Duaklir® genueair®
Ukraine
Table of Contents
INSTRUCTIONS for medical use of the medicinal product Duaklir® Genuair®
Composition:
Active substances: aclidinium bromide, formoterol fumarate dihydrate;
One delivered dose (dose exiting the mouthpiece) contains 396 mcg of aclidinium bromide, equivalent to 340 mcg of aclidinium, and 11.8 mcg of formoterol fumarate dihydrate. This corresponds to a metered dose of 400 mcg of aclidinium bromide, equivalent to 343 mcg of aclidinium, and a metered dose of 12 mcg of formoterol fumarate dihydrate;
Excipient: each metered dose contains 11.6 mg of lactose monohydrate.
Pharmaceutical form. Powder for inhalation.
Main physicochemical characteristics: white or almost white, fine granular, free-flowing powder without visible agglomerates or foreign particles.
Pharmacotherapeutic group. Medicinal products affecting the respiratory system. Medicinal products used in obstructive airway diseases. Adrenergic agents, inhalation. Adrenergic agents in combination with anticholinergic agents, including triple combinations with corticosteroids. Formoterol and aclidinium bromide. ATC code R03AL05.
Pharmacological Properties
Mechanism of Action
Duaklir® Genuair® contains two bronchodilators: aclidinium, a long-acting muscarinic receptor antagonist (also known as an anticholinergic agent), and formoterol, a long-acting β2-adrenergic agonist. The combination of these two agents with different mechanisms of action produces an additive effect compared to administration of either component alone. Due to the differing density of muscarinic receptors and β2-adrenergic receptors in central and peripheral airways, muscarinic antagonists are expected to be more effective in dilating central airways, whereas β2-adrenergic agonists are expected to be more effective in dilating peripheral airways. The combined dilation of both central and peripheral airways in combination therapy is expected to positively affect lung function.
Aclidinium is a competitive, selective antagonist of muscarinic receptors with a longer residence time on M3 receptors than on M2 receptors. M3 receptors mediate contraction of airway smooth muscle. Inhaled aclidinium bromide acts locally in the lungs as an antagonist of M3 receptors on airway smooth muscle, resulting in bronchodilation. Aclidinium has also been shown to benefit patients with COPD by reducing symptoms, improving health status specific to the disease, reducing the frequency of exacerbations, and increasing exercise tolerance. Aclidinium bromide is rapidly degraded in blood plasma, resulting in a low incidence of systemic anticholinergic adverse reactions.
Formoteropen is a potent, selective β2-adrenergic agonist. Bronchodilation occurs due to direct relaxation of airway smooth muscle, mediated by increased intracellular cyclic AMP levels resulting from adenylate cyclase activation. In addition to improving lung function, formoterol has also been shown to reduce disease symptoms and improve quality of life in patients with COPD.
Pharmacodynamics
Clinical efficacy studies demonstrated that Duaklir® Genuair® provides clinically significant improvement in lung function (measured as forced expiratory volume in one second [FEV1]) more than 12 hours after dosing.
Duaklir® Genuair® demonstrated a rapid onset of action within 5 minutes after the first inhalation compared to placebo (p < 0.0001). The onset of action of Duaklir® Genuair® was similar to that of formoterol 12 μg, a short-acting β2-adrenergic agonist. Maximum bronchodilatory effect (peak FEV1) relative to baseline was observed on day 1 (304 mL) and was maintained throughout the 6-month treatment period (326 mL).
Cardiac Electrophysiology
In a 6–12 month Phase III clinical trial involving 4000 patients with COPD, no clinically significant effect of Duaklir® Genuair® on ECG parameters (including QT interval) was observed compared to aclidinium, formoterol, or placebo. No clinically significant effect of Duaklir® Genuair® on heart rate was observed during 24-hour Holter monitoring in a subgroup of 551 patients (114 of whom received Duaklir® Genuair® twice daily).
