Seretide diskus
Ukraine
Table of Contents
INSTRUCTIONS FOR MEDICAL USE OF THE MEDICINAL PRODUCT Seretide Diskus (Seretide Diskus)
Composition:
Active substances: salmeterol xinafoate, fluticasone propionate;
One dose of the medicinal product contains 50 mcg of salmeterol (as micronized salmeterol xinafoate) and 100 mcg of fluticasone propionate (micronized), or 50 mcg of salmeterol (as micronized salmeterol xinafoate) and 250 mcg of fluticasone propionate (micronized), or 50 mcg of salmeterol (as micronized salmeterol xinafoate) and 500 mcg of fluticasone propionate (micronized);
Excipient: lactose monohydrate.
Pharmaceutical form. Powder for inhalation, metered.
Main physicochemical properties: white or almost white powder.
Pharmacotherapeutic group. Anti-asthmatic agents for inhalation use. Adrenergic agents in combination with other anti-asthmatic drugs. Salmeterol and fluticasone. ATC code R03AK06.
Pharmacological properties.
Pharmacodynamics. Seretide Diskus contains salmeterol and fluticasone propionate, which have different mechanisms of action.
Salmetrol
Salmeterol is a selective, long-acting (12 hours) β2-adrenergic receptor agonist, possessing a long side chain that binds to the external domain of the receptor.
Salmeterol provides more prolonged bronchodilation (not less than 12 hours) compared to recommended doses of conventional short-acting β2-adrenergic agonists.
Fluticasone propionate
When inhaled at recommended doses, fluticasone propionate exerts a pronounced glucocorticoid anti-inflammatory effect in the lungs, leading to a reduction in clinical symptoms and frequency of exacerbations of bronchial asthma, without causing adverse reactions typically observed with systemic corticosteroid administration.
Pharmacokinetics
When salmeterol and fluticasone propionate are used in combination via inhalation, the pharmacokinetics of each component remain unchanged compared to when each component is administered separately. Therefore, their pharmacokinetic profiles are described individually.
Salmetrol
Salmeterol acts locally in lung tissue; therefore, its plasma concentration does not correlate with therapeutic effect. Furthermore, pharmacokinetic data for salmeterol are limited due to technical difficulties in measuring very low plasma concentrations of the drug (approximately 200 pg/mL or less) following inhaled administration at therapeutic doses.
Fluticasone propionate
Absolute bioavailability of fluticasone propionate after inhalation in healthy volunteers is approximately 5–11% of the nominal dose, depending on the inhalation device used. Lower systemic exposure levels are observed in patients with bronchial asthma following inhaled administration of fluticasone propionate. Systemic absorption occurs primarily in the lungs, initially rapidly and then more slowly. A portion of the inhaled dose may be swallowed, but its systemic effect is minimal due to the poor water solubility of fluticasone propionate and extensive first-pass metabolism in the liver. Bioavailability of fluticasone propionate following absorption from the gastrointestinal tract is less than 1%. A linear increase in plasma concentration of fluticasone propionate is observed with increasing inhaled dose. Distribution of fluticasone propionate is characterized by high plasma clearance (1150 mL/min), a large volume of distribution (approximately 300 L), and an elimination half-life of approximately 8 hours. Plasma protein binding is relatively high (91%). Fluticasone propionate is rapidly cleared from systemic circulation, primarily via metabolism into an inactive carboxylic acid metabolite by the CYP3A4 isoenzyme of the cytochrome P450 system. Other unidentified metabolites are excreted in feces. Renal clearance of fluticasone propionate is negligible, with less than 5% of the dose excreted in urine, primarily as metabolites. The majority of the dose is excreted in feces as metabolites and unchanged drug.
Clinical characteristics.
Indications.
