Glenspray active
Ukraine
Table of Contents
INSTRUCTIONS FOR MEDICAL USE OF THE MEDICINAL PRODUCT GLENSPRAY ACTIVE (GLENSPRAY ACTIVE)
Composition:
Active substances: mometasone furoate and azelastine hydrochloride;
1 dose contains 50 mcg of mometasone furoate and 140 mcg of azelastine hydrochloride;
Excipients: microcrystalline cellulose and sodium carboxymethylcellulose; carbomer; anhydrous glucose; polysorbate 80; benzalkonium chloride; disodium edetate; neotame; citric acid, monohydrate; sodium citrate; water for injections.
Pharmaceutical form. Nasal spray, metered, suspension.
Main physicochemical characteristics: white or almost white suspension.
Pharmacotherapeutic group.
Anti-edematous and other drugs for local use in nasal cavity disorders. Corticosteroids. ATC code R01AD.
Pharmacological properties.
Pharmacodynamics. A combined anti-edematous agent for topical use containing mometasone furoate and azelastine hydrochloride.
Azelastine hydrochloride is a phthalazinone derivative. It exerts a prolonged antiallergic effect. It has pronounced selective properties as a histamine H1-receptor antagonist. Azelastine inhibits the synthesis or release of chemical mediators involved in the development of early and late stages of allergic reactions, such as leukotrienes, histamine, PAF inhibitors, and serotonin. The main metabolite of azelastine is desmethylazelastine, which is also a histamine H1-receptor antagonist.
Mometasone furoate is a synthetic corticosteroid for topical use that exerts a pronounced anti-inflammatory effect. The exact mechanism of action of corticosteroids in allergic rhinitis is not yet known. Corticosteroids demonstrate a broad range of effects on various cells, including mast cells, eosinophils, neutrophils, macrophages, lymphocytes, as well as on inflammatory mediators (histamine, eicosanoids, leukotrienes, and cytokines). The mechanism of the anti-inflammatory and antiallergic action of mometasone furoate is mainly related to its ability to inhibit the release of mediators of allergic reactions.
Studies have shown that mometasone furoate administered as a nasal spray at a dose of 50 mcg per dose, when used locally, reduces the levels of certain mediators of the early and late phases of the allergic reaction, decreases (compared to placebo) the levels of histamine and eosinophilic cationic protein, and reduces (compared to baseline values) the number of eosinophils, neutrophils, and epithelial cell adhesion proteins.
Pharmacokinetics. A separate pharmacokinetic study of the nasal spray containing azelastine hydrochloride and mometasone furoate (140 mcg/50 mcg) has not been conducted.
Absorption
After intranasal administration of 2 sprays in each nostril of azelastine nasal spray (total dose 548 mcg), the mean peak plasma concentration (Cmax) of azelastine is 200 pg/mL, the mean systemic exposure (AUC) is 5122 pg × h/mL, and the mean time to reach Cmax (Tmax) is 3 hours. Systemic bioavailability of azelastine hydrochloride after intranasal administration is approximately 40%.
The suspension of mometasone furoate when administered as a nasal spray has very low bioavailability (<1%), as demonstrated by a sensitive quantitative analysis with a lower limit of quantification (LOQ) of 0.25 pg/mL.
Distribution
Following intravenous and oral administration, the volume of distribution at equilibrium for azelastine is 14.5 L/kg. In vitro, plasma protein binding of azelastine and its active metabolite desmethylazelastine is 88% and 97%, respectively.
In vitro plasma protein binding of mometasone furoate ranges from 98% to 99% over a concentration range of 5 to 500 ng/mL.
Metabolism
Azelastine is metabolized via the cytochrome P450 enzyme system through oxidation to its main active metabolite, desmethylazelastine. The specific P450 isoenzymes responsible for the biotransformation of azelastine have not been identified. After a single intranasal dose of azelastine nasal spray (total dose 548 mcg), the mean Cmax of desmethylazelastine is 23 pg/mL, AUC is 2131 pg × h/mL, and mean Tmax is 24 hours. After reaching steady-state concentrations with intranasal administration, plasma concentrations of desmethylazelastine range between 20–50% of azelastine concentrations.
