Fluconazole-darnitsa
Ukraine
Table of Contents
INSTRUCTIONS FOR MEDICAL USE OF THE MEDICINAL PRODUCT FLUCONAZOLE-DARNITSA (FLUCONAZOLE-DARNITSA)
Composition:
Active ingredient: fluconazole;
1 ml of solution contains 2 mg of fluconazole;
Excipients: sodium chloride, water for injections.
Pharmaceutical form. Infusion solution.
Main physicochemical properties: clear, colorless liquid.
Pharmacotherapeutic group. Antifungal agents for systemic use. Triazole derivatives. ATC code J02A C01.
Pharmacological Properties.
Pharmacodynamics.
Mechanism of action.
Fluconazole, an antifungal agent of the triazole class, is a potent and selective inhibitor of fungal enzymes essential for ergosterol synthesis. Its primary mechanism of action is the inhibition of fungal 14-alpha-lanosterol demethylation, mediated by cytochrome P450, which is an essential step in fungal ergosterol biosynthesis. Accumulation of 14-alpha-methyl sterols correlates with subsequent depletion of ergosterol in the fungal cell membrane and may account for the antifungal activity of fluconazole. Fluconazole is more selective for fungal cytochrome P450 enzymes than for various cytochrome P450 enzyme systems in mammals.
Administration of fluconazole at a dose of 50 mg once daily for 28 days does not affect plasma testosterone levels in men or endogenous steroid levels in women of reproductive age. Fluconazole at doses of 200–400 mg once daily does not exhibit clinically significant effects on endogenous steroid levels or on the response to ACTH stimulation in healthy male volunteers.
Interaction studies with antipyrine demonstrated that single or multiple doses of 50 mg fluconazole do not affect antipyrine metabolism.
In vitro susceptibility.
Fluconazole demonstrates in vitro antifungal activity against the most common Candida species (including C. albicans, C. parapsilosis, C. tropicalis). C. glabrata shows a wide range of susceptibility to fluconazole, whereas C. krusei is resistant.
Fluconazole also demonstrates in vitro activity against Cryptococcus neoformans and Cryptococcus gattii, as well as against endemic molds such as Blastomyces dermatitidis, Coccidioides immitis, Histoplasma capsulatum, and Paracoccidioides brasiliensis.
Pharmacodynamics–Pharmacokinetics.
Based on animal studies, there is a correlation between minimum inhibitory concentration (MIC) and efficacy against experimental models of mycoses caused by Candida species. Clinical studies indicate a linear relationship between AUC and fluconazole dose (approximately 1:1). There is also a direct, although not fully sufficient, relationship between AUC or dose and positive clinical response in the treatment of oral candidiasis and, to a lesser extent, candidemia. Treatment outcomes for infections caused by strains exhibiting high minimum inhibitory concentrations to fluconazole are less favorable.
Mechanism of resistance.
Candida species exhibit multiple mechanisms of resistance to azole antifungal agents. Fluconazole shows high minimum inhibitory concentrations against fungal strains possessing one or more resistance mechanisms, which negatively impacts its in vivo efficacy and clinical effectiveness. Cases of superinfection with Candida spp., other than C. albicans, including species frequently resistant to fluconazole (e.g., Candida krusei), have been reported. Alternative antifungal agents should be used for the treatment of such infections.
Pharmacokinetics.
Pharmacokinetic properties of fluconazole are similar following intravenous and oral administration.
Distribution.
The volume of distribution is approximately equal to total body water. Plasma protein binding is low (11–12%).
Fluconazole penetrates well into all studied body fluids. Concentrations in saliva and sputum are similar to those in plasma. In patients with fungal meningitis, fluconazole concentrations in cerebrospinal fluid reach 80% of plasma levels.
High concentrations of fluconazole in the skin, exceeding serum levels, are achieved in the stratum corneum, epidermis, dermis, and sweat. Fluconazole accumulates in the stratum corneum. After administration of a 50 mg once-daily dose, fluconazole concentration on day 12 of treatment was 73 µg/g, and 7 days after treatment completion, the concentration remained at 5.8 µg/g. With a dose of 150 mg once weekly, the concentration on day 7 of treatment was 23.4 µg/g; 7 days after the next dose, the concentration was still 7.1 µg/g.
Fluconazole concentrations in nails after 4 months of 150 mg once weekly dosing were 4.05 µg/g in healthy volunteers and 1.8 µg/g in patients with nail disorders; fluconazole was detectable in nail samples up to 6 months after therapy completion.
Metabolism.
Fluconazole is minimally metabolized. After administration of radiolabeled doses, only 11% of fluconazole is excreted in urine in altered form. Fluconazole is a selective inhibitor of CYP2C9 and CYP3A4 isoenzymes and an inhibitor of the CYP2C19 isoenzyme. Fluconazole is a moderate inhibitor of CYP2C9 and CYP3A4 and a potent inhibitor of CYP2C19.
Excretion.
The plasma half-life of fluconazole is approximately 30 hours. The majority of the drug is excreted by the kidneys, with 80% of the administered dose recovered unchanged in urine. Fluconazole clearance is proportional to creatinine clearance. No circulating metabolites have been identified.
The prolonged plasma half-life allows for single-dose treatment of vaginal candidiasis and once-weekly dosing for other indications.
Renal impairment.
In patients with severe renal impairment (glomerular filtration rate < 20 mL/min), the elimination half-life increases from 30 hours to 98 hours. Therefore, dose reduction is required in this patient population. Fluconazole is removed by hemodialysis and, to a lesser extent, by peritoneal dialysis. A 3-hour hemodialysis session reduces plasma fluconazole levels by approximately 50%.
Pediatric population.
Pharmacokinetic data were evaluated in 113 children across 5 studies: 2 single-dose studies, 2 multiple-dose studies, and 1 study involving preterm neonates.
After administration of 2–8 mg/kg fluconazole to children aged 9 months to 15 years, AUC was approximately 38 µg × hour/mL per 1 mg/kg dose. Following multiple dosing, the mean plasma half-life of fluconazole ranged between 15 and 18 hours; the volume of distribution was 880 mL/kg. A longer half-life of approximately 24 hours was observed after single-dose administration. This is comparable to the plasma half-life observed after a single 3 mg/kg intravenous dose in children aged 11 days to 11 months. The volume of distribution in this age group was approximately 950 mL/kg.