Clinical Efficacy and Safety
The Phase III clinical development program included 4000 patients with a clinical diagnosis of COPD. This phase included two 6-month randomized, placebo-controlled studies with an active comparator (ACLIFORM-COPD and AUGMENT), a 6-month extension of the AUGMENT study, and an additional 12-month randomized, controlled trial. Patients were allowed to continue their usual therapy with inhaled corticosteroids, low-dose systemic corticosteroids, oxygen therapy (if used less than 15 hours/day), or xanthines, and use of salbutamol as rescue medication was permitted. Efficacy was assessed based on lung function measurements, disease-specific symptomatic outcomes, use of rescue medication, and exacerbation rates. Long-term safety studies demonstrated sustained efficacy of Duaklir® Genuair® over more than one year, with no evidence of tachyphylaxis.
Effect on Lung Function
Administration of Duaklir® Genuair® 340 μg/12 μg twice daily consistently provided clinically significant improvement in lung function (measured by FEV1, forced vital capacity, and maximal expiratory volume) compared to placebo. In Phase III trials, clinically significant bronchodilation was observed within 5 minutes after the first dose and persisted throughout the dosing interval. Sustained effects were observed during both 6-month and 12-month Phase III studies. FEV1 at 1 hour post-dose and trough FEV1 (compared to 400 μg aclidinium and 12 μg formoterol, respectively) were defined as co-primary endpoints in both 6-month pivotal Phase III studies to demonstrate the bronchodilatory effects of formoterol and aclidinium in Duaklir® Genuair®.
In the ACLIFORM-COPD study, Duaklir® Genuair® demonstrated an increase in FEV1 at 1 hour post-dose compared to placebo and aclidinium: 299 mL and 125 mL, respectively (both p < 0.0001), and an increase in trough FEV1 compared to placebo and formoterol: 143 mL and 85 mL, respectively (both p < 0.0001). In the AUGMENT study, Duaklir® Genuair® demonstrated an increase in FEV1 at 1 hour post-dose compared to placebo and aclidinium: 284 mL and 108 mL, respectively (both p < 0.0001), and an increase in trough FEV1 compared to placebo and formoterol: 130 mL (p < 0.0001) and 45 mL (p = 0.01), respectively.
Positive Effect on Symptom Reduction and Disease-Specific Health Status
Dyspnea and Other Symptoms
Duaklir® Genuair® provided clinically significant reduction in dyspnea (assessed by the Transition Dyspnea Index [TDI]), with improvement in the TDI focal score after 6 months of treatment compared to placebo by 1.29 units in the ACLIFORM-COPD study (p < 0.001) and by 1.44 units in the AUGMENT study (p < 0.0001). The percentage of patients achieving a clinically significant improvement in TDI focal score (defined as an increase of at least 1 unit) was higher in the Duaklir® Genuair® group compared to placebo in the ACLIFORM-COPD study (64.8% vs. 45.5%; p < 0.001) and in the AUGMENT study (58.1% vs. 36.6%; p < 0.0001). A pooled analysis of these two studies demonstrated that Duaklir® Genuair® resulted in a statistically significant improvement in TDI focal score compared to aclidinium (0.4 units, p = 0.016) or formoterol (0.5 units, p = 0.009). Additionally, the percentage of patients achieving clinically significant improvement in TDI focal score was higher in the Duaklir® Genuair® group compared to aclidinium or formoterol groups (61.9% vs. 55.7% and 57.0%, respectively; p = 0.056 and p = 0.100, respectively). Duaklir® Genuair® reduced daytime COPD symptoms such as dyspnea, "chest symptoms" (respiratory tract symptoms), cough, and sputum production (assessed by the total E-RS score), as well as overall nighttime symptoms, morning symptoms, and symptoms limiting morning activity, compared to placebo, aclidinium, and formoterol, although improvements were not always statistically significant. Aclidinium/formoterol did not significantly reduce, compared to placebo, the average number of nighttime awakenings due to COPD symptoms.
Health-Related Quality of Life
Duaklir® Genuair® provided clinically significant improvement in health-related quality of life (assessed by the St. George's Respiratory Questionnaire [SGRQ]) in the AUGMENT study, where improvement in total SGRQ score compared to placebo was -4.35 units (p < 0.0001). The percentage of patients in the AUGMENT study achieving a clinically significant improvement in total SGRQ score compared to baseline (defined as a decrease of at least 4 units) was higher in the Duaklir® Genuair® group than in the placebo group (58.2% vs. 38.7%; p < 0.001). In the ACLIFORM-COPD study, a non-significant reduction in total SGRQ score was observed compared to placebo due to a pronounced placebo response (p = 0.598); the percentage of patients achieving clinically significant improvement compared to baseline was 55.3% in the Duaklir® Genuair® group and 53.2% in the placebo group (p = 0.669). A pooled analysis of these two studies demonstrated that Duaklir® Genuair® resulted in significant improvement in total SGRQ score compared to formoterol (-1.7 units; p = 0.018) or aclidinium (-0.79 units; p = 0.273). Additionally, a higher percentage of patients receiving Duaklir® Genuair® achieved clinically significant improvement in total SGRQ score compared to aclidinium and formoterol groups (56.6% vs. 53.9% and 52.2%, respectively; p = 0.603 and p = 0.270, respectively).