Bronchial asthma
Regular treatment of bronchial asthma in patients who require combination therapy with a long-acting beta2-adrenergic agonist and an inhaled corticosteroid:
- patients with inadequate disease control despite regular monotherapy with an inhaled corticosteroid and as-needed use of a short-acting beta2-adrenergic agonist;
- patients with adequate disease control on treatment with an inhaled corticosteroid and a long-acting beta2-adrenergic agonist.
Chronic obstructive pulmonary disease
Maintenance therapy of chronic obstructive pulmonary disease (COPD) in patients with FEV1 < 60% of predicted values (pre-bronchodilator) and a history of recurrent exacerbations, in whom significant symptoms persist despite regular bronchodilator therapy.
Contraindications.
Hypersensitivity to any component of the medicinal product.
Interaction with other medicinal products and other forms of interaction.
Concomitant administration of non-selective and selective β2-blockers should be avoided, except when there are compelling medical reasons.
Concomitant use of medicinal products containing other β-adrenergic agents may have a potential additive effect.
Fluticasone propionate
Under normal conditions, inhaled administration results in low plasma concentrations of fluticasone propionate due to extensive first-pass metabolism and high systemic clearance mediated by cytochrome CYP3A4 in the liver and intestine. Therefore, the likelihood of clinically significant drug interactions mediated by fluticasone propionate is very low.
Data from drug interaction studies in healthy volunteers using intranasal fluticasone propionate have shown that ritonavir (a strong inhibitor of cytochrome CYP3A4) can significantly increase plasma concentrations of fluticasone propionate, leading to a marked reduction in serum cortisol levels. Such data for inhaled fluticasone propionate are lacking, but a notable increase in serum fluticasone propionate levels is expected. Cases of Cushing's syndrome and adrenal suppression have been reported. Concomitant use should be avoided unless the therapeutic benefit outweighs the increased risk of systemic glucocorticoid side effects.
In a small study in healthy volunteers using the less potent CYP3A inhibitor ketoconazole, exposure to fluticasone propionate after a single inhalation increased by 150%, resulting in a greater reduction in plasma cortisol levels compared to fluticasone propionate alone. Concomitant use with other strong CYP3A inhibitors (e.g., itraconazole, cobicistat-containing products) and moderate CYP3A inhibitors (e.g., erythromycin) is expected to increase systemic exposure to fluticasone propionate and the risk of systemic adverse effects.
Such combinations should be avoided unless the expected benefit outweighs the potential increased risk of systemic adverse reactions associated with corticosteroids; in such cases, patients should be monitored for the development of systemic adverse effects.
Salbutamol (Salmetrol)
Strong CYP3A4 inhibitors
Concomitant administration of ketoconazole (400 mg orally once daily) and salmeterol (50 mcg inhaled twice daily) for 7 days in 15 healthy volunteers resulted in a significant increase in plasma exposure to salmeterol (1.4-fold increase in Cmax and 15-fold increase in AUC). This may lead to an increased incidence of other systemic effects of salmeterol treatment (e.g., QT interval prolongation and enhanced heart rate) compared to administration of salmeterol or ketoconazole alone (see section "Special precautions").
No significant clinical effects on blood pressure, heart rate, blood glucose, or serum potassium levels were observed. Concomitant use with ketoconazole did not increase the elimination half-life of salmeterol or accumulation with repeated dosing.
Concomitant use with ketoconazole should be avoided unless the benefit outweighs the potential risk of systemic adverse effects associated with salmeterol treatment. A similar interaction risk is likely with other strong CYP3A4 inhibitors (e.g., itraconazole, telithromycin, ritonavir).
Moderate CYP3A4 inhibitors
Concomitant administration of erythromycin (500 mg orally three times daily) and salmeterol (50 mcg inhaled twice daily) for 6 days in 15 healthy volunteers resulted in a small and statistically non-significant increase in plasma exposure to salmeterol (1.4-fold increase in Cmax and 1.2-fold increase in AUC). Concomitant use with erythromycin was not associated with any adverse effects.
Special precautions for use.
