Risperdal consta
UkraineTable of Contents
INSTRUCTIONS FOR MEDICAL USE OF THE MEDICINAL PRODUCT RISPOLEPT consta® (RISPOLEPT consta®)
Composition:
Active substance: risperidone;
One vial contains risperidone 25 mg or 37.5 mg (1 g of microspheres contains 381 mg of risperidone);
Excipients: poly(lactic-co-glycolic acid) (polymer 7525 DL JN1 [poly-(d,l-lactide-co-glycolide)]; polyvinyl alcohol; ethyl acetate; benzyl alcohol; anhydrous ethanol; water for injections;
Solvent: sodium carmellose 40 mPa·s; polysorbate 20; sodium hydrogen phosphate, dihydrate; citric acid, anhydrous; sodium chloride; sodium hydroxide; water for injections.
Pharmaceutical form. Powder and solvent for prolonged-release injectable suspension.
Main physicochemical properties:
Contents of the powder vial: white or almost white free-flowing powder, free from visible foreign particles;
Contents of the solvent syringe: clear, colorless solution without visible foreign particles.
Pharmacotherapeutic group. Psychotropic agents. Antipsychotic agents. Other antipsychotics. Risperidone. ATC code N05AX08.
Pharmacological Properties
Pharmacodynamics
Risperidone is a selective monoaminergic antagonist with unique properties. It exhibits high affinity for serotonergic 5-HT2 and dopaminergic D2 receptors. Risperidone also binds to α1-adrenergic receptors and, to a lesser extent, to H1-histaminergic and α2-adrenergic receptors. Risperidone has no affinity for cholinergic receptors. Although risperidone is a potent D2 antagonist, which contributes to its efficacy against the positive symptoms of schizophrenia, it causes minimal suppression of motor activity and induces catalepsy to a lesser extent compared to classical neuroleptics. The balanced central antagonism of serotonin and dopamine reduces the propensity for extrapyramidal side effects and broadens the therapeutic effect to include negative and affective symptoms of schizophrenia.
Pharmacokinetics
Absorption. Risperidone is completely absorbed from the Risperdal Consta® suspension.
After a single intramuscular injection of Risperdal Consta®, the release profile consisted of a minimal initial release of risperidone (<1% of the dose) followed by a lag period lasting 3 weeks. The main release of risperidone began in week 3, continued from week 4 to week 6, and declined in week 7. An oral antipsychotic should be administered during the first three weeks of treatment with Risperdal Consta® (see section "Dosage and Administration").
The combination of the release profile and dosing regimen (intramuscular injections every two weeks) results in maintenance of therapeutic plasma concentrations. Therapeutic plasma concentrations are maintained for up to 4–6 weeks after the last injection of Risperdal Consta®.
After repeated intramuscular injections of 25 or 50 mg of Risperdal Consta® every two weeks, the mean trough and peak plasma concentrations of the active antipsychotic fraction ranged from 9.9–19.2 ng/mL and 17.9–45.5 ng/mL, respectively. In patients receiving 25–50 mg injections every two weeks, no accumulation of risperidone was observed during long-term use (12 months).
The studies described above were conducted with injections into the gluteal muscle. Injections of equivalent doses into the gluteal and deltoid muscles are bioequivalent and may be alternated.
Distribution. Risperidone is rapidly distributed throughout the body. The volume of distribution is 1–2 L/kg. In plasma, risperidone is bound to albumin and acidic α1-glycoprotein. Risperidone is 90% bound to plasma proteins; 9-hydroxyrisperidone is 77% bound.
Metabolism and Elimination. Risperidone is metabolized by cytochrome CYP2D6 to 9-hydroxyrisperidone, which exerts a pharmacological effect similar to risperidone. Risperidone and 9-hydroxyrisperidone together form the active antipsychotic fraction. CYP2D6 is subject to genetic polymorphism. "Rapid" metabolizers convert risperidone to 9-hydroxyrisperidone quickly, whereas "poor" metabolizers do so significantly more slowly. Although "rapid" metabolizers have lower risperidone and higher 9-hydroxyrisperidone concentrations than "poor" metabolizers, the combined pharmacokinetics of risperidone and 9-hydroxyrisperidone (i.e., the active antipsychotic fraction) after single and multiple doses are similar in both "rapid" and "poor" CYP2D6 metabolizers.
Another metabolic pathway of risperidone is N-dealkylation. In vitro studies using human liver microsomes have shown that at clinically relevant concentrations, risperidone does not significantly inhibit the metabolism of drugs metabolized by cytochrome P450 isoenzymes, including CYP1A2, CYP2A6, CYP2C8/9/10, CYP2D6, CYP2E1, CYP3A4, and CYP3A5. One week after administration of oral risperidone, 70% of the dose is excreted in urine and 14% in feces. In urine, risperidone and 9-hydroxyrisperidone account for 35–45% of the oral dose. The remainder consists of inactive metabolites. The elimination phase ends approximately 7–8 weeks after the last injection.
Linearity. The pharmacokinetics of risperidone are linear within the dose range of 25–50 mg administered intramuscularly every 2 weeks.
Elderly patients, patients with renal or hepatic impairment.
Pharmacokinetic studies of single-dose oral risperidone showed, on average, a 43% higher plasma concentration of the active antipsychotic fraction, a 38% longer elimination half-life, and a 30% reduction in clearance of the active antipsychotic fraction in elderly patients.
In adult patients with moderate renal impairment, clearance of the active antipsychotic fraction was approximately 48% of that in patients with normal renal function (aged 25–35 years). In adult patients with severe renal impairment, clearance of the active antipsychotic fraction was approximately 31% of that in patients with normal renal function. The elimination half-life of active metabolites was 16.7 hours in adult patients, 24.9 hours in patients with moderate renal impairment (approximately 1.5 times longer than in adult patients), and 28.8 hours in patients with severe renal impairment (approximately 1.7 times longer than in adult patients).
Plasma risperidone concentrations were within the normal range in patients with hepatic impairment, but the mean free fraction of risperidone in plasma was increased by 37.1%.
Clearance after oral administration and the elimination half-life of risperidone and its active metabolites in adult patients with moderate or severe hepatic impairment did not differ significantly from those in patients with normal renal function.