Experience with fluconazole in neonates is limited to pharmacokinetic studies involving 12 preterm infants with a gestational age of approximately 28 weeks. The median age at first dose was 24 hours (range 9–36 hours); mean birth weight was 900 g (range 750–1100 g). The study protocol was completed in 7 patients. Up to 5 intravenous doses of fluconazole 6 mg/kg were administered every 72 hours. The mean half-life was 74 hours (range 44–185) on day 1, decreasing to 53 hours (range 30–131) on day 7 and to 47 hours (range 27–68) on day 13. The area under the curve (AUC, µg × hour/mL) was 271 (range 173–385) on day 1, increased to 490 (range 292–734) on day 7, then decreased to 360 (range 167–566) on day 13. The volume of distribution (mL/kg) was 1183 (range 1070–1470) on day 1, increased to 1184 (range 510–2130) on day 7, and to 1328 (range 1040–1680) on day 13.
Elderly patients.
A pharmacokinetic study was conducted in 22 patients (aged 65 years and older) who received 50 mg oral fluconazole. Ten participants were concurrently receiving diuretics. Cmax was 1.54 µg/mL, reached within 1.3 hours after fluconazole administration. Mean AUC was 76.4 ± 20.3 µg × hour/mL. Mean half-life was 46.2 hours. These pharmacokinetic parameters are higher than those observed in younger healthy volunteers. Concomitant diuretic use had no significant effect on Cmax or AUC. Additionally, creatinine clearance (74 mL/min), percentage of unchanged fluconazole excreted in urine (0–24 hours, 22%), and renal clearance of fluconazole (0.124 mL/min/kg) in this age group were lower than in younger volunteers. Therefore, pharmacokinetic changes in elderly patients are dependent on renal function parameters.
Clinical characteristics.
Indications.
Fluconazole-Darnytsia is indicated for the treatment of the following fungal infections in adults:
- cryptococcal meningitis;
- coccidioidomycosis;
- invasive candidiasis;
- mucosal candidiasis, including oropharyngeal candidiasis and esophageal candidiasis, candiduria, chronic cutaneous and mucosal candidiasis;
- chronic atrophic oral candidiasis (denture stomatitis) when oral hygiene or local therapy is ineffective.
Fluconazole-Darnytsia is indicated for the prevention of the following conditions in adults:
- recurrence of cryptococcal meningitis in patients at high risk of developing it;
- recurrence of oropharyngeal or esophageal candidiasis in HIV-infected patients at high risk of developing it;
- prophylaxis of candidiasis in patients with prolonged neutropenia (e.g., patients with hematological malignancies receiving chemotherapy or patients undergoing hematopoietic stem cell transplantation).
Fluconazole-Darnytsia is administered to children from birth for the treatment of mucosal candidiasis (oropharyngeal candidiasis, esophageal candidiasis), invasive candidiasis, cryptococcal meningitis, and for the prevention of candidiasis in immunocompromised patients. The medicinal product may be used as maintenance therapy to prevent recurrence of cryptococcal meningitis in children at high risk of developing it.
Treatment with the medicinal product may be initiated before obtaining results of culture and other laboratory tests; antibacterial therapy should be adjusted accordingly after test results become available.
Contraindications.
Hypersensitivity to fluconazole, to other azole compounds, or to any of the excipients of the medicinal product.
Concomitant administration of fluconazole and terfenadine to patients receiving fluconazole repeatedly at doses of 400 mg/day or higher (based on results of multiple-dose interaction studies).
Concomitant administration of fluconazole and other medicinal products that prolong the QT interval and are metabolized via the CYP3A4 enzyme (e.g., cisapride, astemizole, pimozide, quinidine, and erythromycin).
Interaction with other medicinal products and other forms of interaction
Concomitant use of fluconazole and the following medicinal products is contraindicated.
Cisapride. Cases of cardiac adverse reactions, including paroxysmal ventricular tachycardia of the "torsades de pointes" type, have been reported in patients who concurrently received fluconazole and cisapride. A controlled study demonstrated that concomitant administration of 200 mg fluconazole once daily and 20 mg cisapride four times daily significantly increased plasma levels of cisapride and prolonged the QT interval. Concomitant use of fluconazole and cisapride is contraindicated (see section "Contraindications").
Terfenadine. Due to cases of severe cardiac arrhythmias caused by QTc interval prolongation in patients receiving azole antifungal agents concomitantly with terfenadine, interaction studies between these drugs were conducted. In one study, administration of fluconazole at a dose of 200 mg daily did not result in QTc interval prolongation. Another study using fluconazole at doses of 400 and 800 mg daily demonstrated that fluconazole at doses of 400 mg daily or higher significantly increased plasma levels of terfenadine when both drugs were administered concomitantly. Concomitant use of fluconazole at doses of 400 mg or higher with terfenadine is contraindicated (see section "Contraindications"). When fluconazole is used at doses below 400 mg daily concomitantly with terfenadine, careful patient monitoring is required.
Astemizole. Concomitant use of fluconazole and astemizole may reduce the clearance of astemizole. The resulting increase in plasma concentration of astemizole may lead to QT interval prolongation and, rarely, to paroxysmal ventricular tachycardia of the "torsades de pointes" type. Concomitant use of fluconazole and astemizole is contraindicated.
Pimozide and quinidine. Concomitant use of fluconazole and pimozide or quinidine may lead to inhibition of pimozide or quinidine metabolism, although appropriate in vitro and in vivo studies have not been conducted. Increased plasma concentrations of pimozide or quinidine may cause QT interval prolongation and, rarely, lead to the development of paroxysmal ventricular tachycardia of the "torsades de pointes" type. Concomitant use of fluconazole and pimozide or quinidine is contraindicated.
Erythromycin. Concomitant use of erythromycin and fluconazole may potentially increase the risk of cardiotoxicity (QT interval prolongation, paroxysmal ventricular tachycardia of the "torsades de pointes" type) and, as a consequence, sudden cardiac death. The use of this combination of medicinal products is contraindicated.