Seretide Diskus is not a medication for relieving acute symptoms requiring rapid- and short-acting bronchodilators. Patients should be advised to always carry a reliever medication for symptom relief.
Seretide Diskus should not be initiated during an exacerbation of disease, or in cases of significant or acute worsening of the patient's condition and disease course.
Serious asthma-related adverse reactions and exacerbations may occur during treatment with Seretide Diskus. Patients should be advised to continue therapy but to consult their physician if symptoms remain uncontrolled or worsen after starting treatment with Seretide Diskus.
An increased use of short-acting bronchodilators to relieve asthma symptoms indicates worsening asthma control. In such cases, the patient should consult a physician.
Sudden and progressive deterioration in asthma control is potentially life-threatening, and the patient must be evaluated by a physician. An increase in corticosteroid dosage may be necessary. The patient should also seek medical evaluation if the prescribed dose of Seretide Diskus fails to provide adequate control of asthma symptoms.
When asthma symptom control has been achieved, the dose of Seretide Diskus should be gradually reduced. Regular monitoring of the patient's condition is essential during dose reduction. The lowest effective dose of this medicinal product should be used (see section "Dosage and administration").
The need for additional corticosteroid therapy should be considered in patients with asthma or COPD.
Due to the risk of asthma exacerbation, treatment with Seretide Diskus should not be stopped abruptly; the dose should be reduced gradually under medical supervision. Dose reduction must be performed under physician supervision. In patients with chronic obstructive lung diseases, discontinuation of treatment may also lead to symptom decompensation and should therefore be conducted under medical supervision.
As with any other inhaled corticosteroid-containing medication, Seretide Diskus should be administered with caution in patients with active or latent pulmonary tuberculosis, fungal, viral, or other respiratory tract infections. In such cases, appropriate treatment should be initiated immediately if necessary.
Cardiovascular effects such as increased systolic blood pressure and heart rate may occur with all sympathomimetic drugs, especially when high doses are used. Therefore, the medication should be used with caution in patients with cardiovascular disorders.
Rarely, Seretide Diskus at high therapeutic doses may cause cardiac arrhythmias, such as supraventricular tachycardia, extrasystoles, or atrial fibrillation, and mild transient reduction in serum potassium levels. Therefore, the medication should be used with caution in patients with cardiac arrhythmias, diabetes mellitus, thyrotoxicosis, uncorrected hypokalemia, or in patients predisposed to low serum potassium levels.
Very rarely, increased blood glucose levels have been reported (see section "Adverse reactions"), and this should be considered when prescribing the medication to patients with a history of diabetes mellitus.
As with other inhaled medications, paradoxical bronchospasm with immediate increase in wheezing after inhalation may occur. Immediate treatment with a rapid-acting inhaled bronchodilator should be administered. Seretide Diskus must be discontinued immediately, the patient evaluated, and alternative therapy initiated if necessary.
Adverse pharmacological effects associated with β2-agonists such as tremor, palpitations, and headache have been reported, but these are transient and tend to diminish with regular use (see section "Adverse reactions").
Seretide Diskus contains 12.5 mg of lactose monohydrate per delivered dose. This amount generally does not cause reactions in individuals with lactose intolerance. However, lactose contains a small amount of milk protein, which may trigger allergic reactions.
Prolonged use of inhaled corticosteroids, particularly at high doses, may lead to systemic effects. These are much less likely than with oral corticosteroids (see section "Overdose"). Possible systemic effects include Cushing's syndrome, Cushingoid features, adrenal suppression, growth retardation in children and adolescents, decreased bone mineralization, cataract, and glaucoma. Rarely, psychiatric disturbances and behavioral changes may occur, including psychomotor hyperactivity, sleep disturbances, agitation, depression, or aggression (predominantly in children). Therefore, it is important that patients are regularly reviewed and the dose of inhaled corticosteroid reduced to the lowest effective dose that maintains asthma control.
