Gonal-f®
Ukraine
Table of Contents
INSTRUCTIONS FOR MEDICAL USE OF THE MEDICINAL PRODUCT GONAL-fâ (GONAL-fâ)
Composition:
Active substance: follitropin alfa (recombinant human follicle-stimulating hormone – r-hFSH);
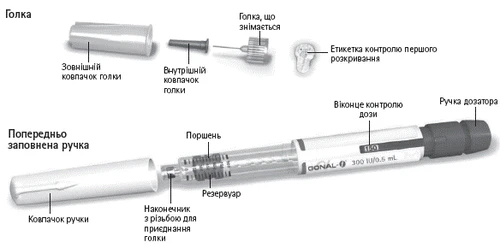
One pen is intended for administration:
300 IU of follitropin alfa, equivalent to 22 mcg, in 0.48 mL of solution; or
450 IU of follitropin alfa, equivalent to 33 mcg, in 0.72 mL of solution; or
900 IU of follitropin alfa, equivalent to 66 mcg, in 1.44 mL of solution;
Excipients: poloxamer 188, sucrose, methionine, disodium hydrogen phosphate dihydrate, sodium dihydrogen phosphate monohydrate, m-cresol, phosphoric acid concentrated, sodium hydroxide, water for injections.
Medicinal form. Solution for injection.
Main physicochemical characteristics: solution, practically free from visible particles.
Pharmacotherapeutic group. Sex hormones and modulators of the reproductive system. Gonadotrophins.
ATC code G03G A05.
Pharmacological Properties.
Pharmacodynamics.
GONAL-f® is a follicle-stimulating hormone (FSH) preparation obtained by recombinant DNA technology using Chinese hamster ovary cells.
Follicle-stimulating hormone (FSH) and luteinizing hormone (LH) are secreted by the anterior pituitary in response to gonadotropin-releasing hormone (GnRH) and play complementary roles in follicular development and ovulation. FSH stimulates the development of ovarian follicles, while LH is involved in follicular development, steroidogenesis, and final maturation.
After administration of recombinant FSH (r-hFSH), serum levels of inhibin and estradiol (E2) increase, leading to induction of follicular development. Serum inhibin levels rise rapidly and can be detected as early as day 3 after initiation of r-hFSH treatment, whereas E2 levels require more time and begin to rise only from day 4 of treatment. Total follicular volume starts to increase after 4–5 days of daily r-hFSH administration, and depending on the patient's response, maximal effect is achieved approximately 10 days after the start of r-hFSH treatment.
In clinical studies, patients with severe FSH and LH deficiency were defined by a serum level of endogenous LH < 1.2 IU/L; however, it should be noted that LH assay results may vary between different laboratories.
In comparative clinical trials conducted within assisted reproductive technology (ART) programs and ovulation induction, GONAL-f® demonstrated superior efficacy compared to urinary FSH, as evidenced by a lower total dose and shorter treatment duration required to achieve follicular maturation. In ART cycles, the use of a lower total dose of GONAL-f® over a shorter treatment period resulted in a higher number of retrieved oocytes and embryos undergoing cleavage on day 2 after fertilization compared to urinary FSH. In ovulation induction, treatment with GONAL-f® was associated with a lower rate of cycle cancellation due to therapeutic inefficacy compared to urinary FSH.
Results from Study GF 8407: a randomized, parallel-group design study comparing the efficacy and safety of GONAL-f® and urinary FSH in assisted reproductive technology (ART)
| Parameter |
GONAL-f® (n = 130) |
Urinary FSH (n = 116) |
| Number of oocytes retrieved |
11.0 ± 5.9 |
8.8 ± 4.8 |
| Stimulation duration, days |
11.7 ± 1.9 |
14.5 ± 3.3 |
| Total required FSH dose (number of 75 IU FSH vials) |
27.6 ± 10.2 |
40.7 ± 13.6 |
| Dose increase required (%) |
56.2 |
85.3 |
The difference between the two groups was statistically significant (p < 0.05) for all the criteria listed above.