Pharmacokinetic/Pharmacodynamic Relationship
No correlation was observed between plasma concentrations of the active antipsychotic fraction and changes in positive and negative symptoms or extrapyramidal symptoms during phase III trials evaluating safety and efficacy.
Sex, Race, and Smoking
Population pharmacokinetic analysis did not reveal any significant influence of sex, race, or smoking on the pharmacokinetics of risperidone or the active antipsychotic fraction.
Clinical characteristics.
Indications.
Maintenance therapy in the treatment of schizophrenia in patients whose condition has been stabilized with oral antipsychotic agents.
Contraindications.
Severe hypersensitivity to risperidone or to any other component of the medicinal product.
Interaction with other medicinal products and other forms of interaction.
Systematic studies on interactions of the medicinal product Risperdal Consta® with other medicinal products have not been conducted. The interaction data presented in this section are based on studies of interactions with oral risperidone.
Pharmacodynamic interactions.
Medicinal products that prolong the QT interval.
As with other antipsychotic medicinal products, caution should be exercised when prescribing Risperdal Consta® concomitantly with medicinal products that prolong the QT interval, such as antiarrhythmics (e.g., quinidine, disopyramide, procainamide, propafenone, amiodarone, sotalol), tricyclic antidepressants (e.g., amitriptyline), tetracyclic antidepressants (e.g., maprotiline), certain antihistamines, other antipsychotics, certain antimalarials (such as quinine and mefloquine), and medicinal products causing electrolyte imbalance (hypokalemia, hypomagnesemia), bradycardia, or inhibitors of hepatic metabolism of risperidone. This list is indicative and not exhaustive.
Central-acting medicinal products and alcohol.
Risperidone should be used with caution in combination with other centrally acting substances, particularly alcohol, opioids, antihistamines, and benzodiazepines, due to an increased risk of sedation.
Levodopa and dopamine antagonists.
Risperdal Consta® may exhibit antagonistic effects to levodopa and other dopamine antagonists. If such combination is considered necessary, especially in the terminal stage of Parkinson’s disease, the lowest effective doses should be prescribed.
Medicinal products with hypotensive effects.
During the post-marketing period, cases of clinically significant arterial hypotension have been observed with concomitant use of risperidone and antihypertensive agents.
Psychostimulants.
Combined use of psychostimulants (e.g., methylphenidate) with risperidone may lead to the emergence of extrapyramidal symptoms upon changing one or both agents for treatment (see section "Special precautions for use").
Pharmacokinetic interactions.
Risperidone is primarily metabolized via CYP2D6 and to a lesser extent via CYP3A4. Risperidone and its active metabolite 9-hydroxyrisperidone are substrates of P-glycoprotein (P-gp). Substances that modify CYP2D6 activity, or potent inhibitors or inducers of CYP3A4 and/or P-gp, may affect the pharmacokinetics of the active antipsychotic fraction of risperidone.
Potent CYP2D6 inhibitors.
Concomitant use of Risperdal Consta® with a potent CYP2D6 inhibitor may increase plasma concentrations of risperidone, but to a lesser extent than the active antipsychotic fraction. Higher doses of a potent CYP2D6 inhibitor may increase the concentration of the active antipsychotic fraction of risperidone (e.g., paroxetine, see below). Other CYP2D6 inhibitors such as quinidine are expected to affect plasma concentrations of risperidone similarly. At the initiation of concomitant therapy, and upon discontinuation of paroxetine, quinidine, or another strong CYP2D6 inhibitor, especially at high doses, the physician should review the dose of Risperdal Consta®.
Inhibitors of CYP3A4 and P-gp.
Concomitant use of Risperdal Consta® with potent inhibitors of CYP3A4 and/or P-gp may significantly increase plasma concentrations of the active antipsychotic fraction of risperidone. At the initiation of concomitant therapy, and upon discontinuation of itraconazole or other potent inhibitors of CYP3A4 and/or P-glycoprotein, the physician should review the dose of Risperdal Consta®.
Inducers of CYP3A4 and P-gp.
Concomitant use of Risperdal Consta® with potent inducers of CYP3A4 and/or P-gp may reduce plasma concentrations of the active antipsychotic fraction of risperidone. At the start of therapy, and upon discontinuation of carbamazepine or other strong inducers of CYP3A4/P-glycoprotein, the physician should review the dose of Risperdal Consta®. The effect of CYP3A4 inducers depends on time, with maximum impact potentially achieved at least 2 weeks after initiation of treatment. Accordingly, after discontinuation of inducers, CYP3A4 induction may persist for at least 2 weeks.
Medicinal products with high protein binding.
When risperidone is used concomitantly with other medicinal products that are highly bound to plasma proteins, clinically significant displacement of either drug from protein binding has not been observed. When used concomitantly with such medicinal products, the prescribing information of the other agent should be consulted regarding metabolic pathways and the need for dose adjustment.
Children.
Interaction studies have been conducted only in adult patients. It is unknown whether the results obtained can be applied to children.
Effect of other medicinal products on the pharmacokinetics of risperidone.
Antibacterial medicinal products
- Erythromycin, a moderate inhibitor of CYP3A4 and an inhibitor of P-gp, does not alter the pharmacokinetics of risperidone or the active antipsychotic fraction.
- Rifampicin, a potent inducer of CYP3A4 and an inducer of P-gp, reduces plasma concentrations of the active antipsychotic fraction.
Cholinesterase inhibitors
- Donepezil and galantamine, substrates of CYP2D6 and CYP3A4, do not demonstrate clinically significant effects on the pharmacokinetics of risperidone or the active antipsychotic fraction.
Antiepileptic medicinal products
- Carbamazepine, a potent inducer of CYP3A4 and an inducer of P-gp, has demonstrated an effect in reducing plasma concentrations of the active antipsychotic fraction of risperidone. A similar effect may be observed with phenytoin and phenobarbital, which are also inducers of hepatic enzymes CYP3A4 and P-glycoprotein.
- Topiramate moderately reduces the bioavailability of risperidone but does not affect the bioavailability of the active antipsychotic fraction. It is unlikely that this interaction would cause a clinically significant effect.
