Fulvestrant-vista
Ukraine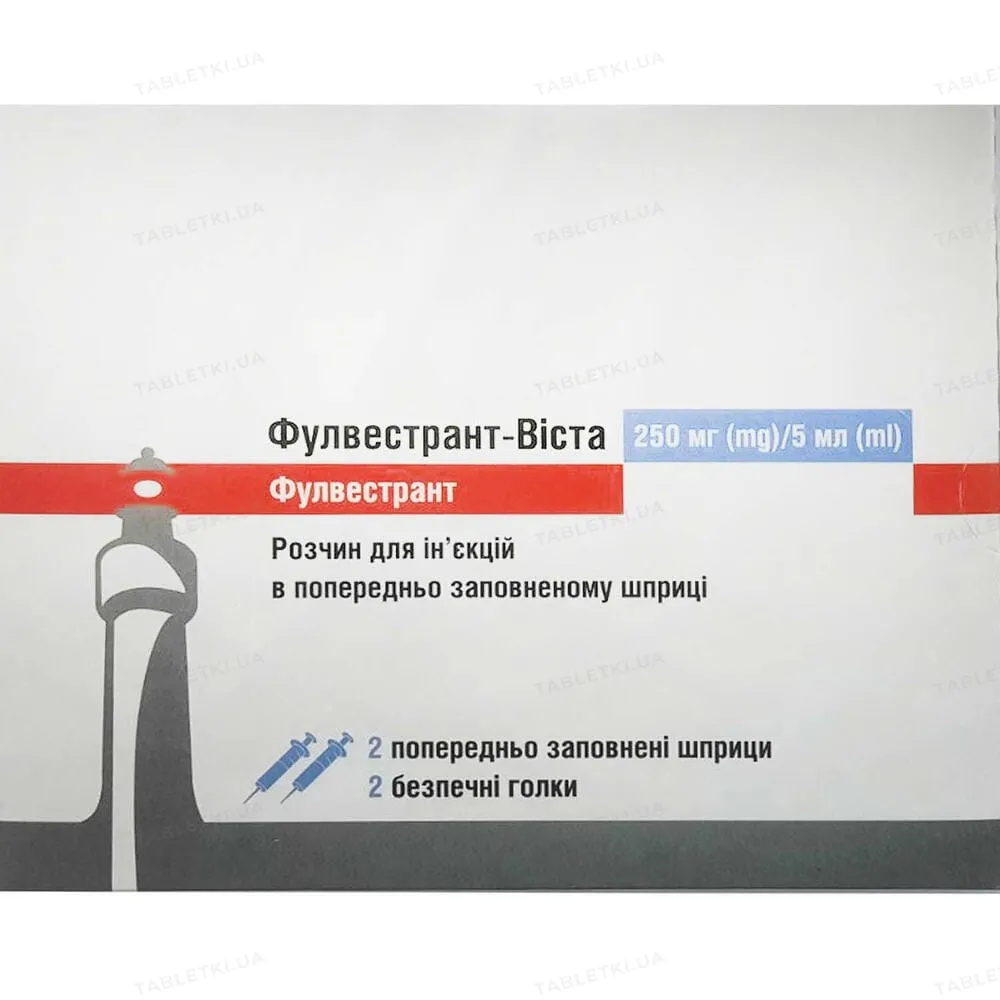
Table of Contents
INSTRUCTIONS FOR MEDICAL USE OF THE MEDICINAL PRODUCT FULVESTRANT-VISTA (FULVESTRANT-VISTA)
Composition:
Active ingredient: fulvestrant;
1 pre-filled syringe (5 ml) contains 250 mg of fulvestrant;
Excipients: ethanol 96%, benzyl alcohol (E1519), benzyl benzoate, refined castor oil.
Pharmaceutical form. Solution for injection.
Main physicochemical properties: clear, viscous liquid ranging from colorless to yellow.
Pharmacotherapeutic group. Hormone antagonists and related agents. Anti-estrogenic agents. ATC code L02BA03.
Pharmacological Properties.
Pharmacodynamics.
Mechanism of action and pharmacodynamic effects.