Concomitant administration of GONAL-fâ and human chorionic gonadotropin (hCG) for at least 4 months leads to induction of spermatogenesis in men with FSH deficiency.
Pharmacokinetics.
When follitropin alfa and lutropin alfa are administered simultaneously, no pharmacokinetic interaction occurs.
Distribution
After intravenous administration, follitropin alfa distributes into the interstitial fluid with an initial half-life of approximately 2 hours and is eliminated with a terminal half-life of 14 to 17 hours. The volume of distribution at steady state ranges from 9 to 11 L.
After subcutaneous administration, the absolute bioavailability is 66%, and the apparent terminal half-life ranges from 24 to 59 hours. After subcutaneous administration, dose-proportional pharmacokinetics have been demonstrated for doses up to 900 IU. Repeated administration of follitropin alfa results in a threefold increase in accumulation, reaching steady-state within 3–4 days.
Elimination
Total clearance is 0.6 L/h, and approximately 12% of the dose of follitropin alfa is excreted in urine.
Clinical characteristics.
Indications.
Treatment of adult women
- Anovulation (including polycystic ovary syndrome) in women who have failed to respond to clomiphene citrate treatment.
- Stimulation of multiple follicular development in patients undergoing superovulation as part of assisted reproductive technologies (ART), such as in vitro fertilization (IVF), gamete intrafallopian transfer (GIFT), and zygote intrafallopian transfer (ZIFT).
- Stimulation of follicular development in women with severe deficiency of luteinizing hormone (LH) and follicle-stimulating hormone (FSH) (in combination with an LH-containing preparation).
Treatment of adult men
- Stimulation of spermatogenesis in men with congenital or acquired hypogonadotropic hypogonadism, in combination with human chorionic gonadotropin (hCG) therapy.
Contraindications.
- Hypersensitivity to the active substance or to any of the excipients of the medicinal product;
- hypothalamic or pituitary tumors;
- ovarian enlargement or cysts unrelated to polycystic ovary syndrome or of unknown origin;
- gynecological bleeding of unknown origin;
- carcinoma of the ovaries, uterus, or breasts.
GONAL-fâ must not be used in cases where an effective response to treatment cannot be expected, such as:
- primary ovarian failure;
- congenital abnormalities of the genital organs incompatible with pregnancy;
- uterine fibroids incompatible with pregnancy;
- primary testicular failure.
Interaction with other medicinal products and other forms of interaction.
Concomitant use of GONAL-fâ with other medicinal products used for ovulation induction (such as hCG, clomiphene citrate) may enhance follicular response, whereas concomitant use with gonadotropin-releasing hormone (GnRH) agonists or antagonists inducing pituitary desensitization may lead to increased dosage requirements of GONAL-fâ necessary to achieve adequate ovarian response. No other clinically significant drug interactions during GONAL-fâ therapy have been reported.
Special precautions for use.
Traceability
To improve traceability of biological medicinal products, the name and batch number of the administered product should be clearly recorded.
General recommendations
Since GONAL-fâ exhibits significant gonadotropic activity capable of causing adverse reactions ranging from mild to severe, the drug should be prescribed only by physicians experienced in infertility management and its treatment methods.
Gonadotropin therapy requires a time commitment from physicians and other healthcare professionals, as well as appropriate equipment for monitoring treatment. Safe and effective use of GONAL-fâ in women requires regular monitoring of ovarian response by ultrasound, preferably combined with serum estradiol level measurements. Patient response to FSH administration is highly individual, with some patients showing very low responsiveness and others exhibiting excessive response. For treatment of both women and men, the lowest effective dose of the drug should be used according to the treatment objective.
Patients with porphyria
Patients with porphyria or a family history of porphyria should be under close medical supervision during treatment with GONAL-fâ. If early signs of porphyria appear or if the condition worsens, treatment may need to be discontinued.
Treatment of women
Before initiating treatment, infertile couples should undergo evaluation to identify existing or potential contraindications to pregnancy. Specifically, patients should be evaluated for hypothyroidism, adrenal insufficiency, hyperprolactinemia, and appropriate specific treatment should be initiated.