Concomitant use of fluconazole and the following medicinal products is not recommended.
Halofantrine. Fluconazole may increase plasma concentrations of halofantrine by inhibiting CYP3A4. Concomitant use of these medicinal products may increase the risk of cardiotoxicity (QT interval prolongation, paroxysmal ventricular tachycardia of the "torsades de pointes" type) and, as a consequence, sudden cardiac death. The use of this combination of medicinal products should be avoided.
Concomitant use of fluconazole and the following medicinal products requires caution and dose adjustment.
Amiodarone. Concomitant use of fluconazole with amiodarone may lead to QT interval prolongation. Fluconazole should be used with caution together with amiodarone, especially when high-dose fluconazole (800 mg) is prescribed.
Effect of other medicinal products on fluconazole.
Interaction studies have demonstrated that oral administration of fluconazole concomitantly with food intake, cimetidine, antacids, or total body irradiation for bone marrow transplantation does not have a clinically significant effect on fluconazole absorption.
Rifampicin. Concomitant administration of fluconazole and rifampicin resulted in a 25 % decrease in AUC and a 20 % reduction in the elimination half-life of fluconazole. Therefore, for patients receiving rifampicin, consideration should be given to increasing the dose of fluconazole.
Hydrochlorothiazide. In a pharmacokinetic interaction study, multiple concomitant administration of hydrochlorothiazide to healthy volunteers receiving fluconazole increased plasma concentrations of fluconazole by 40 %. Such interaction parameters do not require changes in the dosing regimen of fluconazole for patients receiving diuretics concomitantly.
Effect of fluconazole on other medicinal products.
Fluconazole is a moderate inhibitor of CYP2C9 and CYP3A4 isoenzymes of cytochrome P450. Fluconazole is a potent inhibitor of the CYP2C19 isoenzyme. In addition to observed/documentarily confirmed interactions described below, there is a risk of increased plasma concentrations of other compounds metabolized by CYP2C9, CYP2C19, and CYP3A4 when administered concomitantly with fluconazole. Therefore, such combinations of medicinal products should be used with caution; careful monitoring of patients is required. The inhibitory effect of fluconazole on enzymes persists for 4–5 days after its administration due to its long elimination half-life.
Abrocitinib. Fluconazole (inhibitor of CYP2C19, CYP2C9, CYP3A4) increased exposure to the active moiety of abrocitinib by 155 %. When used concomitantly with fluconazole, the dose of abrocitinib should be adjusted according to the instructions for medical use of abrocitinib.
Alfentanil. Concomitant administration of alfentanil at a dose of 20 µg/kg and fluconazole at a dose of 400 mg to healthy volunteers resulted in a twofold increase in AUC10, possibly due to inhibition of CYP3A4. Dose adjustment of alfentanil may be necessary.
Amitriptyline, nortriptyline. Fluconazole enhances the effects of amitriptyline and nortriptyline.
It is recommended to measure concentrations of 5-nortriptyline and/or S-amitriptyline at the beginning of combination therapy and after 1 week. If necessary, the dose of amitriptyline/nortriptyline should be adjusted.
Amphotericin B. Concomitant administration of fluconazole and amphotericin B in immunocompetent and immunocompromised infected mice resulted in the following outcomes: slight additive antifungal effect in systemic C. albicans infection, no interaction in intracranial Cryptococcus neoformans infection, and antagonism between the two medicinal products in systemic A. fumigatus infection. The clinical significance of these findings is unknown.
Anticoagulants. As with other azole antifungal agents, cases of bleeding (hematomas, epistaxis, gastrointestinal bleeding, hematuria, and melena) associated with prolonged prothrombin time have been reported when fluconazole was used concomitantly with warfarin. A twofold increase in prothrombin time was observed when fluconazole was used concomitantly with warfarin, likely due to inhibition of warfarin metabolism via CYP2C9. Prothrombin time should be carefully monitored in patients receiving coumarin anticoagulants or indanediones concomitantly. Dose adjustment of the anticoagulant may be necessary.
Short-acting benzodiazepines, e.g., midazolam, triazolam. Administration of fluconazole after oral administration of midazolam resulted in a significant increase in midazolam concentration and enhanced psychomotor effects. Concomitant administration of fluconazole at a dose of 200 mg and midazolam at a dose of 7.5 mg orally increased AUC and elimination half-life by 3.7 and 2.2 times, respectively. Administration of fluconazole at a dose of 200 mg daily and 0.25 mg triazolam orally increased AUC and elimination half-life of triazolam by 4.4 and 2.3 times, respectively. Potentiation and prolongation of triazolam effects were observed when fluconazole and triazolam were used concomitantly.
If benzodiazepines must be prescribed concomitantly to a patient undergoing fluconazole therapy, their dose should be reduced and appropriate patient monitoring should be established.
Carbamazepine. Fluconazole inhibits carbamazepine metabolism and increases serum carbamazepine levels by 30 %. There is a risk of carbamazepine toxicity. Dose adjustment of carbamazepine may be necessary depending on its concentration and effect.
Calcium channel blockers. Some calcium antagonists (nifedipine, isradipine, amlodipine, and felodipine) are metabolized by the CYP3A4 enzyme. Fluconazole may potentially increase systemic exposure to calcium channel blockers. Careful monitoring for adverse reactions is recommended.
Celecoxib. Concomitant administration of fluconazole (200 mg daily) and celecoxib (200 mg) increased Cmax and AUC of celecoxib by 68 % and 134 %, respectively. When celecoxib and fluconazole are used concomitantly, a reduction in the dose of celecoxib by half may be necessary.
Cyclophosphamide. Concomitant administration of cyclophosphamide and fluconazole leads to increased serum levels of bilirubin and creatinine. These medicinal products may be used concomitantly, with special attention to the risk of increased serum bilirubin and creatinine concentrations.
