L-thyroxine 100 berlin-chemi
Ukraine
Table of Contents
- INSTRUCTION FOR MEDICAL USE OF THE MEDICINAL PRODUCT L-THYROXIN 50 BERLIN-CHEMIE / L-THYROXIN 100 BERLIN-CHEMIE (L-THYROXIN 50 BERLIN-CHEMIE / L-THYROXIN 100 BERLIN-CHEMIE)
- Composition:
- Pharmacological properties.
- Clinical characteristics.
- Special precautions for use.
- Dosage and Administration.
- Adverse reactions.
INSTRUCTION FOR MEDICAL USE OF THE MEDICINAL PRODUCT L-THYROXIN 50 BERLIN-CHEMIE / L-THYROXIN 100 BERLIN-CHEMIE (L-THYROXIN 50 BERLIN-CHEMIE / L-THYROXIN 100 BERLIN-CHEMIE)
Composition:
Active substance: levothyroxine sodium;
One tablet contains 50 mcg or 100 mcg of sodium levothyroxine;
Excipients: cysteine hydrochloride monohydrate (partially present in tablets as cystine); microcrystalline cellulose; pregelatinized starch; corn starch; light magnesium oxide; talc.
Pharmaceutical form. Tablets.
Main physicochemical properties:
L-Thyroxin 50 Berlin-Chemie: round, slightly convex tablets, white to beige in colour, with a score line on one side.
L-Thyroxin 100 Berlin-Chemie: round, slightly convex tablets, white to beige in colour, with a score line on one side.
The tablet can be divided into equal doses.
Pharmacotherapeutic group. Thyroid therapy, thyroid hormones. ATC code H03AA01.
Pharmacological properties.
Pharmacodynamics.
Mechanism of action.
The synthetic levothyroxine contained in L-Thyroxine 50 Berlin-Chemie and L-Thyroxine 100 Berlin-Chemie is identical in action to the natural thyroid hormone primarily produced by the thyroid gland. There are no differences between endogenously produced and exogenous levothyroxine for the organism.
Pharmacodynamic effects.
Following partial conversion to liothyronine (T3), primarily in the liver and kidneys, and entry into body cells, the characteristic effects of thyroid hormones on development, growth, and metabolism are observed via activation of T3 receptors.
Clinical efficacy and safety.
Thyroid hormone replacement leads to normalization of metabolic processes. For example, levothyroxine administration results in a significant reduction of elevated cholesterol levels caused by hypothyroidism.
Pharmacokinetics.
Absorption.
Orally administered levothyroxine is absorbed primarily in the upper segment of the small intestine. The extent of absorption depends mainly on the galenical form of the preparation and may reach up to 80% when administered on an empty stomach. Absorption is significantly reduced if the drug is taken with food.
Maximum plasma concentration is reached approximately 2–3 hours after administration.
The effect of the drug becomes apparent 3–5 days after initiation of oral therapy.
Distribution.
The volume of distribution is approximately 10–12 L. Levothyroxine is approximately 99.97% bound to specific plasma transport proteins. The binding of hormones to proteins is non-covalent, thus allowing for continuous and very rapid exchange between free and bound hormone.
Elimination.
Metabolic clearance of levothyroxine is approximately 1.2 L of plasma per day. Metabolism occurs primarily in the liver, kidneys, brain, and muscles. Metabolites are excreted in urine and feces. The elimination half-life of the drug is approximately 7 days; in hyperthyroidism, this period is shortened (to 3–4 days), whereas in hypothyroidism, it is prolonged (approximately 9–10 days).
Pregnancy and breastfeeding.
Levothyroxine crosses the placenta only in negligible amounts. When administered in usual doses, levothyroxine is excreted in breast milk only in negligible amounts.
Renal impairment.
Due to the high degree of protein binding, neither hemodialysis nor hemoperfusion affects levothyroxine levels.
Clinical characteristics.
Indications.
L-THYROXINE 50 BERLIN-CHEMIE, L-THYROXINE 100 BERLIN-CHEMIE:
- benign goiter with euthyroid function of the thyroid gland;
- prevention of goiter recurrence after resection of goiter with euthyroid function of the thyroid gland;
- replacement therapy in hypothyroidism of various etiologies;
- adjunctive agent in antithyroid therapy of hyperthyroidism after achieving euthyroid functional status;
- suppressive and replacement therapy in thyroid cancer, primarily after thyroidectomy.
