Rigevidon
Ukraine
Table of Contents
INSTRUCTIONS for medical use of the medicinal product RIGEVIDON (RIGEVIDON)
Composition:
Active substances: levonorgestrel, ethinylestradiol;
One coated tablet contains levonorgestrel 0.15 mg and ethinylestradiol 0.03 mg;
Excipients: colloidal anhydrous silicon dioxide, magnesium stearate, talc, maize starch, lactose monohydrate, sodium carmellose, povidone K-30, polyethylene glycol (macrogol 6000), copovidone, titanium dioxide (E 171), calcium carbonate, sucrose.
Pharmaceutical form. Coated tablets.
Main physicochemical properties: white, round, biconvex coated tablets, 6 mm in diameter.
Pharmacotherapeutic group. Hormonal contraceptives for systemic use. Progestogens and estrogens, fixed combinations. ATC code G03A A07.
Pharmacological properties.
Pharmacodynamics.
Combined estrogen-progestogen oral contraceptives (mini-pills).
Pearl Index: 0.1 per 100 woman-years.
Rigevidon is a combined oral contraceptive (COC) containing ethinylestradiol and levonorgestrel. The efficacy of COCs is due to suppression of gonadotropin secretion, which results in inhibition of ovarian activity. The contraceptive effect is based on the interaction of several mechanisms, the most important of which is the inhibition of ovulation.
Pharmacokinetics.
Ethinylestradiol
Absorption
After oral administration, ethinylestradiol is rapidly and completely absorbed from the gastrointestinal tract; maximum plasma concentration (Cmax) is reached within 60–180 minutes. Due to presystemic conjugation and first-pass metabolism, absolute bioavailability is 40–45%. The area under the curve (AUC) and Cmax may slightly increase over time.
Distribution
Ethinylestradiol is 98.8% bound to plasma proteins, almost entirely to albumin.
Biotransformation
Ethinylestradiol undergoes presystemic conjugation in the mucosa of the small intestine and in the liver. Hydrolysis of direct conjugates of ethinylestradiol by intestinal flora regenerates free ethinylestradiol, which can be reabsorbed, thereby completing the enterohepatic circulation. The main metabolic pathway of ethinylestradiol is hydroxylation, mediated by cytochrome P450, resulting in the formation of primary metabolites – 2-OH-ethinylestradiol and 2-methoxyethinylestradiol. 2-OH-ethinylestradiol is further metabolized into chemically reactive metabolites.
Elimination
The elimination half-life (T½) of ethinylestradiol in plasma is approximately 29 hours (26–33 hours); plasma clearance ranges from 10 to 30 L/hour. Excretion of ethinylestradiol conjugates and metabolites occurs 40% via urine and 60% via feces.
Levonorgestrel
Absorption
After oral administration, levonorgestrel is rapidly and completely absorbed from the gastrointestinal tract. Levonorgestrel is fully bioavailable. After oral intake, Cmax of levonorgestrel in plasma is reached within 30–120 minutes. T½ is approximately 24–55 hours.
Distribution
Levonorgestrel binds to albumin and sex hormone-binding globulin (SHBG).
Biotransformation
It is mainly metabolized via reduction of the A-ring followed by glucuronidation. Metabolic clearance shows considerable individual variability, which may partly explain the observed differences in levonorgestrel concentrations among patients.
Elimination
The elimination half-life (T½) of levonorgestrel is approximately 36 hours. Approximately 60% of levonorgestrel is excreted in urine and 40% in feces.
Clinical characteristics.
Indications.
Oral contraception.
The decision to prescribe the drug Rigevidon should be made taking into account the woman's individual risk factors currently present, including risk factors for venous thromboembolism (VTE), as well as the risk of VTE associated with Rigevidon use compared to other combined hormonal contraceptives (CHCs) (see sections "Contraindications" and "Special precautions").
Contraindications.
Combined hormonal contraceptives (CHCs) must not be used in the presence of any of the conditions listed below. If any of the following conditions occurs for the first time during use of combined oral contraceptives, the use of oral contraceptives must be stopped immediately:
- Presence of or risk of venous thromboembolism (VTE):
- Venous thromboembolism – current VTE, including due to anticoagulant therapy, or history of VTE (e.g., deep vein thrombosis (DVT) or pulmonary embolism (PE));
- Known hereditary or acquired predisposition to VTE, such as activated protein C resistance (including factor V Leiden mutation), antithrombin III deficiency, protein C deficiency, protein S deficiency;
- Major surgery with prolonged immobilization (see section "Special precautions");
- High risk of VTE due to presence of multiple risk factors (see section "Special precautions");
- Presence of or risk of arterial thromboembolism (ATE):
- ATE – current arterial thromboembolism, history of ATE (e.g., myocardial infarction), or prodromal state (e.g., angina pectoris);
- Cerebrovascular disorders – current stroke, history of stroke, or presence of prodromal state (e.g., transient ischemic attack (TIA));
- Known hereditary or acquired predisposition to ATE, such as hyperhomocysteinemia and presence of antiphospholipid antibodies (anticardiolipin antibodies, lupus anticoagulant);
- History of migraine with focal neurological symptoms;
- High risk of ATE due to presence of multiple risk factors (see section "Special precautions") or due to presence of one of the following serious risk factors:
- Diabetes mellitus with vascular complications;
- Severe arterial hypertension;
- Severe dyslipoproteinemia;
- Current or past history of pancreatitis associated with severe hypertriglyceridemia;
- Presence or history of severe liver disease until liver function tests return to normal range;
- Presence or history of liver tumors (benign or malignant);
- Diagnosed or suspected hormone-dependent malignancies (e.g., of genital organs or breast);
- Vaginal bleeding of unknown etiology;
- Hypersensitivity to the active substances (levonorgestrel, ethinylestradiol) or to any of the excipients of the drug (see section "Composition");
- Concomitant use of Rigevidon with St. John’s wort (Hypericum perforatum) is contraindicated (see section "Interaction with other medicinal products and other forms of interaction").
