Dexamethasone krka
Ukraine
Table of Contents
INSTRUCTIONS FOR MEDICAL USE OF THE MEDICINAL PRODUCT Dexamethason KRKA
Composition:
Active substance: dexamethasone;
1 tablet contains 4 mg or 8 mg of dexamethasone;
Excipients: lactose monohydrate, pregelatinized starch, colloidal anhydrous silicon dioxide, magnesium stearate.
Pharmaceutical form. Tablets.
Main physicochemical properties:
tablets of 4 mg: white or almost white, round tablets with bevelled edges and a score line on one side; the tablet can be divided into two equal parts along the score line;
tablets of 8 mg: white or almost white, oval tablets with a score line on one side; the tablet can be divided into two equal parts along the score line.
Pharmacotherapeutic group. Corticosteroids for systemic use, glucocorticoids. ATC code H02AB02.
Pharmacological properties.
Pharmacodynamics.
Mechanism of action
Dexamethasone is a highly potent, long-acting glucocorticoid with minimal sodium-retaining capacity, making it particularly suitable for use in patients with heart failure and arterial hypertension.
Its anti-inflammatory activity is 7 times stronger than that of prednisolone. Like other glucocorticoids, dexamethasone exerts anti-allergic, antipyretic, and immunosuppressive effects.
The elimination half-life of dexamethasone is 36–54 hours, allowing its use in conditions requiring continuous glucocorticoid activity.
The RECOVERY trial (Randomised Evaluation of COVid-19 thERapY) was a researcher-initiated, individually randomized, controlled, open-label, adaptive platform trial designed to assess the effects of potential treatments in patients hospitalized with COVID-19.
The trial was conducted across 176 healthcare facilities in the United Kingdom.
A total of 6425 patients were randomly assigned to receive either dexamethasone (2104 patients) or usual care alone (4321 patients). 89% of patients had laboratory-confirmed SARS-CoV-2 infection.
At randomization, 16% of patients were receiving invasive mechanical ventilation or extracorporeal membrane oxygenation, 60% were receiving oxygen alone (with or without non-invasive ventilation), and 24% were receiving neither.
The mean age of patients was 66.1 ± 15.7 years. 36% of patients were women. 24% had a history of diabetes mellitus, 27% had heart disease, and 21% had chronic lung disease.
Primary endpoint
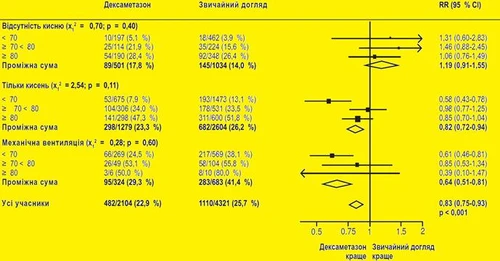
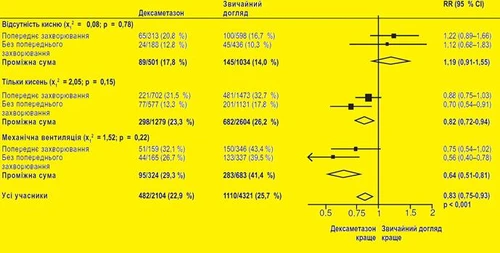
Mortality at day 28 was significantly lower in the dexamethasone group compared to the usual care group, with death reported in 482 of 2104 patients (22.9%) versus 1110 of 4321 patients (25.7%), respectively (rate ratio 0.83; 95% confidence interval [CI], 0.75 to 0.93; P < 0.001).
The dexamethasone group had lower mortality rates than the usual care group among patients receiving invasive mechanical ventilation (29.3% vs. 41.4%; rate ratio, 0.64; 95% CI, 0.51 to 0.81) and among those receiving supplemental oxygen without invasive mechanical ventilation (23.3% vs. 26.2%; rate ratio, 0.82; 95% CI, 0.72 to 0.94).
There was no clear benefit of dexamethasone in patients who were not receiving respiratory support at randomization (17.8% vs. 14.0%; rate ratio, 1.19; 95% CI, 0.91–1.55).
Secondary endpoints
Patients in the dexamethasone group had shorter hospital stays compared to those in the usual care group (median 12 days vs. 13 days) and a higher likelihood of being discharged alive within 28 days (rate ratio 1.10; 95% CI, 1.03 to 1.17).
