Esperoct
UkraineTable of Contents
INSTRUCTION for medical use of the medicinal product Esperoct (Esperoct)
Composition:
Active substance: turoctocog alfa pegol;
500 IU
One vial of powder contains a nominal quantity of 500 IU turoctocog alfa pegol*.
After reconstitution of the product, 1 ml of solution contains approximately 125 IU turoctocog alfa pegol.
1000 IU
One vial of powder contains a nominal quantity of 1000 IU turoctocog alfa pegol*.
After reconstitution of the product, 1 ml of solution contains approximately 250 IU turoctocog alfa pegol.
1500 IU
One vial of powder contains a nominal quantity of 1500 IU turoctocog alfa pegol*.
After reconstitution of the product, 1 ml of solution contains approximately 375 IU turoctocog alfa pegol.
2000 IU
One vial of powder contains a nominal quantity of 2000 IU turoctocog alfa pegol*.
After reconstitution of the product, 1 ml of solution contains approximately 500 IU turoctocog alfa pegol.
3000 IU
One vial of powder contains a nominal quantity of 3000 IU turoctocog alfa pegol*.
After reconstitution of the product, 1 ml of solution contains approximately 750 IU turoctocog alfa pegol.
Activity (in international units, IU) is determined by a chromogenic assay method according to the European Pharmacopoeia. The specific activity of turoctocog alfa pegol is approximately 9500 IU/mg protein.
The active substance, turoctocog alfa pegol, is a covalent conjugate of the protein turoctocog alfa* with polyethylene glycol (PEG) of 40 kDa.
* Human Factor VIII produced by recombinant DNA technology using a Chinese hamster ovary cell line, with no human or animal-derived additives used in this cell line, during purification, conjugation, or manufacturing of the components of Esperoct.
Excipients:
powder: L-histidine; sucrose; polysorbate 80; sodium chloride; L-methionine; calcium chloride dihydrate; sodium hydroxide (for pH adjustment); hydrochloric acid (for pH adjustment);
solvent: sodium chloride; water for injections.
Pharmaceutical form. Powder and solvent for solution for injection.
Main physicochemical properties: lyophilized powder appears as a lyophilisate ranging from white to practically white.
Solvent is clear and colourless; pH 6.9; osmolality 590 mOsmol/kg.
Pharmacotherapeutic group. Haemostatics. Coagulation factor VIII.
ATC code B02BD02.
Pharmacological properties.
Pharmacodynamics.
Mechanism of action
Turoctocog alfa pegol is a purified recombinant human factor VIII (rFVIII) conjugated with a 40 kDa polyethylene glycol (PEG) molecule attached to the protein. The PEG is linked to the O-linked glycan in the truncated B-domain of rFVIII (turoctocog alfa). The mechanism of action of turoctocog alfa pegol is based on replacement of deficient or missing factor VIII in patients with haemophilia A.
When turoctocog alfa pegol is activated by thrombin at the site of injury, the B-domain containing the PEG moiety and the a3-region are cleaved off, resulting in the formation of activated recombinant factor VIII (rFVIIIa), which is structurally similar to native factor VIIIa.
The factor VIII complex with von Willebrand factor consists of two molecules (factor VIII and von Willebrand factor), each having distinct physiological functions. Upon administration of the product to a patient with haemophilia, factor VIII binds to von Willebrand factor in the bloodstream. Activated factor VIII acts as a cofactor for activated factor IX, accelerating the conversion of factor X to activated factor X.
Activated factor X converts prothrombin into thrombin. Thrombin then converts fibrinogen into fibrin, after which a clot can form. Haemophilia A is an X-linked inherited coagulation disorder caused by reduced levels of factor VIII:C, leading to severe bleeding into joints, muscles, or internal organs, either spontaneously or following trauma or surgical procedures. Through replacement therapy with factor VIII, plasma factor VIII levels are increased, thereby enabling temporary correction of the deficiency and counteracting the tendency to bleed.
Clinical efficacy in prophylaxis and treatment of bleeding episodes
The clinical efficacy of the product Esperoct in the prevention and treatment of bleeding was evaluated in seven multicenter prospective clinical studies. All patients had severe haemophilia A.
It should be noted that bleeding rates per year (ABR) obtained from different factor concentrates and in different clinical studies should not be directly compared.
Prophylaxis in adults/children aged 12 years and older
The efficacy of Esperoct in the prevention and treatment of bleeding was assessed in an open-label, uncontrolled study involving adult patients and children aged 12 years and older with severe haemophilia A. The prophylactic effect of Esperoct was demonstrated using a dose of 50 IU/kg administered every 4 days or every 3–4 days (twice weekly) in 175 patients. The mean annual bleeding rate (ABR) in adults and children aged 12 years and older receiving Esperoct was 1.18 (interquartile range (IQR): 0.00; 4.25), with spontaneous bleeding ABR of 0.00 (IQR: 0.00; 1.82), trauma-related ABR of 0.00 (IQR: 0.00; 1.74), and joint bleeding ABR of 0.85 (IQR: 0.00; 2.84). When imputed values (accounting for missing data from patients who discontinued the study) were included, the calculated mean ABR for all bleeding episodes was 3.70 (95% CI: 2.94; 4.66). Of the 175 adults/children aged 12 years and older on prophylaxis, 70 (40%) patients had no bleeding episodes. The mean annual exposure to the medicinal product for prophylaxis was 4,641 IU/kg.