Fentanyl. A fatal case of fentanyl intoxication due to a possible interaction between fentanyl and fluconazole has been reported. In addition, a study involving healthy volunteers demonstrated that fluconazole significantly slowed fentanyl elimination. Increased fentanyl concentration may lead to respiratory depression; therefore, careful patient monitoring is required. Dose adjustment of fentanyl may be necessary.
HMG-CoA reductase inhibitors. Concomitant use of fluconazole and HMG-CoA reductase inhibitors metabolized by CYP3A4 (atorvastatin and simvastatin), or HMG-CoA reductase inhibitors metabolized by CYP2C9 (fluvastatin (reduced hepatic metabolism of statin)), increases the risk of myopathy and rhabdomyolysis (dose-dependent). If concomitant use of these medicinal products is necessary, careful monitoring of patients for symptoms of myopathy and rhabdomyolysis and monitoring of creatine kinase levels should be performed. If creatine kinase levels are significantly elevated, or if myopathy/rhabdomyolysis is diagnosed or suspected, HMG-CoA reductase inhibitors should be discontinued. Dose reduction of HMG-CoA reductase inhibitors may be required, as specified in the instructions for medical use of statins.
Ibrutinib. Moderate CYP3A4 inhibitors, such as fluconazole, increase plasma concentrations of ibrutinib and may increase the risk of toxicity. If combination therapy cannot be avoided, the dose of ibrutinib should be reduced to 280 mg once daily (2 capsules) to continue inhibitor therapy, with continuous clinical monitoring.
Ivacaftor (as monotherapy or in combination with drugs of the same therapeutic class). Concomitant administration of ivacaftor, a cystic fibrosis transmembrane conductance regulator (CFTR) modulator, increased exposure to ivacaftor by 3 times and exposure to hydroxymethylivacaftor (M1) by 1.9 times. Dose reduction of ivacaftor (as monotherapy or in combination) is required, as specified in the instructions for medical use of ivacaftor (as monotherapy or in combination).
Olaparib. Moderate CYP3A4 inhibitors, such as fluconazole, increase plasma concentrations of olaparib; their concomitant use is not recommended. If such a combination cannot be avoided, olaparib intake should be limited to 200 mg twice daily.
Immunosuppressants (e.g., cyclosporine, everolimus, sirolimus, and tacrolimus).
Cyclosporine. Fluconazole significantly increases the concentration and AUC of cyclosporine. Concomitant administration of fluconazole at a dose of 200 mg/day and cyclosporine at a dose of 2.7 mg/kg/day resulted in an 1.8-fold increase in AUC of cyclosporine. These medicinal products may be used concomitantly provided the dose of cyclosporine is reduced based on its concentration.
Everolimus. Although in vitro and in vivo studies have not been conducted, fluconazole may increase serum concentrations of everolimus by inhibiting CYP3A4.
Sirolimus. Fluconazole increases plasma concentrations of sirolimus, likely by inhibiting CYP3A4 and P-glycoprotein metabolism of sirolimus. These medicinal products may be used concomitantly provided the dose of sirolimus is adjusted based on its concentration and effects.
Tacrolimus. Fluconazole may increase serum concentrations of tacrolimus up to 5 times when administered orally due to inhibition of CYP3A4 metabolism of tacrolimus in the intestine. No significant changes in pharmacokinetics were observed with intravenous administration of tacrolimus. Elevated tacrolimus levels are associated with nephrotoxicity. The oral dose of tacrolimus should be reduced based on tacrolimus concentration.
Losartan. Fluconazole inhibits the metabolism of losartan to its active metabolite (E-31 74), which accounts for most of the angiotensin II receptor antagonism during losartan administration. Continuous monitoring of blood pressure in patients is recommended.
Lurasidone. Moderate CYP3A4 inhibitors, such as fluconazole, may increase plasma concentrations of lurasidone. If concomitant use cannot be avoided, the dose of lurasidone should be reduced as specified in the instructions for medical use of lurasidone.
Methadone. Fluconazole may increase serum concentrations of methadone. Dose adjustment of methadone may be necessary when methadone and fluconazole are used concomitantly.
Nonsteroidal anti-inflammatory drugs (NSAIDs). When used concomitantly with fluconazole, Cmax and AUC of flurbiprofen increased by 23 % and 81 %, respectively, compared to administration of flurbiprofen alone. Similarly, concomitant administration of fluconazole with racemic ibuprofen (400 mg) increased Cmax and AUC of the pharmacologically active isomer S-(+)-ibuprofen by 15 % and 82 %, respectively, compared to administration of racemic ibuprofen alone.
Although specific studies have not been conducted, fluconazole may potentially increase systemic exposure to other NSAIDs metabolized by CYP2C9 (e.g., naproxen, lornoxicam, meloxicam, diclofenac). Periodic monitoring for adverse reactions and toxic effects associated with NSAIDs is recommended. Dose adjustment of NSAIDs may be required.
Phenytoin. Fluconazole inhibits hepatic metabolism of phenytoin. Multiple concomitant administration of 200 mg fluconazole and 250 mg phenytoin intravenously increases AUC24 of phenytoin by 75 % and Cmin by 128 %. Plasma concentration of phenytoin should be monitored when these medicinal products are used concomitantly to avoid phenytoin toxicity.
Prednisolone. A case has been reported where a patient after liver transplantation developed acute adrenal insufficiency while receiving prednisolone, which occurred after discontinuation of a three-month course of fluconazole therapy. Discontinuation of fluconazole likely led to increased CYP3A4 activity, resulting in accelerated metabolism of prednisolone. Patients who have received fluconazole and prednisolone concomitantly for a prolonged period should be carefully monitored to prevent adrenal insufficiency after discontinuation of fluconazole.
Rifabutin. Fluconazole increases serum concentrations of rifabutin, leading to an increase in AUC of rifabutin by up to 80 %. Cases of uveitis have been reported when fluconazole and rifabutin are used concomitantly. Symptoms of rifabutin toxicity should be considered when using this combination of medicinal products.
Saquinavir. Fluconazole increases AUC and Cmax of saquinavir by approximately 50 % and 55 %, respectively, due to inhibition of hepatic metabolism of saquinavir by the CYP3A4 enzyme and inhibition of P-glycoprotein. Interactions between fluconazole and saquinavir/ritonavir have not been studied and may be more pronounced. Dose adjustment of saquinavir may be necessary.
