Izifri
Ukraine
Table of Contents
INSTRUCTIONS FOR MEDICAL USE OF THE MEDICINAL PRODUCT Izifri® (IziFri)
Composition:
Active substance: tiotropium bromide;
1 blister contains: tiotropium bromide monohydrate - 0.016 mg (equivalent to tiotropium - 0.013 mg); 10 mcg/dose, 1 dose per blister;
Excipient: lactose monohydrate.
Pharmaceutical form. Powder for inhalation, metered.
Main physico-chemical properties: a white plastic device containing 30 individual aluminum blisters filled with white powder. The device is placed in an aluminum pouch containing a desiccant.
Pharmacotherapeutic group. Medicinal products for the treatment of obstructive airway diseases, inhaled agents. Anticholinergic agents.
ATC code R03BB04.
Pharmacological properties.
Pharmacodynamics.
Mechanism of action. Tiotropium is a specific long-acting anticholinergic agent. Tiotropium has similar affinity for all muscarinic receptor subtypes (from M1 to M5). In the airways, inhibition of M3 receptors leads to relaxation of smooth muscle. In preclinical in vitro and in vivo studies, the bronchoprotective effect was dose-dependent and lasted more than 24 hours.
The duration of effect is due to very slow dissociation from M3 receptors; the half-life of tiotropium is significantly longer than that of ipratropium. As a quaternary ammonium anticholinergic, tiotropium is locally (broncho-) selective when administered by inhalation, demonstrating an acceptable therapeutic range before systemic anticholinergic effects occur. Dissociation from M2 receptors is faster than from M3 receptors in functional in vitro studies. M3 is a more favorable (kinetically controlled) receptor subtype for selectivity than M2. High activity and slow dissociation from receptors clinically correlate with significant and prolonged bronchodilation in patients with chronic obstructive pulmonary disease (COPD).
Pharmacodynamic effects. Bronchodilation after inhalation of tiotropium is primarily a local effect on the airways and is not systemic.
With once-daily administration of tiotropium, significant improvement in lung function (increase in forced expiratory volume in one second (FEV1) and forced vital capacity) was observed within 30 minutes after the first dose, with effects lasting 24 hours. Pharmacodynamic steady state is achieved within one week. In most patients, bronchodilation occurs by the third day.
Based on daily measurements, tiotropium significantly improves morning and evening peak expiratory flow.
Improved lung function is maintained without evidence of tolerance.
Bronchodilation persists over the 24-hour dosing interval compared to placebo. This was independent of whether tiotropium was administered in the morning or evening.
Tiotropium significantly reduces dyspnea; improvement was maintained throughout the treatment period.
Tiotropium significantly reduces the number of COPD exacerbations and prolongs the time to first severe exacerbation.
Tiotropium significantly improves health-related quality of life; improvement was maintained throughout the treatment period.
Tiotropium significantly reduces the number of hospitalizations due to COPD exacerbations and delays the time to first hospitalization.
In two studies, tiotropium significantly improved symptom-limited exercise tolerance by 19.7% and 28.3%.
In a study evaluating tiotropium at doses of 18 mcg and 54 mcg (three times 18 mcg) over 12 days, no QT interval prolongation was observed on electrocardiogram.
In a four-year study involving 5993 patients, tiotropium maintained improvement in FEV1 throughout the study period, although it did not alter the annual rate of decline in FEV1.
During treatment, mortality risk decreased by 16%. The overall incidence of death was 4.79 per 100 patient-years in the placebo group compared to 4.10 per 100 patient-years in the tiotropium group (risk ratio (tiotropium/placebo) 0.84, 95% CI – 0.73; 0.97). Tiotropium treatment reduced the risk of respiratory failure by 19% (2.09 vs. 1.68 events per 100 patient-years, relative risk (tiotropium/placebo) – 0.81, 95% CI – 0.65; 1.00).
Pharmacokinetics.
Tiotropium is a quaternary ammonium compound with moderate water solubility. Tiotropium is administered as a dry powder for inhalation. With inhalation, the majority of the dose deposited is swallowed and absorbed through the gastrointestinal tract, while a smaller portion reaches the lungs.
