Nuwik / nuwiq®
Ukraine
Table of Contents
- INSTRUCTIONS FOR MEDICAL USE OF THE MEDICINAL PRODUCT NUWIQ®
- Composition:
- Pharmacological properties.
- Clinical characteristics.
- Special precautions for use.
- Administration and Dosage
- Adverse Reactions
- Frequency is based on studies with all factor VIII products that included patients with severe hemophilia A.
INSTRUCTIONS FOR MEDICAL USE OF THE MEDICINAL PRODUCT NUWIQ®
Composition:
Active substance: simoctocog alfa (recombinant coagulation factor VIII);
1 vial of powder for solution for injection contains simoctocog alfa (recombinant coagulation factor VIII) 1500 IU, or 2500 IU, or 3000 IU, or 4000 IU;
Excipients: sodium chloride; sucrose; L-arginine hydrochloride; calcium chloride dihydrate; poloxamer 188; sodium citrate dihydrate.
Solvent: water for injections.
Pharmaceutical form. Powder and solvent for solution for injection.
Main physicochemical properties:
Powder: white cake. A small amount of white powder may be present.
Solvent: clear, colorless liquid, free from particles.
Pharmacotherapeutic group. Antihemorrhagics. Coagulation factor VIII.
ATC code B02BD02.
Pharmacological properties.
Pharmacodynamics.
Blood coagulation factor VIII binds to von Willebrand factor in the patient's circulation. Activated factor VIII acts as a cofactor for activated factor IX, reducing the time required for conversion of factor X into activated factor X. Activated factor X then converts prothrombin into thrombin. Thrombin subsequently converts fibrinogen into fibrin, leading to clot formation.
Hemophilia A is a hereditary, sex-linked disorder caused by congenital deficiency of coagulation factor VIII:C, resulting in bleeding into joints, muscles, and internal organs, occurring either spontaneously or following accidental or surgical trauma. Replacement therapy increases factor VIII levels in plasma, thereby temporarily correcting the deficiency of blood coagulation factor VIII and reducing the tendency to bleed.
Adult population and patients aged 12–65 years.
Prophylaxis: In a clinical trial involving 32 adult patients with severe hemophilia A, the mean prophylactic dose of the medicinal product Nuwiq was 468.7 IU/kg/month. Bleeding treatment: The mean dose for treating bleeding episodes in patients receiving prophylaxis was 33.0 IU/kg. In another clinical trial, 22 adult patients received on-demand treatment. A mean dose of 30.9 IU/kg was administered in a total of 986 bleeding episodes. Overall, minor bleeding episodes required lower doses, while major bleeding episodes required approximately three times higher mean doses.
Individualized prophylaxis: Individualized prophylaxis based on pharmacokinetic (PK) assessment was evaluated in 66 previously treated adult patients (PTPs) with severe hemophilia A. After a 1- to 3-month standard prophylaxis phase (receiving doses every other day or three times weekly), 44 (67%) patients transitioned to a dosing regimen based on individual PK assessment, and 40 patients completed 6 months of prophylaxis according to the prescribed dosing regimen. Of these patients, 34 (85%) received treatment twice weekly or less frequently. Thirty-three (82.5%) patients experienced no bleeding episodes, and 36 (90.0%) patients had no spontaneous bleeding episodes. The mean + SD annualized (calculated on a yearly basis) bleeding rate (ABR) was 1.2 + 3.9, and the mean + SD dose was 52.2 + 12.2 IU/kg per injection and 99.7 + 25.6 IU/kg per week.
It should be noted that the annualized bleeding rate (ABR) is not comparable across different factor concentrates or between different clinical trials.
Paediatric population
Data were obtained from 29 previously treated children aged 2 to 5 years, 31 children aged 6 to 12 years, and one adolescent aged 14 years. The mean prophylactic injectable dose was 37.8 IU/kg. Twenty patients received mean doses exceeding 45 IU/kg. The mean monthly prophylactic dose of the medicinal product Nuwiq was 521.9 IU/kg. Children received a higher mean dose of Nuwiq for bleeding treatment (43.9 IU/kg) compared to adults (33.0 IU/kg), as well as higher mean doses for treating both minor and major bleeding episodes (78.2 IU/kg vs. 41.7 IU/kg). Younger children generally required higher mean doses (6–12 years: 43.9 IU/kg; 2–5 years: 52.6 IU/kg). These findings were confirmed during long-term follow-up of 49 such children, who were treated for an additional mean period of approximately 30 months (range: 9.5 to 52 months); during this period, 45% of the children had no spontaneous bleeding episodes.
