Genotropin®
Ukraine
Table of Contents
INSTRUCTIONS FOR MEDICAL USE OF THE MEDICINAL PRODUCT GENOTROPIN® (GENOTROPIN®)
Composition:
Active substance: somatropin;
front chamber: somatropin 6.1 mg or 13.8 mg;
1 ml of reconstituted solution contains somatropin 16 IU (5.3 mg) or 36 IU (12 mg);
Excipients: glycine, mannitol (E 421), sodium dihydrogen phosphate anhydrous, sodium hydrogen phosphate (dodecahydrate);
rear chamber (solvent): m-cresol, mannitol (E 421), water for injections.
Pharmaceutical form. Lyophilized powder and solvent for solution for injection.
Main physicochemical properties: lyophilized homogeneous white substance. The solvent should be practically free from mechanical inclusions.
Pharmacotherapeutic group. Hormones of the anterior pituitary gland and their analogues. Somatropin and somatropin agonists. Somatropin. ATC code H01AC01.
Pharmacological Properties
Pharmacodynamics
Somatropin is a potent metabolic hormone that plays an important role in lipid, carbohydrate, and protein metabolism. Somatropin is produced in Escherichia coli cells using recombinant DNA technology. In children with deficiency of endogenous growth hormone, somatropin accelerates skeletal linear growth and growth velocity. In both adults and children, somatropin supports normal body composition by increasing nitrogen retention, stimulating skeletal muscle growth, and mobilizing body fat. Visceral adipose tissue is particularly sensitive to somatropin. In addition to stimulating lipolysis, somatropin reduces the uptake of triglycerides into fat stores. Serum concentrations of IGF-1 (insulin-like growth factor 1) and IGFBP-3 (insulin-like growth factor binding protein 3) increase in response to somatropin. The following effects have also been demonstrated:
- Lipid metabolism. Somatropin stimulates hepatic low-density lipoprotein (LDL) receptors and affects the serum lipid and lipoprotein profile. Overall, somatropin administration in patients with growth hormone deficiency leads to a reduction in LDL and apolipoprotein B concentrations. A decrease in total cholesterol levels may also occur.
- Carbohydrate metabolism. Somatropin increases insulin levels, but fasting glucose levels usually remain unchanged. In children with hypopituitarism, fasting hypoglycemia may occur. Somatropin reverses this condition.
- Water and electrolyte metabolism. Growth hormone deficiency is associated with reduced plasma and interstitial fluid volumes. Both parameters increase rapidly after treatment with somatropin. Somatropin promotes retention of sodium, potassium, and phosphorus in the body.
- Bone metabolism. Somatropin stimulates skeletal bone turnover. In patients with growth hormone deficiency and osteoporosis, long-term treatment with somatropin leads to increased bone mineral content and bone mineral density at weight-bearing sites.
- Physical capacity. Long-term treatment with somatropin increases muscle strength and physical endurance. Somatropin also increases cardiac output, although the mechanism of this effect has not yet been fully elucidated. A possible contributing factor may be a reduction in peripheral vascular resistance.
In clinical studies involving short-stature children born small for gestational age, doses ranging from 0.033 to 0.067 mg/kg body weight per day were administered until final height was reached. In 56 patients who were continuously treated and who reached (or nearly reached) final height, the mean change in height from baseline expressed as standard deviation score (SDS) was +1.90 SDS for the 0.033 mg/kg/day dose and +2.19 SDS for the 0.067 mg/kg/day dose. Published data on untreated children born small for gestational age who failed to achieve catch-up growth suggest a late growth gain of approximately 0.5 SDS.
Pharmacokinetics
Absorption. The bioavailability of somatropin administered subcutaneously is approximately 80% in both healthy volunteers and patients with growth hormone deficiency. A subcutaneous dose of 0.035 mg/kg of somatropin results in plasma Cmax and tmax values within the ranges of 13–35 ng/mL and 3–6 hours, respectively.
Elimination. The mean terminal elimination half-life after intravenous administration of somatropin in adults with growth hormone deficiency is approximately 0.4 hours. However, after subcutaneous administration, the elimination half-life may extend to 2–3 hours. This observed difference is likely due to slow absorption from the injection site following subcutaneous administration.
Subpopulations. The absolute bioavailability of somatropin after subcutaneous administration is similar in males and females.
Information on the pharmacokinetics of somatropin in elderly patients and children, in patients of different racial groups, and in patients with renal or hepatic impairment or heart failure is lacking or incomplete.
Non-clinical Safety Data
In studies of general toxicity, local tolerance, and reproductive toxicity, no clinically relevant adverse effects were observed.
In vitro and in vivo genotoxicity studies assessing gene mutations and induction of chromosomal aberrations yielded negative results.
In one in vitro study using lymphocytes obtained from patients after long-term somatropin treatment followed by additional exposure to the radiomimetic agent bleomycin, increased chromosomal fragility was observed. The clinical significance of this finding is unclear.
In another study, no chromosomal abnormalities were detected in lymphocytes obtained from patients after long-term somatropin treatment.
