Poltech mibi
Ukraine INSTRUCTION |
Poltech MIBI |
Composition:active substance: Tetrakis (2–methoxy–2–methylpropyl–1–isocyanide) copper (1+) tetrafluoroborate; 1 vial contains Tetrakis (2–methoxy–2–methylpropyl–1–isocyanide) copper (1+) tetrafluoroborate excipients: tin chloride dihydrate, L–cysteine hydrochloride monohydrate, sodium citrate dihydrate, D–mannitol. The vial contains less than 1 mmol (23 mg) of sodium. Radionuclides are not part of the kit. |
| Pharmaceutical form. Kit for the preparation of a radiopharmaceutical. Main physico–chemical properties: white lyophilized powder. |
| Pharmacotherapeutic group. Diagnostic radiopharmaceuticals with technetium (99mTc). ATC Code: V09G A01. |
Pharmacological properties.Pharmacodynamics. Chemical concentrations used for diagnostic imaging with technetium (99mTc) sestamibi do not exhibit any pharmacological effect. Pharmacokinetics. After dissolution with sodium pertechnetate (99mTc), the following technetium (99mTc) sestamibi complex is formed: [99mTc (MIBI)6]+, where: MIBI = 2–Methoxyisobutylisonitrile Biodistribution Technetium (99mTc) sestamibi rapidly distributes from the blood: only about 8% of the administered dose remains in the blood 5 minutes after injection. In physiological distribution, visible uptake of technetium (99mTc) sestamibi can be observed in vivo in several organs. In particular, normal uptake is observed in salivary glands, thyroid gland, myocardium, liver, gallbladder, small and large intestine, kidneys, urinary bladder, joint spaces, and skeletal muscles, occasionally in the nipples. Moderate homogeneous uptake in the breasts or inguinal regions is normal. Myocardial perfusion scintigraphy Technetium (99mTc) sestamibi is a lipophilic cationic complex that passively diffuses through capillaries and cell membranes. The agent localizes intracellularly in mitochondria, where it becomes trapped, and retention depends on intact mitochondrial membrane potential, reflecting viable myocytes. After intravenous administration, the agent distributes in the myocardium proportionally to perfusion and viability. Myocardial uptake, dependent on coronary blood flow, amounts to 1.5% of the administered dose during stress and 1.2% at rest. However, irreversibly damaged cells do not take up technetium (99mTc) sestamibi. Myocardial retention decreases under hypoxic conditions. The agent shows minimal redistribution; therefore, separate studies are required for stress and rest conditions. Scintimammography Tissue uptake of technetium (99mTc) sestamibi primarily depends on vascularization, which is typically increased in tumor tissue. Technetium (99mTc) sestamibi accumulates in various tumors and is most prominently localized in mitochondria. Its uptake is associated with increased energy-dependent metabolism and cellular proliferation. Cellular accumulation decreases when multidrug resistance proteins are overexpressed. Parathyroid and hyperfunctioning tissue scintigraphy Technetium (99mTc) sestamibi localizes in both parathyroid tissue and functioning thyroid tissue, but it usually washes out from normal thyroid tissue faster than from abnormal parathyroid tissue. Elimination Elimination of technetium (99mTc) sestamibi occurs mainly via the kidneys and hepatobiliary system. Technetium (99mTc) sestamibi activity from the gallbladder moves into the intestine within 1 hour after administration. Approximately 27% of the administered dose is excreted via the kidneys within 24 hours, and about 33% of the administered dose is excreted in feces within 48 hours. Pharmacokinetics in patients with renal or hepatic impairment has not been studied. Elimination half-life The biological half-life of technetium (99mTc) sestamibi is approximately 7 hours under both rest and stress conditions. The effective half-life (which includes both biological and physical half-lives) is approximately 3 hours for the heart and approximately |
Clinical characteristics.Indications. This medicinal product is intended solely for diagnostic use. After radiolabeling with sodium pertechnetate (99mTc) solution, the resulting technetium (99mTc) sestamibi is indicated for:
|
| Contraindications. Hypersensitivity to the active substance or to any of the excipients. For myocardial scintigraphy under stress conditions, general contraindications related to the induction of ergometric or pharmacological stress should be considered. |
| Special safety precautions. Occurrence of hypersensitivity or anaphylactic reactions In case of hypersensitivity or anaphylactic reactions, administration of the medicinal product should be immediately discontinued and, if necessary, intravenous treatment should be initiated. Necessary medicinal products and equipment, such as an intubation tube and ventilator, should be prepared in advance to ensure prompt emergency assistance. Justification of individual benefit/risk For each patient, radiation exposure must be justified by the probable benefit. The radioactive dose should always be as low as reasonably achievable to obtain the necessary diagnostic information. Renal or hepatic impairment A careful assessment of the risk/benefit ratio should be performed for such patients, as increased radiation exposure may occur. Patient preparation The patient should drink plenty of fluids before the examination and should empty the bladder as frequently as possible during the first hours after the procedure to reduce radiation exposure. Cardiac tomography If possible, the patient