Consistent with the primary endpoint, the greatest benefit in terms of discharge within 28 days was observed in patients receiving invasive mechanical ventilation at randomization (rate ratio 1.48; 95% CI, 1.16 to 1.90), followed by those receiving oxygen alone (rate ratio, 1.15; 95% CI, 1.06–1.24). A favorable effect was absent in patients not receiving oxygen (rate ratio 0.96; 95% CI, 0.85–1.08).
| Result |
Dexamethasone |
Usual care |
Hazard ratio* |
| (N = 2104) |
(N = 4321) |
(95% CI) |
|
| Number/total number of patients (%) |
|||
| Primary endpoint |
482/2104 (22.9) |
1110/4321 (25.7) |
0.83 (0.75–0.93) |
| 28-day mortality |
|||
| Secondary endpoint |
|||
| Discharged from hospital within 28 days |
1413/2104 (67.2) |
2745/4321 (63.5) |
1.10 (1.03–1.17) |
| Invasive mechanical ventilation or death†: |
456/1780 (25.6) |
994/3638 (27.3) |
0.92 (0.84–1.01) |
|
102/1780 (5.7) |
285/3638 (7.8) |
0.77 (0.62–0.95) |
|
387/1780 (21.7) |
827/3638 (22.7) |
0.93 (0.84–1.03) |
* The ratio of outcomes was adjusted for age based on 28-day mortality and hospital discharge results. The risk ratios were adjusted for age regarding the outcome of receiving invasive mechanical ventilation or death and its components;
† Patients who received invasive mechanical ventilation at randomization were excluded from this category.
Safety
During the study, 4 serious adverse events related to the investigational treatment were recorded: 2 cases of hyperglycemia development, 1 case of steroid-induced psychosis, and 1 case of upper gastrointestinal tract bleeding. All cases were resolved.
Subgroup Analysis
Effects of dexamethasone on 28-day mortality according to age and respiratory support method at randomization2
Effects of dexamethasone on 28-day mortality according to respiratory support method at randomization and presence of any chronic comorbidity3
1 www.recoverytrial.net
2, 3 Source: Horby P. et al., 2020; https://www.medrxiv.org/content/10.1101/2020.06.22.20137273v1;
doi: https://doi.org/10.1101/2020.06.22.20137273).
Pharmacokinetics.
Absorption and Distribution
Dexamethasone is well absorbed after oral administration; peak plasma levels are reached within 1 to 2 hours after administration and show a wide range of interindividual variability. The mean elimination half-life is 3.6 ± 0.9 hours. Dexamethasone is protein-bound in plasma (approximately 77%), primarily to albumin. The percentage of dexamethasone protein binding, unlike cortisol, remains practically unchanged with increasing steroid concentrations. Corticosteroids are rapidly distributed into all body tissues, cross the placenta, and may be excreted in small amounts into breast milk.
Biotransformation
Dexamethasone is mainly metabolized in the liver, but also in the kidneys.
Excretion
Dexamethasone and its metabolites are excreted in the urine.
Clinical characteristics.
Indications.
- Cerebral edema associated with brain tumor, neurosurgical intervention, bacterial meningitis, brain abscess.
- Severe acute asthma attack.
- Initial oral treatment of extensive, severe, acute skin diseases responsive to glucocorticoid therapy, e.g., erythroderma, pemphigus vulgaris, acute eczema.
- Initial oral treatment of autoimmune disorders such as systemic lupus erythematosus (especially its visceral forms).
- Severe progressive course of active rheumatoid arthritis, e.g., destructive forms and/or extra-articular manifestations.
- Severe infections with toxic states (e.g., tuberculosis, typhoid fever), only when accompanied by appropriate anti-infective therapy.
- Dexamethasone KRKA is indicated for the treatment of coronavirus disease 2019 (COVID-19) in adults and adolescents (aged 12 years and older with body weight of at least 40 kg) who require supplemental oxygen therapy.
- Palliative tumor therapy.
- Prevention and treatment of postoperative vomiting or vomiting induced by cytostatic agents, in combination with antiemetic agents.
Contraindications.
Hypersensitivity to the active substance or to any of the excipients.
Systemic infection in the absence of appropriate anti-infective therapy.
Peptic ulcer of the stomach or duodenum.
Vaccination with live vaccines during treatment with high therapeutic doses of dexamethasone (and other corticosteroids) due to the risk of viral infection.
Interaction with other medicinal products and other forms of interaction.
Before administering Dexamethasone KRKA in combination with any other medicinal product, the package leaflet of that medicinal product should be consulted.
Pharmacodynamic interactions
Patients receiving nonsteroidal anti-inflammatory drugs (NSAIDs) should be monitored, as NSAIDs may increase the frequency and/or severity of gastric ulcers. Acetylsalicylic acid should be used with caution in combination with corticosteroids in patients with hypoprothrombinemia.
Renal clearance of salicylates is increased during corticosteroid therapy. Therefore, the dose of salicylates may need to be reduced when steroid treatment is discontinued. Cessation of steroid therapy may lead to salicylate intoxication due to increased serum concentrations.
Corticosteroids reduce the effect of antidiabetic agents such as insulin, sulfonylureas, and metformin. Hyperglycemia and diabetic ketoacidosis may occasionally occur.