Reduction in Frequency of COPD Exacerbations
A pooled analysis of efficacy from two 6-month Phase III studies demonstrated a significant (29%) reduction in the rate of moderate or severe exacerbations (requiring treatment with antibiotics or corticosteroids or resulting in hospitalization) with Duaklir® Genuair® compared to placebo (exacerbation rate per patient per year: 0.29 vs. 0.42, respectively; p = 0.036).
Additionally, Duaklir® Genuair® delayed the time to first moderate or severe exacerbation compared to placebo (hazard ratio 0.70; p = 0.027).
Need for Rescue Medication
Duaklir® Genuair® reduced the need for rescue medication over 6 months compared to placebo (by 0.9 inhalations per day [p < 0.0001]), aclidinium (by 0.4 inhalations per day [p < 0.001]), and formoterol (by 0.2 inhalations per day [p = 0.062]).
Lung Volume Functional Parameters, Exercise Tolerance, and Physical Activity
The effect of Duaklir® Genuair® on lung volume functional parameters, exercise endurance, and physical activity was evaluated over 8 weeks in a parallel-group, randomized, placebo-controlled clinical trial in COPD patients with lung hyperinflation (functional residual capacity [FRC] > 120%). After 4 weeks of treatment with Duaklir® Genuair®, improvement in morning (pre-dose) FRC compared to baseline (primary endpoint) was observed compared to placebo, although this difference was not statistically significant (-0.125 L; 95% confidence interval [CI] -0.259, 0.010; p = 0.069*).
* Since statistical significance was not achieved for the primary endpoint, analysis of all p-values for secondary endpoints was conducted using a nominal significance level of 0.05, and no formal statistical conclusion can be drawn.
Treatment with Duaklir® Genuair® resulted in improvement in lung volume functional parameters 2–3 hours after dosing compared to placebo (FRC: -0.366 L [95% CI -0.515, -0.216; p < 0.0001]; residual volume [RV]: -0.465 L [95% CI -0.648, -0.281; p < 0.0001]; inspiratory capacity [IC]: 0.293 L [95% CI 0.208, 0.378; p < 0.0001]). Duaklir® Genuair® also improved exercise endurance compared to placebo after 8 weeks of treatment (55 seconds [95% CI 5.6, 104.8; p = 0.0292]; baseline value 456 seconds). After 4 weeks of treatment with Duaklir® Genuair®, an increase in daily step count compared to placebo was observed (731 steps/day; 95% CI 279, 1181; p = 0.0016) and a reduction in the proportion (%) of patients with low physical activity (< 6000 steps/day) [40.8% vs. 54.5%; p < 0.0001]. Patients receiving Duaklir® Genuair® showed improvement in PROactive scale scores (p = 0.0002), a tool designed to assess physical activity in COPD patients. A lifestyle modification program was added for both treatment groups for an additional 4 weeks. The daily step count in the Duaklir® Genuair® group remained unchanged at 510 steps/day compared to the placebo group (p = 0.1588); the proportion (%) of patients with low physical activity (< 6000 steps/day) decreased compared to the placebo group (41.5% vs. 50.4%; p = 0.1134).
Paediatric Population
The European Medicines Agency has waived the obligation to submit the results of clinical trials of Duaklir® Genuair® in all paediatric subpopulations with COPD (see section "Posology and Method of Administration").
Pharmacokinetics
When administered together by inhalation, the pharmacokinetics of aclidinium and formoterol showed no significant differences compared to administration of each substance alone.