Fulvestrant is a competitive antagonist of estrogen receptors (ER), with affinity comparable to that of estradiol. Fulvestrant blocks the trophic effects of estrogens and does not exhibit partial agonist (estrogen-like) activity. Its mechanism of action is associated with negative regulation of estrogen receptor protein levels. Clinical studies in postmenopausal women with primary breast cancer have shown that fulvestrant significantly reduces ER protein levels in ER-positive tumors compared to placebo. A significant reduction in progesterone receptor expression was also observed, consistent with the absence of effects typical of estrogen agonists. Additionally, it has been demonstrated that fulvestrant at a dose of 500 mg suppresses ER and the proliferation marker Ki67 in breast tumors to a greater extent than fulvestrant at a dose of 250 mg during neoadjuvant treatment of postmenopausal women.
Clinical safety and efficacy in advanced breast cancer. Two Phase 3 clinical trials were conducted overall in 851 postmenopausal women with advanced breast cancer who had disease recurrence during or after adjuvant hormonal therapy or disease progression following hormonal therapy for advanced disease. 77% of the study population had estrogen receptor-positive breast cancer. These trials compared the safety and efficacy of monthly administration of fulvestrant 250 mg with daily administration of 1 mg anastrozole (an aromatase inhibitor). Overall, monthly fulvestrant 250 mg was at least as effective as anastrozole in terms of progression-free survival, objective response rate, and time to death. There were no statistically significant differences between the two treatment groups in any of these endpoints. The primary endpoint was progression-free survival. A combined analysis of both trials showed disease progression in 83% of patients receiving fulvestrant compared to 85% of patients receiving anastrozole. The combined analysis revealed a hazard ratio for progression-free survival of 0.95 (95% CI 0.82–1.10) for fulvestrant 250 mg versus anastrozole. The objective response rate for fulvestrant 250 mg was 19.2% compared to 16.5% for anastrozole. Median time to death was 27.4 months for patients receiving fulvestrant and 27.6 months for those receiving anastrozole. The hazard ratio for time to death for fulvestrant 250 mg versus anastrozole was 1.01 (95% CI 0.86–1.19). Effect on the endometrium in the postmenopausal period. Preclinical data indicate no stimulatory effect of fulvestrant on the postmenopausal endometrium. A two-week study in healthy postmenopausal volunteers receiving 20 mcg/day ethinylestradiol showed that pretreatment with fulvestrant 250 mg significantly reduced the stimulatory effect on the endometrium compared to pretreatment with placebo, as measured by ultrasound assessment of endometrial thickness. Neoadjuvant treatment for up to 16 weeks in patients with breast cancer receiving either fulvestrant 500 mg or fulvestrant 250 mg did not result in clinically significant changes in endometrial thickness, indicating absence of agonist effects. Currently, there is no evidence of adverse effects on the endometrium in patients with breast cancer. Morphological data on endometrial structure are not available. In two short-term studies (1 and 12 weeks) involving premenopausal patients with benign gynecological conditions, no statistically significant differences in endometrial thickness were observed between fulvestrant and placebo groups, as confirmed by ultrasound findings.
Effect on bone.
Long-term data on the effect of fulvestrant on bone are lacking. Neoadjuvant treatment for up to 16 weeks in patients with breast cancer receiving either fulvestrant 500 mg or fulvestrant 250 mg did not result in clinically significant changes in serum markers of bone remodeling.
Pediatric population.
Fulvestrant is not indicated for use in children.
An open-label Phase 2 study evaluated the safety, efficacy, and pharmacokinetics of fulvestrant in 30 girls aged 1 to 8 years with progressive precocious puberty associated with McCune-Albright syndrome (MAS). Children received 4 mg/kg fulvestrant intramuscularly once monthly. This 12-month study assessed a range of efficacy endpoints for fulvestrant use in MAS. Results showed reduced frequency of vaginal bleeding and slowed progression of bone age. Minimum steady-state concentrations of fulvestrant in children in this study were consistent with concentrations observed in adults (see section "Pharmacokinetics"). No new safety concerns arose during this small study, although five-year data are not yet available.
Pharmacokinetics.
Absorption.