Antifungal medicinal products
- Itraconazole, a potent inhibitor of CYP3A4 and an inhibitor of P-gp, at a dose of 200 mg daily, increases plasma concentrations of the active antipsychotic fraction by approximately 70% when co-administered with risperidone at doses of 2 to 8 mg daily.
- Ketoconazole, a potent inhibitor of CYP3A4 and an inhibitor of P-gp, at a dose of 200 mg daily, increases plasma concentrations of risperidone and decreases concentrations of 9-hydroxyrisperidone.
Antipsychotic medicinal products
- Phenothiazines may increase plasma concentrations of risperidone, but not of the active antipsychotic fraction.
Antiviral medicinal products
- Protease inhibitors: study data are lacking; since ritonavir is a potent inhibitor of CYP3A4 and a weak inhibitor of CYP2D6, ritonavir and ritonavir-boosted protease inhibitors may increase plasma concentrations of the active antipsychotic fraction of risperidone.
Beta-blockers
- Some beta-blockers may increase risperidone concentrations but do not affect plasma concentrations of the active antipsychotic fraction.
Calcium channel blockers
- Verapamil, a moderate inhibitor of CYP3A4 and an inhibitor of P-gp, increases plasma concentrations of risperidone and the active antipsychotic fraction.
Medicinal products for gastrointestinal disorders
- H2-receptor antagonists: cimetidine and ranitidine, weak inhibitors of CYP2D6 and CYP3A4, increase the bioavailability of risperidone and have minimal effect on the bioavailability of the active antipsychotic fraction.
SSRIs and tricyclic antidepressants
- Fluoxetine, a potent inhibitor of CYP2D6, increases plasma concentrations of risperidone, but to a lesser extent than the active antipsychotic fraction.
- Paroxetine, a potent inhibitor of CYP2D6, increases plasma concentrations of risperidone, but (at doses up to 20 mg daily) to a lesser extent than the active antipsychotic fraction. However, higher doses of paroxetine may increase concentrations of the active antipsychotic fraction.
- Tricyclic antidepressants may increase plasma concentrations of risperidone but not of the active antipsychotic fraction. Amitriptyline does not affect the pharmacokinetics of risperidone or the active antipsychotic fraction.
- Sertraline, a weak inhibitor of CYP2D6, and fluvoxamine, a weak inhibitor of CYP3A4, at doses up to 100 mg daily, do not cause clinically significant changes in concentrations of the active antipsychotic fraction of risperidone. However, doses of sertraline or fluvoxamine exceeding 100 mg daily may increase concentrations of the active antipsychotic fraction of risperidone.
Effect of risperidone on the pharmacokinetics of other medicinal products.
Antiepileptic medicinal products
- Risperidone has no clinically significant effect on the pharmacokinetics of valproate or topiramate.
Antipsychotic medicinal products
- Aripiprazole, a substrate of CYP2D6 and CYP3A4: oral or injectable formulations of risperidone do not affect the pharmacokinetics of aripiprazole or its active metabolite dehydroaripiprazole.
Cardiac glycosides
- Risperidone has no clinically significant effect on the pharmacokinetics of digoxin.
Lithium
- Risperidone has no clinically significant effect on the pharmacokinetics of lithium.
Concomitant use of risperidone with furosemide.
See section "Special precautions for use" regarding increased mortality in elderly patients with dementia when used concomitantly with furosemide.
Special precautions for use.
In patients who have not previously been treated with risperidone, tolerance to the drug should be assessed by administering oral risperidone prior to initiating treatment with Risperdal Consta® (see section "Method of administration and dosage").
Elderly patients with dementia.
The use of Risperdal Consta® in elderly patients with dementia has not been studied and therefore is not recommended in this patient population. Risperdal Consta® is not indicated for the treatment of behavioral disorders associated with dementia.
Increased mortality in elderly patients with dementia.
Elderly patients with dementia treated with atypical antipsychotics have shown an increased mortality rate compared to placebo (based on meta-analysis of 17 placebo-controlled trials of atypical antipsychotics, including oral risperidone). In placebo-controlled trials of Risperdal® for oral use in this population, mortality rates were 4% in patients treated with Risperdal® compared to 3.1% in the placebo group. The odds ratio (95% confidence interval) was 1.21 (0.7; 2.1). The mean age of patients who died was 86 years (range: 67–100 years). Data from two substantial observational studies indicate that elderly patients with dementia treated with conventional antipsychotics also have a slightly increased risk of fatal outcomes compared to untreated patients. Data are insufficient to precisely quantify the risk, and the cause of the increased mortality risk is unknown. The extent to which the increased mortality risk is associated with antipsychotic use, as opposed to patient characteristics, remains unclear.
Concomitant use with furosemide.
In a placebo-controlled trial in elderly patients with dementia, an increased mortality rate was observed with concomitant use of furosemide and risperidone (7.3%, mean age 89 years, range: 75–97 years) compared to patients treated only with risperidone (3.1%, mean age 84 years, range: 70–96 years) or only with furosemide (4.1%, mean age 80 years, range: 67–96 years). Increased mortality in patients treated with both furosemide and risperidone was observed in two out of four clinical trials. Concomitant use of risperidone with other diuretics (mainly thiazide diuretics at low doses) was not associated with similar outcomes.
The pathophysiological mechanisms underlying this observation have not been established. However, caution should be exercised when prescribing the drug in such cases. No increase in mortality has been observed in patients who concurrently used other diuretics with risperidone. Regardless of treatment, dehydration was a common risk factor for mortality and should be carefully monitored in patients with dementia.
Cerebrovascular adverse reactions.
In randomized, placebo-controlled clinical trials, patients with dementia treated with certain atypical antipsychotics showed approximately a threefold increased risk of cerebrovascular adverse events. Pooled data from six placebo-controlled trials using risperidone, primarily in elderly patients (age >65 years) with dementia, showed cerebrovascular adverse events (serious and non-serious, combined) in 3.3% (30 out of 1009) of patients treated with risperidone and in 1.2% (8 out of 712) of those receiving placebo. The odds ratio (95% confidence interval) was 2.96 (1.34; 7.50). The mechanism of this increased risk is unknown.