For L-THYROXINE 100 BERLIN-CHEMIE:
- as a diagnostic agent in performing the thyroid suppression test.
Contraindications.
Hypersensitivity to the active substance or to any of the excipients of the medicinal product. Untreated hyperthyroidism of any origin. Untreated adrenal insufficiency. Untreated pituitary insufficiency (this leads to adrenal insufficiency requiring treatment). Acute myocardial infarction. Acute myocarditis. Acute pancarditis.
During pregnancy, concomitant use of levothyroxine and any antithyroid agent is contraindicated (more detailed information on use during pregnancy or breastfeeding is provided in the section «Use during pregnancy or breastfeeding»).
Interaction with other medicinal products and other forms of interaction.
Antidiabetic agents
Levothyroxine may reduce the blood glucose-lowering effect of antidiabetic drugs (e.g., metformin, glimepiride, glyburide, and insulin). More frequent monitoring of blood glucose levels is recommended in diabetes, especially at the beginning and end of thyroid hormone therapy. Dose adjustment of the antidiabetic medicinal product may be necessary.
Coumarin derivatives
Levothyroxine may potentiate the effect of coumarin derivatives by displacing them from plasma protein binding sites. Therefore, when used concomitantly, regular monitoring of coagulation parameters is required, and the dose of anticoagulant agents may need to be adjusted (reduced).
Ion-exchange resins
Ion-exchange resins such as cholestyramine, colestipol, or calcium and sodium salts of polystyrene sulfonic acid inhibit the absorption of levothyroxine by binding thyroid hormones in the gastrointestinal tract; therefore, they should be administered 4–5 hours after taking the medicinal product L-Thyroxine Berlin-Chemie.
Proton pump inhibitors (PPIs):
Concomitant use with PPIs may lead to reduced absorption of thyroid hormones due to increased gastric pH caused by PPIs. During concomitant therapy, regular monitoring of thyroid function and clinical observation are recommended. An increase in thyroid hormone dosage may be required. Caution should also be exercised when PPI treatment is discontinued.
Drugs binding bile acids
Colesevelam binds levothyroxine and thereby reduces its absorption in the gastrointestinal tract. No interaction was observed when levothyroxine was administered at least 4 hours before colesevelam. Therefore, L-Thyroxine Berlin-Chemie should be administered at least 4 hours before colesevelam.
Aluminum-containing antacids, as well as iron- and calcium-containing drugs
Absorption of levothyroxine may be reduced when co-administered with aluminum-containing antacids (antacids, sucralfate), iron- and calcium-containing medicinal products. L-Thyroxine Berlin-Chemie should be administered at least 2 hours before these products.
Sevelamer and lanthanum carbonate
Sevelamer and lanthanum carbonate may reduce the bioavailability of levothyroxine (see also section «Special precautions for use»).
Propylthiouracil, glucocorticoids, and beta-blockers (especially propranolol)
These substances inhibit the conversion of thyroxine (T4) to T3 and may lead to decreased plasma T3 concentration.
Amiodarone and iodinated contrast agents
Due to their high iodine content, amiodarone and iodinated contrast agents may cause both hyperthyroidism and hypothyroidism. Particular caution is required in nodular goiter with possible latent autonomy. Amiodarone inhibits the conversion of T4 to T3, resulting in decreased T3 concentration and increased levels of thyroid-stimulating hormone (TSH) in plasma. Due to the effect of amiodarone on thyroid function, dose adjustment of L-Thyroxine Berlin-Chemie may be necessary.
Salicylates, dicoumarol, furosemide, clofibrate
Salicylates (especially at doses above 2 g daily), dicoumarol, high-dose furosemide (250 mg), clofibrate, and other substances may displace levothyroxine from plasma protein binding sites. This may lead to an initial transient increase in free thyroid hormone levels, resulting in decreased total thyroid hormone levels.
Estrogen-containing contraceptives, drugs for hormone replacement therapy in postmenopausal period
Requirement for levothyroxine may increase during use of estrogen-containing contraceptives or hormone replacement therapy in the postmenopausal period. Increased binding of levothyroxine is possible, which may lead to diagnostic and therapeutic errors.
Sertraline, chloroquine/proguanil
These substances reduce the effectiveness of levothyroxine and increase serum TSH levels.