During follicular stimulation as part of treatment for anovulatory infertility or assisted reproductive technology (ART) procedures, ovarian enlargement or hyperstimulation may occur in patients. Adherence to recommended dosing and administration regimens of GONAL-fâ, along with careful monitoring of therapy, will reduce the frequency of such events. Accurate interpretation of follicular development and maturation indicators requires an experienced specialist.
Clinical studies have shown increased ovarian sensitivity to GONAL-fâ when administered concomitantly with lutropin alfa. If an increase in FSH dose is considered necessary, it is best to adjust the dose every 7–14 days by increments of 37.5–75 IU. Direct comparison between GONAL-fâ/LH and human menopausal gonadotropin (hMG) has not been conducted. Comparison with published data suggests that ovulation rates achieved with GONAL-fâ/LH are similar to those obtained with hMG.
Ovarian hyperstimulation syndrome (OHSS)
An expected outcome of controlled ovarian stimulation is some degree of ovarian enlargement. This phenomenon, most commonly observed in women with polycystic ovary syndrome (PCOS), usually resolves spontaneously without specific treatment.
In contrast to uncomplicated ovarian enlargement, OHSS is a syndrome that progresses in severity. It includes marked ovarian enlargement, high serum sex steroid levels, and increased vascular permeability, which may lead to fluid accumulation in the abdominal, pleural, and rarely, pericardial cavities.
In severe cases, OHSS may present with symptoms such as abdominal pain and bloating, significant ovarian enlargement, weight gain, dyspnea, oliguria, and gastrointestinal symptoms including nausea, vomiting, and diarrhea. Clinical examination may reveal hypovolemia, hemoconcentration, electrolyte imbalance, ascites, hemoperitoneum, pleural effusions, hydrothorax, or acute respiratory distress syndrome. In very rare cases, severe OHSS may be complicated by ovarian torsion and thromboembolic events such as pulmonary artery embolism, ischemic stroke, and myocardial infarction.
Independent risk factors for OHSS include young age, low body weight, polycystic ovary syndrome, high doses of exogenous gonadotropins, high or rapidly rising serum estradiol levels, previous episodes of OHSS, a large number of developing ovarian follicles, or a high number of oocytes retrieved in ART cycles.
Adherence to recommended dosing and administration regimens of GONAL-fâ may minimize the risk of ovarian hyperstimulation. Monitoring of stimulation cycles using ultrasound and estradiol level measurements is recommended for early identification of risk factors.
There is evidence suggesting that hCG plays a key role in initiating OHSS and that the syndrome may become more severe and prolonged if pregnancy occurs. Therefore, in the presence of signs of ovarian hyperstimulation, administration of hCG should be withheld, and patients should be advised to abstain from sexual intercourse or use barrier contraception for at least 4 days. OHSS can rapidly progress (within 24 hours) and become a serious medical complication within a few days. It most commonly occurs after discontinuation of hormonal treatment and peaks approximately 7–10 days after treatment ends. Therefore, patients should remain under medical supervision for at least 2 weeks after hCG administration.
In ART procedures, the incidence of hyperstimulation may be reduced by aspirating all follicles prior to ovulation.
Mild or moderate forms of OHSS usually resolve spontaneously. If severe OHSS occurs, gonadotropin treatment must be discontinued if still ongoing, the patient should be hospitalized, and appropriate OHSS therapy initiated.
Multiples pregnancy
In patients undergoing ovulation induction, the rate of multiple pregnancies is increased compared to natural conception. Most multiple pregnancies are twin pregnancies. Multiple pregnancy, especially higher-order, carries an increased risk of adverse obstetric and perinatal outcomes.
To minimize the risk of multiple pregnancy, careful monitoring of ovarian response is recommended.
In ART procedures, the risk of multiple pregnancy is primarily related to the number of embryos transferred, embryo quality, and patient age.
Patients should be informed of the potential risk of multiple births before starting treatment.