Long-term treatment with high doses of inhaled corticosteroids may suppress adrenal function and lead to acute adrenal crisis. Isolated cases of adrenal suppression and acute adrenal crisis have been reported with fluticasone propionate at doses of 500 mcg and 1000 mcg daily. Factors that may precipitate acute adrenal crisis include trauma, surgery, infections, or rapid dose reduction. Symptoms are often nonspecific and may include anorexia, abdominal pain, weight loss, fatigue, headache, nausea, vomiting, hypotension, decreased level of consciousness, hypoglycemia, and seizures. During periods of stress or surgical procedures, consideration should be given to the need for additional systemic corticosteroids.
Inhaled fluticasone propionate reduces the need for oral corticosteroids, but patients transitioning from oral corticosteroids may remain at risk of adrenal reserve impairment for some time. Such patients should be managed with particular care and under regular monitoring of adrenal cortex function. Patients who have previously received high-dose corticosteroids as emergency treatment also carry this risk. Potential residual insufficiency should always be considered in emergency situations or stressful conditions, and the need for corticosteroid therapy should be evaluated. Special consultation may be required before certain procedures to assess the degree of adrenal insufficiency.
Due to the potential for adrenal function impairment, switching patients from oral corticosteroid therapy to Seretide Diskus should be done with particular caution.
When initiating inhaled fluticasone propionate, withdrawal from systemic therapy should be gradual. Patients should be advised to carry a steroid alert card indicating the potential need for additional therapy during stressful situations.
Concomitant use of ritonavir may significantly increase plasma concentrations of fluticasone propionate. Therefore, co-administration should be avoided, except when the potential benefit outweighs the risk of systemic corticosteroid-related adverse reactions. The risk of systemic adverse effects is also increased when fluticasone propionate is used concomitantly with other strong CYP3A inhibitors (see section "Interaction with other medicinal products and other forms of interaction").
Pneumonia in patients with COPD
An increased incidence of pneumonia, including pneumonia requiring hospitalization, has been observed in COPD patients receiving inhaled corticosteroids. Some evidence suggests a higher risk of pneumonia with increasing steroid dose, although this has not been conclusively demonstrated in all studies.
There is no convincing clinical evidence that the use of different classes of inhaled corticosteroids is associated with differing risks of pneumonia.
Physicians should remain vigilant for possible pneumonia in COPD patients, as clinical signs of such infections may mimic symptoms of COPD exacerbation. Risk factors for pneumonia in COPD patients include smoking, advanced age, low body mass index (BMI), and severe COPD.
Concomitant use with systemic ketoconazole significantly increases systemic exposure to salmeterol, potentially increasing the incidence of systemic effects (e.g., QT interval prolongation and increased heart rate). Therefore, concomitant use with ketoconazole and other strong CYP3A inhibitors should be avoided unless the benefit outweighs the potential increased risk of systemic adverse reactions from salmeterol treatment (see section "Interaction with other medicinal products and other forms of interaction").
Visual disturbances
Visual disturbances may occur with both systemic and local use of corticosteroids. If a patient experiences symptoms such as blurred vision or other visual disturbances, they should be referred to an ophthalmologist to evaluate possible causes, which may include cataract, glaucoma, or rare conditions such as central serous chorioretinopathy, which has been reported following systemic and local corticosteroid use.
Children
Children and adolescents under 16 years of age receiving high doses of fluticasone propionate (typically ≥ 1000 mcg/day) are at particular risk of systemic effects. Systemic effects are usually associated with long-term, high-dose treatment. Possible systemic effects include Cushing's syndrome, Cushingoid features, adrenal suppression, acute adrenal crisis, growth retardation in children and adolescents, decreased bone mineralization, cataract, and glaucoma. Rarely, psychiatric disturbances and behavioral changes may occur, including psychomotor hyperactivity, sleep disturbances, agitation, depression, or aggression.
Regular monitoring of growth in children receiving long-term inhaled corticosteroid therapy is recommended. The dose of inhaled corticosteroid should be reduced to the lowest effective dose that controls asthma symptoms.
