Pulmicort turbuhaler
Ukraine
Table of Contents
INSTRUCTIONS FOR MEDICAL USE OF THE MEDICINAL PRODUCT PULMICORT TURBUHALER (Pulmicort® Turbuhaler®)
Composition:
Active substance: budesonide;
1 dose (inhalation) contains 100 mcg or 200 mcg of budesonide.
Pharmaceutical form. Powder for inhalation.
Main physicochemical properties:
100 mcg/dose:
A specially designed powder inhaler made of plastic materials. The rotating dose indicator is light-brown in color. On the base of the rotating dose indicator, "Budesonide 100" is embossed. Contents: round granules from white to almost white, which disintegrate into a fine powder under slight pressure. Powder fraction may be present.
200 mcg/dose:
A specially designed powder inhaler made of plastic materials. The rotating dose indicator is brown in color. On the base of the rotating dose indicator, "Budesonide 200" is embossed. Contents: round granules from white to almost white, which disintegrate into a fine powder under slight pressure. Powder fraction may be present.
Pharmacotherapeutic group. Inhalation agents used in the treatment of obstructive airway diseases. Glucocorticoids. ATC code R03BA02.
Pharmacological properties.
Pharmacodynamics.
Budesonide is a glucocorticosteroid with potent local anti-inflammatory action.
The precise mechanism of action of glucocorticosteroids in the treatment of asthma has not been fully elucidated. The main effects are anti-inflammatory, including suppression of inflammatory mediator release and inhibition of cytokine-mediated immune responses. Budesonide exhibits activity due to its affinity for glucocorticosteroid receptors, which is approximately 15 times greater than that of prednisolone.
Budesonide exerts anti-inflammatory effects that reduce bronchial obstruction in both the early and late phases of the allergic reaction. Budesonide reduces the responsiveness to histamine and methacholine in patients with airway hyperresponsiveness.
Studies have shown that the earlier budesonide treatment is initiated after the onset of asthma symptoms, the greater the improvement in lung function can be expected.
In patients with mild to moderate COPD, Pulmicort Turbuhaler at a dose of 400 mcg twice daily, compared to placebo, led to an improvement in forced expiratory volume in one second (FEV1) after 3–6 months of treatment. This effect was maintained over three years of therapy.
Studies on the use of Pulmicort Turbuhaler in healthy volunteers demonstrated a dose-dependent effect on plasma and urinary cortisol. When used at recommended doses, Pulmicort Turbuhaler has a significantly lower effect on adrenal function than prednisone 10 mg, as demonstrated by ACTH stimulation tests.
In children aged 5 years and older, no systemic effects were observed with doses up to 400 mcg daily. At doses of 400–800 mcg daily, biochemical signs of systemic effects may occur, while such signs are common at daily doses exceeding 800 mcg.
Bronchial asthma itself, as well as the use of inhaled corticosteroids, may lead to growth retardation. However, long-term studies in children treated with budesonide (up to 13 years) have shown that patients reach the expected adult height. In most cases, a slight growth delay (approximately 1 cm) was observed during the first year of treatment. Inhaled budesonide therapy is effective in preventing exercise-induced asthma.
Pharmacokinetics.
Absorption
Inhaled budesonide is rapidly absorbed. Peak plasma concentrations are reached within 30 minutes after inhalation. In studies, the average lung deposition of budesonide after inhalation via Turbuhaler was 25–35% of the administered dose. Systemic bioavailability is approximately 38%.
Distribution and metabolism
Plasma protein binding is approximately 90%. The volume of distribution is approximately 3 L/kg.
Budesonide undergoes extensive (approximately 90%) first-pass metabolism in the liver to metabolites with low glucocorticosteroid activity. The glucocorticosteroid activity of the main metabolites, 6-beta-hydroxybudesonide and 16-alpha-hydroxyprednisolone, is less than 1% of that of budesonide.
Elimination
Budesonide is eliminated via metabolism, primarily catalyzed by the CYP3A4 enzyme. Metabolites are excreted in urine in unchanged or conjugated forms. Only a small amount of unchanged budesonide is detected in urine. Budesonide has a high systemic clearance (approximately 1.2 L/min), and its plasma half-life after intravenous administration averages 4 hours. The pharmacokinetics of budesonide are dose-proportional over the therapeutic dose range.