Therefore, diabetic patients should have their blood and urine tested more frequently at the beginning of treatment. The hypokalemic effect of acetazolamide injections, loop diuretics, thiazide diuretics, potassium-wasting diuretics, amphotericin B, glucomineralocorticoids, tetracosactide, and laxatives may be enhanced. Hypokalemia may lead to cardiac arrhythmias, especially torsade de pointes, and may increase the toxicity of cardiac glycosides. Hypokalemia should be corrected and electrolyte levels and ECG should be assessed before initiating corticosteroid therapy. In addition, concomitant use of amphotericin B and hydrocortisone has been reported to cause cardiac enlargement and heart failure.
Anti-ulcer agents. Carbenoxolone increases the risk of hypokalemia.
Chloroquine, hydroxychloroquine, and mefloquine. Increased risk of myopathy and cardiomyopathy.
Concomitant use with ACE inhibitors increases the risk of hematological disorders. Corticosteroids may affect the antihypertensive effect of antihypertensive drugs; dose adjustment of antihypertensive agents may be required during dexamethasone therapy.
Thalidomide. Particular caution is required when used concomitantly with thalidomide, as cases of toxic epidermal necrolysis have been reported.
The effect of vaccination may be reduced during dexamethasone therapy.
Vaccination with live vaccines during treatment with high therapeutic doses of dexamethasone (and other corticosteroids) is contraindicated due to the risk of viral infection. In such cases, vaccination should be postponed for at least 3 months after discontinuation of corticosteroid therapy. Other forms of immunization during treatment with high therapeutic doses of corticosteroids are hazardous due to the risk of neurological complications and lower or absent increases in antibody titers (compared to expected values), resulting in reduced protective effect. However, patients who have received corticosteroids locally or for a short duration (less than 2 weeks) in lower doses may be vaccinated.
Cholinesterase inhibitors. Concomitant use of cholinesterase inhibitors and corticosteroids may result in severe muscle weakness in patients with myasthenia gravis. If possible, cholinesterase inhibitors should be discontinued at least 24 hours before starting corticosteroid therapy.
There is an increased risk of tendonitis and tendon rupture in patients receiving glucocorticoids and fluoroquinolones concomitantly.
Pharmacokinetic interactions
Effect of other medicinal products on dexamethasone
Dexamethasone is metabolized via cytochrome P450 3A4 (CYP3A4).
Concomitant use of dexamethasone with CYP3A4 inducers such as ephedrine, barbiturates, rifabutin, rifampicin, phenytoin, and carbamazepine may lead to decreased plasma concentrations of dexamethasone; therefore, the dose of dexamethasone may need to be increased.
Aminoglutethimide may accelerate the elimination of dexamethasone and reduce its efficacy. Appropriate dose adjustment of dexamethasone should be performed if necessary.
Bile acid resins such as cholestyramine may reduce the absorption of dexamethasone.
Locally acting gastrointestinal agents, antacids, activated charcoal. Reduced absorption of glucocorticoids has been reported with concomitant use of prednisolone and dexamethasone. Therefore, glucocorticoids and locally acting gastrointestinal agents, antacids, or activated charcoal should be administered at least two hours apart.
Concomitant use of dexamethasone with CYP3A4 inhibitors such as azole antifungals (e.g., ketoconazole, itraconazole), HIV protease inhibitors (e.g., ritonavir), and macrolides (e.g., erythromycin) may lead to increased plasma concentrations and reduced clearance of dexamethasone. If necessary, the dose of dexamethasone should be reduced.
Ketoconazole may not only increase dexamethasone plasma concentrations by inhibiting CYP3A4 but may also suppress adrenal steroid synthesis and cause adrenal insufficiency after discontinuation of corticosteroid therapy.
Estrogens, including oral contraceptives, may inhibit the metabolism of certain corticosteroids and thereby enhance their effects.
Effect of dexamethasone on other medicinal products
Dexamethasone is a moderate inducer of CYP3A4. Concomitant use of dexamethasone with drugs metabolized by CYP3A4 may lead to increased clearance and reduced plasma concentrations of these drugs.
Antituberculosis agents. Decreased plasma concentrations of isoniazid have been observed when used concomitantly with prednisolone. Close monitoring of patients receiving isoniazid is recommended.
Cyclosporine. Concomitant use of cyclosporine and corticosteroids may potentiate the effects of both drugs. There is an increased risk of cerebral seizures.
Praziquantel. Reduced plasma concentrations of praziquantel may result in treatment failure due to increased hepatic metabolism induced by dexamethasone.
Oral anticoagulants (coumarins). Concomitant therapy with corticosteroids may enhance or diminish the effect of oral anticoagulants. When high doses are used or treatment duration exceeds 10 days, there is a risk of bleeding related to corticosteroid therapy (gastrointestinal mucosa, vascular fragility). Patients receiving corticosteroids in combination with oral anticoagulants should be closely monitored (check on day 8, then every two weeks during and after treatment).
Atropine and other anticholinergic agents. Increased intraocular pressure may occur with concomitant use of dexamethasone.