Sulfonylurea derivatives. When used concomitantly, fluconazole prolongs the elimination half-life of oral sulfonylurea derivatives (chlorpropamide, glyburide, glipizide, and tolbutamide) in healthy volunteers. Frequent blood glucose monitoring and appropriate dose reduction of sulfonylurea derivatives are recommended when used concomitantly with fluconazole.
Theophylline. In a placebo-controlled interaction study, administration of fluconazole 200 mg for 14 days reduced the average plasma clearance of theophylline by 18 %. Patients receiving high-dose theophylline or those at increased risk of theophylline toxicity for other reasons should be monitored for signs of theophylline toxicity. Therapy should be modified if signs of toxicity appear.
Tofacitinib. The effect of tofacitinib increases when used concomitantly with medicinal products that cause moderate inhibition of CYP3A4 and potent inhibition of CYP2C19 (e.g., fluconazole). Therefore, it is recommended to reduce the dose of tofacitinib to 5 mg once daily when used in combination with these medicinal products.
Vonoprevir. Exposure to vonoprevir significantly increased (200 % AUC, 80 % Cmax) when vonoprevir, a CYP3A4 substrate, was administered concomitantly with fluconazole, a moderate CYP3A4 inhibitor, significantly increasing the risk of adverse reactions, including marked diuresis, dehydration, and acute renal failure. When prescribed concomitantly, the dose of vonoprevir should be reduced according to the instructions in the medical use instructions, and the patient should be regularly monitored for any adverse reactions related to vonoprevir.
Vinca alkaloids. Although appropriate studies have not been conducted, fluconazole, likely through inhibition of CYP3A4, may increase plasma concentrations of vinca alkaloids (e.g., vincristine and vinblastine), leading to neurotoxic effects.
Vitamin A. A case has been reported where a patient receiving all-trans retinoic acid (acid form of vitamin A) concomitantly with fluconazole developed central nervous system adverse reactions in the form of pseudotumor cerebri, which resolved after discontinuation of fluconazole. These medicinal products may be used concomitantly, but the risk of central nervous system adverse reactions should be remembered.
Voriconazole (inhibitor of CYP2C9, CYP2C19, and CYP3A4). Concomitant oral administration of voriconazole (400 mg every 12 hours for 1 day, then 200 mg every 12 hours for 2.5 days) and fluconazole (400 mg on day 1, then 200 mg every 24 hours for 4 days) to 8 healthy male volunteers resulted in an average increase in Cmax and AUCτ of voriconazole by 57 % (90 % CI: 20 %, 107 %) and 79 % (90 % CI: 40 %, 128 %), respectively. It is unknown whether reducing the dose and/or frequency of voriconazole or fluconazole eliminates this effect. When voriconazole is administered after fluconazole, monitoring for adverse effects associated with voriconazole is recommended.
Zidovudine. Fluconazole increases Cmax and AUC of zidovudine by 84 % and 74 %, respectively, due to a reduction in zidovudine clearance by approximately 45 % after oral administration. The elimination half-life of zidovudine was also prolonged by approximately 128 % after administration of the combination of fluconazole and zidovudine. Patients receiving this combination of medicinal products should be monitored for adverse reactions associated with zidovudine use. Consideration may be given to reducing the dose of zidovudine.
Azithromycin. In an open-label, randomized, three-way crossover study involving 18 healthy volunteers, the effect of azithromycin and fluconazole on each other's pharmacokinetics was evaluated after single oral administration at doses of 1200 mg and 800 mg, respectively. No significant pharmacokinetic interactions were observed.
Oral contraceptives. Two multiple-dose pharmacokinetic studies of fluconazole and combined oral contraceptives were conducted. At a fluconazole dose of 50 mg, no effect on hormone levels was observed, whereas at a fluconazole dose of 200 mg daily, AUC of ethinylestradiol increased by 40 % and levonorgestrel by 24 %. This suggests that multiple administration of fluconazole at the specified doses is unlikely to affect the efficacy of combined oral contraceptives.
Special precautions for use.
Dermatophytosis. According to studies on fluconazole for the treatment of dermatophytosis in children, fluconazole does not exceed griseofulvin in efficacy, and the overall efficacy rate is less than 20%. Therefore, the medicinal product should not be used for the treatment of dermatophytosis.
Cryptococcosis. Evidence of fluconazole efficacy for the treatment of cryptococcosis at other sites (e.g., pulmonary cryptococcosis and cutaneous cryptococcosis) is insufficient; therefore, there are no recommendations regarding dosage regimens for the treatment of such infections.
Deep endemic mycoses. Evidence of fluconazole efficacy for the treatment of other forms of endemic mycoses, such as paracoccidioidomycosis, histoplasmosis, and cutaneous-lymphatic sporotrichosis, is insufficient; therefore, there are no recommendations regarding dosage regimens for the treatment of such infections.
Renal system. The medicinal product should be used with caution in patients with impaired renal function (see section "Dosage and administration").
Adrenal insufficiency. Ketoconazole is known to cause adrenal insufficiency; fluconazole may also rarely cause adrenal insufficiency. Adrenal insufficiency associated with concomitant treatment with prednisolone is described in the section "Interaction with other medicinal products and other forms of interaction. Effect of fluconazole on other medicinal products."
Hepatobiliary system. The medicinal product should be used with caution in patients with impaired liver function. The use of fluconazole has been associated with rare cases of severe hepatotoxicity, including fatal outcomes, primarily in patients with serious underlying diseases. When hepatotoxicity has been associated with fluconazole use, no clear dependence on the total daily dose of the drug, duration of therapy, sex, or age of the patient has been established. Hepatotoxicity caused by fluconazole is usually reversible, and symptoms resolve after discontinuation of therapy.
Patients who develop abnormal liver function test results during fluconazole treatment should be closely monitored for the development of more severe liver injury.
Patients should be informed about symptoms that may indicate serious liver effects (marked asthenia, anorexia, persistent nausea, vomiting, and jaundice). In such cases, fluconazole treatment should be discontinued immediately and medical advice sought.