Absorption
After inhalation of a single dose of Duaklir® Genuair® 340 μg/12 μg, aclidinium and formoterol are rapidly absorbed, reaching peak plasma concentrations within 5 minutes in healthy volunteers and within 24 minutes in patients with COPD. Peak plasma concentrations of aclidinium and formoterol at steady state observed in COPD patients receiving Duaklir® Genuair® twice daily for 5 days were reached within 5 minutes after inhalation and were 128 pg/mL and 17 pg/mL, respectively.
Distribution
The total amount of aclidinium delivered to the lungs via the Genuair inhaler is approximately 30% of the metered dose. In vitro, plasma protein binding of aclidinium likely reflects binding of metabolites due to rapid hydrolysis of aclidinium bromide in plasma; protein binding was 87% for the carboxylic acid metabolite and 15% for the alcohol metabolite. The main plasma protein binding aclidinium bromide is albumin. Plasma protein binding of formoterol is 61–64% (34% primarily with albumin). Binding is not saturated at concentrations achieved with therapeutic dosing.
Biotransformation
Aclidinium bromide is rapidly and extensively hydrolyzed to its pharmacologically inactive alcohol and carboxylic acid derivatives. The plasma level of the acid metabolite after inhalation is approximately 100 times higher than that of the alcohol metabolite and unchanged active substance. Both chemical (non-enzymatic) and enzymatic hydrolysis (mediated by esterases) occur. The main esterase involved in hydrolysis in humans is butyrylcholinesterase. The low absolute bioavailability of aclidinium bromide after inhalation (< 5%) is due to extensive systemic and presystemic hydrolysis in both the lungs and after oral administration. Metabolism via CYP450 enzymes plays a minor role in the overall metabolic clearance of aclidinium bromide.
In vitro studies showed that aclidinium bromide or its metabolites at therapeutic doses do not inhibit or induce any cytochrome P450 (CYP450) enzymes and do not inhibit esterase activity (carboxylesterase, acetylcholinesterase, and butyrylcholinesterase). In vitro studies also showed that aclidinium bromide or its metabolites are not substrates or inhibitors of P-glycoprotein. Formoterol is primarily eliminated via metabolism. The main pathway is direct glucuronidation with O-demethylation followed by conjugation with glucuronic acid. Cytochrome P450 isoenzymes – CYP2D6, CYP2C19, CYP2C9, and CYP2A6 – are involved in O-demethylation of formoterol. Formoterol does not inhibit CYP450 enzymes at therapeutic concentrations.
Elimination
After inhalation of Duaklir® Genuair® 340 μg/12 μg, the terminal half-life of aclidinium bromide, measured in plasma over 24 hours after dosing, ranged from 11 to 33 hours, and for formoterol, from 12 to 18 hours. The mean effective half-life (half-life corresponding to drug accumulation under a known dosing regimen) for both aclidinium and formoterol is approximately 10 hours (calculated based on accumulation ratios).
After intravenous administration of radiolabeled aclidinium bromide (400 μg) to healthy volunteers, about 1% of the dose was excreted unchanged in urine. Up to 65% of the dose was excreted as metabolites in urine and up to 33% as metabolites in feces. After inhalation of 200 μg and 400 μg aclidinium bromide in healthy volunteers and COPD patients, a very small amount, approximately 0.1% of the administered dose, was excreted unchanged in urine, indicating that renal clearance plays a minor role in the overall clearance of aclidinium from plasma. The majority of administered formoterol is metabolized in the liver and then excreted by the kidneys. After inhalation, 6–9% of the delivered dose of formoterol is excreted in urine unchanged or as formoterol conjugates.
Special Patient Populations
Elderly Patients
Pharmacokinetic studies of aclidinium/formoterol in elderly patients have not been conducted. Dose adjustment is not required for elderly patients when aclidinium or formoterol is administered separately. Therefore, dose adjustment is not considered necessary when using aclidinium/formoterol.
Patients with Hepatic or Renal Impairment
Studies in patients with hepatic or renal impairment have not been conducted. Since dose adjustment is not required for aclidinium or formoterol in patients with hepatic or renal impairment, dose adjustment is not considered necessary when using aclidinium/formoterol.
Race
In Japanese and Caucasian subjects, repeated inhalations of Duaklir® Genuair® resulted in similar systemic exposure to aclidinium and formoterol (based on AUC values).