After intramuscular injection of the prolonged-release formulation, fulvestrant is slowly absorbed, with peak plasma concentration (Cmax) reached approximately on day 5. With a dosing regimen of fulvestrant 500 mg, exposure levels at steady state or close to steady state are achieved within the first month of treatment (mean value [coefficient of variation (CV)]: AUC 475 [33.4%] ng·day/mL, Cmax 25.1 [35.3%] ng/mL, Cmin 16.3 [25.9%] ng/mL, respectively). At steady state, plasma concentrations of fulvestrant remain within a relatively narrow range, with approximately a threefold difference between maximum and minimum concentrations. Following intramuscular administration in the dose range of 50 to 500 mg, exposure is approximately dose-proportional.
Distribution.
Fulvestrant is extensively and rapidly distributed. The large apparent volume of distribution at steady state (Vdss) of approximately 3 to 5 L/kg indicates predominantly extravascular distribution. Fulvestrant is highly bound (99%) to plasma proteins. The main binding components are very low-density lipoprotein (VLDL), low-density lipoprotein (LDL), and high-density lipoprotein (HDL) fractions. Studies on protein binding interactions involving competitive displacement have not been conducted. The role of sex hormone-binding globulin (SHBG) has not been established.
Biological transformation.
The metabolism of fulvestrant is not fully characterized but involves a combination of several potential biotransformation pathways similar to those of endogenous steroids. Identified metabolites (including 17-ketone, sulfone, 3-sulfate, and 3- and 17-glucuronides) are either less active or demonstrate activity similar to fulvestrant in antiestrogenic models. Data from studies using human liver preparations and recombinant human enzymes indicate that CYP3A4 is the only P450 isoenzyme involved in the oxidation of fulvestrant; however, non-P450 pathways are believed to predominate in vivo. In vitro data indicate that fulvestrant does not inhibit CYP450 isoenzymes.
Elimination.
Fulvestrant is eliminated predominantly in metabolized form. The main route of elimination is fecal, with less than 1% excreted in urine. Fulvestrant has a high clearance of 11 ± 1.7 mL/min/kg, indicating a high hepatic extraction ratio. The terminal half-life (t1/2) after intramuscular administration is determined by the absorption rate and is estimated to be 50 days.
Special patient populations.
No differences in the pharmacokinetic profile of fulvestrant were observed based on age (range 33 to 89 years), body weight (40 to 127 kg), or race.
Renal impairment.
Mild and moderate renal impairment did not affect the pharmacokinetics of fulvestrant to any clinically significant extent.
Hepatic impairment.
The pharmacokinetics of fulvestrant were evaluated in a clinical study using a single dose in women with mild to moderate hepatic impairment (Child-Pugh class A and B). High doses were administered intramuscularly for a short duration. Compared to healthy subjects, women with hepatic impairment showed an almost 2.5-fold increase in AUC. An increase in exposure of this magnitude is expected to be well tolerated in patients receiving fulvestrant.
Pediatric population.
The pharmacokinetics of fulvestrant were evaluated in 30 girls with progressive precocious puberty associated with McCune-Albright syndrome. Pediatric patients (aged 1 to 8 years) received fulvestrant 4 mg/kg intramuscularly once monthly. The geometric mean (standard deviation) of steady-state minimum concentration (Cmin,ss) and AUCss was 4.2 (0.9) ng/mL and 3680 (1020) ng·hour/mL, respectively. Although data are limited, steady-state minimum concentrations of fulvestrant in children correspond to concentrations observed in adults.
Clinical characteristics.
Indications.
Fulvestrant-Vista is indicated:
- as monotherapy for the treatment of locally advanced or metastatic estrogen receptor-positive breast cancer in postmenopausal women:
- who have not previously received hormonal therapy, or
- who have disease recurrence during or after adjuvant antiestrogen therapy or disease progression during antiestrogen therapy;
- in combination with palbociclib for the treatment of hormone receptor-positive (HR-positive), human epidermal growth factor receptor 2-negative (HER2-negative) locally advanced or metastatic breast cancer in women who have received prior endocrine therapy (see section "Pharmacodynamics").
