Havrix 1440 vaccine for prevention of hepatitis a
Ukraine
Table of Contents
- Instructions for Medical Use of the Medicinal Product Havrix 720 Vaccine for Prevention of Hepatitis A Havrix 1440 Vaccine for Prevention of Hepatitis A
- Composition:
- Clinical characteristics.
- Special precautions for use
- Method of Administration and Dosage
- Adverse reactions
- adverse reactions reported during the post-marketing period but not observed during randomized controlled clinical trials. The frequency category "rare" was determined by statistical calculation based on the total number of children vaccinated during the randomized controlled clinical trial (n=4574).
Instructions for Medical Use of the Medicinal Product Havrix 720 Vaccine for Prevention of Hepatitis A Havrix 1440 Vaccine for Prevention of Hepatitis A
Composition:
Active substance: hepatitis A virus antigen;
1 pediatric dose (0.5 mL) contains hepatitis A virus antigen 720 ELISA units (Havrix 720);
1 adult dose (1 mL) contains hepatitis A virus antigen 1440 ELISA units (Havrix 1440).
Excipients: aluminium hydroxide, amino acids for injection, sodium hydrogen phosphate, potassium dihydrogen phosphate, polysorbate 20, potassium chloride, sodium chloride, water for injections.
Pharmaceutical form. Injection suspension.
Main physicochemical properties:
International non-proprietary name: Hepatitis A vaccine, inactivated
Havrix is a suspension containing hepatitis A virus (strain HM 175) inactivated by formaldehyde and adsorbed onto aluminium hydroxide.
The virus is cultivated in human diploid cells MRC-5. Prior to virus isolation, cells are thoroughly washed to remove the growth medium. The virus suspension is obtained by cell lysis and then purified using ultrafiltration and gel chromatography methods. Virus inactivation is achieved by treatment with formaldehyde.
Havrix is a purified sterile suspension of inactivated hepatitis A virus; antigen content is determined by solid-phase enzyme immunoassay (ELISA).
Havrix is a cloudy liquid suspension. A white sediment with a clear colorless supernatant may be observed during storage.
Havrix complies with the requirements of the World Health Organization for inactivated vaccines for prevention of hepatitis A.
Pharmacotherapeutic group. Inactivated vaccine against hepatitis A virus.
ATC code J07BC02.
Immunological and biological properties
Pharmacodynamics.
Havrix vaccine is intended for immunization to prevent viral hepatitis A by stimulating a specific immune response based on induction of antibodies against hepatitis A virus (HAV).
Immune response
In clinical studies, seroconversion was achieved in 99% of vaccinated individuals within 30 days after administration of the first vaccine dose. In a subgroup of clinical trials designed to determine the kinetics of immune response, early and rapid seroconversion was observed after administration of a single dose of Havrix: in 79% of vaccinated individuals on day 13, 86.3% on day 15, 95.2% on day 17, and 100% on day 19, indicating that this time interval was shorter than the average incubation period for hepatitis A virus (4 weeks) (see also section "Preclinical safety data").
Duration of immune response.
To ensure long-term immune protection, a booster vaccination is required 6–12 months after primary vaccination with Havrix 1440 (adult dose) or Havrix 720 (pediatric dose). Clinical trials have shown that one month after administration of the booster dose, all vaccinated individuals became seropositive. However, if the booster vaccination was not administered within 6–12 months after primary vaccination, administration of the booster dose may be delayed up to 5 years. A comparative clinical trial demonstrated that a booster dose administered up to 5 years after the first dose induces antibody production at the same concentration level as when the booster is given 6–12 months after primary vaccination.
The persistence of antibodies against hepatitis A virus was evaluated after administration of two doses of Havrix with an interval of 6–12 months between doses.
Data collected over 17 years allow prediction that at least 95% and 90% of individuals will remain seropositive (>15 mIU/mL) at 30 and 40 years after vaccination, respectively (see Table 1).
Table 1
Predicted percentage with anti-HAV level ≥ 15 mIU/mL and
95% confidence intervals for studies HAV-112 and HAV-123
| Year |
≥ 15 mMO/mL |
95% confidence interval |
|
| Lower level |
Upper level |
||
| Prediction for HAV-112 |
|||
| 25 |
97.69% |
94.22% |
100% |
| 30 |
96.53% |
92.49% |
99.42% |
| 35 |
94.22% |
89.02% |
98.93% |
| 40 |
92.49% |
86.11% |
97.84% |
| Prediction for HAV-123 |
|||
| 25 |
97.22% |
93.52% |
100% |
| 30 |
95.37% |
88.89% |
99.07% |
| 35 |
92.59% |
86.09% |
97.22% |
| 40 |
90.74% |
82.38% |
95.37% |
Current data support the absence of a need for revaccination among immunocompetent individuals after completion of the two-dose vaccination course.
