Esketamine kalceks
UkraineTable of Contents
INSTRUCTIONS FOR MEDICAL USE OF THE MEDICINAL PRODUCT ESKETAMINE KALCEKS (ESKETAMINE KALCEKS)
Composition:
Active substance: esketamine hydrochloride;
1 ml of solution (1 ampoule) contains esketamine hydrochloride 5.77 mg (equivalent to 5 mg of esketamine);
5 ml of solution (1 ampoule) contains esketamine hydrochloride 28.85 mg (equivalent to 25 mg of esketamine);
1 ml of solution (1 ampoule) contains esketamine hydrochloride 28.85 mg (equivalent to 25 mg of esketamine);
2 ml of solution (1 ampoule) contains esketamine hydrochloride 57.7 mg (equivalent to 50 mg of esketamine);
10 ml of solution (1 ampoule) contains esketamine hydrochloride 288.5 mg (equivalent to 250 mg of esketamine);
Excipients: sodium chloride, hydrochloric acid concentrated, water for injections.
Pharmaceutical form. Solution for injection and infusion.
Main physico-chemical properties: clear, colourless solution.
Pharmacotherapeutic group. Anaesthetics. General anaesthetic agents.
ATC code N01AX14.
Pharmacological Properties
Pharmacodynamics
Esketamine is a chiral derivative of cyclohexanone that exerts analgesic effects and, at higher doses, anesthetic effects. Esketamine produces so-called dissociative anesthesia. By interfering with associative pathways in the brain, esketamine induces a cataleptic state resembling unconsciousness and amnesia.
The components of racemic ketamine include esketamine and (R)-ketamine. Analgesic action is primarily achieved by esketamine blocking N-methyl-D-aspartate (NMDA) receptors. The relative potency of analgesic anesthesia between the R- and S-isomers is approximately 1:3.
Esketamine exerts pronounced local anesthetic effects on the spinal cord and peripheral nerves. Esketamine does not cause respiratory or circulatory depression; it only slightly interferes with protective reflexes. During anesthesia with esketamine, muscle tone is maintained or even enhanced, and protective reflexes are generally preserved. The seizure threshold is not lowered. With spontaneous respiration, an increase in intracranial pressure may occur, which can be avoided by adequate pulmonary ventilation.
Due to its sympathomimetic effect, esketamine increases arterial blood pressure and heart rate, leading to increased myocardial oxygen consumption and coronary blood flow. Esketamine exerts negative inotropic and antiarrhythmic effects on the heart. Peripheral resistance changes only slightly due to opposing effects.
After administration of esketamine, mild hyperventilation may be observed, but this has no significant impact on blood gas exchange.
Esketamine exerts a bronchodilatory effect, making it suitable for use in patients with asthma and during mechanical ventilation in patients with status asthmaticus.
Pharmacokinetics
Differences in the pharmacokinetics of esketamine and racemic (±) ketamine are absent or very minor. Therefore, reference can be made to the pharmacokinetic data of racemic ketamine (hereinafter referred to as ketamine). The pharmacokinetics of ketamine are linear.
Absorption
Ketamine is rapidly absorbed following intramuscular administration, with a bioavailability of 90%.
Distribution
Plasma protein binding is approximately 50%. Ketamine is highly lipid-soluble.
Ketamine rapidly distributes into highly perfused tissues (e.g., heart, lungs, and brain), followed by muscle and peripheral tissues, and subsequently into adipose tissue. In humans, after an intravenous bolus dose of 2.5 mg/kg, the distribution phase of ketamine lasts approximately 45 minutes, with a half-life of elimination of 10 to 15 minutes, corresponding to the duration of the anesthetic effect (approximately 20 minutes). Plasma concentration of esketamine reaches approximately 2.6 µg/mL at 1 minute and 0.9 µg/mL at 5 minutes after an intravenous bolus dose of 1 mg/kg esketamine. Peak plasma concentration of esketamine is approximately 0.14 µg/mL at 25 minutes after an intramuscular dose of 0.5 mg/kg esketamine.