Data from 108 previously untreated patients with severe hemophilia A (˂1% FVIII:C) were obtained in a prospective, open-label clinical trial. In most patients, prophylactic treatment was initiated after the first bleeding episode requiring treatment.
Pharmacokinetics.
Adult population
Table 1.
Pharmacokinetic parameters of the medicinal product Nuwiq (50 IU/kg dose) in adults aged 18 to 65 years with severe hemophilia A who had been previously treated (n=20).
| Pharmacokinetic parameters |
Chromogenic assay |
|
| Mean ± SD |
Median (range) |
|
| AUC (hr*MO/mL) |
22.6 ± 8.0 |
22.3 (8.4 – 38.1) |
| T 1/2 (hr) |
14.7 ± 10.4 |
12.5 (5.4 – 55.6) |
| IVR (%/MO/kg) |
2.5 ± 0.4 |
2.5 (1.7 – 3.2) |
| CL (mL/hr/kg) |
3.0 ± 1.2 |
2.7 (1.5 – 6.4) |
AUC - area under the curve (FVIII:C), T½ - half-life
IVR - in vivo recovery, CL - clearance, SD - standard deviation
Table 2.
Pharmacokinetic parameters of Nuwiq administered at a dose of 50 IU/kg in children aged 6 to 12 years with severe haemophilia A, who had been previously treated (n=12).
| Pharmacokinetic parameters |
Chromogenic assay |
|
| Mean ± SD |
Median (range) |
|
| AUC (hr*IU/mL) |
13.2 ± 3.4 |
12.8 (7.8 – 19.1) |
| T 1/2 (hr) |
10.0 ± 1.9 |
9.9 (7.6 – 14.1) |
| IVR (%/IU/kg) |
1.9 ± 0.4 |
1.9 (1.2 – 2.6) |
| CL (mL/hr/kg) |
4.3 ± 1.2 |
4.2 (2.8 – 6.9) |
AUC - area under the curve (FVIII:C), T½ - half-life
IVR - in vivo recovery, CL - clearance, SD - standard deviation
Table 3.
Pharmacokinetic parameters of Nuwiq administered at a dose of 50 IU/kg in children aged 2 to 5 years with severe haemophilia A, who were previously treated (n = 13).
| Pharmacokinetic parameters |
Chromogenic assay |
|
| Mean ± SD |
Median (range) |
|
| AUC (hr*MU/mL) |
11.7 ± 5.3 |
10.5 (4.9 – 23.8) |
| T 1/2 (hr) |
9.5 ± 3.3 |
8.2 (4.3 – 17.3) |
| IVR (%/MU/kg) |
1.9 ± 0.3 |
1.8 (1.5 – 2.4) |
| CL (mL/hr/kg) |
5.4 ± 2.4 |
5.1 (2.3 – 10.9) |
AUC - area under the curve (FVIII:C), T½ - half-life
IVR - in vivo recovery, CL - clearance, SD - standard deviation
Paediatric population
According to published data, recovery and half-life values were lower in younger children compared to adults, while clearance values were higher, which may be partially explained by a larger plasma volume per kilogram of body weight in younger patients.
Subgroups by body weight
Table 4.