Absorption. After inhalation of the dry powder, absolute bioavailability is 19.5%, indicating high bioavailability of the fraction reaching the lungs. Absolute bioavailability of orally administered tiotropium solution is 2–3%. Maximum plasma concentration of tiotropium is observed within 5–7 minutes after inhalation.
At steady state, the maximum plasma concentration of tiotropium in patients with COPD is 12.9 pg/mL and declines rapidly according to a multicompartment model. The minimum plasma concentration of tiotropium at steady state is 1.71 pg/mL. Systemic exposure after inhalation of tiotropium as dry powder is similar to that after inhalation of tiotropium solution.
Distribution. 72% of the drug is plasma protein-bound. The volume of distribution is 32 L/kg. Local concentration in the lungs is unknown, but based on the route of administration, high concentrations in the lungs are expected. Animal studies have shown that tiotropium does not significantly cross the blood-brain barrier.
Biological transformation. The extent of biotransformation is low, as 74% of unchanged substance is excreted in urine after intravenous administration to healthy volunteers. As an ester, tiotropium undergoes non-enzymatic hydrolysis to N-methylscopolinol and dithienylglycolic acid, neither of which binds to muscarinic receptors.
Further in vitro studies using liver microsomes and hepatocytes show that tiotropium (<20% of the dose after intravenous administration) is metabolized via cytochrome P450-dependent oxidation and subsequent glutathione conjugation into various phase II metabolites. This enzymatic pathway may be inhibited by CYP450 2D6 (and 3A4) inhibitors such as quinidine, ketoconazole, and gestodene. CYP450 2D6 and 3A4 are involved in metabolic transformations responsible for elimination of a minor portion of the dose. Tiotropium, even at supratherapeutic concentrations, does not inhibit cytochrome P450 1A1, 1A2, 2B6, 2C9, 2C19, 2D6, 2E1, or 3A in liver microsomes.
Elimination. The effective half-life of tiotropium ranges between 27 and 45 hours after administration to patients with COPD. Total clearance was 880 mL/min after intravenous administration to young healthy volunteers. After intravenous administration, tiotropium is primarily excreted unchanged in urine. After inhalation of dry powder, urinary excretion of unchanged drug is 7% (1.3 mcg) of the inhaled dose over 24 hours; the remainder is not absorbed from the intestine and is excreted in feces. Renal clearance of tiotropium exceeds creatinine clearance, indicating active renal excretion. After repeated daily inhalation in patients with COPD, pharmacokinetic steady state is reached within 7 days, with no further accumulation.
Linearity/non-linearity. Tiotropium exhibits linear pharmacokinetic properties within the therapeutic range, regardless of the pharmaceutical form.
Pharmacokinetics in elderly patients. As with all other drugs primarily excreted via the kidneys, renal clearance of tiotropium is reduced in elderly patients (365 mL/min in COPD patients <65 years vs. 271 mL/min in COPD patients ≥65 years). This does not result in a corresponding increase in AUC0–6,ss or Cmax,ss values.
Pharmacokinetics in patients with renal impairment. Once-daily inhaled tiotropium at steady state in COPD patients with mild renal impairment (creatinine clearance 50–80 mL/min) resulted in a slight increase in AUC0–6,ss (1.8–30%) and similar Cmax values compared to patients with normal renal function (creatinine clearance >80 mL/min).
In COPD patients with moderate or severe renal impairment (creatinine clearance <50 mL/min), intravenous tiotropium leads to a doubling of total exposure (AUC0–4h increased by 82%, Cmax increased by 52%) compared to patients with normal renal function, confirmed by plasma concentration data after dry powder inhalation.
Pharmacokinetics in patients with hepatic impairment. Hepatic insufficiency has no significant effect on the pharmacokinetics of tiotropium. Tiotropium is predominantly eliminated via renal excretion (up to 74% in young healthy volunteers) and by simple non-enzymatic ester cleavage into metabolites that do not bind to muscarinic receptors.