Adults/children aged 12 years and older who had a low bleeding frequency (0–2 bleeding episodes in the preceding 6 months) and who had received at least 50 doses of Esperoct were eligible for randomization into prophylactic treatment groups receiving either every 7-day (75 IU/kg every 7 days) or every 4-day (50 IU/kg every 4 days) regimens. Overall, 55 of the 120 patients meeting study criteria agreed to be randomized (17 patients to the 50 IU/kg every 4 days group and 38 patients to the every 7-day group). The ABR in randomized patients was 1.77 (0.59; 5.32) with dosing every 4 days and 3.57 (2.13; 6.00) with weekly prophylaxis. During the randomized phase of the study, nine of these patients returned to prophylaxis every 4 days. Overall, considering all extension phases of the study, 31 out of 61 patients receiving prophylaxis every 7 days returned to the treatment regimen with dosing every 4 days.
Prophylaxis in previously treated patients (under 12 years of age)
The efficacy and safety of Esperoct for prophylaxis and on-demand treatment of bleeding episodes were evaluated in an open-label, single-arm, uncontrolled study involving 68 children under 12 years of age with severe haemophilia A.
The prophylactic effect of Esperoct was demonstrated with a prophylactic dose of 64.7 IU/kg administered twice weekly. The median and calculated mean annual bleeding rates (ABR) in children under 12 years receiving Esperoct twice weekly were 1.95 and 2.13, respectively (95% CI: 1.48; 3.06), with spontaneous bleeding ABR of 0.00 and 0.58 (95% CI: 0.24; 1.40), trauma-related ABR of 0.00 and 1.52 (95% CI: 1.07; 2.17), and joint bleeding ABR of 0.00 and 1.03 (95% CI: 0.59; 1.81), respectively. Among the 68 children under 12 years receiving prophylactic Esperoct, 29 patients (42.6%) had no bleeding episodes.
The mean annual requirement of the product for prophylaxis was 6,475 IU/kg.
Due to the long duration of the study, several patients moved out of the age group to which they were initially assigned: some patients < 6 years of age also entered the 6–11 years age group, and some patients from the 6–11 years age group transitioned into the adolescent category. The key efficacy results in patients under 12 years of age from the main and extension phases of the study are summarized in Table 1.
Table 1. Annual bleeding rate (ABR) in the study of previously treated paediatric patients by current age groups (main and extension phases of the study) – full analysis set
| Main Phase |
Extended Phase |
|||
| Age of patient* |
0–5 years (N = 34) |
6–11 years (N = 34) |
0–5 years (N = 27) |
6–11 years (N = 53) |
| Number of bleeding episodes |
30 |
32 |
41 |
134 |
| Main treatment period (years) |
0.46 |
0.51 |
4.79 |
4.86 |
| Overall annual bleeding rate (ABR) |
||||
| Poisson mean |
1.94 |
1.84 |
0.32 |
0.52 |
| Median |
1.94 |
1.94 |
0.22 |
0.21 |
* Some patients were included in two age groups.
Prophylaxis in previously untreated patients (PUPs) (children under 6 years of age)
The efficacy and safety of Esperoct were evaluated in a multinational, non-randomized, open-label phase 3 study. Prior prophylaxis (optional on-demand treatment of bleeding episodes and/or dosing of 60 IU/kg at intervals greater than one week until the patient reached 20 exposure days (ED) or age 24 months) and bleeding prophylaxis were assessed in 81 previously untreated patients under 6 years of age with severe haemophilia A. Of the 81 patients, 55 patients received prior prophylaxis, of whom 42 subsequently transitioned to prophylaxis. Overall, 69 patients received prophylaxis with a prophylactic dose of 68.9 IU/kg body weight administered twice weekly.
The prophylactic effect of Esperoct in previously untreated children under 6 years of age with severe haemophilia A was demonstrated by a median and calculated mean annualized bleeding rate (ABR) of 1.35 and 1.76, respectively (95% CI: 1.26; 2.46).
The mean annual requirement for the 69 previously untreated patients receiving prophylaxis was 5,395 IU/kg.
The key efficacy outcomes in previously untreated patients receiving prophylaxis, summarized by the main and extension phases of the study, are presented in Table 2.
Table 2. Annualized bleeding rate (ABR) in the study of previously untreated pediatric patients (main and extension phases of the study) – full analysis set
| Main Phase |
Extended Phase |
|
| Number of bleeding episodes |
124 |
223 |
| Treatment exposure period (years) |
0.60 |
2.83 |
| Overall annual bleeding rate (ABR) |
||
| Mean Poisson (95% CI) |
2.98 (2.16; 4.10) |
1.43 (0.98; 2.10) |
| Median |
2.49 (0.00; 5.22) |
0.73 (0.00; 2.57) |
During the study, 56 adverse reactions were reported in 43 out of 81 patients, and a total of 80 serious adverse reactions were reported in 48 patients following administration of Esperoct.