An increased risk cannot be excluded when treating other patient populations or with other antipsychotics. Risperdal Consta® should be used with caution in patients at increased risk of stroke.
Orthostatic hypotension.
Since Risperdal Consta® is an α-blocker, orthostatic hypotension may occur, particularly at the beginning of treatment. Clinically significant hypotension has been reported during the post-marketing period with concomitant use of risperidone and antihypertensive agents. Risperidone should be used with caution in patients with cardiovascular disorders (such as heart failure, myocardial infarction, conduction abnormalities, dehydration, hypovolemia, or cerebrovascular disorders). If clinically significant hypotension persists, the risk-benefit ratio of continuing treatment with Risperdal Consta® should be re-evaluated.
Leukopenia, neutropenia, and agranulocytosis.
Cases of leukopenia, neutropenia, and agranulocytosis have been reported during treatment with antipsychotics (including Risperdal Consta®). During the post-marketing period, cases of agranulocytosis were reported very rarely (<1/10,000 patients).
Patients with a history of clinically significant leukopenia or drug-induced leukopenia/neutropenia should be monitored during the first few months of risperidone treatment. Therapy should be discontinued at the first signs of leukopenia in the absence of other causative factors.
Patients with clinically significant neutropenia should be carefully monitored for symptoms of fever or other signs of infection, and treatment should be initiated if such symptoms occur. Patients with severe neutropenia (absolute neutrophil count <1*109/L) should discontinue risperidone therapy and have leukocyte counts monitored until normalization.
Tardive dyskinesia/extrapyramidal symptoms.
Tardive dyskinesia, characterized by involuntary rhythmic movements (predominantly of the tongue and/or face), has been observed with drugs possessing dopamine receptor antagonist properties. The occurrence of extrapyramidal symptoms is a risk factor for tardive dyskinesia. If symptoms of tardive dyskinesia occur, discontinuation of all antipsychotics should be considered.
Caution is advised when risperidone is used concomitantly with psychostimulants (e.g., methylphenidate), as extrapyramidal symptoms may occur when adjusting the dose of either or both agents. Gradual discontinuation of psychostimulants is recommended (see section "Interaction with other medicinal products and other forms of interaction").
Neuroleptic malignant syndrome.
Cases of neuroleptic malignant syndrome have been reported with antipsychotics, characterized by hyperthermia, muscle rigidity, autonomic instability, altered consciousness, and elevated serum creatine phosphokinase levels. Additional symptoms may include myoglobinuria (rhabdomyolysis) and acute renal failure. If neuroleptic malignant syndrome develops, all antipsychotics, including Risperdal Consta®, should be discontinued.
Parkinson's disease and dementia with Lewy bodies.
Physicians should carefully weigh the risks and benefits when prescribing antipsychotics, including Risperdal Consta®, to patients with Parkinson's disease or dementia with Lewy bodies. Risperidone use may worsen the course of Parkinson's disease. Patients with either of these conditions may have an increased risk of neuroleptic malignant syndrome and heightened sensitivity to antipsychotics; such patients were excluded from clinical trials. In addition to extrapyramidal symptoms, manifestations of this heightened sensitivity may include confusion, reduced pain sensitivity, and postural instability with frequent falls.
Hypersensitivity reactions.
Although tolerance to oral risperidone should be established before initiating Risperdal Consta®, rare cases of anaphylactic reactions have been reported during the post-marketing period in patients who previously tolerated oral risperidone well (see sections "Method of administration and dosage" and "Adverse reactions"). If hypersensitivity reactions occur, treatment with Risperdal Consta® should be discontinued, and appropriate supportive measures and monitoring should be provided until symptoms resolve (see sections "Contraindications" and "Adverse reactions").
Hyperglycemia and diabetes mellitus.
Hyperglycemia, diabetes mellitus, or exacerbation of pre-existing diabetes have been reported during treatment with Risperdal Consta®. In some cases, prior weight gain was reported, which may be a risk factor. Diabetic ketoacidosis has been reported very rarely, and diabetic coma rarely. Appropriate clinical monitoring should be performed according to recommendations for antipsychotic use. Patients treated with atypical antipsychotics, including Risperdal Consta®, should be monitored for symptoms of hyperglycemia (e.g., polydipsia, polyuria, polyphagia, weakness), and diabetic patients should be monitored for worsening glycemic control.
Weight gain.
Significant weight gain has been reported with Risperdal Consta®. Patient weight should be monitored regularly.
Hyperprolactinemia.
Hyperprolactinemia is a commonly observed adverse reaction during treatment with Risperdal Consta®. In patients with signs of prolactin-dependent adverse effects (gynecomastia, menstrual disorders, anovulation, impaired fertility, decreased libido, erectile dysfunction, galactorrhea), plasma prolactin levels should be assessed.
Tissue culture studies suggest that prolactin may stimulate growth of human breast tumor cells. Although a clear association with antipsychotic use has not yet been demonstrated in clinical and epidemiological studies, caution is advised in patients with relevant medical history. Risperdal Consta® should be used cautiously in patients with existing hyperprolactinemia or those with suspected prolactin-dependent tumors.
QT interval prolongation.
QT interval prolongation has been very rarely observed during the post-marketing period. As with other antipsychotics, caution is advised when administering Risperdal Consta® to patients with cardiovascular disorders, family history of QT prolongation, bradycardia, or electrolyte imbalances (hypokalemia, hypomagnesemia), as these may increase the risk of arrhythmogenic effects, and when used concomitantly with drugs that prolong the QT interval.
Seizures.
Risperdal Consta® should be used with caution in patients with a history of seizures or other conditions that may lower the seizure threshold.
Priapism.
Priapism may occur during treatment with Risperdal Consta® due to its alpha-adrenergic blocking effects.
Body temperature regulation.
Impaired thermoregulation is a known effect of antipsychotic drugs. Appropriate monitoring is recommended when prescribing Risperdal Consta® to patients who may experience elevated body temperature due to strenuous physical activity, excessive heat exposure, concomitant anticholinergic therapy, or dehydration.
Venous thromboembolism.
Cases of venous thromboembolism have been reported with antipsychotic use. Since patients treated with antipsychotics often have an increased risk of venous thromboembolism, all potential risk factors should be evaluated before and during treatment with Risperdal Consta®, and preventive measures should be taken.