Pharmacokinetic parameters of Nuwiq (dose 50 IU/kg) in adults aged 18 to 65 years with severe haemophilia A, previously treated (n=20), by patient body weight
| Pharmacokinetic parameters |
All patients (n =20) |
Normal body weight (n =14) |
Pre-obese state (n =4) |
Obesity (n =2) |
| Chromogenic assay, mean ± SD |
||||
| AUC (h*IU/mL) |
22.6 ± 8.0 |
20.4 ± 6.9 |
24.9 ± 8.9 |
33.5 ± 6.5 |
| T 1/2 (h) |
14.7 ± 10.4 |
14.7 ± 12.1 |
13.4 ± 5.9 |
17.2 ± 4.8 |
| IVR (%/IU/kg) |
2.5 ± 0.4 |
2.4 ± 0.4 |
2.7 ± 0.4 |
2.8 ± 0.3 |
| CL (mL/h/kg) |
3.0 ± 1.2 |
3.2 ± 1.3 |
2.6 ± 1.0 |
1.8 ± 0.4 |
| Chromogenic assay, median (range) |
||||
| AUC (h*IU/mL) |
22.3 (8.4 – 38.1) |
21.2 (8.4– 32.6) |
23.3 (17.4 – 35.5) |
33.5 (28.9 – 38.1) |
| T 1/2 (h) |
12.5 (5.4 – 55.6) |
12.3 (5.4– 55.6) |
11.2 (9.3 – 22.0) |
17.2 (13.8 – 20.6) |
| IVR (%/IU/kg) |
2.5 (1.7 – 3.2) |
2.4 (1.7 – 3.1) |
2.8 (2.3 – 3.2) |
2.8 (2.6 – 3.0) |
| CL (mL/h/kg) |
2.7 (1.5 – 6.4) |
2.8 (1.7 – 6.4) |
2.5 (1.6 – 3.7) |
1.8 (1.5 – 2.0) |
Normal body weight BMI - 18.5 – 25 kg/m², Increased body weight: BMI 25 – 30 kg/m², Obesity: BMI > 30 kg/m², SD - standard deviation
Clinical characteristics.
Indications.
Treatment and prevention of bleeding in patients with hemophilia A (congenital factor VIII deficiency).
Nuwiq can be used in patients of all age groups.
Contraindications.
Hypersensitivity to the active substance or to any of the excipients of the medicinal product.
Interaction with other medicinal products and other forms of interaction.
No studies on interactions between Nuwiq and other medicinal products have been conducted.
Special precautions for use.
Traceability
To improve traceability of biological medicinal products, the name and batch number of the administered product should be clearly recorded.
The specific activity of Nuwiq is approximately 9500 IU/mg protein.
Simoctocog alfa (recombinant DNA coagulation factor VIII) is a pure protein consisting of 1440 amino acids. The amino acid sequence is similar to the 90+80 kDa form of human factor VIII plasma (i.e., with the B-domain deleted). Nuwiq is produced using recombinant DNA technology in genetically modified human embryonic kidney (HEK) 293F cells. During manufacturing and in the final medicinal product, no materials of animal or human origin are added.
Increased sensitivity
As with any intravenous protein product, there is a possibility of developing allergic reactions and hypersensitivity. Nuwiq contains trace amounts of human cell proteins that differ from factor VIII. If symptoms of hypersensitivity occur, administration of the medicinal product should be stopped immediately and medical attention sought. Patients should be informed about early signs of hypersensitivity reactions, such as urticaria, generalized urticaria, sensation of chest tightness, difficulty breathing, wheezing, arterial hypotension, and anaphylaxis.
In case of shock, standard medical treatment for shock should be initiated.
Inhibitors
Development of neutralizing antibodies (inhibitors) against factor VIII is a known complication in the treatment of patients with haemophilia A. These inhibitors are typically immunoglobulins IgG directed against the procoagulant activity of factor VIII and are quantified in Bethesda Units (BU) per 1 mL of plasma using a modified assay. The risk of inhibitor development correlates with the severity of the disease and depends on exposure to factor VIII, being highest during the first 50 exposure days, but persists throughout life, although the risk is rare.
Cases of recurrent inhibitor formation (low titer) have been observed when switching from one recombinant factor VIII product to another in patients who had previously received treatment for more than 100 days and who had a history of inhibitor development. Therefore, careful monitoring for inhibitor formation is recommended in all patients following any change in medicinal product.
The clinical significance of inhibitor formation depends on the inhibitor titer: low-titer inhibitors, whether transient or persistently low, pose a lower risk of inadequate clinical response compared to high-titer inhibitors.
Careful monitoring of all patients receiving treatment with recombinant factor VIII is required through appropriate clinical observation and laboratory testing. If expected plasma factor VIII activity levels are not achieved or if bleeding is not controlled with an appropriate dose of the product, assays should be performed to determine the presence of factor VIII inhibitors. In patients with high-titer inhibitors, factor VIII therapy may be ineffective, and alternative therapeutic options such as immune tolerance induction (ITI) should be considered. Treatment of such patients should be managed by physicians experienced in the treatment of haemophilia and factor VIII inhibitor management.
Cardiovascular complications
In patients with existing risk factors for cardiovascular disease, replacement therapy with FVIII may increase the risk of cardiovascular events.