Pregnancy loss
In women undergoing follicular stimulation for ovulation induction or ART, the rate of pregnancy loss due to miscarriage or spontaneous abortion is higher than after natural conception.
Ectopic pregnancy
Women with a history of tubal disease have an increased risk of ectopic pregnancy, regardless of whether conception occurs spontaneously or following infertility treatment. The reported incidence of ectopic pregnancy after ART is higher than in the general population.
Reproductive system neoplasia
Cases of both benign and malignant tumors of the ovaries and other reproductive organs have been reported in women who received multiple fertility medications. It has not yet been established whether gonadotropin treatment increases the baseline risk of such tumors in infertile women.
Congenital malformations
The incidence of congenital malformations after ART may be slightly higher than after spontaneous conception. This is believed to be due to differences in parental characteristics (e.g., maternal age, sperm quality) and multiple pregnancies.
Thromboembolic events
In women with recent or existing thromboembolic disorders or those with established risk factors for thromboembolic events (e.g., personal or family history), gonadotropin treatment may further increase the risk of exacerbation or occurrence of such events. In such patients, the benefit of gonadotropin use should be carefully weighed against the existing risk of complications. However, it should be noted that pregnancy itself and OHSS both increase the risk of thromboembolic complications.
Treatment of men
Elevated endogenous FSH levels in patients indicate primary testicular failure. Such patients are unresponsive to treatment with GONAL-fâ/hCG. GONAL-fâ should not be used when an effective treatment response cannot be achieved.
Semen analysis is recommended 4–6 months after initiation of treatment to assess response.
Sodium content
GONAL-fâ contains less than 1 mmol of sodium (23 mg) per dose, i.e., it is essentially "sodium-free."
Use during pregnancy or breastfeeding.
Pregnancy
There are no indications for the use of GONAL-fâ during pregnancy. Data from a limited number of cases of drug use during pregnancy (fewer than 300 cases) suggest no congenital malformations or fetal or neonatal toxicity from follitropin alfa, although clinical data are insufficient to exclude a teratogenic effect of GONAL-fâ.
Breastfeeding
GONAL-fâ is not indicated for use during breastfeeding.
Fertility
GONAL-fâ is indicated for the treatment of infertility (see section "Indications").
Ability to affect reaction speed when driving vehicles or operating machinery.
GONAL-fâ has no or negligible effect on the ability of patients to drive vehicles or operate machinery.
Method of Administration and Dosage
Treatment with GONAL-fâ should be initiated under the supervision of a physician experienced in the management of infertility.
Daily doses, administration schedule, and monitoring procedures for treatment with GONAL-fâ should be individually tailored for each patient to optimize follicular development and minimize the risk of ovarian hyperstimulation. It is recommended to follow the proposed initial doses outlined below.
Bioequivalence has been demonstrated for equivalent doses of the single-dose and multi-dose formulations of GONAL-fÒ.
Women with anovulation, including polycystic ovary syndrome
GONAL-fâ is administered as a course of daily injections. In patients with regular menstruation, treatment should begin within the first 7 days of the menstrual cycle.
In registration studies, the usual treatment regimen started with daily administration of 75–150 IU of FSH. If necessary, the dose may be increased by 37.5 IU (preferably) or 75 IU at intervals of 7 days or (preferably) 14 days to achieve an adequate but not excessive response.
In clinical practice, the initial dose is usually individually selected based on clinical parameters of the patient, such as ovarian reserve markers, age, body mass index, and, if applicable, previous ovarian response to stimulation.
Initial dose
The initial dose may be selected stepwise as follows: (a) less than 75 IU per day if an excessive ovarian response is expected based on the patient’s clinical profile (age, body mass index, ovarian reserve), or (b) more than 75 IU up to a maximum of 150 IU per day if a poor ovarian response is expected.
The patient’s response to treatment should be carefully monitored by ultrasound assessment of follicle size and number and/or by serum estradiol levels.