Non-depolarizing muscle relaxants. Muscle relaxation effect may be prolonged.
Somatotropin. The effect of growth hormone may be reduced.
Protirelin. The expected increase in TSH may be diminished during protirelin administration.
Concomitant use of CYP3A inhibitors, including products containing cobicistat, is expected to increase the risk of systemic adverse effects. Such combinations should be avoided unless the benefit outweighs the increased risk, and in such cases, patients should be monitored for systemic corticosteroid effects.
Special precautions for use.
Adrenal insufficiency
Adrenal insufficiency caused by glucocorticoid therapy may persist for many months and, in some cases, more than one year after discontinuation of treatment. During dexamethasone therapy, temporary dose increases may be required in individual cases of physical stress (e.g., trauma, surgery, childbirth, etc.). Due to the potential risk under stressful conditions, initial corticosteroid administration is necessary for patients undergoing prolonged therapy. Even in cases of prolonged adrenal insufficiency after treatment cessation, glucocorticoid administration may be required in patients experiencing severe stress. Acute adrenal insufficiency induced by therapy can be minimized by gradually tapering the dose prior to planned discontinuation.
Dexamethasone treatment should only be administered strictly according to indications, and additional targeted anti-infective therapy should be considered when the following diseases or conditions are present:
- Acute viral infections (e.g., herpes zoster, herpes simplex virus, varicella, herpetic keratitis);
- HBsAg-positive chronic hepatitis in the active phase;
- Approximately 8 weeks before and 2 weeks after live vaccine administration (see sections "Contraindications" and "Interaction with other medicinal products and other forms of interaction");
- Systemic mycoses and parasitosis (e.g., nematodes);
- Poliomyelitis;
- Lymphadenitis following BCG vaccination;
- Acute and chronic bacterial infections;
- History of tuberculosis (risk of reactivation), only with concomitant administration of antituberculosis agents;
- Known or suspected strongyloidiasis (nematode infestation). Glucocorticoid treatment may lead to strongyloidiasis hyperinfection and widespread larval dissemination.
Furthermore, dexamethasone therapy should only be prescribed under strict indications, and additional specific treatment should be considered for the following conditions:
- Gastrointestinal ulcers;
- Osteoporosis (since corticosteroids negatively affect calcium balance);
- Hypertension that is difficult to control;
- Poorly controlled diabetes mellitus;
- Psychiatric disorders (including history thereof);
- Closed-angle glaucoma and open-angle glaucoma;
- Corneal ulcers and corneal trauma;
- Severe heart failure.
Anaphylactic reactions
Severe anaphylactic reactions may occur.
Tendinitis
There is an increased risk of tendinitis and tendon rupture in patients receiving concomitant glucocorticoids and fluoroquinolones.
Myasthenia
Pre-existing myasthenia may worsen at the beginning of dexamethasone treatment.
Visual disturbances
Visual disturbances have been reported with both systemic and local corticosteroid use. If a patient experiences symptoms such as blurred vision or other visual disturbances, they should be referred to an ophthalmologist for evaluation of possible causes, including cataract, glaucoma, or rare conditions such as central serous chorioretinopathy (CSCR), which has been reported after systemic and local corticosteroid use.
Prolonged corticosteroid use may lead to posterior subcapsular cataracts, glaucoma with possible optic nerve damage, and may increase the risk of secondary ocular infections caused by fungi or viruses.
Corticosteroids should be used with caution in patients with ocular herpes due to the potential risk of corneal perforation.
Gastrointestinal perforation
Due to the risk of gastrointestinal perforation, dexamethasone should only be used in emergency situations and with appropriate monitoring in the following conditions:
- Severe ulcerative colitis with risk of perforation;
- Diverticulitis;
- Enteric anastomosis (immediately after surgery).
Signs of peritoneal irritation following gastrointestinal perforation may be absent in patients receiving high-dose glucocorticoids.
Diabetes mellitus
Increased insulin or oral antidiabetic requirements should be anticipated in diabetic patients receiving dexamethasone.
Cardiovascular system disorders
Regular blood pressure monitoring is required during dexamethasone therapy, especially when high doses are used or in patients with poorly controlled hypertension. Close monitoring is necessary in patients with severe heart failure due to the risk of worsening condition.
Bradycardia may occur in patients receiving high doses of dexamethasone.
Corticosteroids should be used cautiously in patients who have recently experienced myocardial infarction, as cases of myocardial rupture have been reported.
Infections
Dexamethasone treatment may mask symptoms of existing or developing infections, complicating diagnosis. Prolonged use, even at low doses, increases the risk of infection, including by microorganisms that rarely cause disease under normal circumstances (so-called opportunistic infections).
In the treatment of coronavirus disease 2019 (COVID-19), systemic corticosteroids should not be discontinued in patients already receiving systemic (oral) corticosteroids for other reasons (e.g., patients with chronic obstructive pulmonary disease) who do not require supplemental oxygen.
