve the overpressure in the vial (Figure 4).
Remove the syringe and the reconstitution needle.
| |
|
|
|
|
5 |
6 |
7 |
8 |
|





- The powder should dissolve quickly (within 2 minutes), forming a clear solution. Although this usually occurs when only a few drops of solvent are added, the solvent should be added in the full volume. To facilitate dissolution of the powder, the solution should be mixed by gently rotating the vial (Figure 5). Do not shake, as this may cause formation of air bubbles.
The vial with powder dissolved using one pre-filled syringe of solvent is ready for use. If the solution is not clear or contains particles, it should not be used.
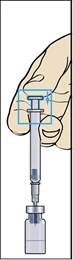
- Take the injection syringe with the attached needle and insert the needle vertically into the center of the vial. The injection syringe already contains a small amount of air, which should be injected into the vial above the liquid. Invert the vial upside down and draw the prescribed dose of Menopur into the injection syringe (Figure 6).
REMEMBER: since this vial contains medication sufficient for several days of therapy, you must ensure that you draw up no more than the dose prescribed by your doctor. If you have been prescribed Bravelle together with Menopur, you may mix these two medicinal products by reconstituting Menopur and then injecting the prescribed dose of Menopur into the reconstituted Bravelle solution. Draw up the mixed solution: you may then administer both medicinal products together, instead of injecting each separately.
- Remove the syringe from the vial and draw a small amount of air into the syringe (Figure 7).
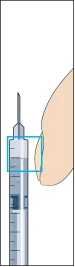
- Gently tap the injection syringe to allow all air bubbles to rise to the hub. Carefully expel all air by pushing the plunger until the first drop of liquid appears at the needle tip.
Your doctor or nurse will instruct you where to administer the injection (e.g., the front of the thigh, abdomen, etc.). Before injecting, disinfect the injection site using the alcohol swabs provided in the package.
| |
9 |
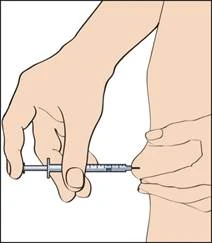
- To administer the injection, pinch the skin to create a skin fold and insert the needle in one quick motion at a 90-degree angle to the body. Gently press the plunger to inject the solution (Figure 9), then remove the syringe.
After removing the syringe, apply pressure to the injection site to stop bleeding. Gently massaging the injection site may help spread the solution under the skin. Do not dispose of used materials in household waste; they must be properly discarded.
- To administer the next injection of the reconstituted Menopur solution, repeat steps 6–9.
Menopur 1200 IU
Menopur is supplied as a powder in a vial. Before injection, it must be reconstituted using two pre-filled syringes containing solvent. The solvents to be used for reconstituting Menopur are provided in pre-filled syringes within the package. Menopur 1200 IU must be reconstituted before use with two pre-filled syringes containing solvent. After reconstitution of the powder with the solvent, this vial contains sufficient medication for several days of therapy. Therefore, you must ensure that you draw up no more than the amount prescribed by your doctor. Your doctor has prescribed your Menopur dose in IU (international units). To obtain the required dose, you must use one of the provided 18 administration syringes, graduated in IU (international units) of FSH/LH.
| |

This should be done as follows:
| |
|
|
1 |
2 |
|



- Remove the protective cap from the vial containing the powder and the rubber cap from one of the pre-filled syringes with solvent (Figure 1).
- Firmly attach the needle (reconstitution needle) to the pre-filled syringe with solvent and remove the protective cap from the needle (Figure 2).
| |
|
|
|
|
|
|
3 |
4 |
5 |
6 |
|||
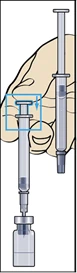