Complications associated with catheter use
If a central venous access device (CVAD) is required, the risk of complications related to its use, including local infections, bacteremia, and catheter-related thrombosis, should be considered.
It is strongly recommended that the name and batch (lot) number of the Nuwiq medicinal product be recorded each time the product is administered to establish a link between the patient's condition and the administered batch.
All warnings apply to both adults and children.
Information on excipients (sodium content)
1 mL of reconstituted solution contains 7.35 mg (18.4 mg sodium per vial), which is essentially "sodium-free."
However, depending on body weight and dosage, a patient may receive more than one vial. This information should be considered for patients on a sodium-controlled diet.
Use during pregnancy or breastfeeding.
Studies on the effect of Nuwiq on reproductive function in animals have not been conducted. Since haemophilia A is rare in women, experience with the use of Nuwiq during pregnancy and breastfeeding is lacking. Therefore, Nuwiq may be prescribed during pregnancy and breastfeeding when clinically indicated and in cases of urgent need. Data on effects on fertility are not available.
Ability to affect reaction speed when driving or operating machinery.
No effects on the ability to drive or operate machinery have been observed.
Administration and Dosage
Treatment should be administered under the supervision of a physician experienced in the management of hemophilia.
Monitoring of Treatment
During the course of treatment, appropriate monitoring of factor VIII levels is recommended to control the required dose and frequency of repeat infusions. Individual patients may exhibit varying responses to factor VIII administration, showing differences in half-life and recovery (restoration). Dose adjustments based on body weight may be necessary in cases of significantly low or high body weight. In the case of major surgical intervention, precise monitoring of replacement therapy using coagulation assays (plasma factor VIII activity) is mandatory.
When using a one-stage assay for coagulation activity based on activated partial thromboplastin time (aPTT) in vitro to determine factor VIII activity in patient blood samples, both the type of aPTT reagent and the standard reference material used in the assay may significantly influence the resulting factor VIII activity values. Moreover, considerable discrepancies may occur between results obtained by the one-stage aPTT-based coagulation assay and those obtained by chromogenic assay according to the European Pharmacopoeia. This is particularly important, especially when changing laboratories and/or reagents used in the assay.
Administration Method
The dosage and duration of replacement therapy depend on the severity of factor VIII deficiency, the location and extent of bleeding, and the patient's clinical condition.
The amount of factor VIII administered is expressed in International Units (IU), calibrated against the WHO standard for factor VIII pharmaceutical products. Factor VIII activity in plasma is measured either in percentages (relative to normal human plasma) or, preferably, in International Units (according to the International Standard for factor VIII in plasma).
1 International Unit (IU) of factor VIII activity is equivalent to the amount of factor VIII present in 1 ml of normal human plasma.
Treatment as Needed
Calculations for the required dose of factor VIII are based on empirical data indicating that 1 International Unit (IU) of factor VIII per 1 kg of body weight raises plasma factor VIII activity by approximately 2% (or 2 IU/dL) from baseline. The required dose can be calculated using the following formula:
I.
Required units = body weight (kg) × desired rise in factor VIII (%) (IU/dL) × 0.5 (IU/kg per IU/dL)
II.
| Expected rise in factor VIII (% of normal) = |
2 × administered IU |
| body weight (kg) |
II.
The dose to be administered and the frequency of administration should always be adjusted according to the clinical response in each individual case.
In the hemorrhagic situations listed below, factor VIII activity should not fall below the specified plasma activity level (% of normal or IU/dL) during the appropriate period. Table 5 can be used to determine dosing during bleeding episodes and surgery.
Table 5
| Severity of bleeding/ type of surgical procedure |
Required level of factor VIII (%) (IU/dl) |
Dosing frequency (hours)/ duration of therapy (days) |
| Bleeding Early hemarthrosis, muscle or oral bleeding |
20–40 |
Repeat every 12–24 hours for at least 1 day until bleeding associated with pain is controlled or until healing is complete |
| More extensive hemarthrosis, muscle bleeding or hematoma |
30–60 |
Repeat every 12–24 hours for 3–4 days or more until pain and acute symptoms have resolved |
| Life-threatening bleeding |
60–100 |
Repeat injections every 8–24 hours until the threat is resolved |
| Surgery Minor surgery, including tooth extraction Major surgery |
30–60 |
Every 24 hours for at least 1 day until complete healing |
| 80–100 (before and after surgical procedure) |
Repeat injections every 8–24 hours until significant wound healing occurs; thereafter continue therapy for at least 7 days to maintain factor VIII activity between 30% and 60% (IU/dl) |
Prophylaxis
For long-term prevention of bleeding episodes in patients with severe hemophilia A, the usual dose is 20 to 40 IU of factor VIII per kg of body weight every 2 to 3 days. In some cases, particularly in younger patients, it may be necessary to increase either the dose or the frequency of administration.