Vaccination
Inactivated vaccines may be administered. However, higher corticosteroid doses may negatively affect immune response and thus reduce vaccination efficacy. In patients undergoing long-term dexamethasone therapy, regular medical check-ups are recommended (including preventive eye examinations every three months).
Metabolic disturbances
With high doses, monitoring of adequate calcium intake, sodium restriction, and serum potassium levels is recommended. Depending on the duration and dosage of treatment, a negative effect on calcium metabolism may be expected; therefore, osteoporosis prophylaxis is advised. This is particularly relevant in the presence of risk factors such as family predisposition, advanced age, postmenopausal status, inadequate protein and calcium intake, smoking, excessive alcohol consumption, and insufficient physical activity. Prophylaxis includes adequate calcium and vitamin D intake and regular physical activity. Additional medical treatment should be considered in cases of existing osteoporosis.
Corticosteroids should be prescribed cautiously in patients with migraine, as corticosteroid use may cause fluid retention.
Psychiatric disturbances
Psychological changes may manifest in various forms, the most common being euphoria. Other possible effects include depression, psychotic reactions, and suicidal tendencies.
These conditions may be serious. They typically begin within a few days or weeks after starting treatment and are more likely with high-dose regimens. Most of these effects resolve upon dose reduction or discontinuation of the drug. If such effects occur, treatment is likely required. In some cases, psychiatric problems have emerged during dose tapering or after discontinuation.
Cerebral edema and increased intracranial pressure
Corticosteroids should not be used in traumatic brain injury, as they are unlikely to provide benefit and may even be harmful.
Tumor lysis syndrome
Tumor lysis syndrome (TLS) has been observed in patients with hematologic malignancies after dexamethasone administration, either alone or in combination with other chemotherapeutic agents. Close monitoring and appropriate preventive measures are necessary in patients at high risk of TLS, such as those with high proliferation rates, large tumor burden, or high sensitivity to cytotoxic agents.
Discontinuation of therapy
Glucocorticoid doses should be gradually tapered.
The following risks should be considered when interrupting or discontinuing long-term glucocorticoid therapy:
- Exacerbation or relapse of the underlying disease, acute adrenal insufficiency, corticosteroid withdrawal syndrome (which may include fever, muscle and joint pain, nasal mucosal inflammation (rhinitis), weight loss, skin pruritus, and eye inflammation (conjunctivitis)).
- Some viral infections (e.g., varicella, measles) may have a severe course in patients receiving glucocorticoids.
- Children and immunocompromised individuals who have not had varicella or measles are particularly susceptible to adverse effects. If such individuals are exposed to measles or varicella during dexamethasone treatment, prophylactic treatment may be necessary.
Pheochromocytoma crisis
A potentially fatal crisis in pheochromocytoma has been reported after systemic corticosteroid administration. Corticosteroids should only be administered to patients with suspected or confirmed pheochromocytoma after appropriate risk-benefit assessment.
Children
Corticosteroids cause dose-dependent growth suppression in infants, children, and adolescents, as they may lead to premature epiphyseal closure, which can be irreversible. Therefore, long-term dexamethasone use in children should only be considered under strict indications, and growth in these patients should be monitored regularly.
Preterm neonates: Available data indicate long-term neurodevelopmental adverse effects after early treatment (<96 hours) of preterm infants with chronic lung disease at initial doses of 0.25 mg/kg twice daily.
Elderly patients
Adverse effects of systemic corticosteroids, particularly in elderly patients, may have serious consequences. These mainly include osteoporosis, hypertension, hypokalemia, diabetes mellitus, increased susceptibility to infections, and skin atrophy. Careful clinical monitoring is required to prevent life-threatening reactions.
Impact on diagnostics
Glucocorticoids may suppress skin reactions during allergy testing. They may also interfere with the nitroblue tetrazolium test for bacterial infections and may lead to false-negative results.
Doping note
Dexamethasone use may result in a positive doping test.
Dexamethasone KRKA contains lactose. Patients with rare hereditary disorders of galactose intolerance, lactase deficiency, or glucose-galactose malabsorption should not take this medicinal product.
Use during pregnancy or breastfeeding.
Pregnancy
Dexamethasone crosses the placenta. Administration of corticosteroids to pregnant animals has resulted in fetal developmental abnormalities, including cleft palate, intrauterine growth retardation, and effects on brain growth and development. There is no evidence that corticosteroids increase the incidence of congenital anomalies such as cleft palate/cleft lip in humans. Long-term or repeated corticosteroid therapy during pregnancy increases the risk of intrauterine growth retardation. Newborns exposed to corticosteroids in utero have an increased risk of adrenal insufficiency; spontaneous postnatal regression usually occurs under normal conditions, but this is rarely clinically significant. Dexamethasone should only be used during pregnancy, especially in the first trimester, if the benefit outweighs the risks to the mother and fetus.