Intraoperative floppy iris syndrome (IFIS).
Intraoperative floppy iris syndrome has been observed during cataract surgery in patients treated with α1-adrenergic receptor antagonists, including Risperdal Consta® (see section "Adverse reactions").
IFIS may increase the risk of ocular complications during and after surgery. Ophthalmic surgeons should be informed about current or past use of this class of drugs. The potential benefits of discontinuing α1-blocking agents prior to surgery have not been established, and the risk of discontinuing antipsychotic therapy should be carefully considered.
Anti-emetic effect.
Anti-emetic effects were observed in preclinical trials of risperidone. In humans, such an effect may mask symptoms of drug overdose, intestinal obstruction, Reye’s syndrome, or brain tumors.
Renal and hepatic impairment.
Risperdal Consta® has not been studied in patients with renal or hepatic impairment. Risperdal Consta® should be used with caution in these patient groups (see section "Method of administration and dosage").
Administration.
Care must be taken to avoid accidental intravascular injection of Risperdal Consta®.
Excipients.
This medicinal product contains less than 1 mmol sodium (23 mg) per dose, i.e., it is considered "sodium-free."
Use during pregnancy or breastfeeding.
Pregnancy
There are no data on the safety of risperidone use in pregnant women.
Risperidone did not show teratogenic toxicity in animal studies, but other forms of reproductive toxicity were observed. The potential risk in humans is unknown.
Use of risperidone (including Risperdal Consta®) during the third trimester of pregnancy is associated with an increased risk of adverse reactions in newborns, including reversible extrapyramidal symptoms and/or withdrawal syndrome. These symptoms vary in severity and duration and may include agitation, hypertonia, hypotonia, tremor, somnolence, respiratory distress syndrome, or gastrointestinal disturbances. Therefore, newborns should be closely monitored.
Risperdal Consta® should not be used during pregnancy unless absolutely necessary.
Breastfeeding
In animal studies, risperidone and 9-hydroxyrisperidone were excreted in breast milk. Observations suggest that risperidone and 9-hydroxyrisperidone may also pass into human breast milk in small amounts. Data on adverse effects in breastfed infants are lacking. Therefore, the benefits of breastfeeding should be weighed against the potential risks to the infant.
Fertility
Like other dopamine D2-receptor antagonists, Risperdal Consta® increases prolactin levels. Hyperprolactinemia may suppress hypothalamic gonadotropin-releasing hormone, leading to reduced pituitary gonadotropin secretion. This, in turn, suppresses reproductive function due to impaired gonadal steroidogenesis in both women and men.
No significant effects were observed in preclinical studies.
Ability to affect reaction speed when driving or operating machinery.
Risperdal Consta® has a negligible or moderate effect on reaction speed when driving or operating machinery, due to central nervous system and visual effects (see section "Adverse reactions"). Patients are advised to refrain from driving or operating machinery until their individual response to the drug is known.
Method of Administration and Dosage.
Adults.
Initial dose. The recommended dose for most patients is 25 mg administered intramuscularly once every two weeks. For patients who have been receiving a fixed dose of oral risperidone for two weeks or longer, the transition scheme indicated below is recommended. Patients receiving oral risperidone doses of 4 mg or less should be administered 25 mg of Risperdal Consta®. Patients receiving higher oral risperidone doses should be administered a higher dose of Risperdal Consta® – 37.5 mg.
For patients not currently taking oral risperidone, prior oral antipsychotic dosing should be considered when selecting the initial intramuscular dose. The recommended starting dose is 25 mg of Risperdal Consta® every two weeks. Patients receiving higher doses of oral antipsychotics should be administered a higher dose of Risperdal Consta® – 37.5 mg.
Adequate antipsychotic effect from prior oral risperidone or previous antipsychotic treatment must be maintained throughout the three-week lag period following the first injection of Risperdal Consta® (see section “Pharmacokinetics”).
Risperdal Consta® should not be used in acute exacerbations of schizophrenia without ensuring adequate antipsychotic effect from oral risperidone or prior antipsychotic treatment during the three-week lag period following the first injection of Risperdal Consta®.
Maintenance dose. The recommended dose for most patients is 25 mg administered intramuscularly once every two weeks. Some patients may require higher doses – 37.5 or 50 mg. The dose may be increased no more frequently than once every 4 weeks. The effect of dose escalation should not be expected earlier than 3 weeks after the first injection of the increased dose. No additional benefits were observed with the 75 mg dose in clinical studies. The maximum dose should not exceed 50 mg once every two weeks.
Elderly patients.
Dose adjustment is not required. The recommended dose is 25 mg administered intramuscularly once every two weeks. For patients not currently taking oral risperidone, the recommended starting dose is 25 mg of Risperdal Consta® every two weeks. For patients who have been receiving a fixed oral risperidone dose for two weeks or longer, the transition scheme indicated below is recommended. Patients receiving oral risperidone doses of 4 mg or less should be administered 25 mg of Risperdal Consta®. Patients receiving higher oral risperidone doses should be administered a higher dose of Risperdal Consta® – 37.5 mg.
Adequate antipsychotic effect must be maintained throughout the three-week lag period following the first injection of Risperdal Consta® (see section “Pharmacokinetics”). Clinical data on the use of Risperdal Consta® in elderly patients are limited. Risperdal Consta® should be used with caution in elderly patients.
Patients with hepatic or renal impairment.
The use of Risperdal Consta® in patients with hepatic or renal impairment has not been studied.
For patients with hepatic or renal insufficiency requiring treatment with Risperdal Consta®, the initial dose should be 0.5 mg of oral risperidone twice daily for one week. During the second week, the patient may receive 1 mg twice daily or 2 mg once daily. If the patient tolerates an oral daily dose of at least 2 mg, they may then receive 25 mg of Risperdal Consta® intramuscularly once every two weeks.
Adequate antipsychotic effect must be maintained throughout the three-week lag period following the first injection of Risperdal Consta® (see section “Pharmacokinetics”).
Method of administration.