Studies have shown that the portion of ingested and absorbed mometasone furoate undergoes active metabolism. No major metabolites were detected in plasma. After in vitro incubation, one of the minor metabolites formed was 6β-hydroxymometasone furoate. In human liver microsomes, metabolite formation is mediated by cytochrome P450 3A4 (CYP3A4).
Elimination
After intranasal administration of azelastine nasal spray, the elimination half-life of azelastine is 22 hours and that of desmethylazelastine is 52 hours. Approximately 75% of an orally administered radiolabeled dose of azelastine hydrochloride is excreted in feces, with less than 10% excreted as unchanged azelastine.
After intravenous administration, the elimination half-life of mometasone furoate is 5.8 hours. It is excreted from the body primarily as metabolites via bile and to a limited extent via urine.
Pharmacokinetics in specific patient populations.
Hepatic impairment
After oral administration of azelastine, hepatic impairment did not affect pharmacokinetic parameters.
Administration of a single inhaled dose of 400 mcg mometasone furoate to patients with mild, moderate, and severe hepatic impairment resulted in detectable peak plasma concentrations of mometasone furoate (50 to 105 pg/mL) in only 1 or 2 patients in each group. Observed peak plasma concentrations increased with the severity of hepatic impairment.
Renal impairment
Studies of single oral doses of azelastine administered to patients with renal impairment (creatinine clearance <50 mL/min) showed increases in Cmax and AUC by 70–75% compared to healthy volunteers. The time to maximum concentration was unchanged.
The effect of renal impairment on the pharmacokinetics of mometasone furoate has not been studied.
Age
Age did not affect the pharmacokinetic parameters of azelastine following oral administration. The pharmacokinetics of mometasone furoate has not been studied in the pediatric population.
Gender
Following oral administration of azelastine, gender did not affect its pharmacokinetic parameters. The effect of gender on the pharmacokinetics of mometasone furoate has not been studied.
Clinical characteristics.
Indications.
Seasonal allergic rhinitis.
Perennial allergic rhinitis.
Contraindications.
Hypersensitivity to azelastine hydrochloride, mometasone furoate, or to any of the excipients of the medicinal product.
Untreated local infection of the nasal mucosa.
Nasal trauma or recent nasal surgery.
Interaction with other medicinal products and other forms of interaction.
Specific studies on drug interactions of the fixed-dose combination of azelastine hydrochloride and mometasone furoate as a nasal spray have not been conducted. The data below refer to the individual components of the medicinal product. Since mometasone and azelastine act on different types of receptors, drug interactions with this combination are not expected.
Azelastine hydrochloride
Central nervous system depressants
Concomitant use of azelastine with alcohol or other central nervous system depressants may result in reduced attention and impaired central nervous system functions.
Erythromycin and ketoconazole
ECG assessment of patients who received oral azelastine hydrochloride concomitantly with erythromycin or ketoconazole showed no clinically significant effect on the QT interval (or QTc interval). Oral administration of erythromycin 500 mg three times daily for 7 days did not affect the pharmacokinetics of azelastine or the QTc interval. Ketoconazole administered at a dose of 200 mg twice daily for 7 days interfered with the measurement of plasma concentrations of azelastine by analytical high-performance liquid chromatography (HPLC); however, no effect on the QTc interval was observed.
Cimetidine
Cimetidine 400 mg twice daily, when administered concomitantly with oral azelastine hydrochloride 4 mg twice daily, increases the mean Cmax and AUC of the latter by approximately 65%.
Mometasone furoate
Cytochrome P450 3A4 inhibitors
Ketoconazole
Mometasone furoate is primarily metabolized in the liver. In vitro studies have confirmed the primary role of cytochrome CYP3A4 in the metabolism of this compound. Concomitant administration with ketoconazole, a potent CYP3A4 inhibitor, may increase plasma concentrations of mometasone furoate.
Ritonavir
Ritonavir, as a protease inhibitor, may inhibit the metabolism of mometasone furoate when administered concomitantly, leading to increased systemic exposure and an increased risk of adverse effects.
Loratadine
Clinical drug interaction studies have been conducted with loratadine. No interaction was observed.
Special precautions for use.