Clinical characteristics.
Indications.
Children.
Growth failure due to inadequate growth hormone secretion (growth hormone deficiency).
Growth failure associated with Turner syndrome or chronic renal insufficiency.
Growth failure (current height standard deviation score less than –2.5 and genetically predicted height standard deviation score less than –1) in short children born small for gestational age, with standard deviation score of birth weight and/or length less than –2, who have not shown catch-up growth (height velocity standard deviation score less than 0 during the past year) by age 4 years or older.
Prader-Willi syndrome, to improve growth and body composition. Diagnosis of Prader-Willi syndrome should be confirmed by appropriate genetic testing.
Genotropin® (somatropin [rDNA origin] for injection) is indicated for the treatment of idiopathic short stature, i.e., short stature without growth hormone deficiency, defined by a standard deviation score < –2.25 (growth rates unlikely to achieve normal adult height range), in children with open epiphyseal growth plates, in whom diagnostic evaluation has excluded other causes of short stature requiring observation or treatment by alternative means.
Adults.
Replacement therapy in adults with severe growth hormone deficiency.
Adult-onset growth hormone deficiency. Patients with severe growth hormone deficiency associated with multiple pituitary hormone deficiencies due to known hypothalamic or pituitary pathology, and patients with deficiency of at least one pituitary hormone other than prolactin. These patients should undergo an appropriate dynamic test to confirm the presence or absence of growth hormone deficiency.
Childhood-onset growth hormone deficiency. Patients who developed growth hormone deficiency during childhood due to congenital, genetic, acquired, or unknown causes. Patients with childhood-onset growth hormone deficiency should undergo repeat testing of growth hormone secretion capacity after completion of linear growth. In patients with a high likelihood of persistent growth hormone deficiency (e.g., due to congenital causes or secondary to hypothalamic-pituitary disease or stroke), an insulin-like growth factor-1 (IGF-1) standard deviation score less than –2, measured without growth hormone therapy for at least 4 weeks, may be considered sufficient evidence for diagnosing growth hormone deficiency.
For all other patients, IGF-1 analysis and one growth hormone stimulation test are required.
Contraindications.
Hypersensitivity to the active substance or to any of the excipients of the medicinal product.
Somatropin is contraindicated in the presence of any signs of active tumor. Intracranial tumors must be inactive, and anti-tumor therapy must be completed prior to initiating growth hormone therapy. Treatment should be discontinued if any signs of tumor growth occur.
Genotropin® should not be used to stimulate growth in children with closed epiphyseal growth plates.
Genotropin® treatment is contraindicated in patients who are in acute critical conditions following complications of open-heart surgery, abdominal surgery, multiple trauma, acute respiratory failure, or similar conditions (see section "Special precautions" for information on patients receiving replacement therapy).
Interaction with other medicinal products and other types of interactions.
Concomitant use with glucocorticoids suppresses the growth-promoting effect of somatropin products. Patients with adrenocorticotropic hormone deficiency should receive carefully adjusted glucocorticoid replacement therapy to avoid any growth-suppressing effects.
Therefore, growth in patients receiving glucocorticoid therapy should be closely monitored to assess the potential impact of glucocorticoid use on growth.
Growth hormone reduces the conversion of cortisone to cortisol and may unmask previously undiagnosed central adrenal insufficiency or render low-dose glucocorticoid replacement therapy ineffective (see section "Special precautions").
Data from drug interaction studies conducted in adult patients with growth hormone deficiency indicate that somatropin may increase the clearance of compounds metabolized by cytochrome P450 isoenzymes. Clearance of substances metabolized by cytochrome P450 3A4 (such as sex steroid hormones, corticosteroids, anticonvulsants, and cyclosporine) may be significantly increased, leading to reduced plasma concentrations of these agents. The clinical significance of this is unknown.
For additional information regarding diabetes mellitus and thyroid dysfunction, see section "Special precautions."
Women receiving oral estrogen replacement therapy may require higher doses of growth hormone to achieve treatment goals (see section "Special precautions").
Special precautions for use.
Diagnosis, initiation of therapy with Genotropin® and ongoing monitoring should be performed by qualified physicians experienced in the diagnosis and treatment of patients according to the approved indications.
Myositis is a very rare adverse effect that may be caused by the preservative m-cresol contained in the formulation. In case of myalgia or increased pain at the injection site, myositis should be suspected. If myositis is confirmed, a formulation of Genotropin® that does not contain m-cresol should be used.
The maximum recommended daily dose should not be exceeded (see section "Method of administration and dosage").
Insulin sensitivity.
Somatropin may reduce insulin sensitivity. In patients with diabetes mellitus, insulin dosage adjustments may be required after initiation of somatropin therapy. Patients with diabetes mellitus, glucose intolerance, or additional risk factors for developing diabetes should be closely monitored during somatropin therapy.
Thyroid function.