Preclinical Safety Data
Preclinical safety data based on conventional safety pharmacology, repeated-dose toxicity, genotoxicity, carcinogenicity, and reproductive toxicity studies revealed no special risks for humans associated with the use of aclidinium and formoterol. In preclinical studies, effects of aclidinium on reproductive organs (fetotoxic effects) and fertility (slight reduction in mating frequency, number of corpora lutea, and pre- and post-implantation embryonic death) were observed only at doses significantly exceeding the maximum human dose, indicating limited relevance to clinical use. In formoterol studies, reduced fertility (post-implantation embryonic death) in rats and reduced postnatal survival and birth weight were observed at high systemic exposure levels. A slight increase in uterine leiomyoma incidence was observed in rats; this effect is considered specific to this rodent species following prolonged exposure to high-dose β2-adrenergic agonists. Preclinical studies evaluating the cardiovascular effects of aclidinium/formoterol demonstrated increased heart rate and arrhythmias at doses significantly exceeding the maximum human dose, indicating limited clinical relevance. These effects are known reactions to β2-adrenergic agonists.
Clinical characteristics.
Indications.
Maintenance bronchodilator therapy for symptomatic relief of chronic obstructive pulmonary disease (COPD) in adult patients.
Contraindications.
Hypersensitivity to the active substances or to any of the excipients.
Interaction with other medicinal products and other forms of interactions.
Medicinal products used for the treatment of COPD
Concomitant use of Duaklir® Genuair® with other anticholinergic medicinal products and/or long-acting β2-adrenergic agonists is not recommended, as it has not been studied. Although formal in vivo drug interaction studies with Duaklir® Genuair® have not been conducted, it has been used concomitantly with other medicinal products used for the treatment of COPD, including short-acting β2-adrenergic bronchodilators, methylxanthines, and inhaled corticosteroids, without occurrence of clinical signs of drug interactions.
Treatment of hypokalaemia
Concomitant use with methylxanthine derivatives, steroids, or non-potassium-sparing diuretics may potentiate the possible hypokalaemic effect of β2-adrenergic agonists; therefore, their combined use requires caution (see section "Special warnings and precautions for use").
β-blockers
β-blockers may attenuate the effect of β2-adrenergic agonists or produce antagonistic effects. If β-blockers (including ophthalmic drops) must be used, cardioselective β-blockers are recommended, although they should also be used with caution.
Other pharmacodynamic interactions
Duaklir® Genuair® should be used with caution in patients taking medicinal products that may prolong the QTc interval, such as monoamine oxidase inhibitors, tricyclic antidepressants, antihistamines, or macrolides, since the cardiovascular effects of formoterol contained in Duaklir® Genuair® may be enhanced by these medicinal products. Medicinal products that may prolong the QTc interval are associated with an increased risk of ventricular arrhythmia.
Metabolic interactions
In vitro studies have shown that aclidinium at therapeutic doses or its metabolites do not interact with medicinal products that are substrates of P-glycoprotein (P-gp), or with medicinal products metabolized by cytochrome P450 (CYP450) enzymes and esterases. Formoterol at therapeutic concentrations does not inhibit CYP450 enzymes (see section "Pharmacokinetics").
Special precautions for use.
Bronchial asthma
The medicinal product Duaklir® Genuair® should not be used in patients with bronchial asthma, as clinical trials of Duaklir® Genuair® have not been conducted in asthma.
Paradoxical bronchospasm
Paradoxical bronchospasm was not observed during clinical studies with Duaklir® Genuair®. However, paradoxical bronchospasm has been reported with other inhaled therapies. If paradoxical bronchospasm occurs, Duaklir® Genuair® should be discontinued immediately and alternative therapy should be considered.
Not intended for emergency use
Duaklir® Genuair® is not indicated for the treatment of acute bronchospasm attacks.
Effects on the cardiovascular system
β2-adrenergic agonists may increase heart rate and blood pressure. In some patients, electrocardiogram (ECG) changes such as T-wave flattening, ST-segment depression, and QTc interval prolongation have been observed. If such effects occur, discontinuation of the medicinal product may be necessary. Long-acting β2-adrenergic agonists should be used with caution in patients with QTc interval prolongation syndrome, a history of QTc prolongation, or in patients receiving medications that affect the QTc interval (see section "Interaction with other medicinal products and other forms of interaction").