It is recommended to monitor factor VIII levels throughout the course of treatment in order to adjust the dose and frequency of repeat infusions. In the case of major surgery, precise monitoring of replacement therapy through measurement of factor VIII activity in plasma is required. Depending on factor VIII levels, individual patients may exhibit different half-lives and recovery rates. The dosing regimen may be adjusted based on the patient's response.
The route of administration is the same for adults, children, and adolescents; however, for children and adolescents, shorter intervals between doses or higher doses may be required. There are no data available regarding use in children under 2 years of age.
Method of administration
Nuvig is intended for intravenous administration.
It is recommended to administer no more than 4 ml per minute.
Instructions for reconstitution of the medicinal product prior to administration.
The powder should be reconstituted only with the provided diluent (2.5 ml of water for injections) using the supplied injection preparation kit. The vial should be gently swirled until the powder is completely dissolved. After reconstitution, the solution should be drawn into the syringe that contained the diluent.
The prepared solution should be inspected visually for the presence of particulate matter and discoloration prior to administration. The reconstituted solution should be clear, colorless, free of foreign particles, and have a pH between 6.5 and 7.5. Solutions that are cloudy or contain precipitate should not be used.
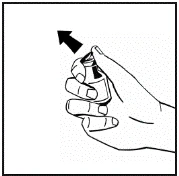
Instructions for preparation and administration of the medication.
|
Fig. 1 |
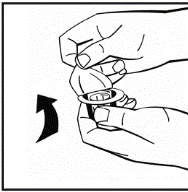
|
Fig. 2 |
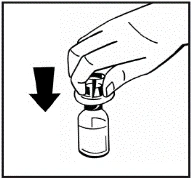
|
Fig. 3 |
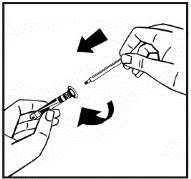
|
Fig. 4 |
|
Fig.5 |
|
Fig.6 |
|
Fig.7 |
|
Fig.8 |
|
|
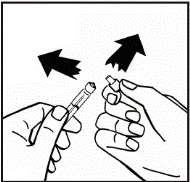
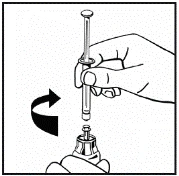
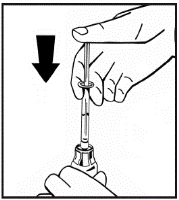
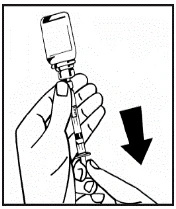
If more than one vial of powder is used for a single procedure, the same injection needle may be reused. The vial adapter and syringe are intended for single use only.
Unused medicinal product and waste materials must be disposed of in accordance with local requirements.
Children.
Nuvik can be used in children of any age; however, there are no data regarding use in children under 2 years of age.
Overdose.
No cases of overdose have been reported.
Adverse Reactions
Summary of Safety Profile
Hypersensitivity and allergic reactions (which may include angioneurotic edema, burning and stinging at the infusion site, chills, flushing, generalized urticaria, headache, urticaria, arterial hypotension, somnolence, nausea, rash, restlessness, tachycardia, dyspnea, paresthesia, urticaria, generalized urticaria, vomiting, wheezing/stridor) have been rarely observed following administration of FVIII factor products, but may in some cases progress to severe anaphylaxis (including shock).
In patients with hemophilia A treated with factor VIII products, including Nuwiq, neutralizing antibodies (inhibitors) to factor VIII may develop. If inhibitors are detected, the cause of their development is considered to be inadequate clinical response manifested by persistent bleeding or recurrent bleeding episodes despite appropriate prophylaxis. In such cases, consultation with a specialized hemophilia treatment center is recommended.