Rigevidon is contraindicated for concomitant use with medicinal products containing ombitasvir/paritaprevir/ritonavir, dasabuvir, glecaprevir/pibrentasvir, and sofosbuvir/velpatasvir/voxilaprevir (see sections "Interaction with other medicinal products and other forms of interaction" and "Special precautions").
Interaction with other medicinal products and other forms of interaction.
Carefully review information on any concomitantly administered medicinal product to identify potential interactions.
Interactions between combined contraceptives and other substances may lead to increased or decreased plasma concentrations of estrogen and progestogen.
Reduced plasma concentrations of estrogen and progestogen may lead to increased frequency of intermenstrual bleeding and may reduce the efficacy of combined contraceptives.
Contraindicated combinations
St. John’s wort (Hypericum perforatum)
Decreased plasma concentrations of hormonal contraceptives due to enzyme-inducing effects of St. John’s wort, resulting in risk of reduced or even absent efficacy, which may lead to serious consequences (pregnancy).
Ombitasvir/paritaprevir/ritonavir, dasabuvir; glecaprevir/pibrentasvir; and sofosbuvir/velpatasvir/voxilaprevir
Increased hepatotoxicity.
Pharmacodynamic interactions
Concomitant use of Rigevidon with medicinal products containing ombitasvir/paritaprevir/ritonavir, dasabuvir (with or without ribavirin), glecaprevir/pibrentasvir, or sofosbuvir/velpatasvir/voxilaprevir may increase the risk of elevated ALT (see sections "Contraindications" and "Special precautions"). Therefore, women taking Rigevidon should switch to an alternative method of contraception (e.g., progestogen-only contraceptives or non-hormonal methods) prior to initiating therapy with the above-mentioned combination products. Use of Rigevidon may be resumed 2 weeks after completion of treatment.
Pharmacokinetic interactions
Effect of other medicinal products on Rigevidon
Interactions with medicinal products that induce microsomal enzymes may occur, leading to increased clearance of sex hormones and resulting in breakthrough bleeding and/or loss of contraceptive efficacy.
Treatment
Enzyme induction may be observed within a few days of treatment. Maximum enzyme induction generally occurs after several weeks. After discontinuation of the inducing agent, enzyme induction may persist for up to 4 weeks.
Short-term treatment
Women taking enzyme-inducing medicinal products should temporarily use a barrier method or another contraceptive method in addition to COCs. A barrier method should be used throughout the entire period of treatment with the enzyme-inducing agent and for an additional 28 days after discontinuation. If treatment with the enzyme-inducing agent continues beyond the last tablet of a 21-tablet pack, the next pack of COCs should be started immediately without a break.
Long-term treatment
Women undergoing long-term therapy with enzyme-inducing substances are advised to use another reliable non-hormonal method of contraception.
The following interactions have been reported according to published data.
Substances that increase COC clearance (reduced COC efficacy due to enzyme induction), e.g., barbiturates, bosentan, carbamazepine, phenytoin, primidone, rifampicin, and agents used for HIV treatment: ritonavir, nevirapine, and efavirenz; also possibly felbamate, griseofulvin, oxcarbazepine, topiramate, and medicinal products containing St. John’s wort (Hypericum perforatum).
Substances with variable effects on COC clearance
Concomitant use of COCs with a large number of HIV protease inhibitors and non-nucleoside reverse transcriptase inhibitors, including combinations with hepatitis C virus (HCV) inhibitors, may increase or decrease plasma concentrations of estrogens or progestins. The net effect of these changes may be clinically significant in some cases. Therefore, information on the medicinal product used for HIV/HCV treatment should be reviewed to identify potential interactions and any additional recommendations. In case of any doubts, women should additionally use a barrier method of contraception during therapy with protease inhibitors or non-nucleoside reverse transcriptase inhibitors.
Effect of Rigevidon on other medicinal products
COCs may affect the metabolism of other drugs. Therefore, plasma and tissue concentrations of active substances may be altered—either increased (e.g., cyclosporine) or decreased (e.g., lamotrigine).
Not recommended combinations
Enzyme inducers
Anticonvulsant drugs (phenobarbital, phenytoin, fosphenytoin, primidone, carbamazepine, oxcarbazepine), rifabutin, rifampicin, efavirenz, nevirapine, dabrafenib, enzalutamide, eslicarbazepine.