Cardiac arrhythmias, including atrial fibrillation and paroxysmal tachycardia, have been reported after administration of Duaklir® Genuair® (see section "Adverse reactions"). Therefore, Duaklir® Genuair® should be used with caution in patients with cardiac arrhythmias, a history of cardiac arrhythmias, or risk factors for cardiac arrhythmias.
Systemic effects
Duaklir® Genuair® should be used with caution in patients with severe cardiovascular disorders, seizure disorders, thyrotoxicosis, or pheochromocytoma.
Metabolic effects such as hyperglycemia and hypokalemia may occur when β2-adrenergic agonists are used at high doses. In Phase III clinical trials, the incidence of notable increases in blood glucose levels with Duaklir® Genuair® was low (0.1%) and similar to that observed with placebo. Hypokalemia is usually reversible and does not require replacement therapy. In patients with severe COPD, hypokalemia may be exacerbated by hypoxia and concomitant therapy (see section "Interaction with other medicinal products and other forms of interaction"). Hypokalemia may increase the risk of cardiac arrhythmias.
Due to its anticholinergic activity, Duaklir® Genuair® should be used with caution in patients with symptomatic benign prostatic hyperplasia, urinary retention, or narrow-angle glaucoma (although direct contact of the medicinal product with the eyes is highly unlikely). Dry mouth, commonly observed during anticholinergic therapy, may lead to dental caries when treatment is prolonged.
Lactose
Duaklir® Genuair® should not be administered to patients with rare hereditary conditions of galactose intolerance, congenenital lactase deficiency, or glucose-galactose malabsorption.
Use during pregnancy or breastfeeding
Pregnancy
There are no data on the use of Duaklir® Genuair® in pregnant women.
Animal studies have shown fetal toxicity only at doses significantly exceeding the maximum recommended human dose of aclidinium. Adverse effects were also observed in reproductive function studies with formoterol at very high systemic exposure levels (see section "Preclinical safety data").
Duaklir® Genuair® should be used during pregnancy only if the expected benefit outweighs the potential risk.
Breastfeeding
It is unknown whether aclidinium and/or its metabolites or formoterol are excreted in human breast milk. Animal studies have shown that small amounts of aclidinium and/or its metabolites and formoterol are excreted in milk. Therefore, the use of Duaklir® Genuair® during breastfeeding should only be considered if the expected benefit to the mother outweighs any potential risk to the infant.
Fertility
Animal studies have shown a slight reduction in fertility only at doses significantly exceeding the maximum recommended human doses of aclidinium and formoterol (see section "Preclinical safety data"). It is considered unlikely that Duaklir® Genuair®, when used at the recommended dose, would affect human fertility.
Ability to influence the ability to drive and use machines
Duaklir® Genuair® has no effect or negligible effect on the ability to drive and use machines. However, the occurrence of blurred vision or dizziness may affect the ability to drive and use machines.
Method of Administration and Dosage
The recommended dose is 1 inhalation of Duaklir® Genuair® twice daily.
If a dose is missed, the next dose should be taken as soon as possible, and the subsequent dose should be taken at the usual time. However, if it is almost time for the next scheduled dose, the missed dose should not be administered.
Elderly Patients
Dosage adjustment is not required in elderly patients (see section "Pharmacokinetics").
Renal Impairment
Dosage adjustment is not required in patients with renal impairment (see section "Pharmacokinetics").
Hepatic Impairment
Dosage adjustment is not required in patients with hepatic impairment (see section "Pharmacokinetics").
Paediatric Population
There is no experience with the use of Duaklir® Genuair® for the treatment of COPD in children and adolescents (under 18 years of age).
Method of Administration
For inhalation use only.
Patients must be instructed on the correct use of the medicinal product, as the Genuair® inhaler may function differently from inhalers previously used. Patients should be advised to carefully read the patient information leaflet for Duaklir® Genuair®.
Before first use, open the sealed package and remove the inhaler. Discard the packaging and the desiccant.
Instructions for Use
Familiarize yourself with the parts of the Genuair® inhaler

Before use:
- Open the sealed packaging before first use and remove the inhaler. Discard the packaging and the desiccant.
- Do not press the orange button until you are ready to take the dose.