Lactation
Corticosteroids pass into breast milk. There is insufficient information on the excretion of dexamethasone into breast milk. Risk to the newborn/infant cannot be excluded. Suppression of adrenal function may occur in infants whose mothers receive high doses of systemic corticosteroids over a prolonged period.
The decision to continue or discontinue breastfeeding and/or dexamethasone therapy should be based on the benefits of breastfeeding for the child and the benefits of dexamethasone therapy for the mother.
Fertility
Dexamethasone reduces testosterone biosynthesis and endogenous ACTH secretion, thereby affecting spermatogenesis and the ovarian cycle.
Ability to influence reaction speed when driving or operating machinery.
Studies on the effect on the ability to drive or operate machinery have not been conducted.
Dexamethasone may cause confusion, hallucinations, dizziness, somnolence, fatigue, syncope, and blurred vision. Patients should be advised not to drive, operate machinery, or perform hazardous tasks during dexamethasone treatment.
Method of Administration and Dosage
Dosage
Dexamethasone is administered in usual doses ranging from 0.5 to 10 mg per day, depending on the disease being treated. Higher doses exceeding 10 mg per day may be required for more severe conditions. The dose should be adjusted according to the individual patient's response and severity of the disease. Initial doses of dexamethasone are used until a clinical response is achieved, after which the dose should be gradually reduced to the lowest clinically effective dose. Significantly higher doses are used for treatment of acute severe conditions compared to chronic diseases. To minimize adverse effects, the lowest effective dose should be used.
If not otherwise directed, follow the dosage recommendations below.
The dosage recommendations provided below are for informational purposes only. Initial and daily doses must always be determined based on the individual patient's response and disease severity.
Cerebral edema: Depending on the cause and severity of the condition, the initial dose is 8–10 mg (up to 80 mg)/day administered intravenously, followed by oral administration of 16–24 mg (up to 48 mg)/day divided into 3–4 (not more than 6) doses for 4–8 days. Longer-term therapy with lower doses of dexamethasone may be required in cases of radiation therapy and conservative management of brain tumors not amenable to surgical intervention.
Cerebral edema due to bacterial meningitis: 0.15 mg/kg body weight every 6 hours for 4 days, administered before antibiotic therapy; in children – 0.4 mg/kg body weight every 12 hours for 2 days.
Acute asthma attack: Adults – 8–20 mg/day, followed if necessary by 8 mg every 4 hours.
Children – 0.15–0.3 mg/kg body weight.
Acute skin diseases: Daily dose ranges from 8–40 mg depending on the nature and severity of the condition, and may reach up to 100 mg in some cases; the dose should then be reduced according to clinical necessity.
Active phase of systemic rheumatic diseases: Systemic lupus erythematosus – 6–16 mg/day.
Exacerbation of rheumatoid arthritis with severe progressive course: Used in rapidly destructive forms at doses of 12–16 mg/day; in extra-articular manifestations – 6–12 mg/day.
Severe infectious diseases, toxic states (e.g., tuberculosis, typhoid): 4–20 mg for several days only in combination with concomitant anti-infective therapy.
Treatment of COVID-19: 6 mg orally once daily for up to 10 days in adult patients.
Pediatric population: Adolescents (aged 12 years and older) are recommended to take 6 mg/dose orally once daily for up to 10 days.
Duration of treatment depends on clinical response and individual patient needs.
Dose adjustment is not required in elderly patients or in patients with renal or hepatic impairment.
Palliative treatment of neoplastic diseases: Initial dose is 8–16 mg/day; for long-term use – 4–12 mg/day.
Prevention and treatment of vomiting induced by cytostatics, emetogenic chemotherapy, in combination with antiemetics: Oral administration of 10–20 mg dexamethasone before initiation of chemotherapy, followed if necessary by 4–8 mg 2–3 times daily for 1–3 days (with moderately emetogenic therapy) or up to 6 days (with highly emetogenic therapy).
Prevention and treatment of postoperative nausea and vomiting: Single dose of 8–20 mg before surgery; in children aged 2 years and older – 0.15–0.5 mg/kg body weight (maximum 16 mg).
Renal impairment
In patients undergoing active hemodialysis, drug clearance may be increased through the dialysate, potentially requiring dose adjustment of corticosteroids.
Hepatic impairment
Dose adjustment may be necessary in patients with severe liver disease. In patients with severe hepatic insufficiency, the biological effects of dexamethasone may be enhanced due to slower metabolism (prolonged plasma half-life) and hypoalbuminemia (increased levels of free drug in plasma), which may also lead to increased adverse effects.
Elderly patients
Treatment of elderly patients, particularly with long-term therapy, should take into account the more serious consequences of common corticosteroid side effects in this age group (osteoporosis, diabetes mellitus, hypertension, reduced immunity, psychiatric changes). In such patients, plasma concentrations of dexamethasone may be higher and elimination slower than in younger patients; therefore, the dose should be appropriately reduced.