Japanese COPD patients. In cross-study comparisons, the mean maximum plasma concentration of tiotropium 10 minutes after dosing at steady state was 20–70% higher in Japanese patients compared to Europeans after tiotropium inhalation. However, there were no signs of increased mortality or cardiac risk in Japanese patients compared to Europeans. Pharmacokinetic data for other races or ethnic groups are insufficient.
Pharmacokinetic/pharmacodynamic relationship. There is no direct relationship between pharmacokinetics and pharmacodynamics.
Clinical characteristics.
Indications.
Maintenance bronchodilator therapy for symptomatic relief in chronic obstructive pulmonary disease (COPD).
Contraindications.
Contraindicated in patients with known hypersensitivity to tiotropium bromide, atropine or its derivatives (such as ipratropium or oxitropium), or to any of the excipients of the medicinal product.
Interaction with other medicinal products and other forms of interaction.
Although formal drug interaction studies have not been conducted, tiotropium bromide has been used concomitantly with other medications (sympathomimetic bronchodilators, methylxanthines, oral and inhaled corticosteroids used in the treatment of COPD) without clinical evidence of interaction with other medicinal products.
It has not been established that the use of long-acting beta2-adrenergic agonists or inhaled corticosteroids alters tiotropium exposure.
However, the co-administration of Isifree® with other anticholinergic medicinal products has not been studied; therefore, such use is not recommended.
Special precautions for use.
Izifree® is a bronchodilator that should be administered once daily for maintenance therapy and should not be used for initial treatment of acute bronchospasm attacks.
Immediate-type hypersensitivity reactions may occur after administration of Izifree®.
As with other anticholinergic agents, Izifree® should be used with caution in patients with narrow-angle glaucoma, benign prostatic hyperplasia, or bladder neck obstruction (see section "Adverse reactions").
Inhaled medications may induce bronchospasm caused by inhalation.
The drug should be used with caution in the following patients: those who recently suffered myocardial infarction (<6 months); patients with any unstable or life-threatening arrhythmia, or arrhythmia requiring intervention or change in therapy within the past year; and patients hospitalized due to heart failure (NYHA class III or IV) within the last year. These patients were excluded from clinical trials. Anticholinergic effects may be harmful in such conditions.
Since plasma concentrations of tiotropium bromide increase in patients with moderate to severe renal impairment (creatinine clearance ≤ 50 mL/min), Izifree® should be used only if the expected benefit outweighs the potential risk. Data on long-term use of Izifree® in patients with renal impairment are lacking (see section "Pharmacokinetics").
Patients should avoid getting the powder into their eyes. This may precipitate or worsen narrow-angle glaucoma, cause eye pain or discomfort, temporary blurred vision, perception of halos or colored images, in combination with eye redness due to conjunctival or corneal hyperemia.
If any of these symptoms appear in any combination, use of tiotropium bromide should be discontinued immediately and specialized medical help should be sought without delay.
Dry mouth, which may occur during anticholinergic therapy, may potentially be associated with dental caries in the long term.
Izifree® should not be used more than once daily.
Izifree® contains lactose. If a patient has known intolerance to certain sugars, consultation with a physician is necessary before taking this medicinal product.
Use during pregnancy or breastfeeding.
Pregnancy. Data on the use of tiotropium in pregnant women are very limited. Preclinical studies did not reveal any direct or indirect harmful effects related to reproductive toxicity at clinically relevant doses. As a precautionary measure, use of Izifree® during pregnancy should be avoided.
Breastfeeding. It is unknown whether tiotropium bromide passes into human breast milk. Despite studies in rodents showing only minimal transfer of tiotropium bromide into breast milk, use of the drug during breastfeeding is not recommended.
Tiotropium bromide is a long-acting compound. The decision whether to continue or discontinue breastfeeding or to continue or discontinue treatment with Izifree® should be made after considering the benefits of breastfeeding for the child and the benefits of therapy for the woman.
Fertility. There are no available clinical data on the effect of tiotropium on fertility. Preclinical studies of tiotropium did not show any adverse effect on fertility.
