Imunat
UkraineTable of Contents
INSTRUCTIONS FOR MEDICAL USE OF THE MEDICINAL PRODUCT IMUNATE (IMMUNATE)
Composition:
Active substances: human blood coagulation factor VIII, von Willebrand factor (vWF:RCo);
1 vial of powder contains:
| Active substance |
Content of substance per vial |
||
| 250/190 IU |
500/375 IU |
1000/750 IU |
|
| Human blood coagulation factor VIII (adjusted for albumin content)* |
250 IU (50 IU/mL) |
500 IU (100 IU/mL) |
1 000 IU (100 IU/mL) |
| Specific activity** |
(70 ± 30) IU/mg protein |
||
| von Willebrand factor (vWF:RCo)*** |
190 IU (38 IU/mL) |
375 IU (75 IU/mL) |
750 IU (75 IU/mL) |
Solvent: water for injections – 5 ml (for 250/190 IU and 500/375 IU) and 10 ml (for 1000/750 IU);
Excipients: human albumin, glycine, lysine hydrochloride, sodium chloride, trisodium citrate dihydrate, calcium chloride dihydrate.
____________________________________________________________________
* Factor VIII activity was determined using the WHO international standard for factor VIII concentrates.
** Without stabilizer (albumin).
Maximum specific activity at a factor VIII to von Willebrand factor antigen ratio of 1:1 is 100 IU per mg of protein.
*** von Willebrand factor activity was determined using the WHO international standard for factor VIII and von Willebrand factor concentrates in plasma.
Pharmaceutical form. Powder and solvent for solution for injection.
Main physicochemical properties: powder or brittle mass, white or pale yellow in color.
Pharmacotherapeutic group. Haemostatics. Coagulation factors. von Willebrand factor in combination with coagulation factor VIII.
ATC code B02BD06.
Immunological and biological properties.
Pharmacodynamics.
The factor VIII/von Willebrand factor complex consists of two molecules (blood coagulation factor VIII and von Willebrand factor) that have different physiological functions.
Activated factor VIII acts as a cofactor for activated factor IX, accelerating the conversion of factor X to activated factor X. Activated factor X then converts prothrombin into thrombin. Thrombin subsequently converts fibrinogen into fibrin, forming a fibrin clot. Hemophilia A is an X-linked inherited coagulation disorder due to reduced levels of factor VIII activity, leading to severe bleeding into joints, muscles, and internal organs, occurring either spontaneously or following trauma or surgery. Plasma factor VIII levels are increased by replacement therapy, which temporarily corrects the factor deficiency and reduces bleeding tendency.
In addition to its role as a protective protein for factor VIII, von Willebrand factor (vWF) mediates platelet adhesion to sites of vascular injury and plays a role in platelet aggregation, making it essential for replacement therapy in patients with von Willebrand disease.
Pharmacokinetics.
Pharmacokinetic parameters obtained from a pharmacokinetic study in patients aged over 12 years are presented in Tables 1 and 2.
Table 1 describes the pharmacokinetic properties based on coagulation factor VIII.
| Parameter |
|||||
| Number of patients |
Mean value |
Standard deviation |
Median |
90% CI |
|
| AUC0–48 h ([MU × h]/ml) |
18 |
11.4 |
2.8 |
11.6 |
10.9–12.7 |
| AUC0–∞ h ([MU × h]/ml) |
18 |
12.2 |
3.1 |
12.4 |
11.1–13.2 |
| Cmax (MU/ml) |
18 |
1.0 |
0.3 |
0.9 |
0.8–1.0 |
| Tmax (h) |
18 |
0.3 |
0.1 |
0.3 |
0.3–0.3 |
| Terminal elimination half-life (h) |
18 |
12.7 |
3.2 |
12.2 |
10.8–15.3 |
| Clearance (ml/h) |
18 |
283 |
146 |
232 |
199–254 |
| Mean residence time (h) |
18 |
15.3 |
3.6 |
15.3 |
12.1–17.2 |
| Vss (ml) |
18 |
4166 |
2021 |
3613 |
2815–4034 |
| Recovery increment of activity level ([MU/ml]/[MU/kg]) |
18 |
0.020 |
0.006 |
0.019 |
0.016–0.020 |
Table 1
Table 2 describes the pharmacokinetic properties by FV antigen.