Efficacy of HAVRIX vaccine in controlling disease outbreaks
The efficacy of HAVRIX vaccine was evaluated in population groups across various geographically distant regions where disease outbreaks had been identified (Alaska, Slovakia, USA, United Kingdom, Israel, and Italy).
These studies demonstrated that vaccination with HAVRIX leads to the cessation of disease outbreaks. Vaccination of 80% of the population results in termination of outbreaks within 4 to 8 weeks.
Impact of mass vaccination on disease incidence
A decline in hepatitis A incidence has been observed in countries where the two-dose immunization schedule with HAVRIX™ has been implemented for children in their second year of life:
• In Israel, two retrospective database studies showed that after implementation of the vaccination program, hepatitis A incidence in the general population decreased by 88% and 95% at 5 and 8 years, respectively. Data from the National Surveillance System also indicate a 95% reduction in hepatitis A incidence compared to the pre-vaccination period.
• In Panama, a retrospective database study showed a 90% reduction in hepatitis A incidence among the vaccinated population and an 87% reduction in the general population three years after implementation of the vaccination program.
- Observations of reduced hepatitis A incidence in the general population (both vaccinated and unvaccinated) in both countries demonstrate herd immunity.
Preclinical safety data: In a study involving 8 non-human primates, animals were exposed to a heterologous strain of hepatitis A virus and vaccinated 2 days after exposure. As a result of this post-exposure vaccination, protection was achieved in all animals.
Clinical characteristics.
Indications.
Havrix vaccine is intended for active immunization of individuals belonging to groups at risk of infection with hepatitis A virus.
The vaccine does not prevent infections caused by other pathogens, such as hepatitis B virus, hepatitis C virus, hepatitis E virus, or other agents causing liver diseases.
In areas with low and moderate endemicity of hepatitis A, vaccination with Havrix is recommended primarily for individuals who constitute or may constitute high-risk groups for infection. These include:
- Travelers. Individuals traveling to regions with high prevalence of hepatitis A. These regions include Africa, Asia, the Mediterranean basin, the Middle East, Central and South America.
- Military personnel. Military personnel deployed to regions with increased endemicity or regions with poor sanitary conditions are at higher risk of hepatitis A virus infection. Active immunization is indicated for such individuals.
- Individuals at risk of hepatitis A due to their occupation, or those at increased risk of transmitting the disease. These include: staff of childcare facilities, nurses, physicians, junior medical personnel in hospitals and other healthcare institutions, especially in gastroenterology and pediatric departments, workers servicing sewage systems and water treatment facilities, public food service workers and food storage personnel, and other categories.
- Individuals at increased risk due to their sexual behavior. Homosexuals, individuals with multiple sexual partners.
- Patients with hemophilia.
- Individuals who use injectable drugs.
- Individuals in contact with infected persons. Since virus excretion by infected individuals may occur over a prolonged period, active immunization is recommended for individuals in close contact with infected persons.
- Individuals requiring protection as part of hepatitis A outbreak control, or due to increased incidence in the region.
- Certain population groups known to have high rates of hepatitis A infection.
For example, American Indians and Eskimos are groups in which epidemics caused by hepatitis A virus are widespread.
- Individuals with chronic liver disease or at increased risk of developing chronic liver disease (e.g., chronic carriers of hepatitis B virus or hepatitis C virus, and individuals who abuse alcohol).
In regions with moderate to high prevalence of hepatitis A (e.g., Africa, Asia, the Mediterranean basin, the Middle East, Central and South America), active immunization is recommended for susceptible individuals. This includes immunization of children and adolescents, particularly in higher socioeconomic groups and urban areas.
Contraindications.
Havrix should not be administered to individuals with known hypersensitivity to any component of the vaccine or to neomycin (present as a residual from the manufacturing process) (see section “Composition”), or in case of hypersensitivity reactions following prior administration of Havrix vaccine.
Interaction with other medicinal products and other forms of interaction.
Havrix is an inactivated vaccine; therefore, its concomitant use with other inactivated vaccines should not affect the magnitude of the immune response.
Havrix may be administered simultaneously with vaccines against typhoid fever, yellow fever, cholera (injections), tetanus, or with monovalent and combination vaccines against measles, mumps, rubella, and varicella.
Concomitant administration of Havrix with immunoglobulin does not affect seroconversion rates, but may result in reduced antibody titers.