Use during pregnancy or breastfeeding.
Fertility
There are no data on effects on human fertility. Animal studies did not show effects of salmeterol or fluticasone propionate on fertility.
Pregnancy
Human data on use during pregnancy are limited. Seretide Diskus should be used during pregnancy only if the expected benefit to the mother outweighs any potential risk to the fetus. Use of Seretide Diskus during pregnancy (over 1000 cases) has not been associated with disturbances in embryonic development or fetal malformations. Results from retrospective epidemiological studies showed no increased risk of major congenital malformations after exposure to fluticasone propionate during the first trimester of pregnancy compared to other inhaled corticosteroids.
Animal studies have shown reproductive toxicity following administration of β2-adrenergic agonists and glucocorticosteroids.
The lowest effective dose of fluticasone propionate should be prescribed to pregnant women to maintain adequate asthma control.
Breastfeeding
There are no data on the concentration of the drug in human breast milk. Studies have shown that salmeterol and fluticasone propionate and their metabolites are excreted in rat milk. A risk to the infant from breastfeeding during maternal treatment with Seretide Diskus cannot be excluded. Seretide Diskus should be used during breastfeeding only if the expected benefit to the mother outweighs any potential risk to the infant.
Ability to affect the speed of reactions while driving or operating machinery.
Specific studies on the effect of Seretide Diskus on driving or operating machinery have not been conducted. However, based on the pharmacology of both components, no effect is expected.
Method of Administration and Dosage
SERETIDE DISKUS is intended for inhalation only.
Patients should understand that SERETIDE DISKUS must be used regularly, even during symptom-free periods.
Patients should undergo regular medical evaluations to ensure that their prescribed dose remains optimally effective. Dose adjustments may only be made by a physician. The dose should be reduced to the lowest effective dose that maintains control of disease symptoms. If adequate symptom control is achieved with the lowest effective dose administered twice daily, the next step may be to switch the patient to an inhaled corticosteroid alone. As an alternative for patients requiring long-acting β₂-agonists, the dose of SERETIDE DISKUS may be reduced to once daily if, in the physician’s opinion, adequate control of disease symptoms is maintained. If the patient has a history of nocturnal asthma attacks, this single daily dose should be taken at bedtime; if symptoms occur predominantly during the day, the dose should be taken in the morning.
The amount of fluticasone propionate in the chosen SERETIDE DISKUS formulation should correspond to the severity of the disease. If higher than recommended doses are required, appropriate doses of β₂-agonists and/or corticosteroids should be prescribed.
Recommended Doses
Asthma
Adults and children aged 12 years and older:
- One inhalation (50 mcg salmeterol / 100 mcg fluticasone propionate) twice daily;
- or one inhalation (50 mcg salmeterol / 250 mcg fluticasone propionate) twice daily;
- or one inhalation (50 mcg salmeterol / 500 mcg fluticasone propionate) twice daily.
For the treatment of adults and adolescents with moderate persistent asthma (daily symptoms, daily use of reliever medication, and moderate to severe airflow limitation), SERETIDE DISKUS may be used as initial maintenance therapy when rapid symptom control is required. In such cases, the recommended starting dose is one inhalation of 50 mcg salmeterol and 100 mcg fluticasone propionate twice daily. After achieving asthma symptom control, therapy should be reviewed and consideration given to switching the patient to inhaled corticosteroid monotherapy. During therapy review, regular assessment of lung function should be performed.
When one or two severity criteria are not clearly present, no clear advantage of using SERETIDE DISKUS over inhaled fluticasone propionate alone as initial maintenance therapy has been demonstrated. In general, inhaled corticosteroids remain first-line therapy for most patients. SERETIDE DISKUS is not indicated for initial treatment of mild asthma. SERETIDE DISKUS 50 mcg/100 mcg is not appropriate for the treatment of adults and children with severe asthma. For patients with severe asthma, an appropriate dose of inhaled corticosteroid should first be established before initiating any fixed-dose combination.