Long-term treatment
For long-term treatment of certain conditions following initial therapy, glucocorticoid treatment should be switched from dexamethasone to prednisone/prednisolone to reduce suppression of adrenal cortex function.
Discontinuation of therapy
Acute adrenal insufficiency may occur after abrupt discontinuation of prolonged high-dose glucocorticoid therapy. Therefore, in such cases, glucocorticoid doses should be gradually tapered to discontinue treatment (see section "Special precautions").
Method of administration
Dexamethasone should be taken during or immediately after a meal to minimize gastrointestinal irritation. Beverages containing alcohol or caffeine should be avoided.
Dexamethasone KRKA is available in tablet form in strengths of 4 mg, 8 mg, 20 mg, and 40 mg. Tablets may be divided into equal parts to provide additional doses of 2 mg and 10 mg, facilitating swallowing for patients.
When alternate-day therapy is not feasible, the total daily dose of glucocorticoids is usually administered as a single morning dose; however, some patients may require divided daily doses of glucocorticoids.
Children
The range of initial doses of dexamethasone is 0.08–0.3 mg/kg/day or 2.5–10 mg/m² body surface area per day in 3–4 divided doses. Dexamethasone elimination is approximately similar in children and adults when the dose is adjusted according to body surface area. Dosing should be individualized considering potential effects on growth and development and signs of adrenal suppression. Preterm neonates: Available data indicate long-term neurological adverse effects following early treatment (within 96 hours) of preterm infants with chronic lung disease at initial doses of 0.25 mg/kg twice daily.
Overdose
Symptoms
Acute toxicity and/or fatal cases following glucocorticoid overdose are rarely reported.
Overdose or prolonged use may exacerbate glucocorticoid side effects.
Treatment
No antidote exists. Treatment is symptomatic and supportive. Gradual dose reduction or slow discontinuation of dexamethasone is anticipated if possible. Treatment may not be indicated for reactions arising from chronic intoxication, except when the patient's condition renders them particularly susceptible to the adverse effects of corticosteroids. In such cases, gastric lavage should be performed and symptomatic treatment initiated as needed. Anaphylactic reactions and hypersensitivity reactions can be treated with epinephrine (adrenaline), artificial ventilation with positive pressure, and aminophylline. The patient should be kept warm and at rest. The plasma half-life of dexamethasone is approximately 190 minutes.
Adverse Reactions
Summary of Safety Profile
The frequency of expected adverse reactions correlates with the relative potency of the substance, dose, duration of administration, and length of treatment. The risk of adverse effects is low during short-term therapy, provided that dosage recommendations are followed and careful patient monitoring is maintained.
Common adverse effects of short-term dexamethasone treatment (days/weeks) include weight gain, psychiatric disturbances, impaired glucose tolerance, and transient adrenal insufficiency. Long-term dexamethasone therapy (months/years) is usually associated with central obesity, skin fragility, muscle atrophy, osteoporosis, growth suppression, and long-term adrenal insufficiency (see also section "Special Warnings and Precautions for Use").
| Body system classes |
Adverse reactions (frequency unknown) |
| Infections and infestations |
Increased susceptibility to infections* or exacerbation of latent infections, including sepsis, tuberculosis, eye infections, chickenpox, measles, fungal and viral infections, with masking of clinical symptoms, opportunistic infections |
| Blood and lymphatic system disorders |
Leukocytosis, lymphopenia, eosinopenia, polycythemia, coagulation disorders |
| Immune system disorders |
Allergic reactions, including anaphylaxis, decreased immunity (see also "Infections and infestations") |
| Endocrine disorders |
Suppression of the hypothalamic-pituitary-adrenal axis and induction of Cushing's syndrome (typical symptoms: moon face, facial redness (plethora), obesity), secondary adrenal and pituitary insufficiency (especially under stress such as trauma or surgery), growth suppression in infants, children and adolescents, menstrual irregularities and amenorrhea, hirsutism |
| Metabolism and nutrition disorders |
Weight gain, negative protein and calcium balance, increased appetite, sodium and water retention, potassium loss* (caution: arrhythmia), hypokalemic alkalosis, manifestation of latent diabetes mellitus, impaired carbohydrate tolerance requiring increased doses of antidiabetic agents*, hypercholesterolemia, hypertriglyceridemia |
| Psychiatric disorders* |
Psychological dependence, depression, insomnia, exacerbation of schizophrenia, psychiatric disorders ranging from euphoria to severe psychosis |
| Nervous system disorders |
Increased intracranial pressure with papilledema in children (idiopathic intracranial hypertension), usually after discontinuation of treatment; manifestation of latent epilepsy, increased frequency of seizures in existing epilepsy, dizziness, headache |
| Eye disorders |