Table 2
| Parameter |
|||||
| Number of patients |
Median |
90% CI |
|||
| AUC0–∞ ([MO × h]/mL) |
15 |
24.6 |
12.8–48.3 |
||
| Cmax (MO/mL) |
17 |
1.40 |
1.15–1.51 |
||
| Tmax (h) |
17 |
0.28 |
0.25–1.00 |
||
| Terminal elimination half-life (h) |
16 |
13.6 |
10.5–47.2 |
||
| Clearance (mL/h) |
15 |
136 |
68–178 |
||
| Mean residence time (h) |
15 |
23.1 |
12.4–57.1 |
||
| Vss (mL) |
15 |
3156 |
2391–4672 |
||
| Incremental recovery of activity level ([MO/mL] / [MO/kg]) |
17 |
0.028 |
0.024–0.030 |
||
Clinical characteristics.
Indications.
Treatment and prevention of bleeding in patients with hemophilia A (congenital factor VIII deficiency, hemophilia A with factor VIII inhibitor, acquired factor VIII deficiency due to spontaneous development of factor VIII inhibitors).
Von Willebrand's disease with factor VIII deficiency.
Note. The efficacy and safety of Immunate in von Willebrand-Jürgens syndrome has been clinically studied only in a small number of patients. This should be particularly taken into account for type 3 of this disease.
Contraindications.
Hypersensitivity to the active substance or to any of the excipients of the medicinal product.
Interaction with other medicinal products and other forms of interaction.
Studies on interactions with Immunate have not been conducted. There have been no reports of specific interactions between human coagulation factor VIII and other medicinal products.
Special precautions for use
As with all intravenously administered substances, allergic-type hypersensitivity reactions may occur. Patients should be informed about early signs of hypersensitivity reactions, including hypotension, tachycardia, chest pain, dyspnea, swelling (particularly facial swelling and eyelid edema), urticaria, rash, hyperemia, and pruritus, as well as anaphylaxis up to anaphylactic shock.
If symptoms of hypersensitivity occur, patients should be advised to immediately discontinue administration of the drug and contact their physician. In case of shock, standard medical treatment for shock should be initiated.
Other infusion-related reactions have also been reported with Imunat, such as chills, fever, or nausea.
Since the amount of sodium in the maximum daily dose may exceed 200 mg, this should be taken into account by individuals on a low-sodium diet.
250 and 500 IU per vial
Imunat contains approximately 9.8 mg of sodium per vial. This corresponds to 0.5% of the 2 g maximum daily sodium intake recommended by WHO for adults.
1000 IU per vial
Imunat contains approximately 19.6 mg of sodium per vial. This corresponds to 1% of the 2 g maximum daily sodium intake recommended by WHO for adults.
Development of neutralizing antibodies (inhibitors) against factor VIII is a known complication during treatment of patients with hemophilia A. These inhibitors are usually IgG immunoglobulins directed against the coagulant activity of factor VIII and are quantitatively measured in Bethesda units (BU) per 1 mL of plasma using a modified assay. The risk of inhibitor development correlates with disease severity and exposure to factor VIII. This risk is highest during the first 50 days of treatment but persists throughout life, although it is rare.
Patients receiving treatment with factor VIII coagulation factor products should be closely monitored for the development of inhibitors through appropriate clinical observations and laboratory testing (see also section "Adverse reactions").
The risk of inhibitor development depends on various factors related to individual patient characteristics. Key risk factors include, in particular, the type of factor VIII gene mutation, family history, and patient’s ethnicity.
Inhibitors have been predominantly reported in previously untreated patients.
Imunat is manufactured from human plasma. Standard measures to prevent infection transmission associated with medicinal products derived from human blood or plasma include donor selection, screening of individual plasma units and plasma pools for specific infection markers, and effective manufacturing steps for virus inactivation/removal. Despite these measures, the possibility of transmitting infectious agents with products derived from human blood or plasma cannot be completely excluded. This also applies to unknown or newly emerging viruses and other pathogens.