Reduced contraceptive efficacy due to enhanced hepatic metabolism of hormonal contraceptives by the inducer.
When using these drug combinations and during the following cycle, another method of contraception (e.g., mechanical) is recommended.
Lamotrigine (see also "Combinations requiring precautions" below)
Risk of reduced lamotrigine concentration and efficacy due to enhanced hepatic metabolism.
Oral contraceptives are not recommended during lamotrigine dose titration.
Protease inhibitors in combination with ritonavir
Amprenavir, atazanavir, darunavir, fosamprenavir, indinavir, lopinavir, ritonavir, saquinavir, and tipranavir
Risk of reduced contraceptive efficacy due to decreased plasma concentrations of hormonal contraceptives resulting from increased hepatic metabolism induced by ritonavir.
When using these drug combinations and during the following cycle, another method of contraception (e.g., condom or intrauterine device) is recommended.
Topiramate
Dose of topiramate ≥200 mg/day: risk of reduced contraceptive efficacy due to decreased estrogen concentration.
Another method of contraception (e.g., mechanical) is recommended.
Troleandomycin
May increase the risk of intrahepatic cholestasis when used concomitantly with COCs.
Modafinil
Risk of reduced contraceptive effect during and in the cycle following discontinuation of modafinil, as it is a microsomal liver enzyme inducer.
Standard oral contraceptives (not low-dose) or other contraceptive methods should be used.
Vemurafenib
Risk of decreased estrogen and progestogen concentrations, leading to potential contraceptive failure.
Perampanel
When perampanel is used at a dose ≥12 mg/day, there is a risk of reduced contraceptive effect. Alternative methods of contraception, preferably barrier methods, are recommended.
Ulipristal
Risk of progesterone antagonism. Combined contraceptives should not be resumed earlier than 12 days after discontinuation of ulipristal.
Combinations requiring precautions
Bosentan
Risk of reduced contraceptive efficacy due to enhanced hepatic metabolism of the hormonal contraceptive.
Use a reliable, additional, or alternative method of contraception during and in the cycle following concomitant use of this drug combination.
Griseofulvin
Risk of reduced contraceptive efficacy due to enhanced hepatic metabolism of the hormonal contraceptive.
Use of another method of contraception, especially mechanical, is advisable during and in the cycle following concomitant use of this drug combination.
Lamotrigine
Risk of reduced lamotrigine concentration and efficacy due to enhanced hepatic metabolism.
Clinical monitoring and dose adjustment of lamotrigine are recommended at the start and after discontinuation of oral contraceptives.
Rufinamide
Causes moderate reduction in ethinylestradiol concentration. Alternative contraceptive methods, preferably barrier methods, are recommended.
Elvitegravir
Reduced ethinylestradiol concentrations with risk of reduced contraceptive efficacy. Additionally, increased progestogen concentration is observed.
Use a combined contraceptive containing at least 30 mcg ethinylestradiol.
Apripritant
Reduced concentrations of combined contraceptives or progestogens with risk of reduced contraceptive efficacy.
Use of another method of contraception, especially mechanical, is advisable during and in the cycle following concomitant use of this drug combination.
Boceprevir
Risk of reduced contraceptive efficacy due to enhanced hepatic metabolism of the hormonal contraceptive by boceprevir.
Use a reliable, additional, or alternative method of contraception during concomitant use of this drug combination.
Telaprevir
Risk of reduced contraceptive efficacy due to enhanced hepatic metabolism of the hormonal contraceptive by telaprevir.
Use a reliable, additional, or alternative method of contraception during concomitant use of this drug combination and for the next two cycles.
Combinations to be used with caution
Etoricoxib
Increased ethinylestradiol concentration has been observed when used concomitantly with etoricoxib.
Laboratory tests
Use of contraceptive steroids may affect results of certain laboratory tests, including biochemical parameters of liver function, thyroid function, adrenal and renal function, as well as levels of plasma transport proteins such as corticosteroid-binding globulin and lipid/lipoprotein fractions; carbohydrate metabolism parameters; and coagulation and fibrinolysis parameters. Changes usually remain within normal laboratory reference ranges.
Special precautions
Special warnings
If any of the diseases or risk factors listed below are present, the beneficial effects of COCs should be weighed against the possible risks of their use in an individual woman, and the relevant benefits and risks should be discussed with her before she decides to use such medications. If any of these diseases or risk factors appear for the first time, worsen, or recur, the woman should consult her physician. The physician must decide whether COC use should be discontinued.
Circulatory disorders
Risk of venous thromboembolism (VTE)
The use of any combined oral contraceptive (COC) increases the risk of venous thromboembolism (VTE), such as deep vein thrombosis (DVT) or pulmonary embolism (PE), compared to non-use. COCs containing levonorgestrel, norgestimate, or norethisterone are associated with a lower risk of VTE. The decision to prescribe Rigevidon should only be made after discussing it with the woman. It is essential to ensure that she understands the risk of VTE associated with Rigevidon, how her individual risk factors may influence this risk, and that the risk of VTE is highest during the first year of using the medication. Some data suggest that the risk of VTE may increase when resuming COC use after a break of 4 weeks or more.