Children aged 4 to 12 years: one inhalation (50 mcg salmeterol / 100 mcg fluticasone propionate) twice daily.
The maximum daily dose of fluticasone propionate in SERETIDE DISKUS for children is 100 mcg twice daily.
There are no data on the use of SERETIDE DISKUS in children under 4 years of age; therefore, its use is not recommended.
Chronic Obstructive Pulmonary Disease (COPD)
Adults:
- One inhalation (50 mcg salmeterol / 500 mcg fluticasone propionate) twice daily.
Special Patient Groups
No dose adjustment is required for elderly patients or those with renal or hepatic impairment.
Instructions for Using the Inhaler
DISKUS is designed to release powder for subsequent inhalation into the lungs.
Instructions for using the DISKUS inhaler are provided below.
How to use the DISKUS INHALER
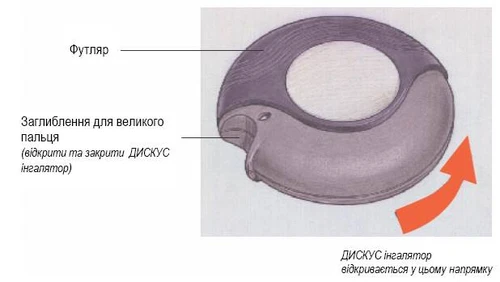
Inhaler position CLOSED (see Figure 1)
When you remove your DISKUS inhaler from the box, it should be in the closed position.
**
**
Figure 1
Inhaler position OPEN (see Figure 2)
A new DISKUS inhaler contains 60 doses of medication. The dose counter indicates how many doses remain.
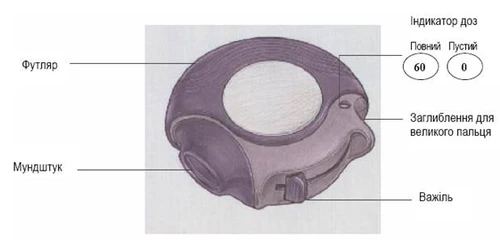
Figure 2
This DISKUS inhaler contains 60 individually packaged doses of your medication in powder form. Each dose is therefore accurately measured and hygienically protected. No special maintenance or refilling of doses is required.
The dose counter on top of the DISKUS inhaler shows how many doses of medication remain. Numbers from 5 to 0 appear in red to warn you that only a few doses are left.
The DISKUS inhaler is easy to use. When it is time to take a dose of medication, perform the following four steps, illustrated in the figures below:
- Open the inhaler.
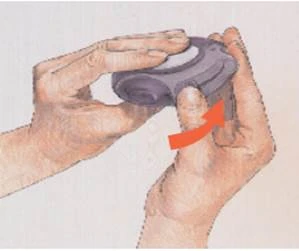
- Push the lever.
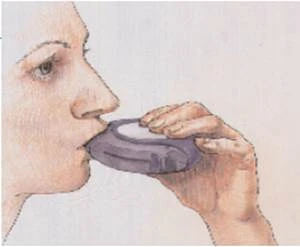
- Breathe in.
- Close the inhaler.
- Rinse the mouth with water and spit it out.
How Your DISKUS Inhaler Works
When the lever is pressed, a small opening in the mouthpiece opens and a dose is released, ready for inhalation. When you close the DISKUS inhaler, the lever automatically returns to its starting position, and the inhaler is ready to prepare the next dose if needed. The case protects your DISKUS inhaler when not in use.