Biotransformation
Ketamine is metabolized in the liver by demethylation (via the cytochrome P450 system) into the significantly less potent primary metabolite norketamine and other inactive metabolites. The enzyme CYP3A4 is the primary enzyme responsible for N-demethylation of ketamine to norketamine in human liver microsomes; interactions with CYP2B6 and CYP2C9 enzymes are secondary. Metabolism is rapid and largely complete, with a metabolic clearance rate of 1200 to 1500 mL/min.
Elimination
The terminal elimination half-life of ketamine ranges from 79 minutes (after continuous infusion) to 186 minutes (after low-dose intravenous administration). Approximately 98% of ketamine and its metabolites are excreted via the kidneys and 2% via feces, with only a negligible amount excreted unchanged. About 95% of the administered dose is eliminated within the first 24 hours.
Clinical characteristics.
Indications.
- Induction and maintenance of general anesthesia as a sole anesthetic agent or in combination with another anesthetic;
- anesthesia and analgesia in emergency medicine;
- supplementation to regional or local anesthesia.
Contraindications.
- Patients for whom increased arterial or intracranial pressure poses a serious risk.
- As a sole anesthetic agent in patients with evident ischemic cardiac disorders.
- Eclampsia and pre-eclampsia.
- In combination with xanthine derivatives and ergometrine.
- Hypersensitivity to the active substance or to any of the excipients of the medicinal product.
Interaction with other medicinal products and other forms of interaction.
Concomitant administration is contraindicated:
The seizure threshold may be lowered when used in combination with xanthine derivatives (e.g., aminophylline, theophylline); therefore, such combinations should be avoided. The medicinal product should not be used in combination with ergometrine.
Concomitant administration with caution:
Sympathomimetics (direct or indirect-acting), thyroid hormones, and vasopressin may lead to increased blood pressure and heart rate, which should be taken into account when administering esketamine concomitantly.
When used in combination with sedatives, benzodiazepines, or antipsychotics, adverse effects are reduced, but the duration of action of esketamine is prolonged.
Barbiturates and opioids administered concurrently with esketamine may prolong the recovery phase.
Diazepam is known to increase the elimination half-life of racemic ketamine and prolong its pharmacodynamic effect. Therefore, dose adjustment may also be required for esketamine.
The anesthetic effect of halogenated hydrocarbons (e.g., halothane, isoflurane, desflurane, sevoflurane) is enhanced by the administration of esketamine; therefore, lower doses of halogenated hydrocarbons may be required.
The effect of non-depolarizing (e.g., pancuronium) and depolarizing (e.g., succinylcholine) muscle relaxants may be prolonged due to the use of esketamine.
The risk of cardiac arrhythmia following epinephrine administration may be increased when esketamine and halogenated hydrocarbons are administered simultaneously.
Concomitant administration of esketamine and vasopressin may result in increased blood pressure.
Medicinal products that inhibit CYP3A4 enzyme activity generally reduce hepatic clearance, leading to increased plasma concentrations of CYP3A4 substrate drugs such as esketamine. When esketamine is used concomitantly with agents that inhibit CYP3A4, a reduced dose of esketamine may be required to achieve the desired clinical effect.
Agents that induce CYP3A4 enzyme activity generally increase hepatic clearance, leading to decreased plasma concentrations of CYP3A4 substrate drugs such as esketamine. When esketamine is used concomitantly with CYP3A4-inducing agents, an increased dose of esketamine may be required to achieve the desired clinical effect.
Special precautions for use.
Esketamine should be used with caution in the following situations:
- Hypovolemia, dehydration, or heart disease, particularly ischemic heart disease (e.g., congestive heart failure, myocardial ischemia, and myocardial infarction), due to a significant increase in myocardial oxygen consumption;
- Decompensated heart failure and untreated hypertension;
- Unstable angina or myocardial infarction within the last 6 months;
- Mild to moderate hypertension and tachyarrhythmia;
- Increased intracranial pressure and injury or disease of the central nervous system, as increased cerebrospinal pressure has been reported in association with ketamine anesthesia;
- Pulmonary or upper respiratory infection (esketamine sensitizes the pharyngeal reflex, potentially causing laryngospasm);
- In patients with elevated intraocular pressure (e.g., glaucoma), penetrating eye injury, or during eye examination or surgery where intraocular pressure must not increase;
- Acute intermittent porphyria (due to the potential to provoke a porphyric reaction);
- Patients under chronic or acute alcohol influence;
- Patients who have or have had serious psychiatric disorders;
- Poorly controlled hyperthyroidism;
- Situations requiring a relaxed uterine myometrium (e.g., threatened uterine rupture, umbilical cord prolapse).