Dose adjustment
If the patient does not respond adequately to treatment within 4 weeks (with either poor or excessive ovarian response), the continuation of the current treatment cycle should be re-evaluated and managed according to standard treatment protocols. In case of poor response, the daily dose should not exceed 225 IU of FSH.
If excessive ovarian response is observed by the physician, treatment should be discontinued and administration of hCG should be cancelled (see section "Special precautions"). In the subsequent cycle, treatment should be initiated with a dose lower than that used in the previous cycle.
Final follicular maturation
Upon achieving optimal ovarian response, 250 mcg of recombinant human chorionic gonadotropin alpha (r-hCG) or 5000–10000 IU of hCG should be administered as a single dose 24–48 hours after the last injection of GONAL-fâ. Patients are advised to have sexual intercourse on the day of hCG administration and the following day. Alternatively, intrauterine insemination may be performed.
Stimulation of multiple follicular development in women undergoing superovulation as part of ART or in vitro fertilization
In registration studies for superovulation, the usual regimen consisted of daily administration of 150–225 IU of GONAL-fâ, starting on day 2 or 3 of the cycle.
In clinical practice, the initial dose is usually individually selected based on clinical parameters of the patient, such as markers of ovarian reserve, age, body mass index, and, if applicable, previous ovarian response to stimulation.
Initial dose
If a poor ovarian response is expected, the initial dose may be stepwise adjusted, but should not exceed 450 IU. Conversely, if an excessive ovarian response is expected, the initial dose may be reduced to below 150 IU.
The patient’s response to treatment should be carefully monitored by ultrasound assessment of follicle size and number and/or by serum estradiol levels until adequate follicular development is achieved.
GONAL-fâ may be administered alone or in combination with a gonadotropin-releasing hormone (GnRH) agonist or antagonist to prevent premature luteinization.
Dose adjustment
If the patient does not respond adequately to treatment (with either poor or excessive ovarian response), the continuation of the current treatment cycle should be re-evaluated and managed according to standard treatment protocols. In case of poor response, the daily dose should not exceed 450 IU of FSH.
Final follicular maturation
Upon achieving optimal ovarian response, 250 mcg of r-hCG or 5000–10000 IU of hCG should be administered as a single dose 24–48 hours after the last injection of GONAL-fâ to induce final follicular maturation.
Women with severe deficiency of LH and FSH secretion
In women with severe deficiency of LH and FSH secretion, combined therapy with GONAL-fâ and a luteinizing hormone (LH) preparation aims to promote follicular development followed by final maturation after administration of human chorionic gonadotropin (hCG). GONAL-fâ is administered as a course of daily injections concomitantly with lutropin alfa. If the patient has amenorrhea and low endogenous estrogen secretion, treatment may be initiated at any time.
The recommended treatment regimen starts with daily administration of 75 IU of lutropin alfa together with 75–150 IU of FSH. Treatment should be adjusted according to the individual patient’s response, assessed by ultrasound evaluation of follicle size and serum estradiol levels.
If an increase in FSH dose is considered necessary, it should preferably be adjusted at 7–14 day intervals by increments of 37.5–75 IU. The duration of stimulation may be extended up to 5 weeks within any single treatment cycle.
Upon achieving optimal response, 250 mcg of r-hCG or 5000–10000 IU of hCG should be administered as a single dose 24–48 hours after the last injection of GONAL-fâ and lutropin alfa. Patients are advised to have sexual intercourse on the day of hCG administration and the following day. Alternatively, intrauterine insemination or another assisted reproductive technology procedure may be performed, as individually determined by the physician.
During treatment, luteal phase support should be considered, as deficiency of luteotropic activity (LH/hCG) after ovulation may lead to premature luteal phase deficiency.
If excessive response occurs, treatment should be discontinued and hCG administration should be cancelled. In the subsequent cycle, treatment should be initiated with a lower FSH dose than that used in the previous cycle (see section "Special precautions").