Growth hormone accelerates peripheral conversion of T4 to T3, which may lead to decreased serum T4 concentration and increased serum T3 concentration. While peripheral thyroid hormone levels remain within normal range in most healthy individuals, hypothyroidism may theoretically develop in patients with subclinical hypothyroidism. Therefore, thyroid function should be monitored in all patients. In patients with hypopituitarism receiving standard replacement therapy, potential effects of growth hormone therapy on thyroid function should be carefully monitored.
Adrenal insufficiency.
Initiation of somatropin treatment may lead to inhibition of 11βHSD-1 and decreased serum cortisol concentration. Patients receiving somatropin may develop previously undiagnosed central (secondary) adrenal insufficiency and may require glucocorticoid replacement therapy. Additionally, patients who are already receiving glucocorticoid replacement therapy due to previously diagnosed adrenal insufficiency may require increased maintenance or stress doses after initiation of somatropin treatment (see section "Interaction with other medicinal products and other forms of interaction").
Concomitant use with oral estrogen therapy.
If a woman receiving somatropin starts oral estrogen therapy, an increase in somatropin dose may be necessary to maintain serum IGF-1 levels within the age-appropriate normal range. Conversely, if a woman receiving somatropin discontinues oral estrogen therapy, a reduction in somatropin dose may be required to avoid excess growth hormone and/or adverse effects (see section "Interaction with other medicinal products and other forms of interaction").
In cases of secondary growth hormone deficiency due to treatment of malignancies, patients should be monitored for signs of recurrence of malignant disease. An increased risk of secondary neoplasms has been reported in patients who received somatropin therapy after a prior malignancy, particularly in individuals who had childhood cancer.
The most common secondary neoplasms in patients who received cranial irradiation for a primary tumor were intracranial tumors, particularly meningiomas.
Patients with endocrine disorders, including growth hormone deficiency, may be at increased risk of developing slipped capital femoral epiphysis compared to the general population. Children who develop a limp during somatropin therapy should undergo clinical evaluation.
Benign intracranial hypertension.
In cases of severe or frequent headache, visual disturbances, nausea and/or vomiting, fundoscopy should be performed to detect papilledema. If papilledema is confirmed, benign intracranial hypertension should be considered, and growth hormone therapy should be discontinued if necessary. There is insufficient information to provide recommendations on resuming growth hormone therapy after resolution of intracranial hypertension. After resumption of therapy, careful monitoring for symptoms of intracranial hypertension is required.
Leukemia.
Cases of leukemia have been reported in a small number of patients with growth hormone deficiency, some of whom were receiving somatropin therapy. However, there is no evidence of increased incidence of leukemia in patients receiving growth hormone who do not have predisposition to this disease.
Antibodies.
As with all somatropin products, a small proportion of patients may develop antibodies to Genotropin®. Approximately 1% of patients develop antibodies after administration of Genotropin®. These antibodies are characterized by low binding affinity and do not affect growth velocity. In cases of inadequate response to treatment (unexplained by other causes), testing for anti-somatropin antibodies should be performed.
Elderly patients.
Experience with use in patients aged 80 years and older is limited. Elderly patients may be more sensitive to the effects of Genotropin® and therefore more susceptible to adverse reactions.
Acute critical illness.
The efficacy of Genotropin® during recovery was evaluated in two placebo-controlled studies involving 522 critically ill patients following complications of open-heart surgery, abdominal surgery, multiple trauma, or acute respiratory failure. Mortality was higher in patients receiving 5.3 or 8 mg of Genotropin® per day compared to placebo: 42% versus 19%. Based on this information, critically ill patients should not be treated with Genotropin®. Due to lack of safety data on growth hormone replacement therapy in patients with acute critical illness, the potential benefits and risks of continuing treatment should be carefully weighed.
For all patients who develop another or similar acute critical illness, the potential benefit of treatment with Genotropin® and the associated potential risks should be carefully considered.
Pancreatitis.
Although pancreatitis is rare, its development should be considered in any patient receiving somatropin therapy, especially in children presenting with abdominal pain.
Prader-Willi syndrome.
Treatment of patients with Prader-Willi syndrome should always be combined with a low-calorie diet.
Fatal outcomes have been reported in children with Prader-Willi syndrome receiving growth hormone therapy who had one or more risk factors: severe obesity (patients with body mass index exceeding 200% of normal), history of respiratory insufficiency or sleep apnea, or undiagnosed respiratory infection. Patients with one or more of these risk factors may belong to a high-risk group.
Prior to initiating somatropin therapy in patients with Prader-Willi syndrome, assessment for signs of upper airway obstruction, sleep apnea, or respiratory infections should be performed.
If upper airway abnormalities are detected during evaluation, the child should be referred to an otolaryngologist for treatment and resolution of respiratory disorders before starting growth hormone therapy.
Prior to initiating growth hormone therapy, assessment for sleep apnea should be performed using standard polysomnography or nocturnal oximetry, and monitoring for its development should be continued whenever possible.
If symptoms of upper airway obstruction (e.g., new onset or worsening of snoring) develop during somatropin therapy, treatment should be interrupted and a new ENT evaluation performed.
All patients with Prader-Willi syndrome should be monitored for signs of developing sleep apnea.