Cardiovascular system. Some azoles, including fluconazole, have been associated with QT interval prolongation on electrocardiogram. Fluconazole prolongs the QT interval by inhibiting the rectifying potassium channel (Ikr). QT interval prolongation due to other medicinal products (e.g., amiodarone) may be potentiated by inhibition of the CYP3A4 enzyme of cytochrome P450. Very rare cases of QT interval prolongation and torsades de pointes ventricular tachycardia have been reported with fluconazole use. These reports involved patients with severe underlying conditions and multiple risk factors, such as structural heart disease, electrolyte disturbances, and concomitant use of other medicinal products affecting the QT interval. Patients with hypokalemia and progressive heart failure have an increased risk of life-threatening ventricular arrhythmias and torsades de pointes.
Fluconazole should be used with caution in patients at risk of developing arrhythmias. Concomitant use with medicinal products that prolong the QTc interval and are metabolized by the CYP3A4 enzyme of cytochrome P450 is contraindicated.
Halofantrine. Halofantrine is a substrate of the CYP3A4 enzyme and prolongs the QTc interval when administered at recommended therapeutic doses. Concomitant use of halofantrine and fluconazole is not recommended.
Cutaneous reactions. Rare cases of exfoliative skin reactions such as Stevens-Johnson syndrome and toxic epidermal necrolysis have been reported during fluconazole use. Drug reaction with eosinophilia and systemic symptoms (DRESS syndrome) has also been reported. Patients with AIDS are more prone to developing severe skin reactions when using many medicinal products. If a patient with superficial fungal infection develops a rash that may be related to fluconazole use, further administration of the medicinal product should be discontinued. If a patient with invasive/systemic fungal infection develops a skin rash, careful monitoring is required, and fluconazole treatment should be discontinued in case of bullous eruptions or development of erythema multiforme.
Hypersensitivity. In rare cases, anaphylactic reactions have been reported.
Cytochrome P450. Fluconazole is a moderate inhibitor of CYP2C9 and CYP3A4 enzymes. Fluconazole is also a potent inhibitor of the CYP2C19 enzyme. Patients receiving concomitant fluconazole and medicinal products with a narrow therapeutic window that are metabolized by CYP2C9, CYP2C19, and CYP3A4 should be closely monitored.
Terfenadine. Careful monitoring of the patient is required when terfenadine and fluconazole are used concomitantly at a fluconazole dose of less than 400 mg per day.
Candidiasis. Studies have demonstrated an increasing prevalence of infections caused by Candida species other than C. albicans. These species are often intrinsically resistant (e.g., C. krusei and C. auris) or exhibit reduced susceptibility to fluconazole (C. glabrata). Such infections may require alternative antifungal therapy after failed treatment. Therefore, prescribers are advised to consider the prevalence of resistance among different Candida species to fluconazole.
Important information about excipients. The medicinal product contains 0.9% sodium chloride solution. Each 200 mg (100 ml vial) contains 15 mmol of sodium ions (0.145 mmol sodium per 1 ml) and chloride ions, which should be taken into account when prescribing to patients who need to restrict sodium and fluid intake.
Use during pregnancy or breastfeeding.
Women of childbearing potential.
Before initiating treatment, the patient should be informed about the potential risk to the fetus.
After a single dose, a washout period of fluconazole, approximately 1 week (corresponding to 5–6 half-lives), should be observed before conception (see subsection "Pharmacokinetics").
For prolonged treatment courses, women of childbearing potential should consider using contraception throughout the treatment period and for 1 week after the last dose.
Pregnancy.
Observational studies indicate an increased risk of spontaneous abortion in women who received fluconazole during the first and/or second trimester compared to women who did not take fluconazole or received topical azoles during the same period. Data from several thousand pregnant women who received fluconazole treatment with a cumulative dose ≤ 150 mg during the first trimester show no increased overall risk of fetal malformations. In one large observational cohort study, oral use of fluconazole during the first trimester was associated with a small increased risk of musculoskeletal malformations, corresponding to approximately 1 additional case per 1000 women receiving cumulative doses ≤ 450 mg, compared to women receiving topical azoles, and approximately 4 additional cases per 1000 women receiving cumulative doses > 450 mg. The adjusted relative risk was 1.29 (95% CI: 1.05–1.58) for a 150 mg oral dose of fluconazole and 1.98 (95% CI: 1.23–3.17) for fluconazole doses exceeding 450 mg.
Available epidemiological studies on the development of congenital heart defects following fluconazole use during pregnancy provide conflicting results. However, a meta-analysis of 5 observational studies involving several thousand pregnant women who received fluconazole during the first trimester found a 1.8- to 2-fold increased risk of congenital heart defects in infants compared to infants of mothers who did not use fluconazole and/or used topical azoles.
Congenital malformations have been reported in infants whose mothers received high doses (400 to 800 mg/day) of fluconazole during pregnancy for more than 3 months for the treatment of coccidioidomycosis. Among the congenital malformations observed in these children were brachycephaly, ear dysplasia, enlarged anterior fontanelle, femoral bowing, and radioulnar synostosis. A causal relationship between fluconazole use and congenital malformations has not been established.
Standard doses of fluconazole and short-term fluconazole treatment courses should not be used during pregnancy except when urgently needed.
High-dose fluconazole and/or prolonged fluconazole treatment courses should not be used during pregnancy except for the treatment of life-threatening infections.
Lactation.
Fluconazole passes into breast milk and reaches lower concentrations than in plasma. Breastfeeding may continue after a single standard dose of fluconazole (150 mg).
Breastfeeding is not recommended with repeated use of fluconazole or when fluconazole is used at high doses.
The benefit of breastfeeding for the child's development and health, the mother's clinical need for fluconazole, and any potential adverse effects of fluconazole or the mother's underlying condition on the breastfed infant should be carefully evaluated.
Fertility.
Fluconazole did not affect fertility in male and female rats.
Ability to influence reaction rate when driving or operating machinery.
Studies on the effect of the medicinal product on the ability to drive or operate machinery have not been conducted.