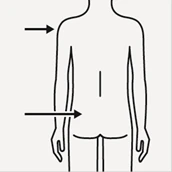
Risperdal Consta® should be administered once every two weeks by deep intramuscular injection into the deltoid or gluteal muscle, using the sterile needle of appropriate length provided with the pre-filled syringe. For deltoid injection, use a 25 mm needle, alternating injection sites between the right and left sides. For gluteal injection, use a 51 mm needle, alternating injection sites between the right and left buttocks. The drug must not be administered intravenously.
For information on the preparation and administration of the solution, see the section “Instructions for Use of the West Needle-Free Device System”.
Children.
Risperdal Consta® is not recommended for use in children due to insufficient data on safety and efficacy.
Instructions for Use of the West Needle-Free Device System
Warning!
To ensure successful administration of Risperdal Consta®, carefully read the instructions below.
Use only the components of the Risperdal Consta**®** packaging to prepare the long-acting injectable suspension. Only the solvent provided in the pre-filled syringe should be used to reconstitute the powder. Do not substitute any components of the packaging with other products.
The suspension should not be stored after preparation. The medicinal product should be administered immediately after reconstitution to prevent microbiological contamination.
To ensure the full dose of risperidone is administered, the entire contents of the vial must be injected.
The prepared suspension should be administered intramuscularly only using the safe needles provided in the packaging (51 mm needle for gluteal injection and 25 mm needle for deltoid injection).
The components of the packaging are intended for single use only. Any attempt to prepare the packaging components for subsequent reuse may adversely affect the integrity of the devices or lead to reduced performance.
Packaging Components

Before preparing the suspension, remove the Risperdal Consta**®** packaging from the refrigerator and allow it to warm to room temperature for at least 30 minutes. Do not heat the kit by any other method.
- Remove the colored plastic cap from the vial. Wipe the gray rubber stopper with alcohol, without removing it, and wait for it to dry. Do not remove the gray rubber stopper.

- Prepare the needle-free device for use. Open the blister pack. Do not remove the needle-free device.
Under no circumstances should the sharp tip of the device be touched.
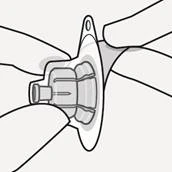
- It is very important to correctly position the West needle-free device system on the vial to prevent leakage when the solvent is introduced into the vial.
Place the vial on a firm surface. Holding the vial with one hand, position the needle-free device so that its spike is aligned with the center of the vial’s rubber stopper. Press the spike of the device downward onto the center of the rubber stopper until the device’s “skirt” securely locks onto the neck of the vial.

- Remove the blister from the needle-free device only when the patient is ready to break off the white cap from the syringe. While holding the vial vertically to prevent leakage, remove the blister. Do not shake the vial and do not touch the Luer cannula of the needle-free device to prevent contamination.
**
**
- During all manipulations with the syringe, hold it only by the white collar located at the end. Holding the syringe by the white collar prevents disconnection and ensures a secure connection.

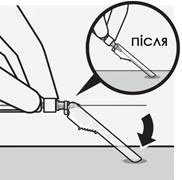
- Open the syringe by breaking off the white cap at its connection point with the syringe (do not twist or cut the white cap), and remove the cap together with the rubber tip inside it. Do not touch the tip of the syringe to prevent contamination.
Do not apply excessive pressure to the syringe parts during manipulations to prevent their disconnection from the syringe body.


- Holding the syringe by the white collar with one hand, insert the syringe tip into the Luer cannula of the needle-free device, press and turn it clockwise to secure the connection between the syringe and the needle-free device. Firmly hold the device by the “skirt” to prevent rotation during connection.
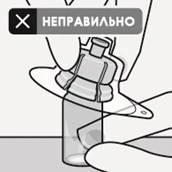
Do not hold the syringe by the barrel, as this may disrupt the connection of the white collar with the needle-free device or cause disconnection.
**

**
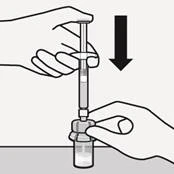
- Inject the entire contents of the syringe (solvent) into the vial. The vial contents will now be under pressure; therefore, hold the plunger in the lower position using the thumb of your hand.
**
**
- While keeping the syringe plunger locked in the lower position, vigorously shake the vial contents for at least 10 seconds until a homogeneous suspension is formed. A properly prepared suspension should be homogeneous, thick, and milky in appearance. The powder microspheres will be visible in the final suspension.
Proceed immediately to the next step to prevent sedimentation of microparticles.

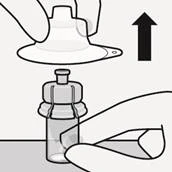
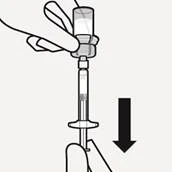
- Invert the vial upside down and slowly draw the vial contents into the syringe.
**
**
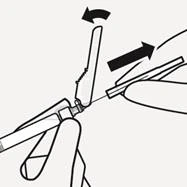
- Holding the syringe by the white collar with one hand, disconnect the syringe from the device by turning it counterclockwise. Discard the vial and the needle-free device.
**

**
- Select the appropriate needle depending on the injection site (gluteal or deltoid muscle).
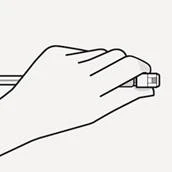
Partially open the packaging, holding the needle by the base as shown in the figure.
To prevent contamination, do not touch the protective needle sheath. Holding the syringe by the white collar with one hand, attach the needle’s Luer cannula to the syringe tip, slightly turning it clockwise.


- Immediately before administration, resuspend Risperdal Consta® as microgranules may settle in the vial after suspension preparation. To resuspend the microgranules, vigorously shake the syringe.
- Holding the syringe by the white collar with one hand, remove the protective needle sheath as shown in the figure and carefully remove the transparent needle cap without rotating it.
- Gently tap the syringe with your finger to bring air bubbles to the top. Expel air bubbles from the syringe and needle by holding the syringe vertically with the needle pointing upward and slightly advancing the plunger.
**

**
- Immediately inject the entire contents of the syringe into the patient’s gluteal or deltoid muscle. Do not administer intravenously.