The measures taken are considered effective against enveloped viruses such as human immunodeficiency virus (HIV), hepatitis B virus, hepatitis C virus, and also against the non-enveloped hepatitis A virus. However, the measures may have limited effectiveness against non-enveloped viruses such as parvovirus B19. Infection caused by parvovirus B19 may be dangerous for pregnant women (fetal infection) and for individuals with immunodeficiency or increased erythropoiesis (e.g., hemolytic anemia).
During long-term treatment of von Willebrand disease with a factor VIII-containing product, factor VIII:C levels may become excessively elevated. There is a risk of thrombotic events during treatment of patients with von Willebrand syndrome, especially in patients with known clinical or laboratory risk factors. Therefore, patients should be monitored for early signs of thrombosis. In patients with a history of venous thromboembolism, a high endogenous factor VIII level has been associated with an increased risk of further thrombotic events.
In patients receiving a product containing von Willebrand factor and factor VIII, plasma levels of factor VIII:C should be monitored to avoid sustained excessive levels of factor VIII:C in plasma, which may increase the risk of thrombotic events.
Prophylaxis of venous thromboembolism should be performed according to current guidelines.
In patients with von Willebrand disease, especially those with type 3, neutralizing antibodies (inhibitors) against von Willebrand factor may develop.
Such antibodies may occur in close association with anaphylactic reactions. Therefore, patients experiencing anaphylactic reactions should be tested for the presence of such an inhibitor. If expected vWF:RCo activity levels in plasma are not achieved or if bleeding is not controlled with an appropriate dose, testing for the presence of a von Willebrand factor inhibitor should be performed. In patients with high inhibitor levels, von Willebrand factor therapy may be ineffective, and alternative treatment options should be considered. Treatment should be administered under the supervision of a physician experienced in managing coagulation disorders.
Patients who are regularly or repeatedly treated with factor VIII derived from human plasma should be considered for appropriate vaccination (hepatitis A and B).
It is recommended that, each time Imunat is used, the patient’s diary should record the name and batch number of the product to establish a link between the patient and the product batch.
Imunat contains blood group isohemagglutinins (anti-A and anti-B). Hemolysis may occur in patients with blood group A, B, or AB after repeated administration at short intervals or after administration of very high doses. Very high doses over a short period may be used within immune tolerance induction therapy for hemophilia with factor VIII inhibitors.
Before prescribing Imunat, it must be confirmed that the coagulation disorder is indeed due to factor VIII deficiency (hemophilia A) or von Willebrand factor deficiency (von Willebrand disease).
Use during pregnancy and breastfeeding
Studies on the effects of factor VIII on reproductive functions in animals have not been conducted. Due to the rarity of hemophilia A in women, experience with the use of factor VIII during pregnancy and breastfeeding is lacking. Therefore, factor VIII should be used during pregnancy and breastfeeding only if clearly indicated.
Information on parvovirus B19 infection can be found in the section "Special precautions for use."
Ability to affect reaction speed when driving or operating machinery
There is no information available on the effect of Imunat on the ability to drive or operate machinery.
Administration and Dosage
Treatment should be carried out under the supervision of a physician experienced in the treatment of hemophilia A.
Standard Dosing
The dosage and duration of replacement therapy depend on the severity of factor VIII deficiency, the location and extent of bleeding, as well as the patient's clinical condition.
The administered amount of factor VIII is expressed in international units (IU), defined by the current WHO standard for factor VIII-containing medicinal products. Factor VIII activity in blood plasma is expressed either as a percentage (relative to the normal human plasma value) or in international units (relative to the international standard for factor VIII in plasma).
One international unit (IU) of factor VIII activity is equivalent to the amount of factor VIII present in 1 ml of normal human plasma.