Patients should be informed about the possibility of developing dizziness or seizures during treatment. If such symptoms occur, driving or operating machinery is not recommended.
Administration and Dosage.
The dose of fluconazole depends on the type and severity of the fungal infection.
If repeated administration is required, treatment of infections should be continued until clinical and laboratory signs of fungal infection activity have disappeared. Inadequate duration of treatment may lead to recurrence of active infection.
The medicinal product should be administered intravenously by infusion. There is no need to change the daily dose when switching the route of administration from oral to intravenous or vice versa.
The infusion solution should be administered at a rate not exceeding 10 ml/min.
Compatibility of the medicinal product.
The medicinal product is compatible with the following solutions:
- 5% and 20% glucose solutions;
- Ringer's solution;
- Hartmann's solution;
- potassium chloride in glucose solution;
- 4.2% and 5% sodium bicarbonate solutions;
- 3.5% aminozine solution;
- 0.9% sodium chloride solution;
- dialaflex (6.36% solution for intraperitoneal dialysis).
Fluconazole may be administered through the same infusion system as one of the solutions listed above. Although cases of nonspecific incompatibility of the medicinal product with other drugs have not been reported, mixing fluconazole with other medicinal products before infusion is not recommended.
The intravenous infusion solution is intended for single use only. Dilution should be performed under aseptic conditions. The solution should be inspected for the presence of foreign particles and discoloration. The solution should be used only if it is clear and free of foreign particles. Any unused portions of the medicinal product must be discarded.
Adults.
Cryptococcosis.
- Treatment of cryptococcal meningitis: the recommended loading dose is 400 mg on the first day, followed by a maintenance dose of 200–400 mg/day. The duration of treatment is usually at least 6–8 weeks. For life-threatening infections, the daily dose may be increased to 800 mg.
- Maintenance therapy to prevent recurrence of cryptococcal meningitis in patients at high risk: the recommended dose is 200 mg/day for an indefinite duration.
Coccidioidomycosis. The recommended dose is 200–400 mg/day. The duration of treatment is 11–24 months or longer, depending on the patient's condition. For certain forms of infection, especially meningitis, a dose of 800 mg/day may be appropriate.
Invasive candidiasis. The loading dose is 800 mg on the first day, followed by a maintenance dose of 400 mg/day. The recommended duration of treatment for candidemia is usually 2 weeks after the first negative blood culture results and resolution of signs and symptoms of candidemia.
Oropharyngeal candidiasis.
- Oropharyngeal candidiasis: the loading dose is 200–400 mg on the first day, followed by a maintenance dose of 100–200 mg/day. The duration of treatment is 7–21 days (until remission is achieved), but may be extended in patients with severe immunodeficiency.
- Esophageal candidiasis: the loading dose is 200–400 mg on the first day, followed by a maintenance dose of 100–200 mg/day. The duration of treatment is 14–30 days (until remission is achieved), but may be extended in patients with severe immunodeficiency.
- Candiduria: the recommended dose is 200–400 mg/day for 7–21 days. The duration of treatment may be extended in patients with severe immunodeficiency.
- Chronic atrophic candidiasis: the recommended dose is 50 mg/day for 14 days.
- Chronic cutaneous and mucosal candidiasis: the recommended dose is 50–100 mg/day. The duration of treatment is up to 28 days, but may be extended depending on the severity and type of infection or degree of immunosuppression.
Prevention of recurrent mucosal candidiasis in HIV patients at high risk of developing the infection.
- Oropharyngeal candidiasis, esophageal candidiasis: the recommended dose is 100–200 mg/day or 200 mg three times a week. The duration of treatment is indefinite in patients with immunosuppression.
Prophylaxis of candidiasis in patients with prolonged neutropenia. The recommended dose is 200–400 mg. Treatment should be initiated several days before the expected onset of neutropenia and continued for 7 days after the neutrophil count rises above 1000/mm³.
Elderly patients.
Dosage should be adjusted according to renal function (see below).
Patients with renal impairment.
Fluconazole is primarily excreted unchanged in the urine. Dose adjustment is not required after a single dose. For patients (including children) with impaired renal function requiring multiple doses, an initial dose of 50–400 mg should be administered on the first day of treatment, depending on the indication. Thereafter, the daily dose (depending on the indication) should be adjusted according to the table:
| Creatinine clearance (ml/min) |
Percentage of recommended dose |
| > 50 |
100 % |
| ≤ 50 (without hemodialysis) |
50 % |
| Hemodialysis |
100 % after each hemodialysis |
Patients undergoing haemodialysis should receive 100 % of the recommended dose after each haemodialysis session. On days when dialysis is not performed, the patient should receive a dose adjusted according to creatinine clearance.
Patients with hepatic impairment.
Fluconazole should be used with caution in patients with hepatic dysfunction, as there is insufficient information regarding the use of fluconazole in this patient population.
Children.
The maximum daily dose of 400 mg should not be exceeded.
As with similar infections in adults, the duration of treatment depends on clinical and mycological response. Fluconazole should be administered once daily.
Dosage recommendations for children with renal impairment are provided in the section «Patients with renal impairment».
The pharmacokinetics of fluconazole have not been studied in children with renal impairment (see below information on use in neonates, in whom primary renal immaturity is frequently observed).
Children aged 12 years and older.
Depending on body weight and pubertal development, the physician should assess which dosage (adult or paediatric) is optimal for the patient. Clinical data indicate that children have a higher clearance of fluconazole compared to adults. Administration of doses of 100, 200, and 400 mg in adults and doses of 3, 6, and 12 mg/kg in children results in comparable systemic exposure.
Children aged 28 days to 11 years.
- Mucosal candidiasis: initial dose is 6 mg/kg/day, maintenance dose is 3 mg/kg/day. The initial dose may be administered on the first day to achieve steady-state concentrations more rapidly.
- Invasive candidiasis, cryptococcal meningitis: dosage is 6–12 mg/kg/day depending on the severity of the disease.
- Maintenance therapy for prevention of recurrence of cryptococcal meningitis in children at high risk: dosage is 6 mg/kg/day depending on the severity of the disease.