Men with hypogonadotropic hypogonadism
GONAL-fâ is administered at a dose of 150 IU three times per week, concomitantly with hCG, for at least 4 months. If no response is observed after this period, combined treatment may be continued. Current clinical experience indicates that, if necessary, treatment may be continued for at least 18 months to achieve spermatogenesis.
Special patient populations
Elderly patients
There are no relevant indications for the use of GONAL-fâ in elderly patients. Safety and efficacy of the drug in this population have not been established.
Patients with renal or hepatic impairment
Safety, efficacy, and pharmacokinetic parameters of GONAL-fâ in patients with renal or hepatic impairment have not been established.
If self-administering GONAL-fâ, please read and follow the instructions below.
General recommendations
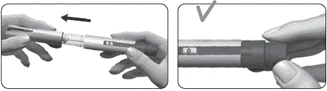
The drug is intended for subcutaneous administration. The solution should not be used if it is cloudy or contains particles.
Self-administration may be performed only by properly trained patients who have access to medical consultation if needed.
Daily injections should be administered at approximately the same time each day, rotating injection sites. Ensure that patients always have an adequate supply of pens as prescribed in the treatment regimen.
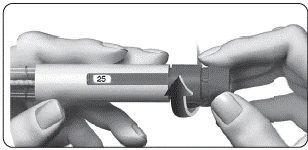
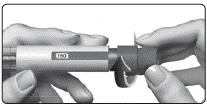
Prepare the pre-filled pen with GONAL-fÒ for injection and administer the prescribed dose as described below. The number displayed in the dose control window indicates the amount of follitropin alfa in international units (IU).
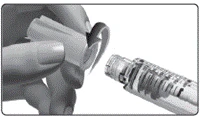
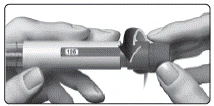
Immediately after injection, remove and discard the needle.
Do not reuse needles. The pen and/or needles must not be shared with other individuals.
Do not use the pen if it has been dropped, cracked, or damaged, as this may result in injury.
Dose administration diary
Use a dose administration diary to record daily doses administered. Administering an incorrect dose may impair your treatment.
- Record the treatment day (1), date (2), and time (3) of each injection, as well as the pen’s dose setting (4).
- Record the prescribed dose in column (5).
- Before injection, verify that you have selected the correct dose (6).
- After injection, check the number in the dose control window.
- Confirm that the full injection has been administered (7), or record the number displayed in the dose control window if it differs from "0" (8).
- If necessary, administer a second injection using another pen, setting the dose indicated in the column “Dose to be set for second injection” (8).
- Record this remaining dose in the “Dose to be administered” column in the next row (column 6).
Example of dose administration diary recording
| Treatment day |
Date |
Time |
Pen dosage |
Prescribed dose |
Dose check window |
||||||||||||||||||||||||||||
| Dose to be administered |
Dose to be set for second injection |
||||||||||||||||||||||||||||||||
| 1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
||||||||||||||||||||||||||
| No. 1 |
June 10 |
7:00 |
300 IU |
125 |
125 |
√ If 0, injection completed |
□ If not 0, second injection required; Administer _____ using a new pen |
||||||||||||||||||||||||||
| No. 2 |
June 11 |
7:00 |
300 IU |
125 |
125 |
√ If 0, injection completed |
□ If not 0, second injection required; Administer _____ using a new pen |
||||||||||||||||||||||||||
| No. 3 |
June 12 |
7:00 |
300 IU |
125 |
125 |
□ If 0, injection completed |
√ If not 0, second injection required; Administer 75 using a new pen |
||||||||||||||||||||||||||
| No. 3 |
June 12 |
7:00 |
300 IU |
- |
75
Do not use a microwave or other heating devices to warm the solution.