The pharmacokinetics of budesonide in children and in patients with renal impairment have not been established. The effect of budesonide may be increased in patients with hepatic disease.
Clinical characteristics.
Indications.
- Persistent bronchial asthma requiring treatment with inhaled glucocorticoids.
- Treatment of moderate to severe chronic obstructive pulmonary disease (COPD).
Contraindications.
Hypersensitivity to budesonide.
Interaction with other medicinal products and other types of interactions.
Pulmicort Turbuhaler may enhance the effect of inhaled beta-2 sympathomimetics. Budesonide metabolism is primarily mediated by the CYP3A4 enzyme, belonging to the cytochrome P450 enzyme subfamily. Therefore, concomitant use of inhibitors of this enzyme, such as ketoconazole, itraconazole, clotrimazole, ritonavir, cyclosporine, ethinylestradiol, troleandomycin, and HIV protease inhibitors, may lead to several-fold increases in systemic exposure to budesonide (see section "Special precautions for use"). Since data on dosage recommendations for these combinations are lacking, such combinations should be avoided. If avoidance is not possible, the interval between administration of the drugs should be as long as possible. A reduction in the dose of budesonide may also be considered.
Limited data on these interactions with high doses of inhaled budesonide indicate that significant increases in plasma levels (on average 4-fold) may occur when itraconazole 200 mg once daily is co-administered with inhaled budesonide (single dose 1000 µg). In vivo studies have shown that oral administration of ketoconazole and itraconazole may increase systemic concentrations of budesonide. This has minimal clinical significance for short-term treatment (1–2 weeks), but should be considered during prolonged therapy.
Concomitant administration of cimetidine and budesonide may lead to a slight increase in plasma budesonide levels; however, this is not clinically significant.
Increased plasma concentrations and enhanced effects of corticosteroids have been observed in women receiving estrogens or oral contraceptives. However, no significant changes have been noted with concomitant use of budesonide and low-dose combined oral contraceptives.
Since adrenal function may be suppressed, an ACTH stimulation test, intended for diagnosis of pituitary insufficiency, may yield false results (low values).
Special precautions for use.
Exacerbations of COPD should be treated with additional medications according to the decision of the responsible physician.
Budesonide is not intended for the relief of acute asthma attacks when short-acting inhaled bronchodilators are required.
Transition from oral corticosteroids
Patients receiving systemic corticosteroid therapy should be switched to Pulmicort Turbuhaler once control of symptoms has been achieved. In patients with impaired adrenal function, systemic corticosteroids should be discontinued gradually, not abruptly. During the initial transition to Pulmicort Turbuhaler, systemic corticosteroids should be continued for approximately 1 week. Thereafter, the daily dose of systemic corticosteroids may be reduced by an amount equivalent to 2.5 mg of prednisone per 1–2 weeks, depending on the patient's response.
Particular caution is required when treating patients transitioning from oral corticosteroids, as they may remain at risk of adrenal insufficiency for a prolonged period. Patients requiring emergency high-dose corticosteroid therapy or long-term treatment with inhaled corticosteroids at the highest recommended dose may also be at risk. Such patients may develop symptoms of adrenal insufficiency during periods of severe stress. During stressful periods or planned surgical procedures, consideration should be given to additional systemic corticosteroid therapy.
If stressful or emergency situations (e.g., severe infections, trauma, surgery) occur within the first few months after switching from systemic corticosteroids to inhaled therapy, re-institution of systemic corticosteroids may be necessary.
Systemic effects of inhaled corticosteroids
Systemic effects of inhaled corticosteroids may occur, particularly when used at high doses over prolonged periods. These effects are considerably less likely than with oral corticosteroids. Potential systemic effects include Cushing's syndrome, Cushingoid features, adrenal suppression, growth retardation in children and adolescents, decreased bone mineral density, cataract, glaucoma, and, less commonly, a range of psychological and behavioral effects such as psychomotor hyperactivity, sleep disturbances, anxiety, depression, or aggression (particularly in children). Therefore, it is important that the dose of inhaled corticosteroid is reduced to the lowest dose at which effective control of asthma is maintained.
Effect on growth
In children and adolescents receiving long-term corticosteroid therapy, regardless of the formulation used, regular monitoring of growth is recommended. The benefits of corticosteroid therapy should be weighed against the potential risk of growth retardation. In addition, referral to a pediatric pulmonologist should be considered.