- Prophylaxis of candidiasis in patients with immunodeficiency: dosage is 3–12 mg/kg/day depending on the severity and duration of induced neutropenia (see adult dosing).
Children from birth to 27 days of age.
In neonates, fluconazole is eliminated slowly. Pharmacokinetic data supporting dosing recommendations for term neonates are provided in the section «Pharmacokinetics».
- Term neonates aged 0 to 14 days: doses equivalent to those specified above for children aged 28 days to 11 years should be administered every 72 hours. The maximum dose should not exceed 12 mg/kg every 72 hours.
- Term neonates aged 15 to 27 days: doses equivalent to those specified above for children aged 28 days to 11 years should be administered every 48 hours. The maximum dose should not exceed 12 mg/kg every 48 hours.
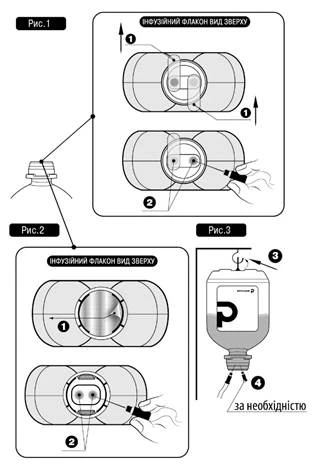
Administration method
Do not insert needle(s) into non-designated areas of the polymer bottle, only into sterile ports!
For infusion administration, follow the procedure below:
- Remove the tamper-evident plastic cap (if present).
- Remove protective closure(s) No. 1 as shown in Fig. 1 and Fig. 2 (manufacturers may use different types and materials for protective closures).
- Remove the needle cap and insert the needle into any of the designated ports No. 2 of the infusion bottle (see Fig. 1 and Fig. 2).
- The other sterile port may be used to introduce other medicinal products into the infusion bottle (No. 4, see Fig. 3), or, if necessary, for a venting needle (No. 4, see Fig. 3), in case of insufficient flow rate.
- Hang the bottle using the dedicated hanging ring No. 3 located at the bottom of the bottle (see Fig. 3).
Children. The medicinal product can be used in children from birth; see section «Dosage and administration».
Overdose.
Cases of fluconazole overdose have been reported, with concomitant hallucinations and paranoid behaviour.
In case of overdose, symptomatic and supportive treatment should be administered, and gastric lavage should be performed if necessary.
Fluconazole is largely excreted in urine; forced diuresis may accelerate drug elimination. A 3-hour haemodialysis session reduces plasma fluconazole levels by approximately 50 %.
Adverse reactions.
The most commonly reported adverse reactions (> 1/10) are: headache, abdominal pain, diarrhea, nausea, vomiting, rash, increased levels of alanine aminotransferase (ALT), aspartate aminotransferase (AST), and alkaline phosphatase in blood, drug reaction with eosinophilia and systemic symptoms (DRESS syndrome) associated with fluconazole treatment (see section "Special precautions").
The following classification is used to assess the frequency of adverse reactions: very common (≥ 1/10), common (≥ 1/100 to < 1/10), uncommon (≥ 1/1000 to < 1/100), rare (≥ 1/10,000 to < 1/1000), very rare (< 1/10,000), frequency not known (cannot be estimated from the available data).
From the ear and labyrinth disorders:
Uncommon: vertigo.
From the gastrointestinal disorders:
Common: abdominal pain, nausea, diarrhea, vomiting.
Uncommon: constipation, dyspepsia, flatulence, dry mouth.
From the liver and biliary disorders:
Common: increased alanine aminotransferase (ALT) levels, increased aspartate aminotransferase (AST) levels, increased alkaline phosphatase levels.
Uncommon: cholestasis, jaundice, increased bilirubin levels.
Rare: hepatic failure, hepatocellular necrosis, hepatitis, hepatocellular injury.
From metabolism and nutritional disorders:
Uncommon: decreased appetite.
Rare: hypercholesterolemia, hypertriglyceridemia, hypokalemia.
From the nervous system disorders:
Common: headache.
Uncommon: convulsions, paresthesia, dizziness, taste disturbance.
Rare: tremor.
From psychiatric disorders:
Uncommon: insomnia, somnolence.
From the cardiac disorders:
Rare: paroxysmal ventricular tachycardia of the "torsades de pointes" type, QT interval prolongation.
From blood and lymphatic system disorders:
Uncommon: anemia.
Rare: agranulocytosis, leukopenia, thrombocytopenia, neutropenia.
From the immune system disorders:
Rare: anaphylaxis.
From the skin and subcutaneous tissue disorders:
Common: rash.
Uncommon: drug rash (including fixed drug eruption), urticaria, pruritus, increased sweating.
Rare: toxic epidermal necrolysis, Stevens-Johnson syndrome, acute generalized exanthematous pustulosis, exfoliative dermatitis, angioneurotic edema, facial swelling, alopecia.
Frequency not known: drug reaction with eosinophilia and systemic symptoms (DRESS).
From musculoskeletal and connective tissue disorders:
Uncommon: myalgia.
General disorders and administration site conditions:
Uncommon: increased fatigue, malaise, asthenia, fever.
Children. The frequency and nature of adverse reactions and laboratory abnormalities observed in clinical trials involving children are comparable to those in adults.
Reporting of suspected adverse reactions.
Reporting suspected adverse reactions after medicine authorization is an important procedure. It allows continuous monitoring of the benefit-risk ratio of the medicinal product. Healthcare professionals should report any suspected adverse reactions via the national reporting system.
Shelf life. 3 years.
Storage conditions.
Store in the original packaging at a temperature not exceeding 25 °C. Do not freeze.
Keep out of reach and sight of children.
Incompatibilities.
No incompatibility issues with the medicinal product have been reported. The medicinal product should not be mixed with other medicinal products in the same container, except as specified in the section "Dosage and administration".
Packaging.
100 ml in a bottle; 1 bottle in a carton; bottles of 100 ml.
Prescription status. Prescription only.
Manufacturer. JSC "Pharmaceutical Company "Darnytsia".
Manufacturer's address and location of its business activity.
13, Borispilska Street, Kyiv, 02093, Ukraine.