- After injection, place the needle into the protective sheath. Carefully press the protective sheath with one hand onto a flat surface at a 45° angle so that the needle fully enters the sheath. Visually confirm that the needle is securely fixed within the protective sheath and immediately discard it.
Do not reuse any components of the Risperdal Consta® packaging kit.
THE SUSPENSION MUST NOT BE ADMINISTERED INTRAVENOUSLY!
Warning: To prevent injury to healthcare personnel from contaminated needles, follow these safety precautions:
- Do not touch the protective sheath while placing it over the needle after injection;
- Do not detach the needle safety guard;
- Do not attempt to straighten the needle or place the protective sheath if the needle is bent or damaged;
- Handle the needle protective sheath carefully and ensure the needle tip does not protrude from the sheath.
Overdose.
Overdose is less likely with parenteral formulations of Risperdal Consta® than with oral formulations; therefore, the information below pertains to oral formulations.
Symptoms.
Mainly observed signs and symptoms associated with increased known pharmacological effects of risperidone. These include somnolence and sedation, tachycardia and arterial hypotension, extrapyramidal symptoms. Cases of QT interval prolongation and seizures have been reported in overdose. Atrial flutter was observed in combined overdose of oral risperidone and paroxetine.
In cases of acute overdose, consider the possibility of concomitant use of other drugs.
Treatment.
Ensure and maintain airway patency for adequate ventilation and oxygenation. Cardiac and cardiovascular function should be monitored, including continuous ECG monitoring to detect possible arrhythmias.
Risperdal® has no specific antidote; therefore, appropriate supportive measures should be taken. For arterial hypotension and circulatory collapse, appropriate measures such as intravenous fluid administration and/or sympathomimetics should be used. In case of severe extrapyramidal symptoms, anticholinergic drugs should be administered. Continuous medical supervision and monitoring should be maintained until signs of overdose have resolved.
Adverse Reactions
The most frequently observed adverse reactions (frequency ≥ 1/10) were insomnia, anxiety, headache, upper respiratory tract infections, parkinsonism, and depression. Dose-dependent adverse reactions included parkinsonism and akathisia.
During the post-marketing period, serious local injection site reactions such as injection site necrosis, abscess, cellulitis, ulceration, hematoma, cyst, and induration have been reported. The frequency is classified as unknown (cannot be estimated from available data). Some cases required surgical intervention.
All adverse reactions listed below were observed during clinical trials and in the post-marketing period. The following frequency classification was used: very common (≥ 1/10), common (≥ 1/100 to < 1/10), uncommon (≥ 1/1000 to < 1/100), rare (≥ 1/10,000 to < 1/1000), very rare (< 1/10,000). Within each frequency group, adverse effects are listed in decreasing order of severity.
Infections and infestations:
Very common – upper respiratory tract infections;
Common – pneumonia, bronchitis, sinusitis, urinary tract infections, influenza;
Uncommon – respiratory tract infections, cystitis, ear infections, eye infections, tonsillitis, onychomycosis, cellulitis, infections, localized infections, viral infections, acarodermatitis, subcutaneous abscess.
Blood and lymphatic system disorders:
Common – anemia;
Uncommon – decreased leukocyte count, thrombocytopenia, decreased hematocrit;
Rare – agranulocytosis, neutropenia, increased eosinophils.
Immune system disorders:
Uncommon – hypersensitivity;
Rare – anaphylactic reactions.
Endocrine disorders:
Common – hyperprolactinemia;
Uncommon – presence of glucose in urine;
Rare – inappropriate antidiuretic hormone secretion.
Metabolism and nutrition disorders:
Common – hyperglycemia, weight gain, increased appetite, weight loss, decreased appetite;
Uncommon – diabetes mellitusb, anorexia, increased blood triglycerides, increased blood cholesterol;
Rare – water intoxication, hypoglycemia, hyperinsulinemia, polydipsia;
Very rare – diabetic ketoacidosis.
Psychiatric disorders:
Very common – insomniab, depression, anxiety;
Common – sleep disorders, agitation, decreased libido;
Uncommon – mania, confusion, anorgasmia, restlessness, night terrors;
Rare – catatonia, sleepwalking, sleep-related eating disorder, emotional blunting.
Nervous system disorders:
Very common – parkinsonismd, headache;
Common – sedation/somnolence, akathisiad, dystoniad, dizziness, dyskinesiad, tremor;
Uncommon – tardive dyskinesia, cerebral ischemia, loss of consciousness, seizuresd, syncope, psychomotor hyperactivity, balance disorder, coordination disorder, postural dizziness, attention disturbance, dysarthria, dysgeusia, hypoesthesia, paresthesia;
Rare – neuroleptic malignant syndrome, cerebrovascular disorders, unresponsiveness, decreased level of consciousness, diabetic coma, rhythmic head bobbing.
Eye disorders:
Common – blurred vision;
Uncommon – conjunctivitis, dry eyes, increased lacrimation, ocular hyperemia;
Rare – central retinal artery occlusion, glaucoma, eye movement disorders, eye rolling, photophobia, eyelid margin crusting, intraoperative floppy iris syndrome.
Ear and labyrinth disorders:
Uncommon – vertigo, tinnitus, ear pain.
Cardiac disorders:
Common – tachycardia;
Uncommon – atrial fibrillation, atrioventricular block, cardiac conduction disorders, QT interval prolongation on electrocardiogram, bradycardia, electrocardiogram abnormalities, palpitations;
Rare – sinus arrhythmia.
Vascular disorders:
Common – arterial hypotension, arterial hypertension;
Uncommon – orthostatic hypotension;
Rare – pulmonary embolism, deep vein thrombosis, flushing.
Respiratory, thoracic and mediastinal disorders:
Common – dyspnea, pharyngolaryngeal pain, cough, nasal congestion;
Uncommon – pulmonary hyperventilation, worsening airway patency, wheezing, epistaxis;
Rare – sleep apnea syndrome, aspiration pneumonia, pulmonary congestion, rales, dysphonia, respiratory tract disorders.