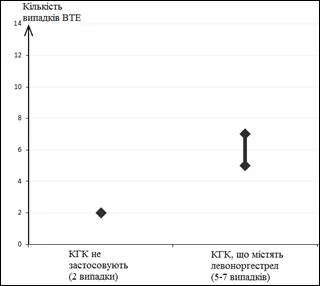
Among women who do not use COCs and are not pregnant, the incidence of VTE is approximately 2 cases per 10,000 women per year. However, in any individual woman, the risk level may be significantly higher depending on her underlying risk factors (see below).
It has been estimated that among 10,000 women using COCs containing levonorgestrel, approximately 6 cases of VTE will occur per year.
The number of VTE cases per year is lower than that typically expected during pregnancy or the postpartum period.
VTE can be fatal in 1–2% of cases.
1 On average, 5–7 cases per 10,000 woman-years, based on the relative risk of COCs containing levonorgestrel compared to non-users of COCs (approximately 2.3–3.6 cases).
Number of VTE cases per 10,000 women per year
Very rarely, thrombosis in other blood vessels—for example, in the arteries or veins of the liver, kidneys, retina, or mesenteric vessels—has been reported in women using contraceptive tablets.
Risk factors for VTE
The risk of developing venous thromboembolic complications while using COCs may be substantially increased in women with additional risk factors, particularly when multiple risk factors are present (see Table 1).
Rigevidon is contraindicated in women with multiple risk factors that place them at high risk of venous thrombosis (see section "Contraindications"). If a woman has more than one risk factor, the increase in risk may be greater than the sum of the risks associated with each individual factor; therefore, the overall risk of VTE should be considered. COCs should not be prescribed if the benefit-risk balance is unfavorable (see section "Contraindications").
Table 1
Risk factors for VTE
| Risk factor |
Note |
| Obesity (body mass index (BMI) over 30 kg/m²). |
Risk increases significantly with increasing BMI. Particular attention is required in women with other risk factors. |
| Long-term immobilization, major surgery, any surgery on legs or pelvic organs, neurosurgery, or extensive trauma. Note: temporary immobilization, including air travel over 4 hours, may also be a risk factor for VTE, especially in women with other risk factors. |
In such cases, it is recommended to discontinue the use of the patch/tablets/ring (at least 4 weeks before elective surgery) and not resume use until at least 2 weeks after full resumption of mobility. To avoid unintended pregnancy, another contraceptive method should be used. Antithrombotic therapy should be considered if use of Rigevidon has not been discontinued in advance. |
| Family history (VTE in a sibling or parent, especially at a relatively young age, e.g., under 50 years). |
If hereditary predisposition is suspected, women should consult a specialist before using any COC. |
| Other conditions associated with VTE |
Cancer, systemic lupus erythematosus, hemolytic-uremic syndrome, chronic inflammatory bowel disease (Crohn’s disease or ulcerative colitis), and sickle cell anemia. |
| Increasing age |
Particularly individuals aged 35 years and older. |
There is no consensus regarding the possible influence of varicose veins and superficial thrombophlebitis on the development or progression of venous thrombosis.
Particular attention should be paid to the increased risk of thromboembolism during pregnancy, especially during the first 6 weeks postpartum (see section "Use in pregnancy or breastfeeding").
Signs and symptoms of VTE (DVT and PE)
If any of the symptoms listed below occur, women should seek immediate medical attention and inform their physician that they are taking COCs.
Symptoms of deep vein thrombosis (DVT) may include:
- Unilateral leg and/or foot swelling, or swelling along a vein in the leg;
- Pain or increased sensitivity in the leg, which may only be felt when standing or walking;
- A sensation of warmth in the affected leg; redness or discoloration of the skin on the leg.
Symptoms of PE may include:
- Sudden unexplained shortness of breath or rapid breathing;
- Sudden onset of cough, which may be accompanied by hemoptysis;
- Sudden chest pain;
- Presyncope or dizziness;
- Rapid or irregular heartbeat.
Some of these symptoms (e.g., shortness of breath, cough) are nonspecific and may be misinterpreted as more common or less severe conditions (e.g., respiratory tract infections).
Other signs of vascular occlusion may include sudden pain, swelling, and mild cyanosis of a limb.
In occlusion of ocular vessels, initial symptoms may include blurred vision without pain, which may progress to vision loss. Sometimes, vision loss occurs almost instantaneously.
Risk of ATE
Epidemiological studies have shown that the use of any COCs is associated with an increased risk of ATE (myocardial infarction) or cerebrovascular events (e.g., transient ischemic attack, stroke). Arterial thromboembolic events can be fatal.
ATE risk factors
When using COCs, the risk of developing arterial thromboembolic complications or cerebrovascular events increases in women with risk factors (see Table 2). Rigevidon is contraindicated if a woman has one serious or multiple risk factors that may increase the risk of arterial thrombosis (see section "Contraindications"). If a woman has more than one risk factor, the increase in risk may be greater than the sum of the risks associated with each individual factor; therefore, the overall risk of ATE should be considered. COCs should not be prescribed if the benefit-risk ratio is unfavorable (see section "Contraindications").