- Insert the needle vertically through the center of the rubber stopper on the vial containing the powder and slowly inject all of the solvent, avoiding the formation of bubbles (Figure 3).
- After adding the solvent, a slight overpressure may develop in the vial. Therefore, release the syringe plunger, allowing it to rise on its own for approximately 10 seconds. This will help eliminate the overpressure in the vial (Figure 4).
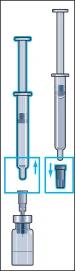
- Carefully disconnect the syringe from the needle by twisting it, leaving the needle in the vial.
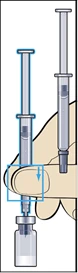
Remove the protective cap from the second pre-filled syringe containing the solvent and firmly attach the syringe to the needle secured in the vial. Slowly inject all the solvent, avoiding the formation of bubbles (Figure 5).
- After adding the solvent, a slight overpressure may develop in the vial. Therefore, release the syringe plunger, allowing it to rise on its own for approximately 10 seconds. This will help eliminate the overpressure in the vial (Figure 6).
Remove the reconstitution syringe and needle.
| |
|
|
|
|
7 |
8 |
9 |
10 |
|





- The powder should dissolve quickly (within 2 minutes), forming a clear solution. Although this usually occurs upon adding just a few drops of solvent, the solvent should be added in the full volume. To facilitate dissolution of the powder, gently swirl the vial (Figure 7). Do not shake, as this may cause formation of air bubbles.
The vial containing the powder dissolved using two pre-filled syringes with solvent is ready for use. Do not use the solution if it is not clear or contains particles.
- Take the injection syringe with the pre-attached needle and insert the needle vertically into the center of the vial. The injection syringe already contains a small amount of air, which should be injected into the vial above the liquid. Invert the vial and draw the prescribed dose of Menopur into the injection syringe (Figure 8).
REMEMBER: since this vial contains medication sufficient for several days of treatment, you must ensure that you draw up no more than the dose prescribed by your doctor. If Bravelle has been prescribed together with Menopur, you may mix these two medications by reconstituting Menopur and injecting the prescribed dose of Menopur into the reconstituted Bravelle solution. Draw up the mixed solution: you may administer both medications together, instead of injecting each separately.
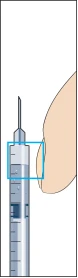
- Remove the syringe from the vial and draw a small amount of air into the syringe (Figure 9).
- Gently tap the injection syringe to allow all air bubbles to rise into the needle hub (Figure 10). Carefully expel all air and continue pressing until the first drop of liquid appears at the needle tip.
Your doctor or nurse will tell you where to administer the injection (e.g., the front of the thigh, abdomen, etc.). Before injecting, disinfect the injection site using the alcohol swabs provided in the pack.
| |
11 |
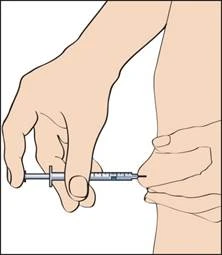
- To administer the injection, pinch the skin to create a skin fold and insert the needle quickly at a 90-degree angle to the body. Carefully press the plunger to inject the solution (Figure 11), then remove the syringe.
After removing the injection syringe, apply gentle pressure to the injection site to stop bleeding. Gentle massage of the injection site will help distribute the solution under the skin. Do not dispose of used materials in regular household waste; they must be properly discarded.
- To administer the next injection of the reconstituted Menopur solution, repeat steps 8–11.
If you have administered more Menopur than prescribed, please inform your nurse or doctor. If you forget to inject Menopur, do not administer a double dose to compensate for the missed dose. Please inform your nurse or doctor.
General instructions
Do not administer the prepared solution if it contains particles or appears cloudy. Any unused medicine or waste should be disposed of according to local regulations.
Children
This medicine is not intended for use in children.
Overdose
Treatment with LH may lead to ovarian hyperstimulation, which becomes clinically apparent only after administration of hCG to induce ovulation (see section "Adverse reactions").