In 31 out of 59 previously untreated patients without inhibitors, a transient decrease in incremental recovery (IR) of factor VIII was observed after exposure to Esperoct. There were 17 previously untreated patients with consecutive measurements showing reduced IR; all of these patients had IgG antibodies to PEG. A relationship between anti-PEG antibodies and low IR cannot be excluded.
Clinical efficacy of Esperoct in the treatment of bleeding episodes and on-demand use
The clinical efficacy of Esperoct in the treatment of bleeding episodes was demonstrated in all previously treated patients across all age groups.
The majority of bleeding episodes treated with Esperoct were of mild to moderate severity.
The overall success rate of hemostatic therapy for treatment of bleeding episodes in previously treated patients was 84.4%.
The success rates of hemostatic therapy in age groups of previously treated patients were 89.4% (0−5 years), 82.6% (6−11 years), 78.9% (12−17 years), and 84.9% (≥ 18 years), respectively; 94.2% were successfully treated, with bleeding resolved after administration of 1–2 injections.
The efficacy of Esperoct in the treatment of bleeding episodes was demonstrated in previously untreated patients aged < 6 years. The overall success rate of hemostatic therapy was 91.9%; 93.3% were successfully treated, with bleeding resolved after administration of 1–2 injections.
In the core study, 12 patients aged 18 years and older chose to remain on demand treatment. In these patients, 1,270 bleeding episodes were treated with a mean dose of 37.5 IU/kg (range: 20–75 IU/kg). After administration of 1–2 doses of Esperoct, 97% of all bleeding episodes were stopped.
Clinical efficacy of Esperoct in surgical procedures
The hemostatic effect of Esperoct during surgical procedures was evaluated in four studies, one of which was a dedicated surgical procedure study.
In the dedicated surgical study, 49 major surgical procedures in 35 previously treated adolescent and adult patients were analyzed. On the day of surgery, patients received a preoperative mean dose of 55.7 IU/kg (range: 27.2–86.2 IU/kg), and the postoperative mean dose was 30.7 IU/kg (range: 10.1–58.8 IU/kg). The overall success rate of hemostatic therapy with Esperoct during major surgical procedures was 95.9%, with hemostatic efficacy rated as excellent or good in 47 out of 49 major surgical procedures performed.
In two studies involving previously treated pediatric patients (under 12 years of age), 24 patients underwent 46 surgical procedures, of which only one was a major surgery with a successful hemostatic response. Minor surgeries in these patients did not result in any complications, although hemostatic efficacy and factor VIII levels were not monitored during these procedures. In 26 previously untreated pediatric patients (under 6 years of age) in the study involving previously untreated patients, successful hemostatic effect was recorded in all 4 major surgical procedures and in 25 out of 30 minor surgeries. Esperoct was administered according to recommended dosing guidelines.
Pharmacokinetics
Overall, 129 pharmacokinetic (PK) profiles obtained after a single dose of Esperoct were evaluated in 86 patients (including 24 pediatric patients aged 0 to 12 years).
All pharmacokinetic studies with Esperoct were conducted in patients with severe hemophilia A (factor VIII level < 1%) who had been previously treated. Patients received a single dose of 50 IU/kg, and blood sampling was performed before administration and multiple times over 96 hours after dosing.
In adult patients, the half-life of Esperoct was 1.6 times longer than that of conventional unmodified factor VIII products.
Pharmacokinetic parameters
A total of 108 pharmacokinetic profiles obtained after a single 50 IU/kg dose of Esperoct were evaluated in 69 patients. Pharmacokinetic parameters after single-dose administration were comparable between younger children (0 to 6 years), middle-aged children (6 to 12 years), older children (12 to 17 years), and adults (≥ 18 years).
As expected, children under 12 years of age showed lower incremental recovery (IR) and higher body weight-adjusted clearance compared to adults and patients aged 12 years and older. Overall, a trend toward increasing incremental recovery (IR) and decreasing clearance (mL/h/kg) with age was observed. This is consistent with a higher volume of distribution per kilogram of body weight in children under 12 years compared to adults (Table 1).
Pharmacokinetic parameters of Esperoct after single-dose administration, determined after 28 weeks of prophylactic treatment, were consistent with the initial pharmacokinetic parameters.
Pharmacokinetic parameters of Esperoct after single administration are presented in Table 3.
Table 3. Pharmacokinetic parameters of Esperoct 50 IU/kg after single administration in previously treated patients, determined by chromogenic assay [geometric mean (CV% – coefficient of variation)]
| PK parameter, |
Patients aged 0 to 6 years (N = 13) |
Patients aged 6 to 12 years (N = 11) |
Patients aged 12 to 18 years (N = 3) |
Patients aged 18 years and older (N = 42) |
| Number of PK profiles |
13 |
11 |
5 |
79 |
| IR (IU/dL)/(IU/kg)a |
1.80 (29) |
1.99 (25) |
2.79 (12) |
2.63 (22) |
| Maximum Factor VIII activity (IU/dL)a |
101.2 (28) |
119.6 (25) |
133.2 (9) |
134.4 (23) |
| t1/2 (hours) |
13.6 (20) |
14.2 (26) |
15.8 (43) |
19.9 (34) |
| AUCinf (IU*hour/dL) |
2,147 (47) |
2,503 (42) |
3,100 (44) |
3,686 (35) |
| CL (mL/hour/kg) |
2.6 (45) |
2.4 (40) |
1.5 (43) |
1.4 (32) |
| Vss (mL/kg) |
44.2 (34) |
41.2 (25) |
33.4 (10) |
37.7 (27) |
| MRT (hours) |
17.0 (22) |
17.3 (31) |
21.7 (45) |
25.2 (29)b |
Abbreviations: AUC – area under the pharmacokinetic curve describing the time course of factor VIII activity; t1/2 – terminal half-life; MRT – mean residence time; CL – clearance; V
a Incremental recovery (IR) and factor VIII activity were determined 30 minutes after administration in patients aged 12 years and older, and 60 minutes after administration (first sample collection) in children under 12 years of age.
b Calculations based on data from 67 profiles.