Table 2
ATE risk factors
| Increased age |
Particularly individuals aged 35 years and older. |
| Smoking |
Women who wish to use COCs should be advised to stop smoking. Women aged 35 years and older who continue to smoke should be strongly advised to use a different method of contraception. |
| Arterial hypertension |
|
| Obesity (BMI greater than 30 kg/m²) |
Risk increases significantly with increasing BMI. Requires particular attention when other risk factors are present in women. |
| Family history (arterial thromboembolism in a sibling or parent, especially at a relatively young age, e.g., under 50 years). |
If there is suspicion of hereditary predisposition, women should be advised to consult a specialist before using any COCs. |
| Migraine |
An increase in the frequency or severity of migraine during COC use (which may be a prodromal sign of cerebrovascular events) may necessitate immediate discontinuation of COCs. |
| Other conditions associated with adverse vascular reactions |
Diabetes mellitus, hyperhomocysteinemia, heart valve disorders, atrial fibrillation, dyslipoproteinemia, and systemic lupus erythematosus. |
Arterial Thromboembolism (ATE) Symptoms
If any of the symptoms listed below occur, women should seek immediate medical attention and inform their doctor that they are taking COCs.
Symptoms of cerebrovascular disorders may include:
- sudden numbness or weakness of the face, arms, or legs, especially on one side of the body;
- sudden difficulty walking, dizziness, loss of balance or coordination;
- sudden confusion, speech or comprehension difficulties;
- sudden vision problems in one or both eyes;
- sudden severe or prolonged headache with no known cause;
- loss of consciousness or fainting, with or without seizures.
Transient symptoms may indicate a transient ischemic attack (TIA).
Symptoms of myocardial infarction (MI) may include:
- pain, discomfort, pressure, heaviness, squeezing, or fullness in the chest, arm, or behind the breastbone;
- discomfort radiating to the back, jaw, throat, arm, or abdomen;
- a feeling of fullness, indigestion, or choking;
- excessive sweating, nausea, vomiting, or dizziness;
- extreme weakness, restlessness, or shortness of breath;
- rapid or irregular heartbeat.
Tumors
Cervical Cancer
Some epidemiological studies have reported an increased risk of cervical cancer in women who have used COCs for a long time (>5 years). However, this observation remains controversial, as it is not fully established whether study results adequately account for confounding risk factors such as sexual behavior and human papillomavirus (HPV) infection.
Breast Cancer
A meta-analysis of data from 54 epidemiological studies indicates a slight increase in relative risk (RR = 1.24) of developing breast cancer in women using COCs. This increased risk gradually decreases over 10 years after stopping COCs. Since breast cancer is rare in women under 40 years of age, the increase in diagnosed cases among women currently or recently using COCs is small compared to the overall lifetime risk of breast cancer. The studies do not provide evidence of a causal relationship.
The increased risk may be related to earlier diagnosis of breast cancer in women using COCs, the biological effects of COCs, or a combination of both factors. Breast cancer is diagnosed at a slightly earlier stage in women using oral contraceptives compared to those who have not used COCs.
Liver Tumors
In rare cases, benign (adenoma, focal nodular hyperplasia) and even more rarely malignant liver tumors have been observed in women taking COCs. In individual cases, these tumors may lead to life-threatening intra-abdominal hemorrhage. The possibility of a liver tumor should be considered in the differential diagnosis when women taking COCs present with severe upper abdominal pain, hepatomegaly, or signs of intra-abdominal bleeding.
The use of COCs at high doses (50 mcg ethinylestradiol) reduces the risk of endometrial and ovarian cancer. It remains to be confirmed whether these findings also apply to low-dose COCs.
Other Conditions
Depression
Depressed mood and depression are common adverse reactions associated with hormonal contraceptives (see section "Adverse Reactions"). Depression can be severe and is a known risk factor for suicidal behavior and suicide. Women should be advised to contact their doctor if they experience mood changes or symptoms of depression, even if these occur shortly after starting treatment.
Hypertriglyceridemia
Women with hypertriglyceridemia or a family history of this condition are at increased risk of developing pancreatitis while using COCs.
Arterial Hypertension
A slight increase in blood pressure has been reported in many women using COCs, although clinically significant elevations are rare. In only rare cases has immediate discontinuation of COCs been warranted. If blood pressure continues to rise during COC use in women with pre-existing hypertension, or if a significant increase in blood pressure does not respond adequately to antihypertensive treatment, COC use should be discontinued. In some cases, COC use may be resumed if normal blood pressure values can be achieved with antihypertensive therapy.
Liver Disease
Acute or chronic impairment of liver function may require discontinuation of COCs until liver function tests return to normal.
Angioedema
Exogenous estrogens may induce or exacerbate symptoms of hereditary or acquired angioedema.
Glucose Tolerance/Diabetes Mellitus
Although COCs may affect peripheral insulin resistance and glucose tolerance, there are no data indicating a need to change the therapeutic regimen in women with diabetes who are taking low-dose COCs (containing <0.05 mg ethinylestradiol). However, women with diabetes should be under close medical supervision throughout the duration of COC use.