Patients should be regularly checked for signs of respiratory infections, which should be diagnosed early and actively treated.
Body weight should be carefully monitored in all patients with Prader-Willi syndrome before and during growth hormone therapy.
Scoliosis is common in patients with Prader-Willi syndrome. In some children, scoliosis may progress due to rapid growth. Signs of scoliosis should be monitored during treatment.
Experience with long-term use of growth hormone for treatment of adults and patients with Prader-Willi syndrome is limited.
Children born small for gestational age.
Before initiating treatment in children born small for gestational age, other medical conditions or treatments that may affect growth should be excluded.
Prior to initiating treatment in children born small for gestational age, fasting insulin and glucose levels should be measured and repeated annually. An oral glucose tolerance test should be performed in patients at high risk for diabetes (e.g., family history of diabetes, obesity, marked insulin resistance, acanthosis nigricans). If diabetes is diagnosed, growth hormone should not be administered.
Prior to initiating treatment in children born small for gestational age, IGF-1 levels should be measured and repeated twice a year. If IGF-1 standard deviation score exceeds +2 SD compared to age- and puberty-appropriate norms upon repeat measurement, IGF-1/IGFBP-3 ratio should be considered when determining dose adjustments.
Experience with initiating treatment immediately before the onset of puberty in children born small for gestational age is limited. Therefore, initiation of therapy immediately before puberty is not recommended. Experience in patients with Silver-Russell syndrome is limited.
Some of the growth gained during growth hormone therapy in children born small for gestational age may be lost if treatment is discontinued before final height is achieved.
Chronic renal insufficiency.
In chronic renal insufficiency, renal function should be less than 50% of normal before starting therapy. Growth failure should be documented by monitoring height over one year prior to therapy. Conservative management of renal dysfunction (including control of acidosis, hyperparathyroidism, and nutrition) should be initiated and maintained during growth hormone therapy. Treatment should be discontinued following kidney transplantation.
Currently, there are no data on final adult height in patients with chronic renal dysfunction treated with Genotropin®.
Sodium content.
This medicinal product contains less than 1 mmol sodium (23 mg) per dose. Patients on a low-sodium diet may be informed that this medicinal product can be considered sodium-free.
Special precautions for handling and disposal of waste.
The solution is prepared by twisting the sections of the prefilled mixing pen to combine the solvent with the powder in the dual-chamber cartridge. The powder is dissolved by gently tilting the pen forward and backward. Do not shake vigorously, as this may cause denaturation of the active substance. The reconstituted injection solution should be colorless or slightly opalescent. The reconstituted solution should be inspected before use and only clear, particle-free solutions should be administered.
Any unused medicinal product or waste material should be disposed of in accordance with local requirements. Used prefilled pens should never be refilled and must be properly discarded.
Use during pregnancy or breastfeeding.
Pregnancy.
There are insufficient data from animal studies on the effects of Genotropin® on pregnancy, embryonal development, parturition, or postnatal development (see section "Pharmacokinetics"). Clinical studies on use during pregnancy are lacking. Therefore, somatropin-containing products are not recommended for use in pregnant women or women of childbearing potential who are not using contraception.
Breastfeeding.
Clinical studies on the use of somatropin in breastfeeding women have not been conducted. It is unknown whether somatropin is excreted in human breast milk, but absorption of intact protein from the gastrointestinal tract of the infant is highly unlikely. Therefore, somatropin products should be used with caution in breastfeeding women.
Ability to affect reaction speed when driving or operating machinery.
Genotropin® does not affect reaction speed during driving or operating machinery.
Administration and dosage.
Dosage and administration regimen should be individually adjusted.
The injection should be administered subcutaneously, and the injection site should be rotated to prevent lipodystrophy.
Growth retardation due to growth hormone deficiency in children. The usual recommended dose is 0.025–0.035 mg/kg body weight per day or 0.7–1.0 mg/m² body surface area per day. There is experience with even higher doses.
If growth hormone deficiency originated in childhood and persists into adolescence, treatment should be continued until full somatic development (i.e., body build, bone mass) is achieved. As a control measure during the transition period, one of the therapeutic goals should be reaching normal peak bone mass, defined as a T-score >–1 (i.e., standardized to adult peak bone mass, measured by dual-energy X-ray absorptiometry, adjusted for patient's sex and ethnicity). Adult dosing instructions are described below.
Prader–Willi syndrome, for improvement of growth and body composition in children. The usual dose is 0.035 mg/kg body weight per day (1.0 mg/m² body surface area per day). The daily dose should not exceed 2.7 mg. Treatment should not be used in children with growth velocity less than 1 cm per year or at an age when epiphyseal growth plates begin to close.
Growth retardation due to Turner syndrome. The recommended dose is 0.045–0.050 mg/kg body weight per day or 1.4 mg/m² body surface area per day.
Idiopathic short stature. The recommended dose is up to 0.47 mg/kg body weight per week, i.e., up to 0.067 mg/kg body weight per day.