Mild hyperstimulation (Grade I) is characterized by moderate ovarian enlargement (ovary size 5–7 cm), excessive steroid secretion, and abdominal pain. No specific treatment is required, but patients should be informed about symptoms of hyperstimulation and closely monitored.
Moderate hyperstimulation (Grade II) with ovarian cysts (ovary size 8–10 cm) presents with abdominal pain, nausea, and vomiting. Symptomatic treatment and possibly intravenous fluid replacement may be required.
Severe hyperstimulation (Grade III) with large ovarian cysts (ovary size >10 cm), accompanied by ascites, hydrothorax, abdominal distension, abdominal pain, dyspnea, electrolyte retention, increased hemoglobin concentration, increased blood viscosity, and platelet aggregation with risk of thromboembolism, requires hospitalization.
Adverse reactions
In clinical trials, the most frequently reported adverse reactions with Menopur were OHSS, abdominal pain, headache, and injection site reactions and pain, each occurring at a frequency of up to 5%.
The main adverse reactions observed in women treated with Menopur in clinical trials are listed below, categorized by frequency: very common (≥1/10), common (≥1/100 to <1/10), uncommon (≥1/1000 to <1/100), rare (≥1/10,000 to <1/1000), very rare (<1/10,000), and frequency not known.
- Eye disorders: Frequency not known – visual disturbancesa
- Gastrointestinal disorders: Common – abdominal pain, bloating, nausea; Uncommon – vomiting, abdominal discomfort, diarrhea
- General disorders and administration site conditions: Common – injection site reactionsb; Uncommon – weakness; Frequency not known – pyrexia, malaise
- Immune system disorders: Frequency not known – hypersensitivity reactionsc
- Investigations: Frequency not known – weight gain
- Musculoskeletal and connective tissue disorders: Frequency not known – musculoskeletal paind
- Nervous system disorders: Common – headache; Uncommon – dizziness
- Reproductive system and breast disorders: Common – OHSSe, pelvic painf; Uncommon – ovarian cyst, breast discomfortg; Frequency not known – ovarian torsione
- Skin and subcutaneous tissue disorders: Rare – acne, rash; Frequency not known – pruritus, urticaria
- Vascular disorders: Uncommon – hot flushes; Frequency not known – thromboembolisme
a Isolated cases of transient amaurosis, diplopia, mydriasis, scotoma, photopsia, floaters, blurred vision, and visual disorders have been reported as visual disturbances during the post-marketing period.
b Injection site reactions were most commonly reported as injection site pain.
c There have been reports of isolated cases of localized or generalized allergic reactions, including anaphylactic reactions, accompanied by corresponding symptoms.
d Musculoskeletal pain includes arthralgia, back pain, neck pain, and limb pain.
e In clinical trials with Menopur, gastrointestinal symptoms associated with OHSS such as bloating, discomfort, nausea, vomiting, and diarrhea were reported. Cases of severe OHSS-related ascites, pelvic fluid accumulation, pleuritis, dyspnea, oliguria, thromboembolic events, and ovarian torsion have been reported as rare complications.
f Pelvic symptoms include ovarian pain and uterine prolapse.
g Breast-related symptoms include breast pain, breast tenderness, discomfort, nipple pain, and breast swelling.
Shelf life
3 years. After reconstitution, the solution may be stored for up to 28 days at a temperature not exceeding 25°C.
Storage conditions
Keep out of the reach of children. Store in the refrigerator (2–8°C) in the original packaging. Do not freeze.
Incompatibilities
The reconstituted Menopur solution should not be mixed with other medicinal products except with urofollitropin Bravelle (FSH) manufactured by Ferring. Studies have shown that co-administration of Bravelle and Menopur does not significantly affect the expected bioavailability of either product.
Packaging
- Menopur 600 IU: 1 vial of powder with 1 pre-filled syringe containing 1 mL solvent, 1 diluent needle, and 9 injection syringes.
- Menopur 1200 IU: 1 vial of powder with 2 pre-filled syringes containing 1 mL solvent each, 1 diluent needle, and 18 injection syringes.
Prescription category
Prescription only.
Manufacturer
Ferring GmbH, Germany.
Manufacturer's address
Wittland 11, 24109 Kiel, Germany.