|
|
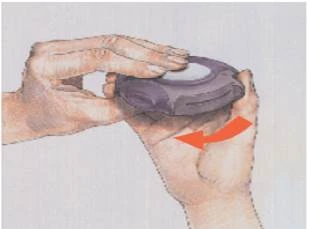
To open your DISKUS inhaler, hold the case in one hand and place the thumb of your other hand into the thumb grip. Push your thumb away from you as far as possible, and you will hear a click. |

|
|
Hold your DISKUS inhaler in either your right or left hand with the mouthpiece facing towards you. Slide the lever away from you as far as it will go until it clicks. Your DISKUS inhaler is now ready to use. Each time the lever is moved back to its starting position, a powder blister is opened and a dose of medicine is made ready to inhale. This can be seen on the dose counter. Do not play with the lever because moving it opens blisters and wastes medicine. |
|
|
Before starting the dose inhalation, carefully read this section of the instructions. Hold the DISKUS inhaler away from the mouth. Breathe out normally. Remember: never breathe out into the DISKUS inhaler.
|
|
|
To close the DISKUS inhaler, place your thumb in the thumb grip and pull towards you as far as possible. When you close the DISKUS inhaler, you will hear a click. The lever will automatically return to its starting position and the device will be reloaded. Your DISKUS inhaler is ready for reuse. |
CLEANING
To clean, wipe the DISKUS inhaler mouthpiece with a dry tissue.
REMEMBER
Keep your DISKUS inhaler in a dry place.
Keep it closed when not in use.
Never breathe out into your DISKUS inhaler.
Press the lever only when you are ready to take a dose.
Never exceed the prescribed dose.
Children.
There are no data on the use of Seretide DISKUS in children under 4 years of age; therefore, its use is not recommended in this age group.
Overdose.
Clinical trial data do not provide information on overdose with Seretide DISKUS; however, data on overdose with each of the active substances are provided below.
Signs and symptoms expected with salmeterol overdose are those typical of β2-adrenergic stimulation: dizziness, tremor, headache, tachycardia, increased systolic blood pressure. If treatment with Seretide DISKUS needs to be discontinued due to overdose of the β2-agonist component, appropriate corticosteroid replacement therapy should be initiated. Hypokalemia may also occur, and potassium replacement should be considered.
Acute overdose
Inhalation of fluticasone propionate in doses exceeding the recommended dose may cause temporary suppression of adrenal function. This does not require emergency intervention, as adrenal function recovers within a few days, which can be confirmed by measuring plasma cortisol levels.
Chronic overdose
There is a risk of adrenal suppression when higher-than-approved doses of Seretide DISKUS are used for prolonged periods.
Very rare cases of acute adrenal crisis have been reported, mainly in children who received doses higher than recommended for prolonged periods (several months or years). These cases were associated with hypoglycemia, confusion, and seizures. Situations that may potentially trigger an acute adrenal crisis include trauma, surgery, infection, and any rapid dose reduction of inhaled fluticasone propionate.
Monitoring of adrenal cortical reserve function is recommended. In case of fluticasone propionate overdose during Seretide DISKUS use, therapy may be continued at appropriate doses to maintain symptom control.
There is no specific antidote for overdose of salmeterol and fluticasone propionate; supportive treatment with monitoring of the patient's condition should be administered.
Adverse Reactions
Since Seretide Disks contains salmeterol and fluticasone propionate, adverse reactions of the types and degrees of severity typical for each component can be expected. No additional adverse effects have been observed with the combined use of both components.
Adverse effects associated with the use of salmeterol/fluticasone propionate are listed below, classified by organ systems and frequency of occurrence. Frequency is defined as: very common (≥ 1/10), common (≥ 1/100 to < 1/10), uncommon (≥ 1/1000 to < 1/100), rare (≥ 1/10,000 to < 1/1000), and not known (cannot be estimated from the available data). Frequency data are derived from clinical trial results. Events reported in the placebo group have not been included in the analysis.