If co-administration of Havrix with other vaccines or immunoglobulins is necessary, these products should be administered using separate syringes and needles at different injection sites.
Special precautions for use
As with other vaccines, administration of Havrix should be postponed in cases of acute severe illness accompanied by fever. However, a mild infection is not a contraindication to vaccination.
Due to the long incubation period of hepatitis A, an asymptomatic infection may be present at the time of immunization. In such cases, it is unknown whether vaccination will prevent the development of hepatitis A.
In patients undergoing hemodialysis or those with impaired immune function, an adequate antibody titer against hepatitis A virus may not be achieved after primary vaccination course, which may require administration of additional vaccine doses.
As with all injectable vaccines, appropriate medical treatment and supervision must be readily available to manage possible anaphylactic reactions, which may rarely occur following vaccination. Therefore, patients should remain under medical observation for at least 30 minutes after vaccination.
Syncope (fainting) may occur during or immediately after any injectable vaccination, as a psychogenic response to needle injection. Vaccination should be performed only while the recipient is in a sitting or lying position, and the recipient should remain in the same position (sitting or lying) for at least 15 minutes after vaccination to minimize the risk of injury due to falls.
Havrix may be administered to HIV-infected individuals.
The presence of antibodies against hepatitis A (seropositive individual) is not a contraindication.
Havrix contains less than 1 mmol (23 mg)/dose of sodium, i.e., essentially "sodium-free".
Havrix contains less than 1 mmol (39 mg)/dose of potassium, i.e., essentially "potassium-free".
Use during pregnancy or breastfeeding
There are insufficient data on the use of the vaccine during pregnancy in humans and adequate studies on reproductive toxicity in animals. However, as with all other inactivated vaccines, the risk of adverse effects on the fetus is considered negligible.
Havrix may be used during pregnancy only if clearly needed.
There are insufficient data on the use of the vaccine during breastfeeding in humans and no adequate reproductive studies in animals. Although the risk is considered negligible, Havrix should be used during lactation only if clearly necessary.
Ability to affect reaction speed while driving or operating machinery
Studies on the effect of Havrix™ on the ability to drive or operate machinery have not been conducted. However, some adverse reactions may temporarily affect reaction speed while driving or operating machinery (see section "Adverse reactions").
Method of Administration and Dosage
Method of Administration
Havrix is intended for intramuscular administration. In adults and older children, the vaccine should be administered into the deltoid muscle region; in younger children, it should be administered into the anterolateral aspect of the thigh.
The vaccine must not be administered intravenously. The vaccine should not be administered intravascularly. Injection into the gluteal muscle is not recommended. Subcutaneous or intradermal administration should also be avoided, as these routes may result in a reduced immune response.
Havrix must not be administered intravascularly.
In patients with thrombocytopenia or coagulation disorders, the vaccine should be administered with caution due to an increased risk of bleeding following intramuscular injection.
Dosage
Primary Vaccination
- Adults aged 19 years and older: For primary immunization, a single dose of Havrix 1440 (adult dose) (1.0 mL of suspension) should be administered.
- Children from 1 year of age and adolescents up to 18 years of age, inclusive: For primary immunization of children and adolescents, a single dose of Havrix 720 (pediatric dose) (0.5 mL of suspension) should be administered.
Booster Vaccination
After primary vaccination with Havrix 1440 (adult dose) or Havrix 720 (pediatric dose), a booster dose is recommended to ensure long-term immune protection. This booster dose should be administered at any time between 6 months and 5 years after the first dose, preferably between 6 and 12 months after the first dose (see section "Immunological and Biological Properties").
Vaccination of children in Ukraine is carried out in accordance with the requirements of the current orders of the Ministry of Health of Ukraine regarding preventive vaccinations.
Instructions for Vaccine Use
Prior to administration, the vaccine should be visually inspected for the presence of any foreign particulate matter and/or changes in physical characteristics. Before use, the vial or prefilled syringe containing Havrix should be shaken vigorously until a slightly opaque, white suspension is obtained. If the vaccine does not meet the specified characteristics, it must be discarded.
Instructions for Use of the Prefilled Syringe:

Hold the syringe by the barrel, not by the plunger.
Unscrew the syringe cap by turning it counterclockwise.
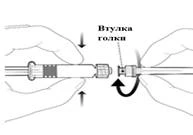
To attach the needle, connect the hub to the Luer-Lock adapter and turn a quarter turn clockwise until the needle is securely fixed.
Do not remove the plunger from the syringe barrel. If this occurs, do not administer the vaccine.
Any unused product or waste material should be disposed of in accordance with local requirements.
Children. Havrix 720 (pediatric dose) is indicated for children from 1 year of age.