should fast for at least 4 hours prior to the examination. It is recommended that patients consume a light fatty meal or drink one or two glasses of milk after each injection before scanning. This promotes rapid hepatobiliary clearance of technetium (99mTc) sestamibi and reduces hepatic activity. Justification of imaging with technetium (99mTc) sestamibi Justification of scintimammography Lesions of the breast smaller than 1 cm in diameter may not always be detected by scintimammography, as the sensitivity of technetium (99mTc) sestamibi for detecting such lesions is low. Negative findings do not exclude breast cancer, especially in such small lesions. After the procedure Close contact with children and pregnant women should be limited for 24 hours after administration. Special precautions When performing myocardial infarction scintigraphy under stress conditions, general contraindications and precautions related to ergometric and pharmacological stress should be considered. This medicinal product contains less than 1 mmol (23 mg) of sodium per vial, i.e., essentially "sodium-free". Dosimetry Technetium (99mTc) from the (99Mo/99mTc) radionuclide generator decays with emission of gamma radiation with a mean energy of 140 keV and a half-life of 6.02 hours to technetium (99Tc), which has a very long half-life of 2.13 × 105 years and can therefore be considered practically stable. The data below are from ICRP 80 and are calculated based on the following assumptions: after intravenous administration, the radiopharmaceutical rapidly clears from the blood and is predominantly taken up in muscle tissues (including the heart), liver, and kidneys, with lower uptake in salivary glands and thyroid gland. When administered in conjunction with stress, there is a significant increase in uptake in the heart and skeletal muscles, correspondingly reducing accumulation in other organs. The radiopharmaceutical is excreted via the liver and kidneys in proportions of 75% and 25%, respectively.
Effective dose calculated based on a 3.5-hour bladder emptying frequency in adults. Cardiac imaging The effective dose following administration of the maximum recommended activity of 2000 MBq of technetium (99mTc) sestamibi in adults with a body weight of 70 kg is 16.4 mSv. For a one-day protocol, an activity of 500 MBq at rest and 1500 MBq under stress is used. For the administered activity of 2000 MBq, typical radiation doses to target organs are: Heart – 14 mGy, and typical radiation doses to critical organs (gallbladder, kidneys, and upper large intestine) are 69, 57, and 46.5 mGy, respectively. The effective dose following administration of the maximum recommended activity of 1800 MBq (900 MBq at rest and 900 MBq under stress) of technetium (99mTc) sestamibi in a two-day protocol for adults with a body weight of 70 kg is 15.2 mSv. For the administered activity of 1800 MBq, typical radiation doses to target organs are: Heart – 12.2 mGy, and typical radiation doses to critical organs (gallbladder, kidneys, and upper large intestine) are 64.8, 55.8, and 44.1 mGy, respectively. Scintimammography The effective dose following administration of the maximum recommended activity of 1000 MBq of technetium (99mTc) sestamibi in adults with a body weight of 70 kg is 9 mSv. For the administered activity of 1000 MBq, typical radiation doses to target organs are: Breast – 3.8 mGy, and typical radiation doses to critical organs (gallbladder, kidneys, and upper large intestine) are 39, 36, and 27 mGy, respectively. Parathyroid gland tomography The effective dose following administration of the maximum recommended activity of 700 MBq of technetium (99mTc) sestamibi in adults with a body weight of 70 kg is 6.3 mSv. For the administered activity of 700 MBq, typical radiation doses to target organs are: Thyroid gland – 3.7 mGy, and typical radiation doses to critical organs (gallbladder, kidneys, and upper large intestine) are 27.3, 25.2, and 18.9 mGy, respectively. Special precautions Radiopharmaceuticals may only be obtained, administered, and prescribed by authorized personnel licensed to work with radiopharmaceuticals and within appropriate clinical settings. Their acquisition, storage, use, transfer, and disposal are regulated by applicable regulations and/or appropriate licenses issued by local authorities. Radiopharmaceuticals must be prepared by the user in a manner ensuring appropriate radiological safety and pharmaceutical quality. Appropriate aseptic precautions must be observed. The vial contents are intended solely for preparation of the radiopharmaceutical technetium (99mTc) sestamibi and must not be administered directly to the patient without prior radiopharmaceutical preparation. The kit contents are non-radioactive prior to reconstitution. However, after adding sodium pertechnetate (99mTc), appropriate shielding of the final preparation must be ensured. Administration of radiopharmaceuticals creates a risk of ionizing radiation exposure or contamination (e.g., from urine spillage, vomiting) to other individuals. Radiation protection measures must be followed in accordance with current regulations when handling ionizing radiation sources. Any unused medicinal product or waste must be disposed of in accordance with local regulations. After use, the container and any unused radiopharmaceutical must be disposed of according to local requirements for radioactive materials. |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Interaction with other