Dosing in Hemophilia A
The required dose of factor VIII is calculated based on the empirically established relationship: 1 international unit (IU) of factor VIII per 1 kg of body weight increases factor VIII activity in plasma by approximately 1.5–2% of normal activity. The required dose can be determined using the following formula:
Required number of units (IU) = body weight (kg) × desired increase
in factor VIII (%) × 0.5
The dose and frequency of administration should always be adjusted to ensure clinical efficacy in each individual patient.
Bleeding Episodes and Surgery
In the event of ongoing bleeding episodes, factor VIII activity should not fall below the target plasma level (in % of normal or IU/dL) during the appropriate period. The table below (Table 3) can be used to determine dosing during bleeding episodes and surgical procedures.
Table 3
| Degree of bleeding/surgical procedure type |
Required factor VIII level (% of normal) (IU/dL) |
Dosing frequency (hours)/duration of treatment (days) |
| Bleeding |
||
| Early haemarthrosis, muscle haemorrhage, or oral cavity bleeding |
20–40 |
Repeat every 12–24 hours for at least 1 day until bleeding stops, as indicated by absence of pain and wound healing. |
| More pronounced haemarthrosis, muscle haemorrhage, or hematoma |
30–60 |
Repeat infusion every 12–24 hours for 3–4 days or longer until pain resolves and significant functional impairment is eliminated. |
| Life-threatening bleeding |
60–100 |
Repeat infusion every 8–24 hours until the threat is resolved. |
| Surgical procedure |
||
| Minor surgical procedure, including tooth extraction |
30–60 |
Every 24 hours for at least 1 day until wound healing. |
| Major surgical procedure |
80–100 (before and after surgery) |
Repeat infusion every 8–24 hours until adequate wound healing; thereafter continue treatment for at least 7 additional days to maintain factor VIII activity levels at 30–60% (IU/dL). |
The dose and frequency of administration should be adjusted according to the clinical response in each individual case. Under certain circumstances (e.g., presence of low titer inhibitors to factor VIII), doses higher than those calculated by the formula may be required, especially at the beginning of treatment.
If bleeding cannot be controlled with the calculated dose, plasma factor VIII levels should be determined and an adequate dose of Immunate administered to achieve a satisfactory clinical response.
During treatment, monitoring of factor VIII activity is recommended to determine the need for dose adjustment and frequency of repeated infusions. In the case of major surgical interventions, precise monitoring during replacement therapy by quantitative assay of factor VIII activity in plasma is essential. Response to factor VIII may vary among individual patients, with different half-life values and degrees of in vivo recovery.
Long-term prophylaxis
For long-term prevention of bleeding in patients with severe hemophilia A, usual doses are 20–40 IU of factor VIII per kg body weight, administered every 2–3 days. In some cases, particularly in young patients, shorter intervals between administrations or higher doses may be required.
Patients with factor VIII inhibitors
Patients should be regularly monitored for the development of factor VIII inhibitors. If expected plasma factor VIII activity levels are not achieved or if bleeding is not controlled with an appropriate dose, testing for the presence of factor VIII inhibitors should be performed. In patients with high inhibitor titers, factor VIII therapy may be ineffective, and alternative treatment options should be considered. Management of such patients should be conducted under the supervision of physicians experienced in treating hemophilia, particularly in cases of factor VIII inhibitor development (see also section "Special precautions").
Cardiovascular events
Replacement therapy with factor VIII may increase cardiovascular risk in patients with pre-existing cardiovascular risk factors.
Von Willebrand disease with factor VIII deficiency
Immunate is indicated for the treatment and prevention of factor VIII deficiency in patients with von Willebrand disease with factor VIII deficiency, and in cases where treatment with desmopressin alone is ineffective or contraindicated. Replacement therapy with Immunate for control of bleeding and for perioperative bleeding prophylaxis should be performed according to the same recommendations as for hemophilia A.
Experience with use in children is limited.
Patients should be monitored for the development of von Willebrand factor inhibitors if expected plasma von Willebrand factor activity levels are not achieved or if bleeding is not controlled with an appropriate dose. In patients with high inhibitor titers, von Willebrand factor therapy may be ineffective, and alternative therapeutic options should be considered (see also section "Special precautions").