In cases of growth retardation and to minimize potential systemic effects, it is important to re-evaluate therapy to ensure that the dose of inhaled corticosteroid has been adjusted to the lowest effective dose required to maintain disease control.
Use in patients with hepatic impairment
Impaired liver function affects the ability to eliminate corticosteroids, resulting in reduced clearance and higher systemic exposure. The possibility of systemic adverse effects should be considered.
Concomitant use with other medicinal products
Concomitant use of the drug with ketoconazole, itraconazole, HIV protease inhibitors, or other potent CYP3A4 inhibitors should be avoided. If avoidance is not possible, the interval between administration of the drugs should be as long as possible (see section "Interaction with other medicinal products and other forms of interaction***").
Respiratory tract infections
Particular caution is required in patients with active pulmonary tuberculosis or latent tuberculosis, as well as in patients with fungal or viral respiratory tract infections.
Oropharyngeal candidiasis
Oropharyngeal candidiasis may develop during treatment with inhaled corticosteroids. To reduce the risk of developing candidiasis in the mouth and throat, Pulmicort Turbuhaler should be used before meals or the patient should rinse the mouth with water after each inhalation. If necessary, appropriate antifungal agents may be used, and some patients may require temporary discontinuation of Pulmicort Turbuhaler (see section "Dosage and administration").
Bronchospasm
As with other inhaled medications, paradoxical bronchospasm with wheezing may occur immediately after administration of the drug. In such cases, treatment with inhaled budesonide should be discontinued immediately, the patient's condition assessed, and alternative therapy initiated if necessary.
Patients should be advised to seek medical attention if overall effectiveness of treatment decreases, as repeated inhalations during severe asthma attacks should not delay initiation of other essential therapy. In case of sudden worsening of condition, treatment should be supplemented with short-term use of oral corticosteroids.
During transition from systemic corticosteroid therapy to Pulmicort Turbuhaler, patients may experience previous symptoms such as muscle and joint pain. In such cases, temporary increase in the dose of oral corticosteroids may be required. If (in individual cases) symptoms such as increased fatigue, headache, nausea, vomiting, or similar occur, steroid insufficiency should be suspected in most cases.
When replacing systemic corticosteroid therapy with Pulmicort Turbuhaler, allergies previously controlled by systemic therapy (e.g., rhinitis, eczema) may occasionally reappear.
Pneumonia in patients with COPD
In patients with chronic obstructive pulmonary disease (COPD) receiving inhaled corticosteroids, an increased incidence of pneumonia, including pneumonia requiring hospitalization, has been observed. There is some evidence of increased pneumonia risk with higher corticosteroid doses, although this has not been definitively demonstrated in any study.
There are no conclusive clinical data demonstrating differences between inhaled corticosteroids in the magnitude of pneumonia risk.
Physicians should remain vigilant for possible development of pneumonia in COPD patients, as clinical signs of such infections overlap with symptoms of COPD exacerbations.
Risk factors for pneumonia in COPD patients include smoking, advanced age, low body mass index (BMI), and severe COPD.
Visual disturbances
Visual disturbances have been reported with both systemic and local use of corticosteroids. If a patient experiences symptoms such as blurred vision or other visual disturbances, they should be referred to an ophthalmologist to determine the possible cause, which may include cataract, glaucoma, or rare conditions such as central serous chorioretinopathy, which has been reported after systemic and topical corticosteroid use.
Note.
Pulmicort Turbuhaler is not suitable for the treatment of acute asthma attacks.
Information for patients not previously treated with corticosteroids.
In patients who have not previously received corticosteroid therapy or have only received short-term intermittent treatment, improvement in breathing may be observed approximately 1 week after regular use of Pulmicort Turbuhaler as prescribed by a physician. However, severe edema and inflammatory changes may cause such bronchial obstruction that budesonide may not be fully effective with local administration.
In such cases, therapy should be initiated with the addition of systemic corticosteroids (initially at a dose equivalent to 40–60 mg prednisone daily). Inhaled therapy should be continued during gradual tapering of systemic corticosteroids.
Worsening of symptoms during acute respiratory infections.