In a study involving previously untreated pediatric patients, the incremental recovery (IR) of factor VIII was assessed in 46 patients under 6 years of age after the first administration, yielding a geometric mean (CV %) of 1.76 (34) [IU/dL]/[IU/kg]. In 17 out of 59 previously untreated patients without inhibitors, consecutive measurements (i.e., 2 or more) of transiently reduced factor VIII incremental recovery (IR) were observed within the range of 5–10 effective doses (further details provided in section "Special Warnings and Precautions for Use").
Mean values of minimum factor VIII activity in previously treated and previously untreated patients by age groups are summarized in Table 4.
Table 4. Mean calculated values of minimum factor VIII activity in previously treated and previously untreated patients by age groups
| Minimum Factor VIII Activity |
Previously treated patients, 60 IU/kg of Esperoct for prophylaxis twice weekly |
Previously treated patients, 50 IU/kg of Esperoct for prophylaxis every 4 days |
Previously untreated patients, 60 IU/kg of Esperoct for prophylaxis twice weekly |
||
| Age groups at time of study entry |
0–5 years |
6–11 years |
12–17 years |
≥ 18 years |
0–5 years |
| Number of patients included in the analysis |
31 |
34 |
23 |
143 |
81 |
| Number of minimum values included in the analysis |
144 |
161 |
112 |
722 |
355 |
| Number of minimum values below LLOQ |
62 |
43 |
16 |
107 |
128a |
| Mixed model resultsb: |
|||||
| 1.2 |
2.0 |
2.7 |
3.0 |
1.5 |
|
| 0.8; 1.6 |
1.5; 2.7 |
1.8; 4.0 |
2.6; 3.5 |
1.1; 1.9 |
|
LLOQ – lower limit of quantification
a Factor VIII activity levels in plasma below the lower limit of quantification (LLOQ) of 0.009 IU/mL were set at half of the LLOQ (0.0045 IU/mL).
b Mixed-effects model of log-transformed factor VIII plasma activity levels, with age group as a fixed effect and patient as a random effect. Separate modeling was performed for each prophylactic treatment regimen (i.e., for each dosing frequency). The minimum level was back-transformed to the natural scale.
Only pre-dose measurements obtained at steady state for this prophylactic treatment regimen were included in the analysis.
Preclinical safety data
Preclinical study data indicate no special hazard for humans, considering the results of standard safety and repeat-dose toxicity studies.
Clinical characteristics.
Indications.
Treatment and prophylaxis of bleeding in patients with hemophilia A (hereditary factor VIII deficiency).
Esperoct can be used in all age groups of patients.
Contraindications.
Hypersensitivity to the active substance or to any of the excipients of the medicinal product (see section "Composition").
Known allergic reaction to hamster proteins.
Interaction with other medicinal products and other forms of interaction.
There are no reports of interactions between recombinant coagulation factor VIII (rDNA) and other medicinal products.
Special precautions for use.
Traceability
In order to improve the traceability of biological medicinal products, the name and batch number of the administered product must be clearly recorded.
Hypersensitivity
Hypersensitivity reactions of an allergic type may occur during administration of Esperoct. This medicinal product contains traces of hamster proteins which may cause allergic reactions in some patients. Patients should be advised to discontinue use immediately and contact their physician if symptoms of hypersensitivity occur. Patients should be informed about early signs of hypersensitivity, including allergic rash, generalized urticaria, chest tightness, wheezing, hypotension, and anaphylaxis.
In the event of shock, standard treatment for shock should be initiated.
Inhibitors
A known complication in the treatment of patients with haemophilia A is the development of neutralizing antibodies (inhibitors) to factor VIII. These inhibitors are typically IgG immunoglobulins directed against the procoagulant activity of factor VIII, quantitatively measured in Bethesda units (BU) per 1 mL of plasma using a modified quantitative assay method. The risk of inhibitor development depends on the severity of the disease and the level of exposure to factor VIII, with the highest risk occurring during the first 50 exposure days. However, the risk persists throughout life, albeit infrequently.
The clinical significance of inhibitor development depends on the inhibitor titer: lower titers are associated with a lower risk of inadequate clinical response compared to higher titers. Overall, all patients receiving factor VIII clotting factor products should be closely monitored clinically and through appropriate laboratory testing to detect inhibitor formation. If expected plasma factor VIII activity levels are not achieved or if bleeding cannot be controlled with appropriate dosing, testing for factor VIII inhibitors should be performed. In patients with high inhibitor titers, therapy with factor VIII may be ineffective, and alternative treatment options should be considered.