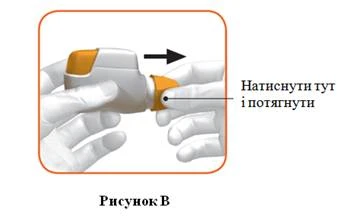
- Remove the cap by gently pressing the arrows on both sides (Figure B).
Step 1: Prepare the Dose
- Look into the mouthpiece opening and ensure it is not blocked (Figure C).
- Check the colour indicator window (should be red, Figure C).

- Hold the inhaler horizontally with the mouthpiece facing towards you and the orange button facing upwards (Figure D).
Stop and Check:
- Ensure the colour indicator window is green (Figure G).
The medicinal product is now ready for inhalation.
Proceed to section "Step 2: Inhale the Medicinal Product"

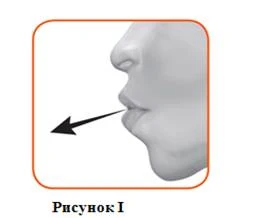
- Hold your head upright and place the mouthpiece between your lips, sealing your lips tightly around it (Figure J).
Do not press and hold the orange button during inhalation.
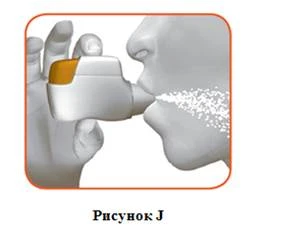
- Take a strong, deep breath in through your mouth. Continue inhaling for as long as possible.
If the inhalation is performed correctly, a click will be heard. After hearing the click, continue inhaling for as long as possible. Some patients may not hear the click. Use the colour indicator window to confirm that the inhalation was performed correctly.
- Remove the inhaler from your mouth.
- Hold your breath for as long as possible.
- Breathe out slowly, but not into the inhaler.
- Hold your breath for as long as possible.
Some patients may feel a sensation of granules in the mouth or a mild sweet or bitter taste. Do not take an additional dose, even if you do not taste anything or feel no sensation after inhalation.
Stop and Check:
- Confirm that the colour indicator window is red (Figure K). This indicates that the inhalation was performed correctly.
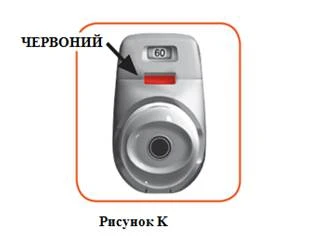
What to do if the colour indicator window remains green after inhalation (Figure L).

Additional Information
What to do if you accidentally prepared a dose?
Keep the inhaler with the protective cap on until the next scheduled dose, then remove the cap and proceed to section 1.6.
How does the dose indicator work?
- The dose indicator shows the total number of doses remaining in the inhaler (Figure N).
- At first use, the inhaler contains at least 60 doses or at least 30 doses, depending on the pack size.
- Each time a dose is prepared by pressing the orange button, the dose indicator moves slightly towards the next number (50, 40, 30, 20, 10 or 0).
When do you need a new inhaler?
You need a new inhaler:
- If your inhaler is damaged or if you have lost the cap, or
- When red stripes appear on the dose indicator, indicating that the last dose is approaching (Figure N), or
- When your inhaler is empty (Figure O).
The dose indicator moves gradually from 60 to 0: 60, 50, 40, 30, 20,
10, 0.

How to know when your inhaler is empty?
When the orange button does not return fully to its upper position and remains stuck in the middle position, this indicates that the last dose has been prepared (Figure O). Even when the orange button is stuck, you will still be able to take the last dose. After this, the inhaler cannot be used again, and you must start using a new inhaler.

How to clean the inhaler?
NEVER use water to clean the inhaler, as this may damage the medicinal product. The inhaler should not be washed. However, if necessary, the mouthpiece may be wiped with a dry cloth or paper towel.
Children
Duaklir® Genuair® is not recommended for use in children (under 18 years of age) due to insufficient clinical experience in this patient population with COPD.
Overdose
Information on treatment measures in case of overdose with Duaklir® Genuair® is limited. High doses of aclidinium bromide may cause symptoms of anticholinergic and/or β2-adrenergic effects; the most common of these symptoms include blurred vision, dry mouth, nausea, muscle cramps, tremor, headache, palpitations, and arterial hypertension. In case of overdose, administration of Duaklir® Genuair® should be discontinued. Supportive and symptomatic therapy is recommended.