When using a medicinal product containing both von Willebrand factor and factor VIII, the treating physician should be aware that continuous treatment may lead to excessive elevation of factor VIII:C levels. Consideration should be given to reducing the dose and/or extending the intervals between administrations after 24 to 48 hours of treatment to avoid excessively high factor VIII:C levels.
Children
Immunate should be used with caution in children under 6 years of age who have had limited exposure to factor VIII products, as clinical data in this patient group are limited. However, based on case reports, efficacy and safety can be inferred.
Route of administration
Instructions for reconstitution of the medicinal product prior to administration are provided in the section "Dosage and administration".
Immunate should be administered slowly intravenously. The maximum infusion rate should not exceed 2 mL per minute.
Preparation of solution
Immunate should be reconstituted immediately before use. The solution should be used immediately, as the product contains no preservatives.
Before administration, reconstituted medicinal products should be visually inspected for the presence of particulate matter and discoloration. Reconstituted solutions that are cloudy or contain precipitates should not be used.
It is recommended to flush implanted venous access devices with isotonic saline solution before and after infusion of Immunate.
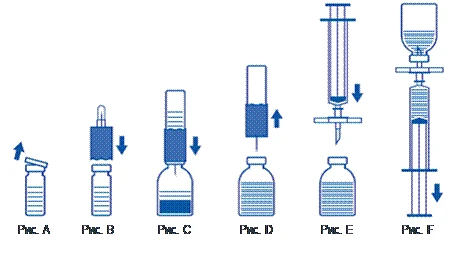
Reconstitution of powder: use aseptic technique as described below
- Warm the unopened vial of diluent (sterile water for injection) to room temperature (not exceeding 37°C).
- Remove protective caps from the powder vial and the diluent vial (Fig. A) and disinfect the rubber stoppers of both vials.
- Place the flanged end of the transfer device onto the diluent vial and press down (Fig. B).
- Remove the protective cover from the other end of the transfer set, taking care not to touch the open end.
- Invert the transfer set with the attached diluent vial over the powder vial and insert the free end of the needle into the rubber stopper of the powder vial (Fig. C). The diluent will be drawn into the powder vial by vacuum.
- Approximately one minute later, disconnect the two vials by removing the transfer set with the attached diluent vial from the powder vial (Fig. D). Since the product dissolves readily, gently swirl the concentrate vial slightly, if necessary. DO NOT SHAKE THE POWDER VIAL. DO NOT INVERT THE POWDER VIAL UNTIL READY TO REMOVE CONTENTS.
- After reconstitution, the prepared solution should be visually inspected for particulate matter and discoloration prior to administration. However, even with careful adherence to the reconstitution procedure, a few fine particles may occasionally be visible. These particles will be removed by the filter provided in the kit, without reducing the efficacy of the product.
Use aseptic technique as described below
- To prevent administration of rubber particles from the stopper (risk of microembolism), use the filter set provided in the kit. Attach the filter set to the supplied single-use syringe and insert it through the rubber stopper (Fig. E).
- Disconnect the syringe momentarily from the filter set. Air will enter the powder vial, and any foam will dissipate. Then draw the solution into the syringe through the filter set (Fig. F).
- Disconnect the syringe from the filter set and administer the solution slowly intravenously (maximum infusion rate: 2 mL per minute) using the provided winged infusion set (or the provided single-use needle).
Any unused medicinal product or waste material should be disposed of in accordance with local requirements.
Children
Immunate should be used with caution in children under 6 years of age who have had limited exposure to factor VIII products, as clinical data in this patient group are limited. However, based on case reports, efficacy and safety can be inferred.
Overdose
No symptoms associated with overdose of human coagulation factor VIII have been reported.
Thromboembolic events are the primary risk. Patients with blood group A, B, or AB are at risk of hemolysis (see also section "Special precautions").
Adverse Reactions
The adverse reactions listed below were identified during clinical trials and reported in the post-marketing period after marketing authorization of the medicinal product Imunat. Frequency is categorized according to the following scale: very common (≥ 10%); common (≥ 1% to < 10%); uncommon (≥ 0.1% to < 1%); rare (≥ 0.01% to < 0.1%); very rare (< 0.01%).