Ability to affect reaction speed when driving or operating machinery.
Studies on the influence of Izifree® on the ability to drive a car or operate machinery have not been conducted. The occurrence of dizziness, headache, or blurred vision may affect the ability to drive or operate machinery.
Method of Administration and Dosage
The medicinal product is intended for inhalation use only.
The recommended dose of IsiFri® is one inhalation of the contents of one blister strip once daily using the Elpenhaler® inhalation device. Inhalation should be performed at the same time each day.
The recommended dose should not be exceeded.
Blister strips are intended for inhalation only and must not be taken orally. IsiFri® blister strips must not be swallowed.
The medication should be used only with the Elpenhaler® inhalation device. The Elpenhaler® device should be stored in its packaging to protect it from moisture and removed immediately before first use.
Special Populations
Elderly patients should use IsiFri® only at the dose recommended by the physician.
Patients with renal impairment should use IsiFri® according to the dose recommended by the physician. Information on the use of IsiFri® in patients with moderate to severe renal impairment (creatinine clearance ≤ 50 mL/min) is provided in the sections "Special Warnings and Precautions for Use" and "Pharmacokinetics".
Patients with hepatic impairment may use IsiFri® according to the dose recommended by the physician (see section "Pharmacokin游戏副本").
Method of Administration
To ensure proper use of the medication, patients must be instructed on how to use the inhaler.
INSTRUCTIONS FOR USING ELPENHALER®
Elpenhaler® is a device for administering powdered medication in measured doses.
Each dose is stored in a blister of a specially designed blister strip, which is divided into individual doses.
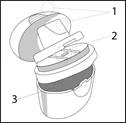
The Elpenhaler® device consists of three parts:
- Mouthpiece and its protective cap (1).
- Surface (2), where the blister strip is placed (support surface).
- Storage compartment (3), where the blister strip is kept.
The three parts are connected and can be opened separately.
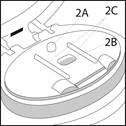
The support surface consists of:
- Attachment point (2A), to which the blister strip is secured.
- Cavity (2B), into which the blister strip is placed.
- Two strip guides (2C), which securely hold the blister strip in the correct position on the support surface.

The blister strip consists of:
- Two aluminum foils (4).
- Blister (5), containing the medication.
- Hole (6).
USING ELPENHALER®
A. Preparing the Device
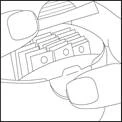
- Open the storage compartment by pressing as shown in the picture, remove a strip, and close the storage compartment again.
- Fully open the mouthpiece by gently pressing on the striped area.
- Unlock and pull back the mouthpiece to expose the support surface.
- Hold the blister strip with the shiny side up so that the blue line is visible, as indicated by the arrow in the picture. The marked surface of the strip should face downward.
- Place the hole of the strip onto the attachment point of the support surface. Apply gentle pressure to ensure the strip is securely fixed at the attachment point.

- The blister of the strip is placed into the cavity of the support surface, and the guides secure the strip in the correct position.
- Close the mouthpiece, horizontally pull the relief tab of the strip to detach it, and discard it.
- The dose is now ready for inhalation.
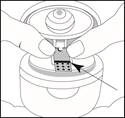
B. Inhalation of the Dose
Hold the device away from the mouth. Breathe out fully. Be careful not to exhale through the device’s mouthpiece. Bring the Elpenhaler® to the mouth and close lips tightly around the mouthpiece.

- Inhale slowly and deeply through the mouth (not through the nose) until the lungs are fully filled.
- Hold breath for approximately 5 seconds, or as long as comfortably possible, and simultaneously remove the device from the mouth.
- Exhale and resume normal breathing.

- Open the mouthpiece.
- It will be evident that the entire powder has been inhaled and that the blister of the strip is empty.
- Remove the empty strip, discard it, and proceed to step C.
C. Cleaning the Device
After each use, wipe the mouthpiece and support surface with a dry cloth or dry paper towel. Do not use water to clean the device.