Azelastine hydrochloride
Somnolence has been reported in some patients during clinical trials with azelastine hydrochloride administered as a nasal spray. Patients should avoid activities requiring increased attention and rapid reaction times while being treated with this medication.
Concomitant use of azelastine nasal spray with alcohol or other central nervous system depressants should be avoided due to the potential for additive CNS depression.
Mometasone furoate
Local effects on the nose
Nasal bleeding
Nasal bleeding was observed more frequently in patients with allergic rhinitis receiving mometasone furoate nasal spray compared to those receiving placebo in clinical studies.
Fungal infection
Localized fungal infections of the nose and throat (Candida albicans) have been observed in isolated cases after administration of mometasone furoate nasal spray at a dose of 50 mcg/dose. If a fungal infection develops, treatment with the drug should be discontinued and appropriate antifungal therapy initiated if necessary.
Nasal septum perforation
Isolated cases of nasal septum perforation have been reported in patients following the use of intranasal corticosteroids, including mometasone furoate. As with any prolonged local treatment of the nasal cavity, patients using mometasone furoate nasal spray for several months or longer should undergo periodic examinations to detect possible changes in the nasal mucosa.
Impaired wound healing
Due to the inhibitory effect of corticosteroids on wound healing, patients who have recently experienced nasal septum ulceration, nasal surgery, or nasal trauma should not use intranasal corticosteroids until full recovery has occurred.
Visual disturbances
Visual disturbances may occur with systemic and topical corticosteroids (including intranasal, inhaled, and intraocular administration). If symptoms such as blurred vision or other visual disturbances occur, patients should undergo ophthalmologic evaluation to assess possible causes, including cataract, glaucoma, or rare conditions such as central serous chorioretinopathy, which have been reported after systemic and topical corticosteroid use.
Hypersensitivity reactions
Hypersensitivity reactions, including wheezing, may occur after intranasal administration of mometasone furoate. In such cases, treatment with the drug should be discontinued.
Immunosuppression
Patients receiving immunosuppressive medications are more susceptible to infections than healthy individuals. For example, varicella and measles may have a more severe course in immunocompromised children and adults receiving corticosteroids. Such patients require special attention and may need antiviral therapy or vaccination. The influence of corticosteroid dose, route, and duration of administration on the risk of generalized infection is not fully understood.
Mometasone furoate nasal spray should be used with caution or avoided entirely in patients with active or latent respiratory tract tuberculosis, as well as in those with untreated fungal, bacterial, systemic viral infections, or herpes simplex infection involving the eyes.
Effects on the hypothalamic-pituitary-adrenal (HPA) axis
Hyperadrenocorticism and adrenal suppression
Systemic effects such as hyperadrenocorticism and adrenal suppression may occur with prolonged use of intranasal corticosteroids, particularly at high doses. It is important to reduce the dose of intranasal corticosteroids to the lowest effective dose once therapeutic effect is achieved, in order to minimize the risk of systemic adverse effects.
If signs of systemic adverse effects appear, treatment with mometasone furoate nasal spray should be gradually discontinued.
Effects on growth in children
Corticosteroids, including mometasone furoate, may cause growth suppression in children. Regular monitoring of growth is recommended in children receiving long-term intranasal corticosteroid therapy.
To minimize systemic effects of intranasal corticosteroids, including mometasone furoate, the dose should be titrated to the lowest effective dose for each patient.
Glen Spray Active contains benzalkonium chloride, which may cause irritation of the nasal mucosa and bronchospasm.
It should be remembered that corticosteroids have a particularly potent diabetogenic effect and may lead to increased hepatic gluconeogenesis, reduced glucose uptake by peripheral tissues, and hyperglycemia.
Use in elderly patients
Clinical safety data on the use of the medicinal product in elderly patients are lacking.
Use during pregnancy or breastfeeding
No specific studies on the use of the drug during pregnancy or breastfeeding have been conducted.
Use during pregnancy
Azastine hydrochloride. Adequate and well-controlled clinical trials in pregnant women have not been conducted. In animal studies, azelastine hydrochloride caused embryotoxicity.
Mometasone furoate. Adequate and well-controlled clinical trials in pregnant women have not been conducted.
