Budesonide-intel
Ukraine
Table of Contents
INSTRUCTIONS FOR MEDICAL USE OF THE MEDICINAL PRODUCT BUDENONID-INTELI (BUDESONID-INTELI)
Composition:
Active substance: budesonid;
1 dose contains 50 mcg or 200 mcg of micronized budesonide;
Excipients: oleic acid, anhydrous ethanol, 1,1,1,2-tetrafluoroethane (HFA-134a).
Pharmaceutical form. Pressurized inhalation, suspension.
Main physicochemical properties:
At release: for the 50 mcg/dose: white suspension;
for the 200 mcg/dose: white suspension with typical odor and taste.
During shelf life: for both strengths: white suspension.
Pharmacotherapeutic group.
Inhaled agents used in the treatment of obstructive airway diseases. Glucocorticoids. ATC code R03BA02.
Pharmacological properties.
Pharmacodynamics. Budesonide is an active synthetic glucocorticoid used for the treatment of allergic and inflammatory diseases of the respiratory tract. It exhibits minimal mineralocorticoid activity. It belongs to prolonged-action drugs suitable for once-daily dosing. Budesonide is characterized by local anti-inflammatory action due to its high lipophilicity and ability to penetrate intracellularly and bind to glucocorticoid receptors. The mechanism of action of budesonide involves the formation of complexes with cytoplasmic glucocorticoid receptors. Hormone-receptor complexes penetrate into the nuclei of target cells (eosinophils, neutrophils, lymphocytes), bind to DNA, and activate genes responsible for lipocortin production. Lipocortin is an inhibitor of phospholipase A2 – an enzyme that suppresses the synthesis of inflammatory mediators: histamine, leukotrienes, cytokines.
In the tissues of the respiratory tract, budesonide forms conjugates with fatty acid esters, which accumulate in cells. When the concentration of budesonide in cells decreases, fatty acid steroid esters are broken down under the influence of lipase. The released budesonide is capable of forming hormone-receptor complexes, which mediate the development of the drug's anti-inflammatory effect. The ability of budesonide to form conjugates with fatty acids explains the mechanism of its delayed-type local anti-inflammatory activity and high level of therapeutic efficacy.
The drug has greater affinity for glucocorticoid receptors in bronchi compared to beclomethasone dipropionate, thus demonstrating higher local anti-inflammatory and anti-allergic activity. Significant improvement in external respiratory function parameters is observed within several days (7–10 days) after the start of treatment. Budesonide does not affect bronchial smooth muscle. The drug reduces bronchial hyperreactivity, suppresses the early phase of allergic reaction (after sufficiently prolonged use) and the late phase of the reaction, thereby preventing asthma attacks. Budesonide also reduces bronchospasm induced by physical exertion, cold air, or sulfur dioxide.
Pharmacokinetics. The drug is rapidly absorbed after inhalation. 34% of the administered dose is deposited in the lungs. Absolute systemic bioavailability amounts to 39% of the inhaled dose. Maximum plasma concentrations of budesonide are achieved within 30 minutes after inhalation. The volume of distribution is approximately 2–3 L/kg. Metabolism of the majority of budesonide (approximately 90%) occurs in the liver via the enzyme CYP3A4, resulting in metabolites with low glucocorticoid activity. The glucocorticoid activity of the main metabolites, 6-beta-hydroxybudesonide and 16-alpha-hydroxybudesonide, is less than 1% compared to the active substance. Approximately 90% of the administered dose is inactivated during the first pass through the liver. Pulmonary metabolism is negligible. In adults, the plasma half-life of the drug averages 2 hours; in children, it is 1.5 hours. Plasma protein binding of budesonide ranges from 85% to 90%. The drug is excreted in urine (70%) and bile. Since the main effect of budesonide occurs in the respiratory tract, there are no data on the correlation between plasma concentration of the drug and its therapeutic efficacy.
Clinical characteristics.
Indications.
Bronchial asthma.
Contraindications.
Hypersensitivity to any component of the drug.
Interaction with other medicinal products and other forms of interaction.