Elevated intraocular pressure, glaucoma, papilledema, cataract*, mainly with posterior subcapsular opacity, corneal and scleral atrophy, increased incidence of ophthalmological viral, fungal and bacterial infections, worsening of symptoms related to corneal ulcers*, blurred vision, chorioretinopathy |
| Cardiac disorders |
Rupture of cardiac muscle following recent myocardial infarction, congestive heart failure in predisposed patients, cardiac decompensation* |
| Vascular disorders |
Arterial hypertension, vasculitis, increased atherosclerosis and risk of thrombosis/thromboembolism (increased blood coagulation may lead to thromboembolic complications) |
| Respiratory, thoracic and mediastinal disorders |
Hiccups |
| Gastrointestinal disorders |
Dyspepsia, abdominal distension*, gastric ulcers with perforation and hemorrhage, acute pancreatitis, ulcerative esophagitis, esophageal candidiasis, flatulence, nausea, vomiting |
| Skin and subcutaneous tissue disorders |
Hypertrichosis, skin atrophy, telangiectasia, striae, erythema, steroid acne, petechiae, ecchymoses, allergic dermatitis, urticaria, angioneurotic edema, hair thinning, pigmentary disturbances, increased capillary fragility, perioral dermatitis, hyperhidrosis, tendency to bruise |
| Musculoskeletal and connective tissue disorders |
Premature epiphyseal closure, osteoporosis, vertebral and long bone fractures, aseptic necrosis of femoral and humeral heads, tendon rupture*, proximal myopathy, muscle weakness, loss of muscle mass |
| Reproductive system and breast disorders |
Impotence |
| General disorders |
Reduced response to vaccination and skin tests. Delayed wound healing, discomfort, malaise, corticosteroid withdrawal syndrome: too rapid dose reduction after prolonged therapy may result in acute adrenal insufficiency, hypotension and death. Withdrawal syndrome may manifest as fever, myalgia, arthralgia, rhinitis, conjunctivitis, development of painful, itchy skin nodules and weight loss. |
*See also section "Special precautions".
Description of individual adverse reactions
Adrenal insufficiency
Adrenal insufficiency caused by glucocorticoid therapy may persist for many months, and in some cases over a year, after discontinuation of treatment, depending on the dose and duration of therapy (see section "Special precautions").
Psychiatric disturbances
Psychiatric disturbances may manifest in various forms, the most common being euphoria. Other possible effects include depression, psychotic reactions, and suicidal tendencies. These conditions can be serious. They usually occur within a few days or weeks after starting treatment and are more likely to occur with high-dose therapy. Most of these problems resolve upon dose reduction or discontinuation of the drug (see section "Special precautions").
Infections
Dexamethasone treatment may mask signs of existing or developing infection. This may complicate diagnosis and may lead to an increased risk of infection (see section "Special precautions").
Gastrointestinal perforation
The use of corticosteroids may be associated with an increased risk of gastrointestinal perforation in conditions such as severe ulcerative colitis with impending perforation, diverticulitis, and enterostomies (immediately after surgery).
Signs of peritoneal irritation following gastrointestinal perforation may be absent in patients receiving high doses of glucocorticoids (see section "Special precautions").
Cardiovascular disorders
Adverse effects may include bradycardia, worsening of severe heart failure, and poorly controlled high blood pressure. Corticosteroids should be used with caution in patients who have recently suffered myocardial infarction, as cases of myocardial rupture have been reported (see section "Special precautions").
Children
Corticosteroids may cause dose-dependent growth retardation in infants, children, and adolescents, as corticosteroids may lead to premature closure of epiphyses, which may be irreversible (see section "Special precautions").
Elderly patients
Adverse effects of systemic corticosteroids may have serious consequences, especially in elderly patients. These mainly include osteoporosis, arterial hypertension, hypokalaemia, diabetes mellitus, increased susceptibility to infections, and skin atrophy (see section "Special precautions").
Reporting suspected adverse reactions
Reporting of suspected adverse reactions after authorization of the medicinal product is important. It allows continued monitoring of the benefit-risk balance of the medicinal product. Medical and pharmaceutical professionals, as well as patients or their legal representatives, are encouraged to report all suspected adverse reactions and lack of efficacy to the State Expert Center of the Ministry of Health of Ukraine via the following link: https://aisf.dec.gov.ua.
Shelf life.
3 years.
Storage conditions.
No special temperature storage conditions are required for this medicinal product.
Store in the original packaging to protect from light and moisture.
Keep out of reach and sight of children.
Packaging.
10 tablets per blister; 1, 2, or 3 blisters per cardboard box.
Prescription status.
Prescription only.
Manufacturer.
KRKA, d.d., Novo mesto / KRKA, d.d., Novo mesto.
Manufacturer's address and location of operations.
Šmarješka cesta 6, 8501 Novo mesto, Slovenia / Smarjeska cesta 6, 8501 Novo mesto, Slovenia.