It should be noted that due to the natural increase in endogenous corticosteroid production during pregnancy, most women require lower doses of exogenous corticosteroids, and many do not require corticosteroid therapy during pregnancy.
Mometasone is minimally systemically absorbed after nasal administration, and use of the drug by the mother is not expected to affect the fetus. Observational data on the use of mometasone furoate in pregnant women are insufficient to assess the risk of major congenital malformations, miscarriage, or other adverse maternal or fetal outcomes. In reproductive studies in pregnant mice, rats, and rabbits, mometasone furoate (administered subcutaneously, topically, or orally) caused increased fetal malformations and reduced fetal survival and growth at doses ⅓ to 8 times the maximum recommended human daily dose (on a mcg/m² or AUC basis). However, experience with oral corticosteroids indicates that rodents are more susceptible to teratogenic effects of corticosteroids than humans.
The baseline risk of major congenital malformations and miscarriage in the indicated population is unknown. All pregnancies carry a background risk of birth defects, loss, or other adverse outcomes. In the general US population, the estimated risk of major congenital malformations and miscarriage in clinically recognized pregnancies is 2–4% and 15–20%, respectively.
In an embryo-fetal development study in pregnant mice dosed during the period of organogenesis, mometasone furoate caused cleft palate at doses lower than the maximum recommended intranasal daily dose (MRID) (on a mcg/m² basis, subcutaneous maternal doses of 60 mcg/kg and higher) and reduced fetal survival at doses approximately less than twice the MRID (on a mcg/m² basis, subcutaneous maternal dose of 180 mcg/kg). No toxicity was observed at a dose lower than the MRID (on a mcg/m² basis, topical maternal doses of 20 mcg/kg and higher).
Use during breastfeeding
Azastine hydrochloride. It is unknown whether azelastine hydrochloride is excreted in human breast milk.
Mometasone furoate. It is unknown whether mometasone furoate is excreted in human breast milk.
Systemic absorption of mometasone in the mother after nasal administration is minimal, and effects of mometasone on the infant via breast milk are not expected. However, the benefits of breastfeeding for the infant's development and health, the mother's clinical need for mometasone, and any potential adverse effects of mometasone furoate or the mother's underlying condition on the infant should be considered.
Ability to affect reaction speed when driving or operating machinery
No specific studies on the effect of the drug on the ability to drive or operate machinery have been conducted.
Since somnolence has been reported in some patients receiving azelastine hydrochloride nasal spray in clinical trials, patients should avoid activities requiring high concentration and rapid reaction times during treatment with this medication.
Method of Administration and Dosage
The product is intended for intranasal use only.
Adults and children aged 12 years and older. The recommended dose is 1 spray into each nostril twice daily.
Patients with renal impairment. Dose adjustment is not required in patients with mild renal impairment (creatinine clearance > 79 mL/min). The drug should be used with caution and under strict medical supervision in patients with moderate to severe renal impairment (creatinine clearance < 79 mL/min to > 10 mL/min).
Patients with hepatic impairment. Dose adjustment is not required.
Elderly patients. No differences in safety and/or efficacy have been observed in elderly patients compared to younger adults.
Administration of Nasal Spray
Before each use, the bottle should be gently shaken for 5 seconds. Then remove the protective cap. Before the first use, prime the pump by pressing down 6 times consecutively. If the nasal spray has not been used for more than 7 days, re-prime the pump by pressing 6 times consecutively before use.
Before each administration, clear the nasal passages of mucus thoroughly. After nasal cleansing, administer the suspension into each nostril while keeping the head slightly tilted forward. After use, wipe the spray nozzle and replace the protective cap.
If the spray pump becomes clogged, clean it as described below.
Do not attempt to clean the spray nozzle with a needle or any other sharp object — this may damage the device and result in incorrect dosing.
To clean the spray nozzle, remove the cap (Figure 1).

Figure 1
Carefully pull the white spray nozzle upward to remove it.
Soak the spray nozzle and dust cap in warm water for several minutes, then thoroughly rinse the spray nozzle and dust cap with warm water, and finally rinse with clean running water (Figure 2).