Budesonide metabolism is mediated primarily by CYP3A4; therefore, inhibitors of this enzyme, such as ketoconazole and itraconazole, may increase systemic exposure to budesonide (see sections "Special warnings and precautions for use" and "Pharmacological properties"). Due to lack of dosing data, concomitant use of these drugs is not recommended. If concomitant use cannot be avoided, the interval between administration of these medicinal products should be as long as possible. A reduction in the dose of budesonide should also be considered. Other potent CYP3A4 inhibitors may likewise lead to a significant increase in budesonide plasma levels.
Limited data on similar interactions with high doses of inhaled budesonide show that co-administration of itraconazole at a dose of 200 mg once daily leads to a significant increase in budesonide plasma concentration (on average, 4-fold) following a single 1000 mcg inhaled dose of budesonide.
In women concurrently using estrogens or hormonal contraceptives, increased plasma concentrations of budesonide and enhanced corticosteroid effects have been observed; however, this effect was not observed when budesonide was used together with low-dose combined oral contraceptives.
Cimetidine exerts a weak inhibitory effect on the hepatic metabolism of budesonide, but this effect is not clinically significant.
Due to possible suppression of adrenal function, an ACTH (adrenocorticotropic hormone) stimulation test for diagnosing pituitary insufficiency may yield false-negative results (low values).
Children
Interaction studies have been conducted only in adults.
Special precautions for use
The drug should be used with caution in patients with active or inactive pulmonary tuberculosis and fungal or viral respiratory tract infections.
Patients not dependent on steroids. Therapeutic effect is usually achieved within 10 days. In patients with excessive mucus secretion in the bronchi, a short-term (approximately 2 weeks) additional course of oral corticosteroids may be initially administered. After completion of oral corticosteroid therapy, treatment with budesonide as monotherapy may be sufficient.
Patients dependent on steroids. Transition from oral corticosteroids to budesonide may be initiated when the patient is in a relatively stable phase of the disease. In such cases, budesonide should be used in combination with the previously administered dose of oral corticosteroid for approximately 10 days.
After this period, the dose of oral corticosteroids should be gradually reduced (e.g., by 2.5 mg of prednisolone or equivalent per month) until the lowest possible dose is reached. In many cases, complete replacement of oral corticosteroids with budesonide is possible.
During transition from oral corticosteroid therapy to budesonide, a reduction in systemic corticosteroid effects is usually observed, which may lead to the appearance of allergy or arthritis symptoms such as rhinitis, eczema, and musculoskeletal pain. Specific treatment should be prescribed for these conditions. In rare cases, symptoms such as fatigue, headache, nausea, and vomiting may occur, indicating systemic glucocorticoid insufficiency. In such cases, temporary increase in the dose of oral corticosteroid may sometimes be required.
As with other forms of inhaled therapy, paradoxical bronchospasm may occur immediately after administration of the dose. If severe reactions occur, the treatment should be re-evaluated and, if necessary, alternative therapy initiated.
Patients who have required high-dose systemic corticosteroid therapy or long-term treatment with inhaled corticosteroids at the highest recommended dose are also at risk of developing adrenal suppression. In such patients, symptoms of adrenal insufficiency may occur during periods of severe stress. Additional systemic corticosteroid therapy may be considered during stressful situations or prior to planned surgical procedures.
Systemic effects may occur with any inhaled corticosteroid, particularly when high doses are used over prolonged periods. The likelihood of such effects is significantly lower with inhaled corticosteroids than with oral corticosteroids. Possible systemic effects include Cushing's syndrome, Cushingoid features, adrenal suppression, growth retardation in children, decreased bone mineral density, cataract, and glaucoma. Less frequently, psychological and behavioral disorders may occur, including psychomotor hyperactivity, sleep disturbances, anxiety, depression, or aggression (especially in children). Therefore, the dose of inhaled corticosteroids should be titrated to the lowest effective dose that maintains adequate control of bronchial asthma.
Budesonide is not intended for rapid relief of acute episodes of bronchial asthma requiring short-acting inhaled bronchodilators. If treatment with short-acting bronchodilators is ineffective or if the patient requires more inhalations than usual, medical intervention is necessary. In such cases, intensification of standard therapy should be considered, for example, by increasing the dose of inhaled budesonide, adding a long-acting beta-agonist, or initiating a course of oral glucocorticoids.
Impaired liver function may affect the elimination of glucocorticosteroids from the body, as reduced clearance leads to increased systemic exposure. The possibility of adverse effects should therefore be considered.