In case of worsening symptoms during acute respiratory infections, the possibility of prescribing appropriate antibiotics should be considered. If necessary, the dose of Pulmicort Turbuhaler may be adjusted, and systemic glucocorticoids may be indicated under certain circumstances.
Use of Pulmicort Turbuhaler may lead to positive doping test results.
Use during pregnancy or breastfeeding.
Pregnancy
Most prospective epidemiological studies and worldwide post-marketing data have not shown an increased risk of adverse effects on the fetus or newborn associated with inhaled budesonide use during pregnancy. It is important for both the mother and the fetus that asthma is adequately controlled during pregnancy. As with any medication used during pregnancy, the benefit of budesonide use for the mother should be weighed against potential risks to the fetus.
Animal studies have demonstrated that glucocorticosteroids may cause developmental abnormalities; however, these findings are not considered relevant to humans when used at recommended doses.
Animal studies have also shown that excess prenatal glucocorticoids may affect intrauterine development, adult cardiovascular disease, and cause permanent changes in glucocorticoid receptor density, neurotransmitter metabolism, and behavior, even at doses below teratogenic levels.
During pregnancy, the lowest effective dose of budesonide should be used, taking into account the risk of worsening asthma.
Breastfeeding period
Budesonide is excreted in human breast milk.
However, when used at therapeutic doses, Pulmicort Turbuhaler is not expected to have any effect on the breastfed infant, as systemic exposure to the infant is negligible. Pulmicort Turbuhaler may be used during breastfeeding.
Maintenance treatment with inhaled budesonide (200 or 400 mcg twice daily) in breastfeeding women with bronchial asthma results in only minimal systemic exposure of budesonide in breastfed infants. In a pharmacokinetic study, the calculated daily dose in the infant was 0.3% of the mother's daily dose for both doses.
The average plasma concentration in infants was estimated to be one six-hundredth of the concentration observed in maternal plasma, assuming complete bioavailability in the infant. Budesonide concentrations in all infant plasma samples were below the limit of quantification.
Ability to affect reaction speed when driving or operating machinery.
No effect.
Method of Administration and Dosage
Bronchial Asthma
The dosage of Pulmicort Turbuhaler should be individually adjusted.
At the beginning of inhaled corticosteroid therapy for the treatment of severe asthma exacerbations, or during dose reduction, or when discontinuing oral corticosteroids, the dosage should be as follows:
Children aged 5–7 years: 100–400 mcg per day, divided into 2–4 inhalations. The total daily dose may be administered as a single dose.
Children aged 7 years and older: 100–800 mcg per day, divided into 2–4 inhalations. When daily doses of up to 400 mcg are used, the entire dose may be administered once daily.
Adults: The usual dosage is 200–800 mcg per day, divided into 2–4 inhalations. In more severe cases, daily doses of up to 1600 mcg may be required. When daily doses of up to 400 mcg are used, the entire dose may be administered once daily.
The maintenance dose should be as low as possible.
When using the Turbuhaler inhaler, an inspiratory flow rate of approximately 35–60 L/min, which is observed in most patients (including children), ensures adequate delivery of the drug and provides therapeutic efficacy. An inspiratory flow rate below 35 L/min has also demonstrated therapeutic effect. The efficacy of Pulmicort Turbuhaler is at least equivalent to that of conventional glucocorticoids delivered via pressurized metered-dose inhalers.
It is possible that when using Pulmicort Turbuhaler, the patient may not feel either taste or the medication itself; this is due to the very small particle size of the substance released during use.
After administration of a single dose, the effect is expected within several hours. Full therapeutic effect is achieved only after several weeks of treatment. Treatment with Pulmicort Turbuhaler is a preventive therapy and has no proven effect on acute episodes.
Clinical studies have shown that administration of Pulmicort Turbuhaler results in greater lung deposition of budesonide compared to administration of Pulmicort via pressurized metered-dose inhaler (pMDI). Switching a stable patient from Pulmicort metered-dose inhaler to Pulmicort Turbuhaler may require a reduction in dose.
In patients for whom an enhanced therapeutic effect is desired, increasing the dose of Pulmicort Turbuhaler is generally preferred over combination therapy with oral corticosteroids, as the risk of systemic side effects is lower with Pulmicort Turbuhaler.