Esketamine is metabolized in the liver, and hepatic clearance is required for termination of clinical effects. Abnormal liver function tests have been reported with esketamine use, particularly with prolonged administration (>3 days) or drug abuse. Prolonged duration of action may occur in patients with cirrhosis or other forms of hepatic impairment. In such patients, dose reduction should be considered.
When high doses are administered or when intravenous injection is performed rapidly, respiratory depression may occur.
Since aspiration and respiratory depression cannot be completely ruled out, intubation and ventilation equipment must be readily available.
Continuous cardiac monitoring during surgery is necessary for patients with hypertensive disease or cardiac decompensation.
If esketamine is administered to patients in shock, principles of shock therapy (volume replacement, oxygenation) must be taken into account. Particular caution is required in severe shock states when arterial pressure is difficult to measure or is absent.
Since the need for additional anesthetics or muscle relaxants cannot always be predicted, patients should fast for 4–6 hours prior to surgery to prevent aspiration. Since pharyngeal reflexes are usually preserved, mechanical stimulation of the pharynx should be avoided unless muscle relaxants are used with appropriate care.
Increased salivation should be prophylactically treated with atropine.
In diagnostic and therapeutic procedures involving the upper airways, hyperreflexia and laryngospasm may occur, especially in children. Therefore, muscle relaxants and controlled ventilation may be required during procedures involving the pharynx, larynx, and bronchi.
For surgical procedures that may involve visceral pain, muscle relaxation and additional analgesia are indicated (controlled ventilation and administration of nitrous oxide/oxygen).
After outpatient anesthesia, patients should be accompanied home, and patients should not consume alcohol for the next 24 hours.
Long-term use
Cases of cystitis, including hemorrhagic cystitis, have been reported in patients using racemic ketamine for prolonged periods (from one month to several years). Similar effects may also occur after esketamine abuse (see section "Special precautions for use" ("Abuse and dependence")). Hepatotoxicity has also been reported in patients with prolonged use of the drug (>3 days).
Abuse and dependence
Racemic ketamine has been reported to be used as a recreational drug. Reports indicate that racemic ketamine causes a variety of symptoms, including flashbacks, hallucinations, dysphoria, anxiety, insomnia, or disorientation. Cases of cystitis, including hemorrhagic cystitis, and hepatotoxicity have also been reported. Therefore, such effects cannot be excluded during esketamine use.
In individuals with a history of drug abuse or substance dependence, dependence and tolerance to esketamine may develop. Therefore, esketamine should be prescribed with caution.
The risk of psychiatric reactions occurring during recovery from anesthesia (see section "Adverse reactions") may be significantly reduced by concomitant administration of a benzodiazepine.
This medicinal product contains less than 1 mmol of sodium (23 mg) per milliliter, i.e., essentially sodium-free*.
*One 2 mL ampoule contains 2.36 mg of sodium.
One 5 mL ampoule contains 15.75 mg of sodium.
One 10 mL ampoule contains 11.8 mg of sodium.
Use during pregnancy or breastfeeding.
Pregnancy
There are no confirmed data on the use of esketamine in pregnant women. Animal studies have demonstrated reproductive toxicity. The use of esketamine should be restricted during pregnancy and administered only after careful consideration if the potential benefit to the mother outweighs the possible risk to the fetus.
Esketamine crosses the placental barrier and may cause respiratory depression in the newborn if administered during labor.
Breastfeeding
Esketamine is excreted in breast milk, but effects on the infant are unlikely when the drug is used at therapeutic doses.
Fertility
There are no data on the effect of esketamine on human fertility.
Ability to affect reaction speed when driving or operating machinery.
Treatment with esketamine may impair reaction ability. This should be taken into account in situations requiring special alertness, such as driving a vehicle or operating machinery.