Gastrointestinal disorders:
Common – abdominal pain, stomach discomfort, vomiting, nausea, constipation, gastroenteritis, diarrhea, dyspepsia, dry mouth, toothache;
Uncommon – fecal incontinence, dysphagia, flatulence;
Rare – pancreatitis, intestinal obstruction, tongue swelling, fecaloma, cheilitis;
Very rare – intestinal obstruction.
Skin and subcutaneous tissue disorders:
Common – rash;
Uncommon – pruritus, alopecia, eczema, dry skin, erythema, skin discoloration, acne, seborrheic dermatitis;
Rare – drug eruption, urticaria, hyperkeratosis, dandruff, skin disorders, skin injury;
Very rare – angioedema.
Musculoskeletal and connective tissue disorders:
Common – muscle spasms, musculoskeletal pain, back pain, arthralgia;
Uncommon – increased blood creatine phosphokinase, joint stiffness, joint swelling, muscle weakness, neck pain;
Rare – rhabdomyolysis, abnormal posture.
Renal and urinary disorders:
Common – urinary incontinence;
Uncommon – polyuria, urinary retention, dysuria.
Pregnancy and neonatal disorders:
Rare – drug withdrawal syndrome in newbornsc.
Reproductive system and breast disorders:
Common – erectile dysfunction, amenorrhea, galactorrhea;
Uncommon – ejaculation disorder, menstrual delay, menstrual cycle disordersd, gynecomastia, sexual dysfunction, breast pain, breast discomfort, vaginal discharge;
Rare – priapismc, breast engorgement, breast enlargement, breast discharge.
General disorders and administration site conditions:
Common – edemad, pyrexia, chest pain, asthenia, fatigue, pain, injection site reactions;
Uncommon – facial swelling, chills, increased body temperature, gait disturbance, thirst, chest discomfort, fever, unusual sensations, indurationc at injection site;
Rare – hypothermia, decreased body temperature, peripheral coldness, drug withdrawal syndrome, discomfort.
Hepatobiliary disorders:
Common – increased transaminases, increased gamma-glutamyl transferase;
Uncommon – increased liver enzymes;
Rare – jaundice.
Injury, poisoning and procedural complications:
Common – falls;
Uncommon – procedural pain.
a Hyperprolactinemia may in some cases lead to gynecomastia, menstrual disorders, amenorrhea, anovulation, galactorrhea, fertility disorders, decreased libido, and erectile dysfunction.
b In a placebo-controlled study, diabetes mellitus was reported in 0.18% of patients treated with risperidone compared to 0.11% in the placebo group. The overall incidence across all clinical trials was 0.43% in patients receiving risperidone.
c Not observed during clinical trials of Risperdal Consta®, but reported in the post-marketing period with risperidone use.
d Extrapyramidal symptoms may include: parkinsonism (hypersalivation, muscle and joint stiffness, parkinsonism, drooling, cogwheel phenomenon, bradykinesia, hypokinesia, mask-like face, muscle tension, akinesia, nuchal rigidity, muscle rigidity, parkinsonian gait, and impaired glabellar reflex); akathisia (akathisia, restlessness, hyperkinesia, restless legs syndrome); tremor; dyskinesia (dyskinesia, muscle twitching, choreoathetosis, athetosis, myoclonus); dystonia. Dystonia includes dystonia, hypertonia, torticollis, involuntary muscle contractions, muscle contractures, blepharospasm, eye movement disorders, tongue paralysis, facial spasms, laryngospasm, myotonia, opisthotonus, oropharyngeal spasm, pleurotonus, tongue spasm, and trismus. A broader range of symptoms is included, not necessarily of extrapyramidal origin. Insomnia includes difficulty falling asleep and intrasomnic disorders; seizures include generalized tonic-clonic seizures; menstrual disorders include irregular menstruation and oligomenorrhea; edema includes generalized edema, peripheral edema, and soft tissue swelling.
Adverse reactions with paliperidone
Paliperidone is the active metabolite of risperidone; therefore, the adverse reaction profiles of both drugs (oral and injectable forms) are comparable. The adverse reactions listed below were observed with paliperidone and may be expected with Risperdal Consta®.
Cardiac disorders: postural orthostatic tachycardia syndrome.
Anaphylactic reactions
In the post-marketing period, very rare cases of anaphylactic reactions have been reported after Risperdal Consta® injection in patients who previously tolerated oral risperidone well.
Adverse reactions typical of this class of drugs
As with other antipsychotics, QT interval prolongation has been very rarely observed in the post-marketing period with risperidone. Other cardiac adverse effects associated with antipsychotics that prolong the QT interval include ventricular arrhythmia, ventricular fibrillation, ventricular tachycardia, sudden cardiac death, cardiac arrest, and flutter/fibrillation.
Venous thromboembolism. Cases of venous thromboembolism, including pulmonary embolism and deep vein thrombosis (frequency unknown), have been reported with antipsychotic drugs.
Weight gain. In 12-week double-blind, placebo-controlled studies, 9% of patients treated with Risperdal Consta® gained ≥ 7% of their baseline body weight, compared to 6% of placebo-treated patients. In one-year open-label studies with Risperdal Consta®, individual body weight changes were within ± 7% of baseline; 25% of patients gained ≥ 7% of their baseline body weight.
Shelf life. 3 years.
Storage conditions.
The medicinal product should be stored at 2–8 °C (in a refrigerator) for 3 years, protected from light. Storage above 25 °C is not recommended. In the absence of a refrigerator, the product may be stored for up to 7 days at temperatures not exceeding 25 °C. Keep out of reach of children.
The stability of the prepared suspension for administration is maintained for 24 hours at temperatures not exceeding 25 °C. Due to the risk of microbial contamination, the suspension should be used immediately after preparation. The prepared suspension may be stored for up to 6 hours at temperatures not exceeding 25 °C, except when the suspension is prepared under aseptic conditions.
Incompatibilities. Data not available.
Packaging.
One kit contains:
one vial of powder, one syringe with 2 mL diluent, one West non-needle device for suspension preparation, and two needles (25 mm and 51 mm in length, each with protective devices) for intramuscular injections; one kit per cardboard box.
Prescription status. Prescription only.
Manufacturer.
Responsible for batch release:
Sílag AG / Cilag AG.
Manufacturer's address.
Hochstrasse 201, 8200 Schaffhausen, Switzerland.