Management of such patients should be performed by physicians experienced in the treatment of haemophilia and factor VIII inhibitor management.
Decreased factor VIII activity in previously treated patients
Post-marketing reports have described decreased factor VIII activity in the absence of detectable factor VIII inhibitors in previously treated patients. Decreased factor VIII activity has been observed during transition to Esperoct and, in some cases, may be associated with antibodies to PEG. Appropriate factor VIII activity monitoring should be considered after switching. For additional information, see section "Adverse reactions".
Cardiovascular events
In patients with pre-existing cardiovascular risk factors, replacement therapy with factor VIII may increase cardiovascular risk.
Catheter-related complications
If a central venous access device (CVAD) is required, the potential risk of CVAD-related complications should be considered, including local infections, bacteremia, and catheter site thrombosis.
Paediatric population
The aforementioned warnings and precautions apply to both adult and paediatric patients.
Decreased incremental recovery (IR) of factor VIII levels in previously untreated patients
In clinical trials, decreased incremental recovery (IR) of factor VIII levels in the absence of detectable factor VIII inhibitors was observed in 31 out of 59 previously untreated patients. Of these, 14 patients had only one measurement of low incremental recovery (IR), while 17 patients had two or more consecutive low IR measurements within 5–10 exposure days. The decreased IR was transient, and by 15–70 exposure days, incremental recovery returned to a level > 0.6 (IU/dL)/(IU/kg). Decreased IR was associated with increased titers of anti-polyethylene glycol antibodies (anti-PEG IgG) in previously untreated patients without development of factor VIII inhibitors. Repeated low IR values may potentially be associated with reduced drug efficacy during this period. Monitoring of paediatric patients, including post-infusion factor VIII activity monitoring, is recommended. If bleeding is not controlled or expected factor VIII activity levels are not achieved with the recommended dose of Esperoct in the absence of factor VIII inhibitors, consideration should be given to dose adjustment, increased dosing frequency, or discontinuation of the medicinal product.
Excipients
This medicinal product contains 30.5 mg of sodium per vial of reconstituted product, equivalent to 1.5% of the World Health Organization (WHO) recommended maximum daily intake of sodium – 2.0 g – for an adult.
Use during pregnancy or breastfeeding.
Reproductive studies with factor VIII in animals have not been conducted. Haemophilia A in women is rare; therefore, experience with factor VIII use during pregnancy and lactation is lacking. Consequently, factor VIII should be used during pregnancy and lactation only if clearly indicated.
Effect on ability to drive and use machines.
Esperoct has no or negligible effect on the ability to drive or operate machinery.
Administration and Dosage
Treatment should be initiated under the supervision of a physician experienced in the management of hemophilia.
Monitoring During Treatment
Appropriate monitoring of factor VIII activity levels is recommended throughout treatment to allow for adjustment of the dosing regimen of Esperoct if necessary. Individual patients may respond differently to factor VIII, as reflected by variations in half-life and incremental recovery (IR). Dose adjustments based on body weight may be required for patients with underweight or overweight conditions. During major surgical procedures, replacement therapy with factor VIII should be closely monitored by measuring factor VIII activity in plasma.
Factor VIII activity in Esperoct can be measured using standard chromogenic and one-stage clotting factor VIII assays. When using the one-stage clotting assay based on activated partial thromboplastin time (aPTT) in vitro for determining factor VIII activity in patient blood samples, results may significantly depend on both the type of aPTT reagent and the reference standard used in the assay.
When using the one-stage clotting assay, certain silicon-based reagents should be avoided, as they may lead to falsely low results. Furthermore, considerable discrepancies may occur between results obtained by the one-stage aPTT-based clotting assay and the chromogenic assay according to the European Pharmacopoeia. This is particularly important when changing analytical laboratories and/or reagents used for testing.
Dosage
The dose, dosing interval, and duration of replacement therapy depend on the severity of factor VIII deficiency, the location and severity of bleeding, the target factor VIII activity level, and the patient's clinical condition. The amount of administered factor VIII is expressed in International Units (IU), referenced to the WHO standard for factor VIII medicinal product concentrates. Factor VIII activity in plasma is expressed either as a percentage (relative to normal human plasma levels) or in International Units per deciliter (relative to the WHO standard for factor VIII in plasma).
One International Unit (IU) of factor VIII activity corresponds to the amount of factor VIII present in 1 ml of human plasma.
On-Demand Treatment and Treatment of Bleeding Episodes
The required factor VIII dose is based on the empirically derived observation that 1 IU of factor VIII per kilogram of body weight raises plasma factor VIII activity by 2 IU/dL.
The required dose can be calculated using the following formula:
Required dose (IU) = body weight (kg) × desired increase in factor VIII level (%) (IU/dL) × 0.5 (IU/kg per IU/dL).
The required dose and frequency of administration should always be adjusted according to the individual clinical response in each patient.
Dosage recommendations for Esperoct in on-demand treatment and management of bleeding episodes are provided in Table 5. Factor VIII activity levels should be maintained at or above the indicated levels in plasma (in IU/dL or as % of normal). In the treatment of bleeding episodes, the maximum single dose of 75 IU/kg and the maximum total daily dose of 200 IU/kg/24 hours may be used.