Growth retardation in patients with chronic renal insufficiency. The recommended dose is 0.045–0.050 mg/kg body weight per day (1.4 mg/m² body surface area per day). Inadequate growth velocity may require higher doses. Dose adjustment may be necessary after 6 months of treatment.
Growth retardation in short children born small for gestational age. The usual recommended dose is 0.035 mg/kg body weight per day (1 mg/m² body surface area per day) until final height is reached (see section "Pharmacological properties").
Treatment should be discontinued after the first year if the standard deviation score for growth velocity is less than +1. Treatment should be stopped if growth velocity is less than 2 cm per year and (if confirmation is needed) bone age exceeds 14 years in girls or 16 years in boys, corresponding to the age of epiphyseal plate closure.
Table 1
Recommended dosing guidelines for children
| Indications |
mg/kg body weight |
mg/m2 body surface area |
| daily dose |
||
| Growth hormone deficiency |
0.025–0.035 |
0.7–1.0 |
| Prader-Willi syndrome |
0.035 |
1.0 |
| Turner syndrome |
0.045–0.050 |
1.4 |
| Chronic renal insufficiency |
0.045–0.050 |
1.4 |
| Growth failure in children born small for gestational age |
0.035 |
1.0 |
| Idiopathic short stature |
up to 0.067 |
up to 2 |
Adult patients with growth hormone deficiency. For patients continuing growth hormone therapy after childhood-onset growth hormone deficiency, the recommended dose is 0.2–0.5 mg per day. The dose should be gradually increased or decreased according to individual patient needs, as determined by IGF-1 concentration.
For patients in whom growth hormone deficiency developed in adulthood, therapy should be initiated at a low dose: 0.15–0.3 mg per day. The dose should be gradually increased according to individual patient needs, as determined by IGF-1 concentration.
In both cases, the goal of treatment is to achieve an IGF-1 concentration within 2 standard deviation scores (SDS) of the age-adjusted mean. Patients with IGF-1 concentrations within the normal range at the start of treatment should receive growth hormone at a dose required to increase IGF-1 concentration to the upper normal range, but not exceeding 2 SDS. Dose titration should also consider clinical response and adverse reactions. It is known that in some patients with growth hormone deficiency, IGF-1 levels do not normalize despite adequate clinical response; such patients do not require dose escalation. The daily maintenance dose rarely exceeds 1.0 mg per day. Women may require higher doses than men, as men tend to become more sensitive to IGF-1 over time. This implies a risk of suboptimal clinical response in women, particularly those receiving oral estrogen replacement therapy, and a risk of excessive response in men. Therefore, the accuracy of the growth hormone dose should be reviewed every 6 months. Since there is a physiological decline in growth hormone production with age, the dose may be reduced. In patients aged 60 years and older, therapy should be initiated at a dose of 0.1–0.2 mg per day; the dose should be slowly increased according to individual patient needs. The lowest effective doses should be used. The daily maintenance dose for these patients rarely exceeds 0.5 mg per day.
Information for the patient
Instructions for using the pre-filled pen for dosing 5.3 mg or 12 mg
Genotropin® is administered using a single-use, multi-dose pre-filled pen (GoQuick pen) containing 5.3 mg or 12 mg of somatropin. The pen containing 5.3 mg allows administration of doses from 0.1 mg to 1.5 mg. Each turn of the black ring changes the dose by 0.05 mg. The pen containing 12 mg allows administration of doses from 0.3 mg to 4.5 mg. Each turn of the black ring changes the dose by 0.15 mg. The medication in the pen is mixed only once before starting a new pen. Cartridges do not need to be replaced. After the medication in the pen is used up, a new pen is used. The pen has a dose memory feature. The dose is set once at the beginning of use. After that, the pen allows delivery of the same preset dose for each injection. This prevents exceeding the preset dose.
Genotropin® 5.3 mg is supplied in a pre-filled pen with an injection button, logo, and blue markings; 12 mg is supplied in purple.
Important information
- Do not mix the powder and liquid in the pre-filled pen if the pen does not have a needle attached.
- Do not store the pen with a needle attached. The medication may leak from your pen, and air bubbles may form in the cartridge. Always remove the needle and replace the cap or needle shield before storage.
- Be careful not to drop the pen. If you drop the pen and any part breaks or becomes damaged, do not use it. Contact your doctor or nurse to obtain a new pen. If you drop the pen but it is not damaged or broken, perform the preparation steps as described in Step 6 (see section "Setting up and using a new GoQuick pen" below).
- Clean the pen with a damp cloth. Do not place the pen in water.
- Always use a new needle for each injection. Do not allow anyone else to use your pen needles.
- The residual volume scale along the side of the cartridge holder is a guide to indicate the amount of Genotropin® remaining in your pen.
Storage and disposal
- Do not use the pen after the expiration date.
- After 28 days from mixing, the pen must be discarded (disposed of), even if some medication remains.
- When discarding (disposing of) the pen, follow applicable health and safety regulations. If you are unsure what to do, consult your doctor or nurse.
Below is a detailed description of the steps for using the pen for dosing 5.3 mg. For dosing 12 mg, perform analogous steps. The external appearance and design of the needle may differ.