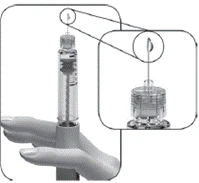
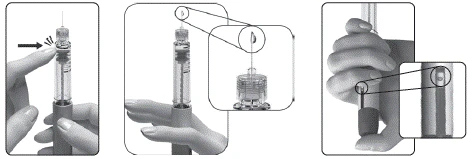
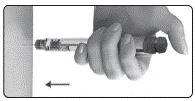
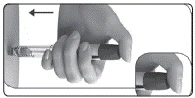
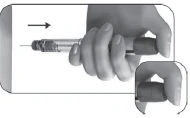
If you do not see small drops of liquid at the needle tip when using a new pen for the first time:
Note: The pre-filled pen contains 300 IU, 450 IU, or 900 IU of follitropin alfa. The maximum single dose that can be set is 300 IU (for the 300 IU pen) or 450 IU (for the 450 IU and 900 IU pens). The minimum single dose that can be set is 12.5 IU.
Do not store the pen with a needle attached, as this may lead to infection. Children. There are no appropriate indications for the use of GONAL-f® in pediatric patients. Overdose. The effects of overdose with GONAL-f® are unknown; however, there is a possibility of developing ovarian hyperstimulation syndrome (OHSS), as described in the section "Special precautions". Adverse reactions.General description of safety profile When using the medication, the most frequently reported adverse reactions were headache, ovarian cysts, and local reactions at the injection site (e.g., pain, erythema, hematoma, swelling and/or irritation at the injection site). Ovarian hyperstimulation syndrome (OHSS) of mild or moderate severity was frequently reported and should be considered an inherent risk of the stimulation procedure. Severe forms of OHSS are uncommon. Very rare cases of thromboembolism are possible (see section "Special precautions"). List of adverse reactions The following terminology is used to define the frequency of adverse reactions: very common (≥ 1/10); common (≥ 1/100 to < 1/10); uncommon (≥ 1/1000 to < 1/100); rare (≥ 1/10000 to < 1/1000); very rare (< 1/10000). Treatment of women Immune system disorders Very rare: Hypersensitivity reactions ranging from mild to severe, including anaphylactic reactions and shock. Nervous system disorders Very common: Headache. Vascular disorders Rare: Thromboembolism (associated and not associated with OHSS). Respiratory system disorders Rare: Exacerbation or worsening of asthma. Gastrointestinal disorders Common: Abdominal pain, sensation of abdominal distension and discomfort, nausea, vomiting, diarrhea. Reproductive system and breast disorders Very common: Ovarian cysts; Common: Mild to moderate OHSS (including associated symptoms); Uncommon: Severe OHSS (including associated symptoms) (see section "Special precautions"); Rare: Complications of severe OHSS. General disorders and administration site conditions Very common: Injection site reactions (e.g., pain, erythema, hematoma, swelling and/or irritation at the injection site). Treatment of men Immune system disorders Very rare: Hypersensitivity reactions ranging from mild to severe, including anaphylactic reactions and shock. Respiratory system disorders Rare: Exacerbation or worsening of asthma. Skin and subcutaneous tissue disorders Common: Acne. Reproductive system and breast disorders Common: Gynecomastia, varicocele. General disorders and administration site conditions Very common: Injection site reactions (e.g., pain, erythema, hematoma, swelling and/or irritation at the injection site). Other Common: Weight gain. Shelf life. 2 years. Do not use after the expiry date stated on the packaging. The patient should record the date of first use of the pre-filled pen with GONAL-f®. Prior to opening and within the shelf life, the medication can be stored without refrigeration at a temperature not exceeding 25 °C for one period of up to 3 months. The medication should be discarded if not used within these 3 months. After opening, the medicinal product should be stored at 2–25 °C for a maximum of 28 days. Storage conditions. Store at 2–8 °C (in the refrigerator). Do not freeze. To protect from light, the pen should be kept with the cap on. Keep out of reach of children. Packaging.
Prescription category. Prescription only. Manufacturer. Merck Serono S.p.A. / Merck Serono S.p.A. Manufacturer's name and address of place of business. Via delle Magnolie 15 (loc. frazione Zona Industriale), 70026 Modugno (Bari), Italy / Via delle Magnolie 15 (loc. frazione Zona Industriale), 70026 Modugno (Bari), Italy. | ||||||||||||||||||||||||||||