Patients should not drive or operate machinery for at least 24 hours after anesthesia with esketamine.
Method of Administration and Dosage
Esketamine should be administered as a slow intravenous (i.v.) or intramuscular (i.m.) injection. If necessary, the injection may be repeated or administered as an infusion.
For hospital or pre-hospital emergency use only. Esketamine must be administered only under the supervision of an anesthesia specialist. Life-support equipment must also be available.
Wherever possible, standard fasting guidelines should be followed when administering esketamine, generally 4 to 6 hours prior to anesthesia.
Although esketamine has only a minimal effect on protective pharyngeal and airway reflexes, the possibility of aspiration of fluids or solid materials cannot be completely excluded. High doses or excessively rapid intravenous administration may cause respiratory depression.
Increased salivation may occur with the use of esketamine, which can be prevented by administering atropine or another anticholinergic agent.
Adults
For induction of general anesthesia, administer 0.5–1 mg/kg esketamine intravenously or 2–4 mg/kg intramuscularly.
To maintain general anesthesia, half of the initial dose should be administered as needed, usually every 10–15 minutes.
Esketamine may also be administered as a continuous infusion at a rate of 0.5 to 3 mg/kg/hour.
Dosage reduction is required in patients with multiple injuries or poor general condition. For example, the dose should be reduced in patients who have experienced shock; as a guideline, approximately half the usual dose should be administered.
For analgesic supplementation of regional and local anesthesia, administer 0.125–0.25 mg esketamine/kg/hour as an intravenous infusion.
For emergency analgesia, administer 0.25–0.5 mg esketamine/kg intramuscularly or 0.125–0.25 mg/kg as a slow intravenous injection.
As with other general anesthetics, individual response to esketamine varies depending on dose, route of administration, patient age, and concomitant use of other medications; therefore, dosage recommendations cannot be absolutely definitive. The dose should be titrated according to the patient's needs.
Hepatic Impairment
In patients with a history of hepatic impairment, dosage reduction should be considered in those with cirrhosis or other liver dysfunction (see section "Special Warnings and Precautions for Use").
Pediatric Population
The dosing of esketamine in pediatric patients of different ages has not been sufficiently studied. Based on limited information, no substantial difference in dosage compared to adults is expected in pediatric patients.
In pediatric surgery and emergency medicine, esketamine is primarily used as a monotherapy; in other cases, combination with sedative agents is recommended.
How to Open the Ampoule:
-
Turn the ampoule so that the colored dot faces you. Gently tap the top of the ampoule with your finger to allow the solution to flow down to the lower part of the ampoule (Fig. 1).
-
Open the ampoule with both hands: hold the lower part of the ampoule in one hand and press the upper part with the other hand away from the colored dot (Fig. 2).
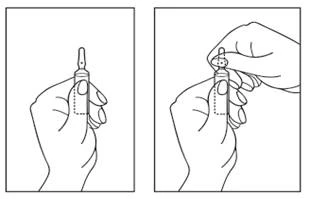
Fig. 1 Fig. 2
Parenteral medicinal products should be visually inspected for particulate matter and discoloration prior to administration whenever solution and container permit. Do not use the solution if discoloration, cloudiness, or particulate matter is present.
For single use only. The medicinal product should be used immediately after opening the ampoule. Any unused medicinal product or waste material should be disposed of in accordance with local requirements.
Esketamine Calhex may be mixed with:
- Sodium chloride 9 mg/ml (0.9%) solution for injection;
- 50 mg/ml (5%) glucose solution for injection.
After dilution to 1 mg/ml and 2 mg/ml with the above-mentioned solutions, Esketamine Calhex is chemically and physically stable in contact with PVC and EVA infusion bags, PVC and polyethylene tubing, and polypropylene and polycarbonate syringes.
Children
The dosing of esketamine in pediatric patients of different ages has not been sufficiently studied. Based on limited information, no substantial difference in dosage compared to adults is expected in pediatric patients.
In pediatric surgery and emergency medicine, esketamine is primarily used as monotherapy; for other indications, combination with sedative agents is recommended.