| Organs and systems |
Adverse reaction |
Frequency |
| Infections and infestations |
Oral and pharyngeal candidiasis Oesophageal candidiasis Pneumonia (in COPD patients) Bronchitis |
Common Rare Common 1,3,5 Common 1,3 |
| Immune system disorders |
Hypersensitivity reactions: skin hypersensitivity reactions, angioedema (mainly of the face and oropharynx), respiratory symptoms (dyspnoea), respiratory symptoms (bronchospasm), anaphylactic reactions, including anaphylactic shock |
Uncommon Rare Uncommon Rare Rare |
| Endocrine system disorders |
Cushing's syndrome, Cushingoid symptoms, adrenal suppression, growth retardation in children and adolescents, decreased bone mineralization |
Rare 4 |
| Metabolism and nutrition disorders |
Hypokalaemia Hyperglycaemia |
Common 3 Uncommon 4 |
| Psychiatric disorders |
Restlessness, sleep disturbances Behavioural changes including hyperactivity and agitation (mainly in children) Depression, aggression (mainly in children) |
Uncommon Rare Not known |
| Nervous system disorders |
Headache Tremor |
Very common 1 Uncommon |
| Eye disorders |
Cataract Glaucoma Visual blurring |
Uncommon Rare 4 Not known 4 |
| Cardiac disorders |
Palpitations Tachycardia Cardiac arrhythmia (including supraventricular tachycardia and extrasystoles) Atrial fibrillation Angina pectoris |
Uncommon Uncommon Rare Uncommon Uncommon |
| Respiratory system disorders |
Nasopharyngitis Throat irritation Hoarseness/dysphonia Sinusitis Paradoxical bronchospasm |
Very common 2,3 Common Common Common 1,3 Rare 4 |
| Skin and subcutaneous tissue disorders |
Contusions |
Common 1,3 |
| Musculoskeletal and connective tissue disorders |
Muscle spasms Traumatic fractures Arthralgia Myalgia |
Common Common 1,3 Common Common |
- Reported as "common" in the placebo group.
- Reported as "very common" in the placebo group.
- Were observed over 3 years during the COPD study.
- See section "Special precautions for use".
- See section "Pharmacological properties".
- See section "Special precautions for use".
- Were observed over 3 years during the COPD study.
- Reported as "very common" in the placebo group.
Description of some adverse reactions
Pharmacologically mediated adverse effects of β2-agonist therapy such as tremor, subjective palpitations, and headache have been reported, but these are usually transient and tend to diminish with regular use.
As with other inhaled medications, paradoxical bronchospasm, with rapid increase in wheezing and breathlessness, may occur after inhalation. Paradoxical bronchospasm should be treated immediately with rapid-acting bronchodilators. In such cases, Seretide Diskus should be discontinued immediately, the patient should be evaluated, and alternative therapy should be considered if necessary.
Fluticasone propionate contained in the medicinal product may cause hoarseness and oropharyngeal candidiasis in some patients, and rarely, oesophageal candidiasis. The incidence of hoarseness and oropharyngeal candidiasis can be reduced by rinsing the mouth with water and/or tooth brushing after using the inhaler. Symptomatic oropharyngeal and oesophageal candidiasis can be treated with topical antifungal agents without discontinuing Seretide Diskus.
Paediatric population
Systemic effects, including Cushing's syndrome, Cushingoid features, adrenal suppression, and growth retardation, may occur in children and adolescents (see section "Special precautions for use"). Children may also experience anxiety, sleep disturbances, and behavioural changes, including hyperkinesis and agitation.
Shelf life.
2 years.
Storage conditions.
Store in the original packaging at a temperature not exceeding 30 °C. Keep out of the reach and sight of children.
Packaging. A plastic delivery device containing a foil blister with 60 evenly spaced compartments, each containing one dose of the medicinal product. Each Diskus contains 60 doses. The Diskus is packed in a cardboard box.
Prescription status. Prescription only.
Manufacturer. Glaxo Wellcome Production, France.
Glaxo Wellcome Production, France.
Address of the manufacturer and location of its operations.
Zone Industrielle No. 2, 23, rue Lavoisier, 27000 Evreux, France.
Zone Industrielle No. 2, 23, rue Lavoisier, 27000 Evreux, France.