Other Conditions
COC use should be discontinued if cholestatic jaundice recurs, which initially occurred during pregnancy or previous use of sex steroid hormones.
Cases of development or worsening of the following conditions have been reported during pregnancy and COC use (causal relationship with COC use not established): jaundice and/or pruritus associated with cholestasis; gallstone formation; porphyria; systemic lupus erythematosus; hemolytic uremic syndrome; Sydenham's chorea; herpes gestationis; hearing loss associated with otosclerosis.
Worsening of endogenous depression, epilepsy, Crohn's disease, and ulcerative colitis has been observed during COC use.
Chloasma may occasionally occur, particularly in women with a history of chloasma of pregnancy. Women prone to chloasma should avoid direct sunlight or ultraviolet radiation while using COCs.
Special attention should be given to patients with hyperprolactinemia.
Medical Examination/Consultation
Before initiating or resuming use of Rigevirone, a thorough patient history, including family history, should be taken, and pregnancy should be ruled out. Blood pressure should be measured, and a general physical examination should be performed, considering contraindications (see section "Contraindications") and special warnings (see section "Special Precautions"). It is important to inform women about venous and arterial thrombosis, including the risk associated with using Rigevirone compared to other COCs, symptoms of VTE and ATE, known risk factors, and what to do in case of suspected thrombosis. The package insert must be carefully read and its recommendations followed. The frequency and nature of examinations should be based on current medical practice guidelines, taking into account individual patient characteristics.
Women should be informed that oral contraceptives do not protect against HIV infection (AIDS) or other sexually transmitted diseases.
Reduced Effectiveness
The effectiveness of COCs may be reduced, for example, if doses are missed (see section "Dosage and Administration"), or in cases of vomiting or diarrhea (see section "Dosage and Administration"), or when used concomitantly with other medicinal products (see section "Interaction with Other Medicinal Products and Other Forms of Interaction").
Reduced Cycle Control
As with all COCs, irregular bleeding (spotting or breakthrough bleeding) may occur, particularly during the first few months of use. Therefore, evaluation of any irregular bleeding should only be conducted after the body has had time to adapt to the medication, which typically takes about three cycles.
If irregular bleeding persists or occurs after several regular cycles, non-hormonal causes should be considered, and appropriate diagnostic measures should be undertaken to exclude malignancy or pregnancy. Such measures may include curettage.
In some women, menstruation may not occur during the usual pill-free interval. If COCs have been taken according to the instructions in the section "Dosage and Administration," pregnancy is unlikely. However, if the instructions in the section "Dosage and Administration" were not followed before the first missed withdrawal bleed, or if menstruation is absent for two consecutive cycles, pregnancy should be ruled out before continuing COC use.
Elevated ALT Levels
During clinical trials in patients receiving medications for hepatitis C virus (HCV) infection containing ombitasvir/paritaprevir/ritonavir and dasabuvir with or without ribavirin, increases in transaminase (ALT) levels greater than five times the upper limit of normal were observed. This occurred more frequently in women using medicinal products containing ethinylestradiol, such as COCs. Increased ALT levels have also been observed with antiviral medicinal products containing glecaprevir/pibrentasvir and sofosbuvir/velpatasvir/voxilaprevir (see sections "Contraindications" and "Interaction with Other Medicinal Products and Other Forms of Interaction").
Excipients
Rigevirone, coated tablets, contains lactose monohydrate. Women with rare hereditary problems of galactose intolerance, total lactase deficiency, or glucose-galactose malabsorption should not take this medicine.
Rigevirone, coated tablets, contains sucrose. Women with rare hereditary fructose intolerance, glucose-galactose malabsorption, or sucrase-isomaltase insufficiency should not take this medicine.
Rigevirone, film-coated tablets, contains sodium carmellose.
One coated tablet contains less than 1 mmol (23 mg)/dose of sodium, i.e., the medicine is essentially "sodium-free."
Use during Pregnancy or Breastfeeding
Pregnancy
Rigevirone is not indicated during pregnancy.
If a woman becomes pregnant while taking Rigevirone, treatment should be discontinued immediately.
Results from numerous epidemiological studies have not shown an increased risk of congenital malformations in children born to women who used COCs prior to pregnancy, nor teratogenic effects from inadvertent use of contraceptive tablets in early pregnancy. When resuming use of Rigevirone, the increased risk of VTE in the postpartum period should be considered (see sections "Special Precautions" and "Dosage and Administration").
Breastfeeding Period
Oral hormonal contraceptives may affect lactation by reducing the quantity and altering the composition of breast milk. Therefore, the use of COCs is not recommended until breastfeeding is discontinued. Small amounts of contraceptive steroids and/or their metabolites may pass into breast milk and may affect the infant. If a woman wishes to breastfeed, alternative contraceptive methods should be recommended.
Ability to affect reaction speed when driving vehicles or operating machinery
No studies on the effect on the ability to drive or operate machinery have been conducted. No effect on the ability to drive vehicles or operate machinery has been observed in women using COCs.
Method of Administration and Dosage
Method of Administration
How to take Rigevidon
Orally, in the order indicated on the packaging, approximately at the same time each day, with a small amount of liquid if necessary.