Parts of the GoQuick pen
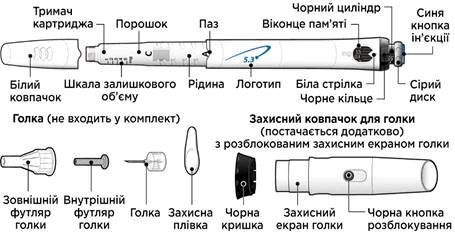
Needles for the pen are not included in the packaging. You will need to purchase needles up to 8 mm in length from a pharmacy.
- Needles suitable for use with the GoQuick pen:
- 31G or 32G — «Becton Dickinson and Company»
- 31G or 32G — «Novo Nordisk®»
- 32.5G or 34G — «Terumo»
Setting up and using a new GoQuick pen
Step 1. Preparation

- Wash and dry your hands.
- Prepare the following items on a clean, flat surface:
- New pen.
- New needle (not included).
- Appropriate sharps container (not included).
- Check the expiration date on the pen label. Do not use the pen if it has expired.
Step 2. Choose an injection site

- Select and clean the injection site according to your doctor’s or nurse’s instructions. Each time you give yourself an injection, choose a different site. Each new injection should be at least 2 cm away from the previous injection site.
- Avoid areas with bones, bruises or redness, painful or hard areas, and areas of skin with scars or skin disorders.
Step 3. Attach a new needle

- Remove the white cap from the pen, holding it straight.
- Take a new needle and remove the protective film.
- Carefully press and then screw the needle onto the pen. Do not overtighten.
Note. Be careful: do not attach the needle at an angle — this may cause the pen to leak.
- Leave both needle caps on the needle.
Step 4. Mix the medication
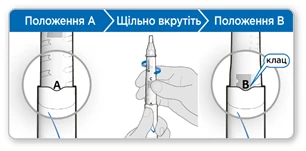
- Hold the pen with the needle end pointing upward so that mark A is facing you.
- Firmly screw the cartridge holder into the pen until it clicks into place at mark B in the groove.
- Carefully tilt the pen from side to side to completely dissolve the powder. Do not shake. Shaking may alter the growth hormone.
- Ensure that the liquid in the cartridge is clear and all powder is dissolved.
- If the liquid is cloudy or you see powder, gently tilt the pen from side to side several more times.
- If the liquid is still cloudy or you see powder, do not use this pen; use a new pen instead.
Step 5. Remove air from the pen
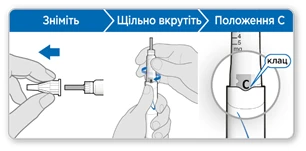
- Remove the outer needle cap. Keep it to remove the needle after injection.
- Leave the inner needle cap in place.
Note: You should see the inner needle cap after removing the outer cap. If you do not see it, try attaching the needle again.
- Hold the pen with the needle end pointing upward.
- Gently tap the cartridge holder to move air bubbles to the top.
- Firmly screw the cartridge holder into the pen until it clicks into place at mark C in the groove.
- A small amount of liquid may appear around the inner needle cap. This is normal.
Step 6. Prime the pen

Priming removes residual air by expelling a small amount of liquid from your pen. The priming dose is 0.1 mg for the pen containing 5.3 mg of somatropin and 0.3 mg for the pen containing 12 mg of somatropin, and differs from the dose prescribed by your doctor or nurse. Prime the pen only the first time you use it.
Remove the inner needle cap and discard it.
Caution! Do not touch the needle to avoid accidental needle stick.
- Ensure that the memory window displays 0.1 mg for the pen containing 5.3 mg of somatropin or 0.3 mg for the pen containing 12 mg of somatropin.
- Turn the grey dial in the direction of the arrows until it stops clicking.
- Hold the pen so that the needle points straight upward.
- Press the blue injection button fully.
- Check for liquid at the needle tip. If liquid appears, your pen is primed.
- If no liquid appears, repeat the priming steps two more times.
- If no liquid still appears, do not use the pen. Contact your doctor or nurse for advice.
Step 7. Set and select your dose

The first time you use the pen, you will set the dose prescribed by your doctor or nurse.
You do not need to set the dose again until you start using a new pen or until your doctor or nurse instructs you otherwise.
- Turn the black ring counterclockwise until your dose aligns with the white arrow in the memory window. Be careful not to turn the grey dial.
- If you turn the ring past your dose so that it goes beyond the white arrow, turn the black ring back to set the correct dose.
Note: If you cannot turn the black ring, press the blue injection button until it stops clicking. Then try setting the dose again. Note that liquid will leak from the needle.
- Turn the grey dial in the direction of the arrows until it stops clicking.
Step 8. Check your dose

Your dose on the black cylinder should align with the white arrow.
- Check that the dose you set on the black cylinder matches the dose you set in the memory window.
- If the doses match, your pen is ready for injection.
- If the doses do not match, ensure that you turned the grey dial in the direction of the arrows until it stopped clicking.