Overdose
During post-marketing surveillance, cases of overdose have been reported. Adverse reactions observed following overdose were similar to those observed with normal vaccination.
Adverse reactions
The safety profile provided below is based on clinical trial data from 5,300 patients and post-marketing surveillance data. It should be noted that the frequency of adverse reactions observed during the post-marketing period could not be determined and therefore are listed as "not known". The most commonly reported reactions following vaccination were pain and redness at the injection site, occurring after administration of 50% of all doses of Havrix 1440 and after administration of 18.2% of all doses of Havrix 720. The next most commonly reported reaction was swelling at the injection site.
Adverse reactions are categorized by frequency into the following groups:
Very common (≥ 1/10)
Common (≥ 1/100 to < 1/10)
Uncommon (≥ 1/1,000 to < 1/100)
Rare (≥ 1/10,000 to < 1/1,000)
Very rare (< 1/1,000)
Not known (frequency cannot be estimated from available data)
Within each frequency category, adverse reactions are listed in order of decreasing severity.
Table 2
| System organ class |
Frequency |
Adverse reactions |
| Infections and infestations |
Uncommon |
Upper respiratory tract infections* Rhinitis* |
| Immune system disorders |
Unknown |
Anaphylaxis Allergic reactions, including anaphylactoid reactions and serum sickness-like reactions |
| Metabolism and nutrition disorders |
Common |
Loss of appetite |
| Psychiatric disorders |
Very common |
Irritability** |
| Nervous system disorders |
Very common |
Headache (common - when using Havrix 720 vaccine) |
| Common |
Somnolence** |
|
| Uncommon |
Dizziness* |
|
| Rare |
Hypoesthesia Paresthesia |
|
| Unknown |
Seizures Guillain-Barré syndrome |
|
| Vascular disorders |
Unknown |
Vasculitis |
| Gastrointestinal disorders |
Common |
Gastrointestinal symptoms * (rare - when using Havrix 720 vaccine#) Nausea Diarrhea (uncommon - when using Havrix 720 vaccine) |
| Uncommon |
Vomiting |
|
| Hepatobiliary disorders |
Unknown |
Transient increase in liver function parameters |
| Skin and subcutaneous tissue disorders |
Uncommon |
Rash** |
| Rare |
Pruritus |
|
| Unknown |
Angioneurotic edema Polymorphic erythema Urticaria |
|
| Musculoskeletal and connective tissue disorders |
Uncommon |
Myalgia* Limitation of musculoskeletal mobility* |
| Unknown |
Arthralgia |
|
| General disorders and administration site conditions |
Very common |
Pain and redness at injection site Fatigue* (rare - when using Havrix 720 vaccine#) |
| Common |
Increased body temperature (≥37.5 °C) Injection site reactions such as swelling or induration (uncommon - when using Havrix 720 vaccine#) Malaise |
|
| Uncommon |
Influenza-like symptoms* |
|
| Rare |
Chills |
* adverse reactions observed after administration of Havrix 1440 vaccine (1 mL, adult dose)
** adverse reactions observed after administration of Havrix 720 vaccine (0.5 mL, pediatric dose)
adverse reactions reported during the post-marketing period but not observed during randomized controlled clinical trials. The frequency category "rare" was determined by statistical calculation based on the total number of children vaccinated during the randomized controlled clinical trial (n=4574).
Shelf life.
36 months. The expiry date of the vaccine is indicated on the label and packaging.
Storage conditions.
The vaccine should be stored in the original packaging to protect from light, at a temperature of 2 to 8 °C. Do not freeze. If the vaccine has been frozen, it must be discarded.
Stability data indicate that Havrix remains stable for 3 days at 25 °C. This information is intended for healthcare professionals only, in case of temporary deviation from the recommended storage temperature.
Incompatibility
Havrix must not be mixed with other vaccines or immunoglobulins in the same syringe.
Packaging.
Injection suspension, 0.5 mL or 1 mL, in vials No. 1 or in pre-filled syringes No. 1, supplied with a needle. Vials and syringes are made of type I neutral glass complying with the requirements of the European Pharmacopoeia.
The cap and plunger rubber stopper of the pre-filled syringe, as well as the vial cap, are made of synthetic rubber.
Prescription status. Prescription only.
Manufacturer.
GlaxoSmithKline Biologicals S.A., Belgium / GlaxoSmithKline Biologicals S.A., Belgium.
Manufacturer's name and address of the place of business
Rue de l’Institut, 89, 1330 Rixensart, Belgium / Rue de l’Institut, 89 1330 Rixensart, Belgium.