Cytochrome P450 inducers
Medicinal products that induce enzymes, such as rifampicin, carbamazepine, phenytoin, barbiturates, and products containing St. John's wort (Hypericum perforatum L.), may increase hepatic clearance of levothyroxine, leading to decreased serum thyroid hormone concentration. Thus, patients receiving thyroid replacement therapy may require an increased dose of thyroid hormones when these drugs are used concomitantly.
Protease inhibitors
There have been reports of loss of therapeutic effect of levothyroxine when co-administered with lopinavir/ritonavir. Therefore, patients receiving levothyroxine and protease inhibitors concomitantly require careful monitoring of clinical symptoms and thyroid function. In patients taking levothyroxine, TSH levels should be monitored at least during the first month after initiation and/or discontinuation of ritonavir therapy.
Tyrosine kinase inhibitors
Tyrosine kinase inhibitors (e.g., imatinib, sunitinib, sorafenib, motesanib) may reduce the effectiveness of levothyroxine. Therefore, careful monitoring of clinical symptoms and thyroid function parameters is required in patients receiving levothyroxine and tyrosine kinase inhibitors concomitantly. Dose adjustment of levothyroxine may be necessary.
Soy-containing products
Soy-containing products may inhibit intestinal absorption of levothyroxine. Reports have been published on increased serum TSH levels in children on a soy-based diet who were treated with levothyroxine due to congenital hypothyroidism. To achieve normal serum T4 and TSH levels, high doses of levothyroxine are recommended. Careful monitoring of serum T4 and TSH levels is required during and after discontinuation of a soy-based diet; dose adjustment of levothyroxine may be necessary.
Orlistat
Hypothyroidism and/or reduced control of hypothyroidism may occur when levothyroxine and orlistat are used concomitantly. This may be due to reduced absorption of levothyroxine.
Kava
Concomitant intake of levothyroxine with kava should be avoided, as it may reduce absorption of levothyroxine from the gastrointestinal tract. Therefore, an interval of half an hour to one hour between administration of levothyroxine and consumption of kava is recommended to minimize the risk of interaction. Patients already receiving levothyroxine therapy are advised not to change their kava consumption habits without medical evaluation and monitoring of levothyroxine levels.
Semaglutide
Concomitant use of semaglutide may affect levothyroxine exposure. The area under the concentration-time curve (AUC) of levothyroxine (corrected for endogenous levels) increased by 33% after a single oral dose of semaglutide, while the maximum concentration (Cmax) remained unchanged. When treating patients with levothyroxine concomitantly with semaglutide, consideration should be given to monitoring thyroid function parameters and adjusting the dose.
Effect on laboratory test results
Biotin may interfere with immunoassays of thyroid function based on biotin-streptavidin interaction, leading to falsely low or falsely high test results (see section «Special precautions for use»).
Special precautions for use.
Before initiating therapy with thyroid hormones or performing thyroid suppression tests, the presence of the following diseases or conditions should be excluded or treated:
- Ischemic heart disease
- Angina pectoris
- Hypertension
- Pituitary insufficiency and/or adrenal cortical insufficiency.
Autonomous thyroid function should also be excluded or treated prior to starting thyroid hormone therapy.
In patients with ischemic heart disease, heart failure, tachyarrhythmia, myocarditis (outside the acute phase), chronic hypothyroidism, or those who have had a myocardial infarction, pharmacologically induced hyperthyroidism—even mild—must be strictly avoided. When treating such patients with thyroid hormones, more frequent monitoring of thyroid hormone levels is required (see section "Dosage and administration").
In cases of secondary hypothyroidism, concomitant adrenal cortical insufficiency should be evaluated. If present, replacement therapy (e.g., with hydrocortisone) should be initiated first. Thyroid hormone therapy in patients with adrenal or pituitary insufficiency, without adequate corticosteroid replacement, may precipitate an Addisonian crisis.
Hemodynamic parameters should be closely monitored in preterm infants with very low birth weight when initiating levothyroxine therapy, due to potential circulatory instability caused by adrenal immaturity.
In suspected autonomous thyroid dysfunction, TSH levels should be measured or thyroid scintigraphy performed prior to initiating treatment.
Postmenopausal women are at increased risk of developing osteoporosis; therefore, levothyroxine sodium dosage should be carefully titrated to achieve the lowest effective dose. To avoid supraphysiological serum levothyroxine concentrations, thyroid function should be monitored more frequently in these patients (see section "Adverse reactions").