medicinal products and other forms of interaction. Medicinal products affecting myocardial function and/or circulation may lead to false-negative results in the diagnosis of coronary artery disease. In particular, beta-blockers and calcium antagonists reduce oxygen consumption and thus also affect perfusion, and beta-blockers prevent increases in heart rate and blood pressure during stress. Concomitant medications must be considered when interpreting scintigraphy results. Recommendations for ergometric and pharmacological stress testing should be followed. When subtraction scintigraphy technique is used for evaluation of parathyroid hyperfunction, recent use of iodine-containing contrast agents, medications used to treat hyper- or hypothyroidism, or several other medicinal products may reduce thyroid image quality or even render subtraction impossible. For a complete list of potential drug interactions, refer to the summary of product characteristics for sodium iodide (123I) or sodium pertechnetate (99mTc). Children Interaction studies have not been conducted. |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Special instructions for use.Use during pregnancy or breastfeeding. Women of reproductive age When administering radiopharmaceuticals to women of reproductive age, it is essential to determine whether the woman is pregnant. Any woman with a delayed menstrual period should be considered pregnant until proven otherwise. If there is uncertainty regarding possible pregnancy (e.g., delayed menstruation with irregular cycles), the patient should be offered alternative diagnostic methods (if available) that do not involve ionizing radiation. Pregnancy Radiopharmaceutical procedures performed during pregnancy also involve radiation exposure to the fetus. Therefore, such procedures should only be performed when the potential benefit clearly outweighs the risk to both mother and fetus. Breastfeeding Before administering a radiopharmaceutical to a breastfeeding woman, consideration should be given to postponing radionuclide administration until after breastfeeding has ended. The choice of radiopharmaceutical should carefully consider the extent of radioactivity excretion into breast milk. If administration of the radiopharmaceutical is necessary, breastfeeding should be interrupted for Fertility Studies have not been conducted. Ability to affect reaction speed when driving or operating machinery. The radioactive medicinal product does not affect the ability to drive or operate machinery. |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Method of administration and dosage.Dosage This medicinal product must be prepared before administration to the patient. The vial contains a solution for injection with a maximum activity of 11 GBq without oxidizing agent (Tc-99m) in 1–5 mL. For the highest activity of 11 GBq, at least 5 mL of solution is required. Radiochemical purity must be verified before administration to the patient. Adults and elderly patients Dosage may vary depending on gamma camera characteristics and detection methods. Administered activity exceeding local DRLs (diagnostic reference levels) must be justified. Recommended activity range for intravenous administration in an adult patient of average body weight (70 kg) for: Diagnosis of reduced coronary perfusion and myocardial infarction 400–900 MBq. Recommended activity range for diagnosing ischemic heart disease according to European procedural guidelines:
Do not exceed 2000 MBq total activity for the one-day protocol and For myocardial infarction diagnosis, a single injection at rest is usually sufficient. For diagnosis of ischemic heart disease, two injections (stress and rest) are required to differentiate transiently reduced myocardial uptake. Assessment of global ventricular function 600–800 MBq administered as a bolus. Scintimammography 700–1000 MBq administered as a bolus, typically in the arm contralateral to the affected area. Localization of hyperfunctioning parathyroid tissue 200–700 MBq administered as a bolus. Typical activity ranges from 500 to 700 MBq. Dosage may vary depending on gamma camera characteristics and detection methods. Administered activity exceeding local DRLs (diagnostic reference levels) must be justified. Renal impairment The administered activity should be carefully considered, as these patients may experience increased radiation exposure. Hepatic impairment Activity selection for patients with impaired liver function should be cautious, typically starting at the lower end of the dosage range. Children and adolescents Use in children and adolescents must be carefully considered based on clinical need and risk-benefit assessment in this patient group. The activity to be administered to children and adolescents may be calculated according to the pediatric dosage card recommendations of the European Association of Nuclear Medicine (EANM); the activity administered to children and adolescents is calculated by multiplying the base activity (for calculation purposes) by weight-dependent coefficients provided in the table below. A [MBq] = base activity × coefficient The base activity required for tumor detection is 63 MBq. For cardiac imaging, the minimum and maximum activities are 42 and 63 MBq, respectively, for two-day scanning of heart failure both at rest and under stress. For a one-day heart failure protocol, the activity is 28 MBq at rest and 84 MBq under stress. The minimum activity for any examination is 80 MBq.