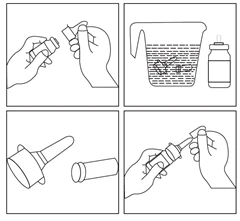
Figure 2
After the spray nozzle has dried, reattach it, ensuring that the pump stem is properly reinserted into the central opening of the nozzle (Figure 3).

Figure 3
Prepare the spray pump for use by pressing the sides of the upper part of the nozzle with the index and middle fingers, while holding the base of the bottle with the thumb. Press and release the spray pump 2 times, or continue pressing until a fine mist appears. (Repeat the rinsing procedure described above if no mist appears.) Do not spray into the eyes. The spray pump is now ready for use.
The spray pump may remain unused for up to 1 week without requiring re-priming. If the spray pump has not been used for more than 1 week, prepare it for use by pressing the nozzle 2 times or until a fine mist appears (Figure 4).

Figure 4
After use, replace the protective cap on the spray nozzle (Figure 5).

Figure 5
Children.
There is insufficient clinical experience regarding the use of this medication in children under 12 years of age; therefore, it should not be used in this age group.
The safety and efficacy of mometasone furoate for the prevention of nasal symptoms of seasonal allergic rhinitis have been established in pediatric patients aged 12 years and older. The use of mometasone furoate for this indication has been confirmed in controlled clinical trials involving both adults and children aged 12 years and older.
Effect on Growth
Controlled clinical studies have shown that intranasal corticosteroids may cause growth suppression in children. This effect has been observed in the absence of laboratory evidence of hypothalamic-pituitary-adrenal (HPA) axis suppression, indicating that growth velocity is a more sensitive indicator of systemic corticosteroid effects in pediatric patients than standard HPA axis function tests. The long-term consequences of this growth suppression associated with intranasal corticosteroids, including the impact on final adult height, are unknown. The potential for catch-up growth after discontinuation of intranasal corticosteroid therapy has not been adequately studied. Growth in children receiving intranasal corticosteroids, including mometasone furoate, should be monitored regularly (e.g., using a stadiometer). The potential impact of long-term therapy on growth should be weighed against the clinical benefits achieved and the availability of safe and effective non-corticosteroid treatment alternatives. To minimize systemic effects of intranasal corticosteroids, including mometasone furoate, the lowest effective dose should be used for each patient.
Overdose.
There have been no reports of overdose with GLENSPREY Active.
In cases of acute overdose, central nervous system disturbances (such as drowsiness, dizziness) may occur. Single oral doses of azelastine hydrochloride up to 16 mg in clinical trials did not increase the incidence of serious adverse effects. Treatment is symptomatic. No antidote is known.
There are no reports of acute or chronic overdose with mometasone furoate nasal spray. Single intranasal doses up to 4 mg and inhaled oral doses up to 8 mg have been administered to volunteers without any adverse effects.
Chronic overdose with any corticosteroid may lead to symptoms of hypercorticism.
Side effects.
During the clinical study, adverse effects associated with the use of the nasal spray containing azelastine hydrochloride and mometasone furoate were reported in 11 out of 282 patients who participated in the study. A total of 18 treatment-related adverse reactions were recorded. The most common adverse reactions were headache and dysgeusia. Other adverse reactions included somnolence, lethargy, nausea, dyspepsia, and sneezing. Most adverse effects were mild in severity, and no serious adverse reactions were reported during the study.
Below are the adverse reactions observed with the use of individual components of the medicinal product.
Azelastine hydrochloride nasal spray
Common (1–10%): a specific bitter taste may occur after administration of the spray (most often due to incorrect administration technique, particularly when the head is tilted too far backward during spraying), which in some cases may lead to nausea.
Uncommon (0.1–1%): temporary irritation of the inflamed nasal mucosa may occur, accompanied by symptoms such as burning, itching, sneezing, and epistaxis.
In very rare cases (<0.01%), hypersensitivity reactions (rash, pruritus, urticaria) have been reported.