Thyroid hormones must not be used for weight reduction. Administration of physiological doses does not lead to weight loss in euthyroid patients. Higher doses may cause serious or even life-threatening adverse reactions, particularly when combined with certain weight-loss agents.
Hypersensitivity reactions (including angioedema), sometimes severe, have been reported with levothyroxine use. If signs or symptoms of allergic reactions occur, levothyroxine therapy should be discontinued and appropriate symptomatic treatment initiated (see sections "Contraindications" and "Adverse reactions").
Once a stable levothyroxine regimen has been established, switching to another thyroid hormone-containing medicinal product should only be done under close laboratory and clinical monitoring.
In patients concurrently receiving levothyroxine and other medicinal products that may affect thyroid function (e.g., amiodarone, tyrosine kinase inhibitors, salicylates, and high-dose furosemide), thyroid function should be monitored (see also section "Interaction with other medicinal products and other forms of interaction").
Caution is advised when prescribing levothyroxine to patients with a history of epilepsy, as these patients may have an increased risk of seizures.
For patients with diabetes mellitus or those receiving anticoagulants, see section "Interaction with other medicinal products and other forms of interaction".
Cases of hypothyroidism have been reported in patients receiving both sevelamer and levothyroxine. Therefore, in patients receiving both agents, TSH levels should be carefully monitored (see also section "Interaction with other medicinal products and other forms of interaction").
Effect on laboratory test results:
Biotin may interfere with thyroid function assays based on the biotin-streptavidin principle, leading to falsely low or falsely high test results. The risk of interference increases with higher biotin doses. When interpreting laboratory test results, potential biotin interference should be considered, especially if results are inconsistent with the clinical picture. Laboratory personnel should be informed about biotin use in patients receiving biotin-containing products to determine the optimal timing for thyroid function testing. Alternative assays not affected by biotin should be used if available (see section "Interaction with other medicinal products and other forms of interaction").
This medicinal product contains less than 1 mmol (23 mg) of sodium per tablet, i.e., essentially "sodium-free".
Use during pregnancy or breastfeeding.
Thyroid hormone therapy should be maintained continuously during pregnancy and breastfeeding.
Thyroid suppression testing should not be performed during pregnancy or breastfeeding.
Pregnancy
Maintaining thyroid hormone levels within the normal range is essential during pregnancy to ensure optimal maternal and fetal health. To date, despite widespread use during pregnancy, no adverse effects of levothyroxine on pregnancy or fetal/neonatal health have been observed.
Levothyroxine requirements may increase during pregnancy due to estrogen effects. Therefore, thyroid function should be monitored throughout pregnancy and after delivery, and thyroid hormone dosage adjusted as necessary.
Since serum TSH levels may rise as early as week 4 of pregnancy, pregnant women receiving levothyroxine should have TSH levels measured during each trimester to ensure values remain within the trimester-specific reference range. Elevated TSH levels should be corrected by increasing the levothyroxine dose. As postpartum TSH levels typically return to pre-pregnancy values, levothyroxine dosage should be adjusted back to the pre-pregnancy dose immediately after delivery. Serum TSH levels should be reassessed 6–8 weeks postpartum.
The use of sodium levothyroxine as an adjunct in antithyroid drug treatment of hyperthyroidism is contraindicated during pregnancy. Additional levothyroxine may necessitate higher doses of antithyroid drugs. Unlike levothyroxine, antithyroid agents cross the placental barrier in significant amounts and may cause fetal hypothyroidism. Therefore, antithyroid drugs should always be used as monotherapy and at the lowest effective dose in pregnant women with hyperthyroidism.
Breastfeeding
Levothyroxine is excreted into human breast milk; however, concentrations achieved with recommended therapeutic doses are not sufficient to cause hyperthyroidism or suppress TSH secretion in the nursing infant.
Fertility
Hypothyroidism or hyperthyroidism may affect fertility. During treatment of hypothyroidism with levothyroxine, dosage should be adjusted based on laboratory monitoring, as underdosing will not produce a beneficial effect, while overdosing may lead to hyperthyroidism.
Effect on ability to drive and use machines.
No studies specifically investigating the effect on the ability to drive or operate machinery have been conducted.
Dosage and Administration.