Rigevidon should be taken daily, one tablet per day, for 21 consecutive days. Each subsequent pack should be started after a 7-day break, during which withdrawal bleeding usually occurs (typically beginning on days 2–3 after taking the last tablet and may continue until the start of the next pack).
Starting Rigevidon
If no hormonal contraceptives were used in the previous month
Begin tablet intake on the first day of the natural cycle, i.e., the first day of menstrual bleeding.
Switching from another combined oral contraceptive (COC), vaginal ring, or transdermal patch
Start Rigevidon the day after taking the last active tablet of the previous contraceptive, but no later than the day following the tablet-free interval of the previous contraceptive.
The first tablet should be taken on the day of removal of the vaginal ring or transdermal patch, but not later than the day when a new transdermal patch should be applied or a new ring inserted.
Switching to Rigevidon from a progestogen-only contraceptive (progestogen-only pills, "mini-pills", injection, implant, or intrauterine system containing progestogen)
Switching from mini-pills can occur on any day of the menstrual cycle. Rigevidon should be started the day after discontinuing the mini-pill.
Switching from an implant or intrauterine system – on the day of removal; from an injection – on the day the next injection would have been due.
In all cases, it is recommended to use an additional contraceptive method for the first 7 days of tablet intake.
After first-trimester abortion
Begin Rigevidon immediately on the same day as the procedure. In this case, additional contraceptive methods are not required.
After childbirth or second-trimester abortion
Rigevidon should be started on days 21–28 postpartum or after second-trimester abortion, and only if breastfeeding is not planned, due to the increased risk of thromboembolic disorders during the postpartum period. If Rigevidon is started later, barrier contraceptive methods should be used additionally for the first 7 days of treatment. However, if sexual intercourse has already occurred, possible pregnancy should be ruled out before starting Rigevidon, or the woman should wait for the first menstrual period.
Lactation period
See section "Use during pregnancy or breastfeeding".
Missed tablet intake
Contraceptive efficacy may decrease if tablets are missed, especially if the interval between taking the last tablet of the current blister pack and the first tablet of the next pack is prolonged.
If less than 12 hours have passed since the missed tablet was due, contraceptive protection is not reduced. The woman should take the missed tablet as soon as she remembers, and take the next tablet at the usual time.
If more than 12 hours have passed since the missed tablet was due, contraceptive protection may be reduced. In this case, follow these two main rules:
- The tablet-free interval must never exceed 7 days.
- Adequate suppression of the hypothalamic–pituitary–ovarian system is achieved only after 7 consecutive days of tablet intake.
Based on the above, the following practical recommendations should be followed:
Week 1
The missed tablet should be taken immediately upon remembering, even if this means taking two tablets at the same time. Continue taking tablets at the usual time. Additionally, use barrier contraception (e.g., condoms) for the next 7 days. If unprotected intercourse occurred within the previous 7 days, consider the possibility of pregnancy. The risk of pregnancy increases with the number of missed tablets and the closer the missed dose is to the 7-day break.
Week 2
The missed tablet should be taken immediately upon remembering, even if two tablets must be taken at the same time. Continue taking tablets at the usual time. If the woman has taken tablets correctly for the 7 days prior to the missed dose, no additional contraceptive methods are needed. Otherwise, or if more than one tablet is missed, use barrier contraception for 7 days.
Week 3
The risk of significantly reduced contraceptive protection is inevitable due to the upcoming 7-day break. However, contraceptive protection can be maintained by following one of the options below, provided tablets were taken correctly for the 7 days before the missed dose. If this is not the case, follow the first option below and use additional barrier contraception (e.g., condoms) for the next 7 days.
- Take the missed tablet immediately upon remembering, even if two tablets must be taken at the same time. Continue taking tablets at the usual time. The next pack should be started the day after the last tablet of the current pack, i.e., without a break between packs. Withdrawal bleeding before the end of the second pack is unlikely, although spotting or breakthrough bleeding may occur.
- Alternatively, the woman may discontinue the current pack. In this case, she should take a break of up to 7 days (including the days when tablets were missed), then start the next pack.
If a woman misses tablets and does not experience withdrawal bleeding during the first usual break, pregnancy should be considered.
Gastrointestinal disturbances
In cases of severe gastrointestinal disturbances (vomiting or diarrhea), incomplete absorption of the drug may occur; therefore, additional contraceptive methods should be used. If vomiting or severe diarrhea occurs within 3–4 hours after taking a tablet, take a new tablet as soon as possible. Ideally, the new tablet should be taken within 12 hours of the usual intake time. If more than 12 hours have passed, follow the instructions under "Missed tablet intake".
If a woman does not wish to change her usual tablet-taking schedule, she should take additional tablet(s) from another pack.
Delaying or shifting menstruation
To delay withdrawal bleeding, start the next pack the day after finishing the current pack, without a break. Breakthrough bleeding or spotting may occur during this period. Regular use of Rigevidon can be resumed after the usual 7-day break.
To shift the day of menstruation to another day of the week, shorten the 7-day break by the desired number of days.