Route of Administration For intravenous use. Extravasation of this radiopharmaceutical may cause tissue damage; therefore, extravasation must be strictly avoided. Safety precautions to be taken before preparing or administering the medicinal product The medicinal product should be prepared immediately prior to administration to the patient. Image Acquisition Cardiac Imaging Imaging should begin approximately 30–60 minutes after injection to allow for hepatobiliary clearance. Longer delays may be required when imaging after vasodilator stress alone due to the risk of higher subdiaphragmatic technetium (99mTc) activity. There is no evidence of significant redistribution or change in radiopharmaceutical concentration in the myocardium; therefore, imaging may be performed up to 6 hours after administration. The study may be performed using either a one-day or two-day protocol. Tomographic imaging may be performed using SPECT (single-photon emission computed tomography), with or without electrocardiographic (ECG) gating. Scintimammography Imaging of the breast should optimally begin 5–10 minutes after administration, with the patient lying supine and the breast freely pendant. The radiopharmaceutical should be administered into a vein in the arm contralateral to the suspected abnormality. If the condition is bilateral, it is preferable to administer the agent into a dorsal foot vein. Conventional gamma camera The patient should be positioned so that the contralateral breast is pendant for lateral imaging. Anterior images may then be obtained with the patient supine and arms raised above the head. Detector designed for breast tomography When using a detector specifically designed for breast tomography, appropriate manufacturer-specific instructions must be followed to obtain images of adequate quality. Parathyroid Gland Tomography Parathyroid imaging depends on the selected protocol. The most commonly used methods are subtraction (dual-isotope) and/or dual-phase techniques, which may be performed together. For the subtraction method, sodium iodide (123I) or sodium pertechnetate (99mTc) can be used to visualize the thyroid gland, as these radiopharmaceuticals accumulate in thyroid tissue. This image is subtracted from the 99mTc-sestamibi image, leaving pathological parathyroid hyperfunction visible after subtraction. When using sodium iodide (123I), administer orally 10–20 MBq. Imaging of the neck and thorax may be performed 4 hours after administration. After acquiring the sodium iodide (123I) image, administer 200–700 MBq of technetium (99mTc) sestamibi and obtain the second image 10 minutes after injection using dual acquisition with two gamma energy peaks (140 keV for technetium (99mTc) and 159 keV for iodine (123I)). When using sodium pertechnetate (99mTc), administer 40–150 MBq and obtain images of the neck and thorax after 30 minutes. Then administer 200–700 MBq of technetium (99mTc) sestamibi and obtain the second image 10 minutes later. For the dual-phase method, administer 400–700 MBq of technetium (99mTc) sestamibi; obtain the first image of the neck and mediastinum after 10 minutes. After a washout period of 1–2 hours, repeat imaging of the neck and mediastinum. Planar imaging may be supplemented with early and delayed imaging, or whole-body SPECT (single-photon emission computed tomography) or SPECT/CT of specific body regions. INSTRUCTIONS FOR THE PREPARATION OF THE RADIOPHARMACEUTICAL Preparation should be performed under aseptic conditions. Vials should not be opened before disinfection of the stopper. The solution should be withdrawn through the stopper using a single-use syringe equipped with a suitable single-use sterile needle with lead shielding, or by using an authorized automated dispensing system. If the vial integrity is compromised, the product must not be used. Instructions for the Preparation of Technetium (99mTc) Sestamibi A. Boiling Procedure Preparation of technetium (99mTc) sestamibi is carried out according to the following aseptic procedure:
Note. The vial must remain vertical during boiling. Use a water bath where the stopper remains above the water level.