The dosage information provided should be considered as recommendations. The individual daily dose of the drug should be determined based on laboratory test results and clinical evaluation. Thyroid hormone therapy should be initiated at a low dose and gradually increased (every 2-4 weeks) until the required therapeutic dose is achieved.
Since serum levels of T4 or free thyroxine (fT4) may be elevated in some patients, monitoring of treatment is best performed by measuring serum TSH concentration.
Adults.
Treatment of benign goiter: 75–200 mcg/day.
Prevention of goiter recurrence: 75–200 mcg/day.
Replacement therapy in hypothyroidism: initial dose is 25–50 mcg/day; maintenance dose is 100–200 mcg/day.
Concomitant therapy in antithyroid drug treatment of hyperthyroidism: 50–100 mcg/day.
Suppressive and replacement therapy in thyroid cancer: 150–300 mcg/day.
Thyroid suppression test (only for L-Thyroxine 100 Berlin-Chemi): 200 mcg (equivalent to 2 tablets)/day for 14 days prior to the test.
Children with congenital and acquired hypothyroidism.
The maintenance dose is usually 100–150 mcg of levothyroxine per 1 m² body surface area per day.
For infants and children with congenital hypothyroidism requiring immediate levothyroxine replacement therapy, the recommended initial dose during the first 3 months of life is 10–15 mcg of levothyroxine per kilogram of body weight per day. Subsequent dose adjustments should be made individually based on clinical findings, thyroid hormone levels, and TSH concentrations.
For children with acquired hypothyroidism, the recommended initial dose is 12.5–50 mcg of levothyroxine per day, using a formulation with appropriate dosage strength. The dose should be gradually increased at intervals of 2–4 weeks based on clinical findings, thyroid hormone levels, and TSH concentrations until the full replacement dose is achieved. Infants and children under 3 years of age should receive the full daily dose at least 30 minutes before the first feeding of the day. Tablets may also be administered as a suspension. To prepare, dissolve the tablet in a small amount of water (10–15 mL), then administer the freshly prepared suspension to the child, adding a small additional amount of water (5–10 mL).
Elderly patients.
In certain cases, particularly in elderly patients with cardiac disease, a gradual reduction in the dose of sodium levothyroxine is recommended, with regular monitoring of TSH levels.
Clinical experience suggests that using the lowest effective dose is optimal in patients with low body weight or large nodular goiter.
The entire daily dose should be swallowed whole, without chewing the tablets, with a small amount of liquid, e.g., ½ glass of water. The drug should be taken on an empty stomach, at least 30 minutes before breakfast.
Due to the special design of the tablet, it can be divided as follows: place the tablet on a hard surface with the score line facing upwards, and press down perpendicularly with a finger (see Figure 1).
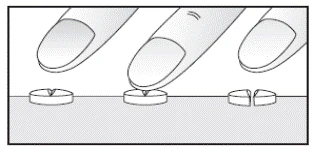
Figure 1
Treatment duration.
The drug is usually administered lifelong in cases of hypothyroidism, following surgical interventions such as strumectomy or thyroidectomy, and for prevention of recurrence after removal of euthyroid goiter. The duration of treatment as an adjunct in hyperthyroidism after achieving euthyroid status corresponds to the duration of antithyroid therapy. In mild forms of euthyroid goiter, treatment duration ranges from 6 months to 2 years. If the patient's condition does not improve after treatment, surgical intervention or radioactive iodine therapy should be considered.
Thyroid suppression test.
For the thyroid suppression test, take 150–200 mcg of sodium levothyroxine daily for 14 days.
Children.
The drug may be used in pediatric practice. Detailed information on recommended doses and administration is provided in the section «Dosage and Administration».
Overdose.
Symptoms of overdose include tachycardia, palpitations, anxiety, sensation of heat, elevated body temperature, increased sweating, arrhythmia, insomnia, tremor, increased frequency of angina attacks, restlessness, weight loss, vomiting, diarrhea, headache, weakness, muscle cramps, menstrual cycle disturbances, and pseudotumor cerebri. Isolated cases of epileptic seizures have been reported in patients when the individual tolerance limit was exceeded.
It is recommended to discontinue the drug and perform follow-up examinations.
Elevated T3 levels are a more reliable indicator of drug overdose than elevated T4 or fT4 levels.