Patients receiving high-dose systemic corticosteroid therapy or long-term treatment with the maximum recommended dose of inhaled corticosteroids may have an increased risk of adrenal suppression. In such patients, signs and symptoms of adrenal insufficiency may occur during periods of severe stress. The need for additional systemic corticosteroid therapy during stressful periods or prior to planned surgery should be considered. These patients should be instructed to carry a card indicating that they may require steroid treatment. Treatment with additional systemic corticosteroids or the medicinal product Budesonide-Intel should not be discontinued abruptly.
However, plasma clearance after intravenous administration of budesonide was similar in patients with liver cirrhosis and healthy volunteers. After oral administration, systemic bioavailability of budesonide increased due to impaired liver function, resulting from reduced presystemic metabolism. The clinical significance of these changes for budesonide treatment has not been fully established, as data on the inhaled formulation are lacking; however, increased plasma levels and, consequently, increased risk of systemic adverse reactions may be expected.
It has been shown that oral administration of ketoconazole and itraconazole (known inhibitors of CYP3A4 activity in the liver and intestinal mucosa) increases systemic exposure to budesonide. Concomitant use of ketoconazole, itraconazole, HIV protease inhibitors, or other potent CYP3A4 inhibitors should be avoided. If concomitant use cannot be avoided, the interval between administration of these drugs should be as long as possible. Consideration should also be given to reducing the dose of budesonide (see section "Interaction with other medicinal products and other forms of interaction").
Oropharyngeal candidiasis may develop during treatment with inhaled corticosteroids. This infection may require appropriate antifungal treatment, and in some patients, discontinuation of therapy may be necessary (see also section "Method of administration and dosage").
Patients using inhaled corticosteroids should rinse the mouth with water after each dose to reduce the risk of fungal colonization of the oropharynx.
Warning: Administration of budesonide by athletes may result in a positive doping test.
Children
Effect on growth
In children receiving long-term treatment with inhaled corticosteroids, regular monitoring of growth is recommended. If growth retardation occurs, therapy should be re-evaluated with the aim of reducing the inhaled corticosteroid dose to the lowest possible level that maintains effective control of bronchial asthma. The benefits of corticosteroid therapy should be carefully weighed against the potential risk of growth suppression. Furthermore, referral of the patient to a pediatric pulmonologist is important.
Use during pregnancy or breastfeeding
Pregnancy
Use of budesonide during pregnancy requires careful assessment of benefit to the mother versus risk to the fetus. Inhaled glucocorticosteroids should be preferred over oral glucocorticosteroids due to their lower systemic effects when used at doses required to achieve equivalent respiratory effects.
Breastfeeding period
Budesonide passes into breast milk. However, when therapeutic doses of budesonide are used, no significant effect on the breastfed infant is expected. Budesonide may be used during breastfeeding.
Supportive treatment with inhaled budesonide (200 or 400 mcg twice daily) in breastfeeding women with bronchial asthma results in only minimal systemic exposure of breastfed infants to budesonide.
Considering available data on inhaled budesonide and the fact that budesonide exhibits linear pharmacokinetic properties within therapeutic dose ranges after nasal, inhaled, oral, or rectal administration, exposure of breastfed infants to budesonide at therapeutic doses is expected to be low.
Ability to affect reaction rate when driving or operating machinery
Budesonide does not affect reaction rate when driving or operating machinery.
Method of administration and dosage.
For inhalation use only.
Children aged 5 to 12 years: 200–800 mcg daily, in 2–4 divided doses.
Adults (including elderly patients) and children aged 12 years and older: 200–1600 mcg daily, in 2–4 divided doses.
After achieving the desired clinical effect, the maintenance dose should be gradually reduced to the lowest dose required to control symptoms.
After each inhalation, the patient should rinse the mouth with water.
Instructions for correct use:
Before using the aerosol, check the expiry date of the medication. If the inhaler is new or has not been used for several days, shake it well and release one dose into the air to ensure it is working properly.
|
|
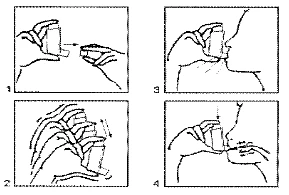
- After inhaling, hold your breath to allow maximum penetration of the drug.