Patients Using Oral Steroids
Pulmicort may allow replacement or significant reduction of oral corticosteroid dosage while maintaining asthma control.
When switching from oral steroids to Pulmicort Turbuhaler, the patient should be in a relatively stable condition. For 10 days, administer a high dose of Pulmicort Turbuhaler in combination with the previously used oral steroid dose. After this period, the oral steroid dose should be gradually reduced, for example, by 2.5 mg/month of prednisolone or equivalent per month, to the lowest possible level. Often, oral steroid therapy can be completely discontinued.
Chronic Obstructive Pulmonary Disease (COPD)
The recommended dose of Pulmicort Turbuhaler is 400 mcg twice daily.
For patients who respond positively to treatment during the first 3–6 months of Pulmicort Turbuhaler therapy, the drug should be used long-term.
When prescribing Pulmicort Turbuhaler to COPD patients who are using oral glucocorticosteroids, dose reduction should follow the recommendations for bronchial asthma therapy.
Hepatic or Renal Impairment
There is no clinical experience in treating patients with hepatic or renal impairment. Since budesonide is primarily eliminated via hepatic metabolism, an enhanced effect may be expected in patients with severe liver cirrhosis.
Instructions for Correct Use of Pulmicort Turbuhaler
The active substance enters the body through inhaled air, i.e., when the patient inhales through the mouthpiece, the substance reaches the airways together with the inhaled air.
It is important to instruct the patient to:
- follow the instructions for use;
- inhale strongly and deeply through the mouthpiece to ensure optimal delivery to the lungs;
- never exhale through the mouthpiece;
- close the Pulmicort Turbuhaler with the cap immediately after use;
- rinse the mouth with water after inhalation of the maintenance dose to minimize the risk of oral candidiasis.
Instructions for Correct Use of Pulmicort Turbuhaler
Pulmicort Turbuhaler is a multi-dose inhaler that delivers a very small amount of powder (Fig. 1). The powder reaches the lungs when inhaled through the mouthpiece. Therefore, it is important to inhale strongly and deeply through the mouthpiece.


Fig. 1.
How to Use the Inhaler
- Unscrew and remove the protective cap.
- Hold the inhaler vertically with the dose counter at the bottom. Do not hold the inhaler by the mouthpiece when turning the dose disk.
- Turn the dose disk fully in one direction, then back fully in the opposite direction until it stops. (Fig. 2). The initial direction of rotation does not matter. During this procedure, a clicking sound may be heard. (For first-time use, repeat this step twice. For second and subsequent uses, perform this step once only.)

Fig. 2.
Overdose is not possible, even if the dose disk is accidentally activated several times.
- First, exhale completely without using the device. Then place the mouthpiece between the lips and inhale strongly and deeply through the device (Fig. 3). Do not chew or bite the mouthpiece, as it may become loose or detached!
Do not use the device if it is damaged or if the mouthpiece has detached.
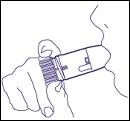
Fig. 3.
- Remove the device from the mouth and hold the breath for a few seconds.
Do not exhale through the device!
If more than one inhalation is prescribed, repeat steps 2–5.
- Replace the protective cap immediately after use, screwing it back tightly onto the device.
Notes
Never exhale through the mouthpiece.
Always replace the protective cap immediately after use.
Since each dose contains only the pure active substance and no inactive ingredients, in most cases the patient may not feel the medication particles depositing on the oral mucosa. In rare cases, a bitter taste may be perceived. Even if the medication cannot be tasted or felt after inhalation, the patient can be confident that the dose was delivered, provided the instructions were followed correctly. To reduce the risk of Candida-induced fungal infection, the patient should use Pulmicort Turbuhaler before meals or rinse the mouth cavity after inhalation.
Cleaning the Mouthpiece
It is recommended to clean the outer surface of the mouthpiece weekly using a dry cloth. Do not use water or other liquids to clean the mouthpiece.
When the Device Content is Used Up
When a red marker appears in the dose indicator window located below the mouthpiece, approximately 20 inhalations remain available (Fig. 4).

Approximately 20 doses remaining
Fig. 4.
When the red marker reaches the bottom edge of the window, these 20 doses have been used (Fig. 5). Although a small amount of active substance may still remain, for technical reasons the device should no longer be used for inhalations.