Table 5. Recommendations for Treatment of Bleeding Episodes with Esperoct
| Severity of bleeding |
Required factor VIII level (IU/dL or % of normal) |
Dosing frequency (hours) |
Duration of therapy |
| Mild Early hemarthrosis, mild muscle or oral bleeding |
20–40 |
12–24 |
Until bleeding stops |
| Moderate More extensive hemarthrosis, muscle bleeding, hematoma |
30–60 |
12–24 |
Until bleeding stops |
| Severe or life-threatening bleeding |
60–100 |
8–24 |
Until the threat is resolved |
a The required dose is calculated using the following formula:
Required number of units (IU) = body weight (kg) × desired increase in factor VIII level (%) (IU/dL) × 0.5 (IU/kg per IU/dL).
Use in perioperative administration
The dose level and dosing interval during surgery depend on the surgical procedure performed and local practice. The maximum single dose of Esperoct 75 IU/kg and the maximum total dose of 200 IU/kg/24 hours may be used.
The dosing frequency and duration of therapy must always be individually adjusted according to the clinical response in each individual patient.
Table 6 provides general dosing recommendations for Esperoct in perioperative administration. Maintenance of factor VIII activity at or above the target range should be ensured.
Table 6. Dosing recommendations for Esperoct in perioperative administration
| Type of surgical procedure |
Required level of factor VIII (IU/dL (%) (IU/dL)a |
Dosing frequency (hours) |
Duration of therapy |
| Minor surgery (including tooth extraction) |
30–60 |
Within one hour before surgery. If necessary, repeat after 24 hours. |
Single or repeated injection every 24 hours for at least one day until healing is achieved. |
| Major surgery |
80–100 (before and after surgery) |
Within one hour before surgery to achieve factor VIII activity within the target range. Repeat every 8–24 hours to maintain factor VIII activity within the target range. |
Repeat injection every 8–24 hours as needed for acceptable wound healing. Consider continuing therapy for an additional 7 days to maintain factor VIII activity between 30% and 60% (IU/dL). |
a The required dose is calculated using the following formula:
Required number of units (IU) = body weight (kg) × desired increase in factor VIII level (%) (IU/dL) × 0.5 (IU/kg per IU/dL).
Prophylaxis
The recommended dose of Esperoct for adults is 50 IU per kilogram of body weight administered every 4 days.
Dose adjustments and modification of dosing intervals may be considered based on achieved factor VIII levels and individual bleeding tendencies.
Children
The recommended dose for children (aged 12 years and older) is the same as for adults.
The recommended dose for prophylaxis in children under 12 years of age is 65 IU per 1 kg of body weight (50–75 IU/kg) twice weekly. Dose and frequency adjustments depend on achieved factor VIII levels and individual bleeding tendency.
For more detailed information regarding pediatric patients, refer to the sections "Special precautions", "Pharmacodynamics", and "Pharmacokinetics".
Method of administration
Esperoct is intended for intravenous use.
Esperoct should be administered by intravenous injection (over approximately 2 minutes) after reconstitution of the powder with 4 mL of diluent supplied with the product (sodium chloride, 9 mg/mL (0.9%) solution for injection).
Instructions for reconstituting the medicinal product prior to administration are provided below in the section "Handling and disposal precautions".
Handling and disposal precautions
Esperoct should be administered intravenously after reconstitution of the powder with the diluent contained in the syringe. After reconstitution, the solution should appear as a clear, colorless liquid without visible particles. Before administration, the reconstituted medicinal product should be visually inspected for presence of particulate matter and discoloration. The solution must be clear and colorless. Do not use the solution if it is cloudy or contains a precipitate.
Instructions for reconstituting the medicinal product prior to administration are provided in the section "Instructions for use of Esperoct".
The infusion rate should be adjusted according to patient comfort and should take approximately 2 minutes.
An infusion set (butterfly needle with tubing), sterile alcohol swabs, gauze pads, and adhesive bandage will also be required. These devices are not included in the Esperoct package.
Always use aseptic technique.
Disposal
After injection, safely dispose of the syringe, infusion set, vial, and vial adapter.
Any unused medicinal product or waste material must be disposed of in accordance with local requirements.