- If necessary, continue for several seconds and repeat the procedure again (3, 4).
- Close with the cap after use.
The plastic adapter must be cleaned regularly. To clean, remove the metal container and wash the adapter with warm (not hot) soapy water.
Rinse the adapter thoroughly, dry it, and reassemble the device. After reassembly, close with the cap.
Children.
The drug is contraindicated in children under 5 years of age.
Overdose.
With prolonged use of high doses, systemic effects of glucocorticoids may occur, such as hypercorticism (edema, facial swelling) and suppression of the hypothalamic-pituitary-adrenal axis. Electrolyte imbalance should be corrected by using potassium-sparing diuretics such as spironolactone and triamterene.
Adverse Reactions
The frequency of adverse effects is presented below according to the following criteria: very common (≥1/10); common (≥1/100 to <1/10); uncommon (≥1/1,000 to <1/100); rare (≥1/10,000 to <1/1,000); very rare (<1/10,000).
Infections and infestations
Common: Oropharyngeal candidiasis.
Rare: Pneumonia (in patients with COPD (chronic obstructive pulmonary disease)).
Immune system disorders
Rare: Immediate and delayed hypersensitivity reactions (including rash, contact dermatitis, urticaria, angioedema, and anaphylactic reaction).
Endocrine system disorders
Rare: Signs and symptoms of systemic corticosteroid effects, including adrenal suppression and growth retardation*.
Psychiatric disorders
Rare: Psychomotor hyperactivity, sleep disorders, aggression, irritability, psychosis.
Behavioral changes (mainly in children).
Uncommon: Anxiety, depression.
Nervous system disorders
Uncommon: Tremor**.
Eye disorders
Uncommon: Cataract.
Not known: Glaucoma.
Respiratory, thoracic and mediastinal disorders
Common: Cough, hoarseness, throat irritation.
Rare: Dysphonia, bronchospasm, hoarseness***.
Skin and subcutaneous tissue disorders
Rare: Bruising.
Musculoskeletal and connective tissue disorders
Not known: Muscle spasms.
* see section "Children" below;
** based on frequency reported in clinical trials;
*** rarely in children.
Description of selected adverse reactions
Oropharyngeal candidiasis may occur due to deposition of the drug in the oropharynx. Rinsing the mouth with water after each inhalation minimizes this risk.
As with any inhaled therapy, paradoxical bronchospasm may very rarely occur (see section "Special precautions").
There is an increased risk of pneumonia in patients with newly diagnosed COPD who initiate inhaled corticosteroid therapy. However, a weighted analysis of eight pooled clinical trials did not demonstrate an increased risk of pneumonia. Results from the first seven of these eight studies were published as a separate meta-analysis.
Systemic effects may occur with inhaled corticosteroids, particularly when high doses are used over prolonged periods. Such effects are considerably less likely with inhaled therapy than with oral corticosteroids. Potential systemic effects include reduced bone mineral density. The effect is likely dependent on dose, duration of exposure, concomitant and prior corticosteroid therapy, and individual sensitivity.
Children
Due to the risk of growth retardation in children, growth monitoring should be performed in pediatric patients as described in the section "Special precautions".
Shelf life. 2 years.
Storage conditions.
Store at temperatures not exceeding 30 °C.
Keep out of reach and sight of children.
Pressurized container – do not pierce. Do not throw into fire, even when empty.
Protect from direct sunlight. Do not store near sources of heat.
Do not freeze.
Packaging.
Aluminum canister containing 200 doses (10 ml) with 50 mcg/dose or 200 mcg/dose of budesonide each, with a plastic actuator and cap, in a cardboard box.
Prescription status. Prescription only.
Manufacturer.
LABORATORIO ALDO-UNION, S.L. / LABORATORIO ALDO-UNION, S.L.
Manufacturer's address.
Baronesa de Malda, 73, 08950 Esplugues de Llobregat, Barcelona, Spain / Baronesa de Malda, 73, 08950 Esplugues de Llobregat, Barсelona, Spain.
Marketing Authorization Holder.
JSC «INTELI GENERICS NORD» / JSC «INTELI GENERICS NORD».
Address of Marketing Authorization Holder.
Seimyniskiu 3, 09312, Vilnius, Lithuania / Seimyniskiu 3, 09312, Vilnius, Lithuania.