The shorter the break, the less likely withdrawal bleeding will occur, and breakthrough or spotting bleeding may occur during intake of tablets from the next pack (as with delaying menstruation). It is important to emphasize that the tablet-free interval must not be extended.
Method of Administration
Oral.
Children
The drug is not intended for use in children.
Overdose
Symptoms of overdose with oral contraceptives have been reported in adults, adolescents, and children up to 12 years of age.
Symptoms that may occur in overdose include: nausea, vomiting, breast tenderness, dizziness, abdominal pain, somnolence/weakness, and vaginal bleeding in young girls.
There is no specific antidote; treatment should be symptomatic.
Adverse reactions.
Adverse reactions reported with concomitant use of ethinylestradiol and levonorgestrel are listed below.
The most serious adverse effects, such as venous and arterial thromboembolism, cervical cancer, breast cancer, and malignant liver tumors, are described in the section "Special precautions".
In women taking COCs, an increased risk of arterial and venous thrombotic and thromboembolic complications, including myocardial infarction, stroke, transient ischemic attack (TIA), venous thrombosis, and pulmonary embolism, has been observed. More detailed information is provided in the section "Special precautions".
| System organ class |
Common (≥1/100, <1/10) |
Uncommon (≥1/1000, <1/100) |
Rare (≥1/10000, <1/1000) |
Very rare (<1/10 000) |
Frequency not known (cannot be estimated from available data) |
| Infections and infestations |
Vaginitis, including vaginal candidiasis |
||||
| Benign, malignant and unspecified neoplasms (including cysts and polyps) |
Hepatocellular carcinoma, benign liver tumours (focal nodular hyperplasia, hepatic adenoma) |
||||
| Immune system disorders |
Increased sensitivity, anaphylactic reactions with very rare cases of urticaria, angioedema, circulatory collapse and severe respiratory distress |
Exacerbation of systemic lupus erythematosus |
Worsening of symptoms in hereditary and acquired angioedema |
||
| Metabolism and nutrition disorders |
Changes in appetite (increase or decrease) |
Impaired glucose tolerance |
Exacerbation of porphyria |
||
| Psychiatric disorders |
Mood changes, including depression, change in libido |
||||
| Nervous system disorders |
Headache, increased irritability, dizziness |
Migraine |
Exacerbation of chorea |
||
| Eye disorders |
Intolerance to contact lenses |
Optic neuritis, retinal vascular thrombosis |
|||
| Vascular disorders |
Arterial hypertension |
Venous thromboembolism (VTE), arterial thromboembolism (ATE) |
Worsening of varicose vein disease |
||
| Gastrointestinal disorders |
Nausea, vomiting, abdominal pain |
Diarrhea, abdominal cramps, bloating |
Ischaemic colitis |
Inflammatory bowel diseases (Crohn's disease, ulcerative colitis) |
|
| Hepatobiliary disorders |
Cholestatic jaundice |
Pancreatitis, gallstones, cholestasis |
Hepatocellular damage (e.g., hepatitis, liver function abnormalities) |
||
| Skin and subcutaneous tissue disorders |
Acne |
Rash, urticaria, chloasma (melanoderma) with risk of persistence, hirsutism, hair loss |
Nodular erythema |
Multiform erythema |
|
| Renal and urinary disorders |
Haemolytic-uraemic syndrome |
||||
| Reproductive system and breast disorders |
Breast pain, tenderness, swelling and discharge, dysmenorrhoea, menstrual cycle disturbances, cervical ectropion and vaginal discharge, amenorrhoea |
||||
| General disorders |
Fluid retention/edema, change in body weight (increase or decrease) |
||||
| Investigations |
Changes in serum lipid levels, including hypertriglyceridaemia |
Decreased serum folate levels |
In women using COCs, the following serious adverse reactions have been reported, as described in section "Special warnings and precautions for use":
- venous thromboembolic disorders;
- arterial thromboembolic disorders;
- arterial hypertension;
- liver tumours;
- Crohn’s disease, ulcerative colitis, porphyria, systemic lupus erythematosus, herpes gestationis, Sydenham’s chorea, haemolytic uraemic syndrome, cholestatic jaundice.
The incidence of diagnosed breast cancer is slightly increased in women taking COCs. Since breast cancer is rare in women under 40 years of age, the increase in the number of diagnosed cases of breast cancer among women currently or recently using COCs is small in relation to the overall risk of breast cancer. A causal relationship with COC use has not been established. For further information, see sections "Contraindications" and "Special warnings and precautions for use".
Interactions
Breakthrough bleeding and/or a reduction in contraceptive efficacy may occur due to interactions between other medicinal products (enzyme inducers) and oral contraceptives.
Reporting of suspected adverse reactions
Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit-risk balance of the medicinal product. Healthcare professionals are encouraged to report suspected adverse reactions.
Shelf life. 30 months.
Storage conditions.
Store at temperatures not exceeding 25 °C.
Keep the medicine out of the reach of children.
Packaging.
21 coated tablets in a blister; 1 or 3 blisters with a cardboard blister holder in a carton.
Prescription category. Prescription only.
Manufacturer. Gedeon Richter Plc., Hungary.
Manufacturer's address and location of operations.
H-1103 Budapest, Demrédi út 19-21, Hungary.