Step 9. Administer the injection
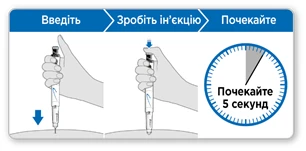
- Hold the pen over the injection site.
- Insert the needle straight into the skin.
- Press the injection button down until it stops clicking.
- Wait 5 seconds to ensure the full dose is delivered. Continue to gently press the injection button while counting.
- After 5 seconds, remove the needle from the skin.
Note: If you see a drop of liquid at the injection site or on the needle tip, try pressing the blue button longer before removing the needle during your next injection.
Step 10. Remove the needle

- Carefully cover the needle with the outer needle cap.
Caution! Do not touch the needle to avoid accidental needle stick.
- Use the needle cap to unscrew the needle.
- Discard (dispose of) the needle in an appropriate sharps container.
- Replace the white cap on the pen.
- Store the pen in the refrigerator until the next injection.
Regular (daily) use of the GoQuick pen
Step 1. Preparation
- Wash and dry your hands.
- Prepare the following items on a clean, flat surface:
- GoQuick pen with mixed solution
- New needle (not included)
- Appropriate sharps container (not included).
- Check the expiration date on the pen label. Do not use the pen if it has expired.
- Do not use the pen if 28 days have passed since first use.
Step 2. Choose an injection site

- Select and clean the injection site according to your doctor’s or nurse’s instructions. Each time you give yourself an injection, choose a different site. Each new injection should be at least 2 cm away from the previous injection site.
- Avoid areas with bones, bruises or redness, painful or hard areas, and areas of skin with scars or skin disorders.
Step 3. Attach a new needle

- Remove the white cap from the pen, holding it straight.
- Take a new needle and remove the protective film.
- Carefully press and then screw the needle onto the pen. Do not overtighten.
Note. Be careful: do not attach the needle at an angle — this may cause the pen to leak.
- Remove both needle caps.
- Keep the outer needle cap to remove the needle after injection.
Step 4. Select your dose

- Turn the grey dial in the direction of the arrows until it stops clicking.
- Your dose on the black cylinder should align with the white arrow.
- Check that the dose you set on the black cylinder matches the dose you set in the memory window.
- If the doses match, your pen is ready for injection.
Note: If your selected dose is lower, this means there is not enough Genotropin® left in your pen to deliver a full dose.
Follow your doctor’s or nurse’s instructions if your pen does not contain a full dose. Or contact your doctor or nurse for advice.
Step 5. Administer the injection

- Hold the pen over the injection site.
- Insert the needle straight into the skin.
- Press the blue injection button down until it stops clicking.
- Wait 5 seconds to ensure the full dose is delivered. Continue to gently press the blue injection button while counting.
- After 5 seconds, remove the needle from the skin.
Note: If you see a drop of liquid at the injection site or on the needle tip, try pressing the blue button longer before removing the needle during your next injection.
Step 6. Remove the needle

- Carefully cover the needle with the outer needle cap.
Caution! Do not touch the needle to avoid accidental needle stick.
- Use the needle cap to unscrew the needle.
- Discard (dispose of) the needle in an appropriate sharps container.
- Replace the white cap on the pen.
- Store the pen in the refrigerator until the next injection.
Using the needle guard (optional)
The needle guard is an additional accessory not included in the packaging, designed to conceal the needle during injection.

Attach the needle guard:
Attach the needle guard after Step 5 (see section "Setting up and using a new GoQuick pen" above) to prevent needle snagging.
- Remove the black cap from the needle guard.
- If the needle shield slips out, reinsert it into the needle guard until it clicks.
- Align the logo on the needle guard with the logo on the pen. Carefully attach the needle guard to the pen until it clicks.
- After Step 6 (see section "Setting up and using a new GoQuick pen" above), press the black button to unlock the needle shield of the needle guard.
- Follow the instructions in Step 7 (see section "Setting up and using a new GoQuick pen" above).
To remove the needle with the attached needle guard:
- Insert the outer needle cap into the end of the needle shield.
- Using the outer needle cap, push the needle shield until it clicks.
- Using the needle cap, unscrew the needle and discard (dispose of) it in an appropriate sharps container.
- Leave the needle guard on the pen.
- Replace the black cap on the needle guard. Store the pen in the refrigerator.
To remove the needle guard:
- First remove the needle, then carefully remove the needle guard from the pen.
- Do not discard the needle guard. It can be reused with the next pen.
Children.
The medication may be used in pediatric practice.
Overdose.
Symptoms. Acute overdose may initially lead to hypoglycemia and subsequently to hyperglycemia.
Chronic overdose may lead to signs and symptoms consistent with known effects of excess human growth hormone.
Adverse Reactions.
Patients with growth hormone deficiency typically have a deficit of extracellular fluid. After initiation of somatropin therapy, rapid compensation of this fluid deficit occurs. In adult patients, fluid retention-related adverse reactions commonly occur and include peripheral edema, facial edema, limb stiffness, arthralgia, myalgia, and paresthesia. Overall, these adverse reactions are mild or moderate in severity, occur during the first months of treatment, and resolve spontaneously or after dose reduction.