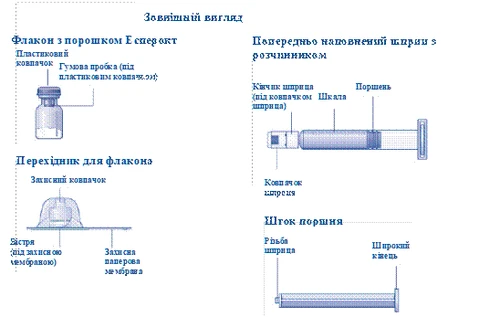
| Instructions for Use of Esperoct Please read this instruction carefully before using Esperoct. Esperoct is supplied as a powder. Before injection, it must be reconstituted using the diluent provided in the syringe. This diluent is 9 mg/mL (0.9%) sodium chloride solution for injection. The reconstituted product must be administered intravenously (IV injection). The equipment provided in this pack is intended for reconstitution and administration of Esperoct. You will also need:
These items are not included in the Esperoct packaging. Do not use the equipment unless you have received proper training from your doctor or nurse. Always wash your hands and ensure a clean working area. When preparing and administering a medication directly into a vein, it is important to use aseptic techniques to maintain sterility. Failure to follow these techniques may result in microbial contamination and bloodstream infection. Do not open the equipment until you are ready to use it. Do not use the equipment if it has been dropped or damaged. In such case, use a new pack. Do not use the equipment after its expiration date. In such case, use a new pack. The expiration date is printed on the carton, vial, vial adapter, and prefilled syringe. Do not use the equipment if you suspect it is contaminated. In such case, use a new pack. Do not dispose of any components until after you have completed the injection of the reconstituted solution. This equipment is intended for single use only. |
|
| Contents The pack contains:
|
|
|
|
|
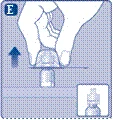
Do not use any other method to warm the vial and prefilled syringe. |
|
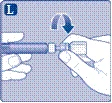
Do not touch the rubber stopper with your fingers, as this may introduce microbes. |
|
If the protective paper membrane is not fully attached or is torn, do not use this vial adapter. Do not remove the vial adapter from its protective cap with your fingers. If you touch the spike of the vial adapter, microbes from your fingers may be introduced. |
|
Once the vial adapter is attached to the vial, do not remove it from the vial. |
|
Do not detach the vial adapter from the vial while removing the protective cap. |
|
|
|
Do not touch the tip of the syringe under the cap. Touching the syringe tip may introduce microbes from your fingers. If the plastic cap is loose or missing, do not use this prefilled syringe. |
|
|
|
|
|
Do not shake the vial, as this may cause foaming.
|
|
| Esperoct should be used immediately after reconstitution. If you cannot use the reconstituted Esperoct solution immediately, it must be used:
The reconstituted solution should be stored in the vial. Do not freeze the reconstituted solution and do not store it in syringes. Keep the reconstituted solution protected from direct sunlight. If more than one vial is required to achieve your dose, repeat steps A through J with additional vials, vial adapters, and prefilled syringes until you obtain the required dose as instructed by your doctor or nurse. |
|
|
|
Do not touch the tip of the syringe. Touching the syringe tip may introduce microbes from your fingers. |
|
The Esperoct product is now ready for intravenous injection.
Do not mix Esperoct with any other intravenous injections or medications. Administration of Esperoct through needle-free intravenous (IV) connectors. Caution! The prefilled syringe is made of glass and is designed for use with standard Luer-lock connections. Some needle-free connectors with internal spikes are incompatible with this prefilled syringe. Such incompatibility may prevent medication delivery and may damage the needle-free connector. Administration through a central venous access device (CVAD), such as a central venous catheter or implanted port:
If the CVAD system needs to be flushed before or after administration of Esperoct, use 9 mg/mL (0.9%) sodium chloride injection solution. |
|
| Disposal.
Do not dispose of these materials in household waste. |
|
| Do not disassemble the equipment before disposal. Do not reuse this equipment. |
|











Children
Treatment and prophylaxis of bleeding in patients with hemophilia A (hereditary factor VIII deficiency).
Esperoct can be used in all age groups.
Detailed information regarding pediatric patients is provided in sections "Pharmacological properties" (subsections "Pharmacodynamics" and "Pharmacokinetics"), "Special precautions for use", "Dosage and administration".
Overdose.
Reports of symptoms related to overdose with recombinant blood coagulation factor VIII have not been recorded.
Adverse reactions.
Summary of safety profile
Hypersensitivity or allergic reactions (including angioedema, burning and stinging at the infusion site, chills, flushing, generalized urticaria, headache, allergic rash, hypotension, somnolence, nausea, restlessness, tachycardia, chest tightness, tingling sensation, vomiting, wheezing) were observed rarely and in some cases could progress to severe anaphylaxis (including shock).
Formation of antibodies to hamster proteins with corresponding hypersensitivity reactions was observed very rarely.
In patients with haemophilia A treated with factor VIII, including Esperoct, neutralizing antibodies (inhibitors) may develop. If such inhibitors form, this is manifested by a suboptimal clinical response to treatment. In such cases, consultation with a specialized haemophilia treatment centre is recommended.
List of adverse reactions
Data on the frequency of adverse reactions were obtained from six clinical studies involving 270 previously treated patients and 81 previously untreated patients with severe haemophilia A (< 1% endogenous factor VIII activity) and no history of factor VIII inhibitors, as shown in Table 7. The adverse reaction categories listed below are classified according to MedDRA system organ classes (SOC) and preferred terms (PT), as specified in Table 7.
The frequency of adverse reactions was assessed using the following categories: very common (≥ 1/10), common (≥ 1/100 to < 1/10), uncommon (≥ 1/1,000 to < 1/100), rare (≥ 1/10,000 to < 1/1,000), very rare (< 1/10,000); frequency not known (cannot be estimated based on available data). The adverse reactions listed below occurred in previously treated patients.