Post-marketing experience
Adverse reactions identified during post-marketing use of azelastine nasal spray: abdominal pain, nasal burning, nausea, sweet taste, throat irritation, anaphylactoid reactions, application site irritation, atrial fibrillation, visual disturbances (blurred vision, cataract, glaucoma, central serous chorioretinopathy (see section "Special precautions")), chest pain, confusion, dizziness, dyspnea, facial swelling, hypertension, muscle twitching, nervousness, tachycardia, paresthesia, parosmia, paroxysmal sneezing, pruritus, rash, disturbances or loss of smell and/or taste, tachycardia, immunological tolerance, urinary retention, xerophthalmia. Since these reactions are reported from a population of unspecified size, it is not always possible to reliably estimate their frequency or establish a causal relationship to the use of the medicinal product.
Mometasone furoate nasal spray
Respiratory, thoracic and mediastinal disorders: epistaxis, pharyngitis, nasal burning or irritation, nasal ulcers – common (1–10%).
General disorders and administration site conditions: headache – common (1–10%).
Epistaxis was generally mild in intensity and did not require medical intervention.
In children, the most commonly observed adverse reactions were epistaxis, headache, nasal mucosal irritation, and sneezing.
Systemic adverse effects during treatment with intranasal corticosteroids may occur with prolonged use of high doses.
Post-marketing experience
Adverse reactions identified during post-marketing use of mometasone furoate nasal spray: nasal burning and irritation, anaphylaxis and angioneurotic edema, taste and smell disturbances, and nasal septum perforation.
Clinically significant adverse reactions described in other sections:
Epistaxis, ulcers, Candida albicans infection, impaired wound healing (see section "Special precautions")
Glaucoma and cataract (see section "Special precautions")
Immunosuppression and risk of infections (see section "Special precautions")
Hypercorticism and adrenal suppression, including growth retardation (see sections "Special precautions" and "Children").
Clinical trial experience
Because clinical trials are conducted under widely varying conditions, the adverse reaction rates observed in clinical trials of a medicinal product cannot be directly compared with those of another medicinal product, and may not reflect the rates observed in practice.
Allergic rhinitis: adults and children aged 12 years and older
In controlled U.S. and international clinical trials, a total of 3210 adults and children aged 12 years and older with allergic rhinitis received mometasone furoate nasal at doses ranging from 50 to 800 mcg/day. The majority of patients (n = 2103) received 200 mcg/day. A total of 350 adults and children aged 12 years and older were treated for one year or longer. Adverse reactions did not differ significantly by age, gender, or race. Four percent or fewer patients in clinical trials discontinued treatment due to adverse effects, and the discontinuation rate was similar between the medicinal product and active comparators.
All adverse reactions (regardless of relationship to treatment) reported in at least 5% of adults and children aged 12 years and older receiving mometasone furoate nasal at a dose of 200 mcg/day occurred more frequently with mometasone furoate than with placebo.
Adults and children aged 12 years and older: adverse reactions from controlled clinical studies in seasonal allergic rhinitis and perennial allergic rhinitis (percentage of patients reporting the event).
Other adverse reactions occurring in ≥2% to <5% of adults and children aged 12 years and older receiving mometasone furoate nasal 200 mcg/day (regardless of relationship to treatment) and more frequently than in the placebo group: arthralgia, asthma, bronchitis, chest pain, conjunctivitis, diarrhea, dyspepsia, ear pain, influenza-like symptoms, myalgia, nausea, and rhinitis.
Use of the nasal spray containing azelastine hydrochloride and mometasone furoate in patients may lead to increased levels of ALT and AST.
Use of the medicinal product Glenspray Active may lead to development of renal and urinary system disorders (hematuria).
Corticosteroids stimulate the secretion of acid and pepsin, which may lead to the development of gastritis and hyperchlorhydria.
Shelf life.
2 years.
Storage conditions.
Store in a light-protected place at a temperature not exceeding 25°C. Do not freeze. Keep out of reach of children.
Packaging.
75 or 150 doses in a polyethylene bottle. One bottle with a metered pump-sprayer, closed with a cap, in a cardboard box.
Prescription status.
Prescription only.
Manufacturer.
Glenmark Pharmaceuticals Ltd. / Glenmark Pharmaceuticals Ltd.
Manufacturer's address and place of business.
Unit III, Village Kishanpura, Baddi-Nalagarh Road, Tehsil Baddi, Distt. Solan (H.P.) 173 205, India.