Mouthpiece

empty empty
Fig. 5.
The sound produced when shaking the Turbuhaler inhaler is caused by movement of residual desiccant, which protects the active substance from excess moisture. The active substance itself does not produce sound.
Other Information
The rotating dosator is embossed with a Braille code to identify Pulmicort Turbuhaler (the code for Pulmicort Turbuhaler is the number 2, distinguishing it from other AstraZeneca products).
Children
Do not use in children under 5 years of age.
Overdose
Acute overdose of Pulmicort Turbuhaler, even at high doses, is not expected to cause any clinical problems. With chronic use of high doses, systemic glucocorticosteroid effects such as hypercorticism and adrenal suppression may occur.
Adverse Reactions
Adverse reactions are categorized by frequency of occurrence:
Very common (≥ 1/10), common (≥ 1/100 to < 1/10), uncommon (≥ 1/1000 to < 1/100), rare (≥ 1/10000 to < 1/1000), very rare (< 1/10000), frequency not known (cannot be estimated based on available data).
Adverse reactions by organ systems and frequency of occurrence during drug use
| Organ system |
Frequency |
Adverse reactions to the use of the medicinal product |
| Infections and infestations |
Common |
Candida infections of the mouth and throat, pneumonia (in patients with COPD) |
| Immune system disorders |
Uncommon |
Immediate and delayed hypersensitivity reactions, including rash, itching, contact dermatitis, urticaria, angioedema, and anaphylactic reaction. |
| Endocrine system disorders |
Uncommon |
Symptoms indicating systemic corticosteroid effects, including adrenal suppression and growth retardation*, increased susceptibility to infections |
| Eye disorders |
Frequency unknown |
Glaucoma. |
| Uncommon |
Cataract**, Blurred vision (see also section "Special warnings and precautions for use"). |
|
| Psychiatric disorders |
Uncommon |
Restlessness, nervousness, behavioral changes (mainly in children). |
| Frequency unknown |
Sleep disturbances, psychomotor hyperactivity, aggression. |
|
| Uncommon |
Anxiety, depression. |
|
| Nervous system disorders |
Uncommon |
Tremor |
| Respiratory, thoracic and mediastinal disorders |
Common |
Cough, throat irritation. |
| Uncommon |
Bronchospasm, dysphonia, hoarseness |
|
| Skin and subcutaneous tissue disorders |
Uncommon |
Contusion (bruising). |
| Musculoskeletal and connective tissue disorders |
Uncommon |
Osteoporosis (with long-term use), muscle cramps. |
* See below "Children".
** See below "Eye disorders".
Sometimes, when using inhaled glucocorticosteroids, symptoms of systemic glucocorticosteroid side effects may occur, which are likely dependent on the dose, duration of exposure, concomitant and previous corticosteroid exposure, as well as individual sensitivity.
Infections and infestations
Due to the risk of developing candidiasis infection in the mouth and throat, patients should rinse their mouth with water after each dose administration.
Eye disorders
Cataract was also reported as an uncommon adverse effect in the placebo group in placebo-controlled studies.
Psychiatric disorders
In pooled clinical trials, 13,119 patients received inhaled budesonide and 7,278 patients received placebo. The incidence of anxiety was 0.52% with inhaled budesonide and 0.63% with placebo; the incidence of depression was 0.67% with inhaled budesonide and 1.15% with placebo.
Children
Due to the risk of growth retardation in children, growth parameters should be monitored regularly (see section "Dosage and administration").
Reporting of suspected adverse reactions
It is important to report suspected adverse reactions during the post-marketing period of the medicinal product. This allows ongoing monitoring of the benefit-risk balance of the medicinal product. Healthcare professionals are required to report any suspected adverse reactions via the national reporting system.
Shelf life. 2 years.
Storage conditions. Store out of reach of children at a temperature not exceeding 30 °C. Replace the inhaler cap after use.
Packaging. 200 doses (for 100 mcg/dose) or 100 doses (for 200 mcg/dose) in a plastic inhaler. One inhaler per cardboard box.
Prescription status. Prescription only.
Manufacturer. AstraZeneca AB/AstraZeneca AB.
Manufacturer's address and place of business.
Forskaragatan 18, Sodertalje, 151 36, Sweden / Forskaragatan 18, Sodertalje, 151 36, Sweden.