Table 7. Frequency of adverse reactions observed during clinical studies
| System organ classification |
Preferred terms |
Frequency (previously treated patients) |
Frequency (previously untreated patients) |
| Blood and lymphatic system disorders |
Inhibition of factor VIII * |
Uncommon |
Very common** |
| Skin and subcutaneous tissue disorders |
Pruritus |
Common |
- |
| Erythema |
Common |
Common |
|
| Rash |
Common |
Common |
|
| General disorders and administration site reactions |
Injection site reactions*** |
Common |
Common |
| Immune system disorders |
Hypersensitivity to medicinal product |
- |
Common |
| Hypersensitivity |
Uncommon |
- |
|
| Investigations |
Decreased factor VIII level |
Unknown**** |
- |
* A patient with confirmed factor VIII inhibitor was defined based on an initial inhibitor test result ≥ 0.6 Bethesda units (BU), confirmed by a second sample obtained no later than 2 weeks later.
** Includes patients with confirmed factor VIII inhibitor among patients in the risk group (at least 10 days of product exposure).
*** Preferred terms included injection site reactions: injection site reaction, vessel puncture site hematoma, infusion site reaction, injection site erythema, injection site rash, vessel puncture site pain, and injection site swelling.
**** Based on post-marketing reports.
Description of selected adverse reactions
Formation of factor VIII inhibitors
One confirmed case of factor VIII inhibitor development was reported during prophylactic treatment with Esperoct in an 18-year-old previously treated patient. The patient had intron 22 inversion in the factor VIII gene and a high risk of developing factor VIII inhibitors.
There is no evidence indicating an increased risk of factor VIII inhibitor formation with Esperoct compared to other factor VIII products.
Development of antibodies to the medicinal product
One case of development of persistent antibodies to the medicinal product was reported, which temporally coincided with the confirmed case of factor VIII inhibitor development (see section on factor VIII inhibitor development). In three patients, test results for antibodies to Esperoct were transiently positive after administration of Esperoct, but no correlation with adverse reactions was observed.
Antibodies to PEG
During the clinical trial program, 37 patients had anti-PEG antibodies prior to Esperoct administration. The anti-PEG antibody test became negative after treatment in 20 out of these 37 patients. Transient low-titer anti-PEG antibodies were detected in 17 patients. No correlation with adverse events was observed.
According to post-marketing reports, anti-PEG antibodies have also been observed during transition to Esperoct. In some patients, anti-PEG antibodies may be associated with lower than expected FVIII activity levels.
Pediatric population
No differences in the safety profile were observed between previously treated pediatric and adult patients.
Transient reduction in factor VIII incremental recovery (IR) was observed in some previously untreated patients in the absence of factor VIII inhibitors (further details provided in section "Special instructions").
Reporting of suspected adverse reactions and lack of efficacy
Reporting suspected adverse reactions after marketing authorization is important. It allows continued monitoring of the benefit-risk balance of the medicinal product. Healthcare professionals, patients, and their legal representatives should report all suspected adverse reactions and lack of efficacy via the Automated Pharmacovigilance Information System at: https://aisf.dec.gov.ua.
Shelf life.
Unopened vial (prior to reconstitution):
36 months when stored in the refrigerator (2–8 °C).
During the shelf life, the product may be stored:
- at room temperature (≤ 30 °C) from the time of manufacture until reconstitution for no more than 12 months
or
- above room temperature (from > 30 °C to 40 °C) from the time of manufacture until reconstitution for no more than 3 months.
Once the product has been stored outside the refrigerator, it must not be returned to the refrigerator.
The date of removal from refrigeration and storage temperature must be recorded in the designated space on the carton.
After reconstitution:
Chemical and physical in-use stability has been demonstrated:
- for 24 hours when stored in the refrigerator (2–8 °C), or
- for 4 hours at ≤ 30 °C, or
- for 1 hour at temperatures from > 30 °C to 40 °C, provided that prior to reconstitution the product was stored at temperatures above room temperature (from > 30 °C to 40 °C) for no more than 3 months.
From a microbiological point of view, the product should be used immediately after reconstitution. If the reconstituted product is not used immediately, the responsibility for storage conditions and duration lies with the user; storage should not exceed the periods specified above, except when reconstitution is performed under controlled and validated aseptic conditions.
The reconstituted solution should be stored in the vial.
Storage conditions.
Store in a refrigerator (2–8 °C). Do not freeze. Store in the original packaging to protect from light.
For information on storage at room temperature (≤ 30 °C) or up to 40 °C, and conditions after reconstitution, refer to the section "Shelf life." Keep out of the reach of children.
Incompatibilities.
Since compatibility studies have not been conducted, this medicinal product must not be mixed with other medicinal products or reconstituted using other injection solutions except for the diluent provided in the pack—sodium chloride solution.
The reconstituted product must not be administered simultaneously with other medicinal products through the same infusion set or via the same container already used for other medicinal products.
Packaging.
Each carton package of Esperoct contains:
- 1 glass vial (Type I glass) containing powder, closed with a chlorobutyl stopper, aluminum cap, and flip-off plastic cap;
- 1 sterile vial adapter for reconstitution;
- 1 pre-filled syringe with 4 mL diluent (0.9% sodium chloride solution) with a reverse plunger (polypropylene), rubber plunger (bromobutyl), and rubber cap (bromobutyl);
- 1 plunger rod (polypropylene).
Prescription status. Prescription only.
Marketing Authorization Holder/Manufacturer.
A/T Novo Nordisk.
Address of the Marketing Authorization Holder/Manufacturer and location of its operations.
Novo Allé,
Bagsværd, 2880,
Denmark.