In cases of overdose and intoxication, symptoms typical of moderate or marked metabolic acceleration occur (see section «Adverse Reactions»). Depending on the severity of overdose, discontinuation of the drug and follow-up monitoring are recommended.
Human cases of levothyroxine overdose (suicide attempts) with doses up to 10 mg have been tolerated without complications. The development of severe complications such as life-threatening disturbances in vital functions (respiration and circulation) is unlikely, provided there is no history of ischemic heart disease. Nevertheless, there have been reports of thyrotoxic crisis, seizures, heart failure, and coma. Isolated cases of sudden death due to cardiac complications have been reported in patients who have been on prolonged high-dose levothyroxine therapy.
In cases of acute overdose, absorption of the drug from the gastrointestinal tract can be reduced by administering activated charcoal. Treatment is generally symptomatic and supportive. In cases of severe beta-sympathomimetic symptoms such as tachycardia, restlessness, agitation, or hyperkinesis, these may be alleviated with beta-adrenergic blockers. Antithyroid drugs should not be used, as thyroid function is already fully suppressed.
In cases of extreme overdose (suicide attempts), plasmapheresis may be beneficial.
Prolonged monitoring is required in cases of levothyroxine overdose. Due to the gradual conversion of levothyroxine to liothyronine, symptom onset may be delayed up to 6 days.
Adverse reactions.
If the patient does not tolerate the dose, which is very rare, or in case of overdose, especially with too rapid dose escalation at the beginning of treatment, typical symptoms of hyperthyroidism may occur.
In such cases, the daily dose should be reduced or administration of the drug should be discontinued for several days. After resolution of adverse effects, treatment can be resumed with careful dose titration.
Allergic reactions may occur in patients hypersensitive to levothyroxine or to any of the excipients, affecting the skin (e.g., angioedema, skin rash, urticaria) or respiratory tract. There have been isolated reports of anaphylactic shock. In such cases, the drug must be discontinued.
Adverse reactions are classified by frequency of occurrence as follows:
| Very common (≥ 1/10) Common (≥ 1/100 — < 1/10) Uncommon (≥ 1/1,000 — < 1/100) Rare (≥ 1/10,000 — < 1/1,000) Very rare (< 1/10,000) Not known (cannot be estimated from available data) |
Immune system side effects
Unknown: hypersensitivity
Endocrine system side effects:
Common: hyperthyroidism
Cardiac side effects
Very common: tachycardia
Common: tachycardia
Unknown: arrhythmia, angina pectoris
Skin and subcutaneous tissue side effects
Unknown: angioneurotic edema, rash, urticaria, hyperhidrosis
Psychiatric disorders
Very common: insomnia
Common: nervousness
Unknown: inner restlessness
Skeletal, muscular and connective tissue side effects
Unknown: muscle weakness, muscle cramps, osteoporosis due to suppressive doses of levothyroxine, particularly in postmenopausal women, mainly during prolonged treatment
Vascular side effects
Unknown: hot flushes, collapse (acute circulatory failure) in premature infants with very low birth weight (see section «Special precautions for use»)
Reproductive system and breast side effects
Unknown: menstrual disorders
Gastrointestinal side effects
Unknown: diarrhea, vomiting, nausea
Additional investigation findings
Unknown: weight loss
Nervous system side effects
Very common: headache
Rare: pseudotumor cerebri (mainly in children)
Unknown: tremor
General disorders and administration site reactions
Unknown: heat intolerance, fever
Reporting suspected adverse reactions.
Reporting of suspected adverse reactions after authorization of the medicinal product is important. It allows ongoing monitoring of the benefit-risk balance of the medicinal product. Medical and pharmaceutical professionals, as well as patients or their legal representatives, should report any suspected adverse reactions and lack of efficacy of the medicinal product via the Automated Pharmacovigilance Information System at the following link: https://aisf.dec.gov.ua.
Shelf life.
3 years. Do not use the medicinal product after the expiry date stated on the packaging.
Storage conditions.
Store at a temperature not exceeding 30 °C. Store in the original blister pack to protect from light. Keep the medicinal product out of the reach of children.
Packaging.
Blister pack of 25 tablets; 1, 2, or 4 blisters per cardboard box.
Prescription category.
Prescription only.
Manufacturer.
BERLIN-CHEMIE AG.
Manufacturer's address and place of business.
Glienicker Weg 125, 12489 Berlin, Germany.