Clinical Trials
The frequency of all adverse reactions listed below, as reported in clinical trials, was uncommon (≥ 0.1% to < 1%).
Immune system disorders
Uncommon: allergic reactions.
Spontaneous reports after marketing authorization
The frequency of all adverse reactions listed below was very rare (< 0.01%).
Blood and lymphatic system disorders
Coagulopathy, inhibition of factor VIII.
Psychiatric disorders
Anxiety.
Cardiac disorders
Palpitations, tachycardia.
Gastrointestinal disorders
Vomiting, nausea.
General disorders and administration site conditions
Chest pain, chest discomfort, swelling (including peripheral edema and facial edema), injection site irritation (including burning sensation), chills, pain, pyrexia.
Immune system disorders
Hypersensitivity.
Nervous system disorders
Headache, dizziness, paresthesia.
Respiratory, thoracic and mediastinal disorders
Cough, dyspnea.
Vascular disorders
Arterial hypotension, hyperemia, pallor.
Eye disorders
Conjunctivitis, eyelid edema.
Skin and subcutaneous tissue disorders
Erythema, exanthema, neurodermatitis, pruritus, rash, erythematous rash, generalized rash, urticaria, hyperhidrosis.
Musculoskeletal and connective tissue disorders
Myalgia.
Adverse reactions listed below have not yet been reported, but may occur during the use of Imunat.
Blood and lymphatic system disorders
Hemolysis in patients with blood group A, B, or AB.
General disorders and administration site conditions
Reduced therapeutic response.
Description of selected adverse reactions
Hypersensitivity reactions or allergic reactions (which may include angioedema, burning and tingling sensation at the infusion site, chills, erythema, generalized urticaria, headache, rash, arterial hypotension, lethargy, nausea, anxiety, tachycardia, chest tightness, tingling, vomiting, wheezing) have been observed rarely and in some cases may progress to severe anaphylaxis (including shock). Patients should be advised to seek immediate medical attention if these symptoms occur.
Pyrexia has been observed in rare cases.
In patients with hemophilia A, neutralizing antibodies (inhibitors) to factor VIII may develop. If such inhibitors develop, the condition manifests as inadequate clinical response. In such cases, consultation with a specialized hemophilia treatment center is recommended.
Hemolysis may occur after administration of high doses (e.g., when factor VIII plasma levels above 100% are required) in patients with blood group A, B, or AB.
For information on viral safety, see section "Special precautions for use".
Reporting of suspected adverse reactions
Reporting suspected adverse reactions after marketing authorization is important. It allows continued monitoring of the benefit-risk balance of the medicinal product. Healthcare professionals and patients, as well as their legal representatives, are encouraged to report all suspected adverse reactions and lack of efficacy via the automated pharmacovigilance information system at: https://aisf.dec.gov.ua.
Shelf life
Medicinal product: 2 years.
Solvent (water for injections): 5 years.
Storage conditions
Store at 2 to 8 °C. Do not freeze. Store in the original packaging to protect from light. Keep out of reach of children. Within the stated shelf life, the medicinal product may be stored at room temperature (not above 25 °C) for up to 6 months.
After reconstitution, the medicinal product may be stored at room temperature (not above 25 °C) for up to 6 hours.
Incompatibilities
Imunat must not be mixed with other medicinal products, as this may adversely affect safety and efficacy. Only the provided infusion sets should be used, as adsorption of human coagulation factor VIII to the internal surface of certain infusion devices may result in reduced treatment efficacy.
Packaging
One vial of powder (250/190 IU, 500/375 IU, or 1000/750 IU) with one vial of solvent (water for injections, 5 ml or 10 ml), and one reconstitution and administration set (one transfer device/filter, one single-use syringe (5 ml or 10 ml), one single-use needle, one infusion set) in a carton.
Prescription status
Prescription only.
Manufacturer
Takeda Manufacturing Austria AG, Austria.
Manufacturer's address and location of operation
Industriestrasse 67, 1221 Vienna, Austria.