Note: Each time radioactive materials are heated in vials, there is a risk of vial rupture and significant contamination. B. Thermal Cycle Procedure Preparation of technetium (99mTc) sestamibi is carried out according to the following aseptic procedure:
8 Before administration, visually inspect the solution for particulate matter and discoloration. 9 Aseptically withdraw the solution using a sterile shielded syringe. Use within 12 hours after preparation.
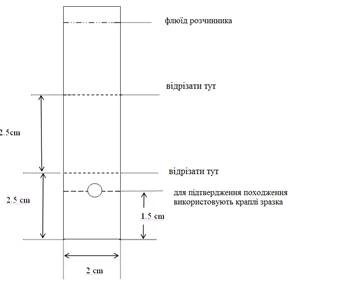
Determination of Radiochemical Purity by Thin-Layer Chromatography 1 Materials
2 Procedure
% Technetium (Tc-99m) sestamibi = Activity in upper portion (Rf = 0.8–1.0) / Total activity of all portions × 100
Note: Do not use the product if radiochemical purity is less than 94%.
Children Use with caution, as the effective dose in MBq is higher than in adults. |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Overdose In the event of radiation overdose with technetium (99mTc) sestamibi, the absorbed dose should be reduced if possible by elimination of radionuclides from the body through defecation and frequent bladder emptying. This may be useful in assessing the administered dose efficacy. |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Adverse ReactionsThe frequency of adverse reactions reported after administration of the medicinal product is presented in the table below.
Immune system disorders Rare: serious hypersensitivity reactions such as dyspnea, hypotension, bradycardia, asthenia, and vomiting (usually within 2 hours after administration), angioneurotic edema. Other hypersensitivity reactions (allergic skin and mucous membrane reactions with exanthema (pruritus, urticaria, swelling), vasodilation). Very rare: other hypersensitivity reactions reported in patients predisposed to such reactions. Nervous system disorders Uncommon: headache. Rare: seizures (occurring some time after administration), convulsions. Cardiac disorders Uncommon: chest pain/angina, abnormal ECG. Rare: arrhythmia. Gastrointestinal disorders Uncommon: nausea. Rare: abdominal pain. Skin and subcutaneous tissue disorders Rare: local reactions at the injection site, hypoesthesia and paresthesia, hyperemia. Unknown: erythema multiforme. General disorders and administration site conditions Common: immediately after administration, a metallic or bitter taste may occur, sometimes accompanied by dryness in the mouth and altered smell. Rare: fever, fatigue, dizziness, transient arthralgia, dyspepsia. Other disorders The effect of ionizing radiation is associated with cancer induction and potential development of hereditary defects. Since the effective dose is 16.4 mSv when the maximum recommended activity of 2000 MBq (500 MBq at rest and 1500 MBq during stress) is used for a one-day protocol, these adverse reactions are expected to occur with lower probability. Reporting of suspected adverse reactions Reporting suspected adverse reactions after marketing authorization of a medicinal product is important. This allows continued monitoring of the benefit-risk balance of the drug. Healthcare professionals are encouraged to report suspected adverse reactions via the national reporting system. |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Shelf life. 1 year. After radiolabeling with sodium pertechnetate (99mTc) solution – 12 hours. Store at a temperature not exceeding 25 °C in an appropriate lead container. |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Storage conditions. Store in a refrigerator at a temperature of (2–8 °C). During transport (for no more than 7 days) at temperatures up to 35 °C. |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Packaging. 10 ml glass vial, pack of 3 or 6 vials in a cardboard box. |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Prescription category. Available only in hospital settings. Supplied only to specialized medical institutions authorized to handle radiopharmaceuticals. |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Manufacturer. National Centre for Nuclear Research / National Centre for Nuclear Research. |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Manufacturer's address and location of operations. Andrzeja Sołtana 7 Street, Otwock, 05–400, Poland / ul. Andrzeja Sołtana 7, Otwock, 05–400, Poland. |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||