The frequency of these adverse effects depends on the dose of the drug, patient age, and possibly is inversely proportional to the age at which growth hormone deficiency developed. Such adverse effects occur infrequently in children.
Genotropin® induces antibody formation in approximately 1% of patients. These antibodies are characterized by low binding affinity, and their formation has not led to any clinical changes (see section "Special Warnings and Precautions for Use").
List of suspected adverse reactions.
Below is a list of adverse reactions classified by system organ classes and frequency for children and adults: very common (≥1/10); common (≥1/100 to <1/10); uncommon (≥1/1000 to <1/100); rare (≥1/10,000 to <1/1000); very rare (<1/10,000); frequency not known (cannot be estimated from available data).
Benign, malignant, and unspecified neoplasms (including cysts and polyps). Uncommon: leukemia† (children).
Metabolism and nutrition disorders. Frequency not known: type 2 diabetes mellitus (adults and children).
Nervous system disorders. Common: paresthesia* (adults), carpal tunnel syndrome (adults); uncommon: benign intracranial hypertension (children), paresthesia* (children); frequency not known: benign intracranial hypertension (adults), headache (adults and children).
Skin and subcutaneous tissue disorders. Uncommon: rash**, pruritus**, urticaria** (children); frequency not known: rash**, pruritus**, urticaria** (adults).
Musculoskeletal and connective tissue disorders. Very common: arthralgia* (adults); common: myalgia* (adults), limb stiffness* (adults), arthralgia* (children); uncommon: myalgia* (children); frequency not known: limb stiffness* (children).
Reproductive system and breast disorders. Uncommon: gynecomastia (adults and children).
General disorders and administration site conditions. Very common: peripheral edema* (adults), injection site reaction$ (children); uncommon: peripheral edema* (children); frequency not known: facial edema* (adults and children), injection site reaction$ (adults).
Investigations. Frequency not known: decreased serum cortisol levels‡ (adults and children).
* Generally, these adverse reactions are mild or moderate in intensity, occur during the first months of treatment, and resolve spontaneously or after dose reduction. The frequency of these adverse reactions depends on the dose of the drug and patient age. Possibly, the frequency is inversely proportional to the age at which growth hormone deficiency developed.
** Adverse reactions identified in post-marketing studies.
$ Transient injection site reactions have been reported in children.
‡ Clinical significance unknown.
† This reaction has been reported in children with growth hormone deficiency receiving somatropin therapy. The incidence is likely not different from that in children without growth hormone deficiency.
Decreased serum cortisol levels.
Somatropin has been reported to reduce serum cortisol levels, possibly due to effects on transport proteins or increased hepatic clearance. The clinical significance of these findings may be limited. Nevertheless, corticosteroid replacement therapy should be optimized prior to initiation of Genotropin® treatment.
Prader–Willi Syndrome.
During the post-marketing period, isolated cases of sudden death have been reported in patients with Prader–Willi syndrome receiving somatropin therapy; however, a causal relationship with treatment has not been established.
Leukemia.
Cases of leukemia have been reported in children with growth hormone deficiency, some of whom were receiving somatropin therapy, including during the post-marketing period. However, there is no evidence of increased risk of leukemia in the absence of predisposing factors such as cranial irradiation.
Slipped capital femoral epiphysis or Legg–Calvé–Perthes disease.
Slipped capital femoral epiphysis and Legg–Calvé–Perthes disease have been reported in children receiving growth hormone therapy. Slipped capital femoral epiphysis most commonly occurs in endocrine disorders, and Legg–Calvé–Perthes disease is most commonly observed in short stature. However, it is unknown whether these two conditions occur more frequently with somatropin therapy. This diagnosis should be considered in a child presenting with discomfort or pain in the hip or knee area.
Other adverse drug reactions.
Other adverse drug reactions that may be considered class effects of somatropin include, in particular, possible hyperglycemia due to reduced insulin sensitivity, decreased levels of free thyroxine, and benign intracranial hypertension.
Reporting of suspected adverse reactions.
Reporting of suspected adverse reactions after marketing authorization is important. It allows continuous monitoring of the benefit-risk balance of the medicinal product.
Shelf life. 3 years.
Storage conditions. Store at 2–8 °C in the original packaging to protect from light.
The reconstituted solution may be stored at 2–8 °C for 28 days in the original packaging to protect from light.
Keep out of the reach of children.
Incompatibilities. Since compatibility studies have not been conducted, this medicinal product must not be mixed with other medicinal products.
Packaging. 5.3 mg: 1 pre-filled pen containing 1 dual-chamber cartridge (front chamber with powder and rear chamber with diluent), in a cardboard box.
12 mg: 1 or 5 pre-filled pens, each containing 1 dual-chamber cartridge (front chamber with powder and rear chamber with diluent), in a cardboard box.
Prescription status. Prescription only.
Manufacturer.
Pfizer Manufacturing Belgium NV.
Manufacturer's address and place of business.
Reyksweg 12, Puurs-Sint-Amands, 2870, Belgium.