Close the mouthpiece and its cap.
Children
There is no experience of appropriate use in pediatric patients (under 18 years of age).
Overdose
High doses of IsiFri® may cause anticholinergic symptoms.
However, systemic anticholinergic side effects were not observed in healthy volunteers after single doses of up to 340 mcg of tiotropium bromide.
No significant adverse reactions other than dry mouth were observed in healthy volunteers after 7 days of tiotropium bromide administration up to 170 mcg.
In multiple-dose studies in patients with COPD, administration of the maximum daily dose of 43 mcg of tiotropium bromide for 4 weeks did not cause significant adverse reactions.
Acute intoxication after oral administration of tiotropium capsules is unlikely due to low oral bioavailability.
Adverse Reactions
Many of the listed adverse effects can be attributed to the anticholinergic properties of IziFri®.
Adverse reactions were identified based on data from clinical trials and spontaneous reports during the post-marketing period. The clinical study database includes 9647 patients who received tiotropium in 28 placebo-controlled clinical trials with treatment duration ranging from 4 weeks to 4 years.
Frequency of adverse reactions according to MedDRA: very common (≥ 1/10); common (≥ 1/100, < 1/10); uncommon (≥ 1/1000, < 1/100); rare (≥ 1/10,000, < 1/1000); very rare (<1/10,000); not known (cannot be estimated from available data).
Metabolism and nutrition disorders: not known – dehydration.
Nervous system disorders: uncommon – dizziness, headache, taste disturbance; rare – insomnia.
Eye disorders: uncommon – blurred vision; rare – glaucoma, increased intraocular pressure.
Cardiac disorders: uncommon – atrial fibrillation; rare – supraventricular tachycardia, tachycardia, palpitations.
Respiratory, thoracic and mediastinal disorders: uncommon – cough, dysphonia, pharyngitis; rare – bronchospasm, epistaxis, laryngitis, sinusitis.
Gastrointestinal disorders: common – dry mouth; uncommon – constipation, gastroesophageal reflux disease, oral and pharyngeal candidiasis; rare – intestinal obstruction, including paralytic ileus; dysphagia, gingivitis, glossitis, stomatitis, nausea; not known – dental caries.
Immune system, skin and subcutaneous tissue disorders: uncommon – rash; rare – angioedema, hypersensitivity (including immediate-type allergic reactions), pruritus, urticaria; not known – dry skin, skin infections and ulceration, anaphylactic reactions.
Musculoskeletal and connective tissue disorders: not known – joint swelling.
Renal and urinary disorders: uncommon – urinary retention, dysuria; rare – urinary tract infection.
Description of selected adverse reactions
In controlled clinical studies, the most commonly observed anticholinergic adverse reaction was dry mouth, reported in approximately 4% of patients.
In 28 clinical trials, dry mouth led to discontinuation of the drug in 18 out of 9647 patients (0.2%).
Among serious adverse effects were glaucoma, constipation, intestinal obstruction (including paralytic ileus), and urinary retention.
Other special patient groups
The number of anticholinergic effects may increase with age.
Shelf life. 2 years.
Use within 60 days after first opening of the aluminum pouch when stored below 25 °C.
Do not use the medicinal product after the expiry date stated on the packaging.
Storage conditions.
The medicinal product does not require special storage conditions. Store in the original packaging to protect from moisture.
Keep out of reach of children.
Packaging.
10 mcg/dose, 1 dose in a blister; 30 blisters in an Elpenhaler® inhaler; 1 inhaler in a pouch; 1 pouch in a cardboard box.
Prescription category. Prescription only.
Manufacturer.
Elpen Pharmaceutical Co. Inc., Greece
Elpen Pharmaceutical Co., Inc., Greece
(manufacturing, primary and secondary packaging, quality control, batch release of the medicinal product).
Manufacturer's address.
Marathonos Avenue 95, Pikermi, 190 09, Greece
Marketing authorization holder. JSC "Farmak"
Address of the marketing authorization holder. Ukraine, 04080, Kyiv, Kyrylivska St., 63.