Overdose
Clinical symptoms of overdose include seizures, cardiac arrhythmia, and respiratory arrest.
Respiratory depression should be treated with assisted or controlled ventilation until adequate spontaneous respiration is achieved.
Convulsions should be treated with intravenous diazepam. If treatment with diazepam does not produce an adequate response, administration of phenytoin or thiopental is recommended.
To date, no specific antidote is known.
Side effects.
Adverse reactions depend on the dose and rate of injection and are spontaneously reversible. Central nervous system (CNS) and psychiatric side effects are more common when esketamine is administered as the sole analgesic agent.
The side effects listed below are categorized according to the following frequency classification:
very common (≥1/10), common (from ≥1/100 to <1/10), uncommon (from ≥1/1000 to <1/100), rare (from ≥1/10000 to <1/1000), very rare (<1/10000), frequency not known (cannot be estimated from the available data).
| From the immune system: |
|
| Rare |
Anaphylaxis |
| From the mental sphere: |
|
| Common |
Emergence reactions1 (vivid dreams, nightmares, dizziness, and motor restlessness2) |
| Frequency unknown |
Hallucinations, dysphoria, anxiety, and disorientation |
| From the nervous system: |
|
| Uncommon |
Tonic and clonic movements which may resemble convulsions (due to increased muscle tone), nystagmus |
| From the eye organs: |
|
| Common |
Blurred vision |
| Uncommon |
Diplopia, increased intraocular pressure |
| From the heart: |
|
| Common |
Transient tachycardia, increased blood pressure and heart rate (approximately 20% above baseline) |
| Rare |
Arrhythmia, bradycardia |
| From the vascular system: |
|
| Rare |
Hypotension (especially associated with circulatory shock) |
| From the respiratory system, thoracic organs and mediastinum: |
|
| Common |
Increased pulmonary vascular resistance and increased mucus secretion. Increased oxygen consumption, laryngospasm, and transient respiratory depression (the risk of respiratory suppression is generally dose- and rate-of-administration dependent) |
| From the gastrointestinal tract: |
|
| Common |
Nausea and vomiting, increased salivation |
| From the liver and/or biliary tract: |
|
| Frequency unknown |
Abnormal liver function tests. |
| From the skin and subcutaneous tissues: |
|
| Uncommon |
Measles-like rashes and exanthema |
| General disorders and injection site reactions: |
|
| Uncommon |
Pain and erythema at injection site |
1 When ketamine is used as the sole analgesic, dose-dependent reactions may occur in the recovery phase in 30% of patients.
2 These reactions can be significantly reduced by administering a benzodiazepine.
3 Prolonged use (>3 days) or drug abuse.
Shelf life.
2 years.
Shelf life after dilution
After dilution, the solution should not be stored in the refrigerator.
Chemical and physical stability after dilution has been demonstrated for 48 hours at 25 °C.
From a microbiological point of view, diluted solutions should be used immediately unless the method of dilution precludes microbial contamination.
Do not use after the expiry date stated on the packaging.
Storage conditions.
No special storage conditions required.
Do not freeze.
Keep out of the reach of children.
Incompatibilities.
Ketamine is chemically incompatible with barbiturates, diazepam, and doxapram due to precipitate formation. They should not be administered using the same syringe and needle.
This medicinal product should not be mixed with other medicinal products except those specified in the section “Dosage and administration”.
Packaging.
5 ml (for 5 mg/ml concentration), 2 ml and 10 ml (for 25 mg/ml concentration) in a clear glass ampoule of hydrolytic class I, with score marks and a break point.
5 ampoules in a blister pack made of polyvinyl chloride film.
1 or 2 blister packs together with the package leaflet in a cardboard carton with a first-opening control in the form of an adhesive label on each opening part of the carton.
Prescription status.
Prescription only.
Manufacturer.
Manufacturer responsible for batch release:
JSC "Kalceks".
Manufacturer's address and place of business.
71E Krustpils Street, Riga, LV-1057, Latvia.
Marketing Authorisation Holder.
JSC "Kalceks".
Address of the Marketing Authorisation Holder.
53 Krustpils Street, Riga, LV-1057, Latvia.