Adverse Reactions
The safety profile is based on experience obtained from the use of the medicinal product Duaklir® Genuair® and its individual components.
Overview of the safety profile
The safety experience with Duaklir® Genuair® covers the period of clinical studies using the recommended therapeutic dose for up to 12 months, as well as post-marketing surveillance. Adverse reactions associated with the use of Duaklir® Genuair® were similar to those observed with its individual components. Since Duaklir® Genuair® contains aclidinium and formoterol, the type and severity of adverse reactions known for each component may also be expected with the use of Duaklir® Genuair®.
The most commonly observed adverse reactions during treatment with Duaklir® Genuair® are nasopharyngitis (7.9%) and headache (6.8%).
Table of adverse reactions
The clinical development program for Duaklir® Genuair® involved patients with moderate to severe COPD. A total of 1222 patients received Duaklir® Genuair® 340 mcg/12 mcg. The frequency of the adverse reactions listed below was determined based on overall incidence rates of adverse reactions associated with Duaklir® Genuair® observed in randomized, placebo-controlled Phase III clinical trials of at least 6 months' duration, or based on experience with its individual components, or from post-marketing data.
The frequency of adverse reactions is classified as follows: very common (≥ 1/10), common (≥ 1/100 to < 1/10), uncommon (≥ 1/1000 to < 1/100), rare (≥ 1/10,000 to < 1/1000), very rare (< 1/10,000); frequency not known (cannot be estimated from available data).
| System organ classes |
Adverse reactions |
Frequency |
| Infections and parasitic diseases |
Nasopharyngitis Urinary tract infections Sinusitis Dental abscess |
Common |
| Immune system disorders |
Hypersensitivity reactions |
Uncommon |
| Angioedema Anaphylactic reaction |
Frequency unknown |
|
| Metabolism and nutrition disorders |
Hypokalaemia Hyperglycaemia |
Uncommon |
| Psychiatric disorders |
Insomnia Anxiety |
Common |
| Agitation |
Uncommon |
|
| Nervous system disorders |
Headache Dizziness Tremor |
Common |
| Dysgeusia |
Uncommon |
|
| Eye disorders |
Blurred vision |
Uncommon |
| Cardiac disorders |
Cardiac arrhythmias, including atrial fibrillation and paroxysmal tachycardia Tachycardia QTc interval prolongation on electrocardiogram Palpitations Angina pectoris |
Uncommon |
| Respiratory, thoracic and mediastinal disorders |
Cough |
Common |
| Dysphonia Throat irritation |
Uncommon |
|
| Bronchospasm, including paradoxical |
Rare |
|
| Gastrointestinal disorders |
Diarrhoea Nausea Dry mouth |
Common |
| Stomatitis |
Uncommon |
|
| Skin and subcutaneous tissue disorders |
Rash Pruritus |
Uncommon |
| Musculoskeletal and connective tissue disorders |
Myalgia Muscle cramps |
Common |
| Renal and urinary disorders |
Urinary retention |
Uncommon |
| Investigations |
Increased blood creatine phosphokinase levels |
Common |
| Increased blood pressure |
Uncommon |
Reporting of suspected adverse reactions.
Reporting of adverse reactions after drug registration is of great importance. It enables continuous monitoring of the benefit-risk balance of the medicinal product. Medical and pharmaceutical professionals, as well as patients or their legal representatives, should report all cases of suspected adverse reactions and lack of efficacy via the automated pharmacovigilance information system at the following link: https://aisf.dec.gov.ua.
Shelf life.
3 years. Use within 60 days after first opening.
Storage conditions.
No special storage conditions required. Store the inhaler in its original packaging until first use. Keep out of reach of children.
Packaging.
60 doses of powder in an inhaler, 1 or 3 inhalers per aluminium laminated pouch, each with a desiccant packet, in a cardboard box.
Prescription status.
Prescription only.
Manufacturer.
Industrias Farmacéuticas Almirall S.A.
Manufacturer's address.
Ctra. de Martorell 41-61, 08740 Sant Andreu de la Barca (Barcelona), Spain.
Marketing Authorization Holder.
Berlin-Chemie AG.
Address of the Marketing Authorization Holder.
Glienicker Weg 125, 12489 Berlin, Germany.