List of adverse reactions in tabular form
Table 6 below is organized by MedDRA (Medical Dictionary for Regulatory Activities) system organ class. The frequency is based on data from clinical trials involving 355 patients with severe hemophilia A, including 247 previously treated patients (PTPs) and 108 previously untreated patients (PUPs).
Frequency categories are defined as follows: very common (≥1/10); common (≥1/100 to <1/10); uncommon (≥1/1000 to <1/100); rare (≥1/10,000 to <1/1000); very rare (<1/10,000); and not known (cannot be estimated from available data).
Within each frequency group, adverse reactions are listed in order of decreasing severity.
Table 6.
| MedDRA Standard System Organ Class |
Adverse Reactions |
Frequency |
| Blood and lymphatic system disorders |
Anaemia Factor VIII inhibition Haemolytic anaemia |
uncommon* uncommon (PTPs)# very common (PUPs)# uncommon* |
| Immune system disorders |
Hypersensitivity |
common* |
| Nervous system disorders |
Dizziness Headache Paraesthesia (sensory disturbance) |
uncommon* uncommon* uncommon* |
| Ear and labyrinth disorders |
Dizziness |
uncommon* |
| Respiratory, thoracic and mediastinal disorders |
Dyspnoea (difficulty breathing) |
uncommon* |
| Gastrointestinal disorders |
Dry mouth |
uncommon* |
| Musculoskeletal and connective tissue disorders |
Back pain |
uncommon* |
| General disorders and administration site conditions |
Pyrexia (fever) Chest pain Injection site inflammation Injection site pain Malaise |
common* uncommon* uncommon* uncommon* uncommon* |
| Investigations |
Positive antibodies without neutralizing activity (in PTPs) |
uncommon* |
*Calculated as the number of patients with adverse reactions divided by the total number of 355 investigated patients, of which 247 patients were previously treated patients (PTPs) and 108 patients were previously untreated patients (PUPs).
Frequency is based on studies with all factor VIII products that included patients with severe hemophilia A.
PTPs = previously treated patients, PUPs = previously untreated patients.
Description of individual adverse reactions
Antibodies to factor VIII antigens without neutralizing activity were detected in one adult patient (see Table 6). The result was positive only in dilution 1, and the antibody titer was very low. Inhibitor activity measured by modified Bethesda assay was not detected in this patient. Clinical efficacy and in vivo recovery of Nuwiq were not affected in this patient.
Children
The frequency, type, and severity of adverse reactions in children are expected to be the same as in adults.
Reporting of potential adverse reactions
Reporting of potential adverse reactions after marketing authorization of a medicinal product is important. This allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals should report potential adverse reactions.
Shelf life.
Powder: 2 years.
Solvent (water for injection): 5 years.
During the entire shelf life, the medicinal product may be stored for up to 1 month at room temperature (up to 25 °C). If the medicinal product has already been removed from the refrigerator, it must not be returned.
The date of commencement of room temperature storage should be indicated on the packaging of the medicinal product.
After reconstitution, chemical and physical stability has been demonstrated for 24 hours when stored at room temperature.
From a microbiological point of view, the medicinal product should be used immediately after reconstitution. If not used immediately, the user is personally responsible for the shelf life and conditions of use of the medicinal product.
Storage conditions.
Powder
Store at 2 to 8 °C. Do not freeze.
Store in the outer carton to protect from light.
Solvent (water for injection)
Store at 2 to 8 °C.
The reconstituted solution should be stored at room temperature.
Do not freeze the reconstituted solution.
Keep out of the reach of children.
Incompatibilities.
Due to the lack of compatibility studies, this medicinal product must not be mixed with other medicinal products.
Only the provided infusion sets should be used, as treatment may fail due to adsorption of coagulation factor VIII onto the internal surfaces of certain infusion devices.
Packaging. 1500 IU, 2500 IU, 3000 IU, or 4000 IU of powder in a vial; 1 vial of powder, 1 pre-filled syringe with 2.5 mL solvent (water for injection), together with a reconstitution and intravenous administration kit (1 vial adapter, 1 butterfly needle, 2 alcohol swabs) in a cardboard box.
Prescription category.
Prescription only.
Manufacturer.
Octapharma AB.
Manufacturer's location and address of place of business.
Lars Forssells gata 23, Stockholm, 11275, Sweden.