In premenopausal or perimenopausal women, combination treatment with palbociclib should be administered in combination with a luteinizing hormone-releasing hormone (LHRH) agonist.
Contraindications.
Hypersensitivity to the active substance or to any of the excipients.
Pregnancy or breastfeeding (see section "Use in pregnancy or breastfeeding").
Severe hepatic impairment (see sections "Pharmacokinetics" and "Special precautions").
Interaction with other medicinal products and other forms of interactions.
A clinical interaction study with midazolam (a CYP3A4 substrate) demonstrated that fulvestrant does not inhibit CYP3A4. Clinical interaction studies with rifampicin (a CYP3A4 inducer) and ketoconazole (a CYP3A4 inhibitor) showed no clinically significant changes in fulvestrant clearance. Therefore, dose adjustment is not required for patients receiving fulvestrant concomitantly with CYP3A4 inhibitors or inducers.
Special precautions for use.
Fulvestrant-Vista should be used with caution in patients with mild to moderate hepatic impairment (see sections "Pharmacokinetics", "Contraindications", and "Dosage and administration").
Fulvestrant-Vista should be used with caution in patients with severe renal impairment (creatinine clearance less than 30 mL/min).
Due to the intramuscular route of administration, Fulvestrant-Vista should be used with caution when treating patients with hemorrhagic diathesis, thrombocytopenia, or those taking anticoagulants.
Thromboembolic events have generally been observed in women with advanced breast cancer enrolled in clinical trials of fulvestrant (see section "Adverse reactions"). This should be taken into account when prescribing the medicinal product to patients who belong to a risk group.
Injection site reactions, including sciatica, neuralgia, neuropathic pain, and peripheral neuropathy, have been reported with fulvestrant administration. Given the proximity of the sciatic nerve, caution should be exercised when administering Fulvestrant-Vista into the upper outer quadrant of the gluteal region (see sections "Dosage and administration" and "Adverse reactions"). There are no data from long-term studies on the effect of fulvestrant on bones. Due to the mechanism of action of fulvestrant, there is a potential risk of developing osteoporosis. The safety and efficacy of fulvestrant (either as monotherapy or in combination with palbociclib) in patients with critical visceral disease have not been studied. When combining Fulvestrant-Vista with palbociclib, also refer to the summary of product characteristics for palbociclib.
Effect on estradiol assays using antibodies.
Due to the structural similarity between fulvestrant and estradiol, fulvestrant may interfere with immunoassay-based estradiol level testing, potentially leading to falsely elevated estradiol levels.
Excipients.
This medicinal product contains 10 vol.% ethanol (alcohol), i.e., up to 1 g per dose, equivalent to 20 mL of beer or 8 mL of wine per dose. This may be harmful in patients with alcoholism. Caution should be exercised when administering to pregnant women, breastfeeding women, children, patients with liver disease, and patients with epilepsy.
This medicinal product contains castor oil, which may cause severe allergic reactions. Fulvestrant-Vista contains 1 g of benzyl alcohol per dose, equivalent to 100 mg/mL. Benzyl alcohol may cause allergic reactions.
Large volumes should be used with caution and only if absolutely necessary, particularly in pregnant and breastfeeding women, as well as in patients with hepatic or renal impairment, due to the risk of accumulation and toxicity (metabolic acidosis).
Children.
Fulvestrant-Vista is not recommended for use in children and adolescents, as its safety and efficacy in this age group have not been established (see section "Pharmacodynamics").
Use during pregnancy or breastfeeding.
Women of reproductive potential.
Women of reproductive potential should use effective contraception during treatment with Fulvestrant-Vista and for 2 years after the last dose.
Pregnancy.
Fulvestrant-Vista is contraindicated during pregnancy (see section "Contraindications"). Fulvestrant has been shown to cross the placental barrier after a single intramuscular dose in animals. Animal studies have revealed reproductive toxicity, including increased incidence of fetal abnormalities and fetal death. If a patient becomes pregnant during treatment with Fulvestrant-Vista, she should be informed of the potential risk to the fetus and the potential risk of pregnancy loss.
Breastfeeding.
Breastfeeding should be discontinued during treatment with Fulvestrant-Vista. Fulvestrant is excreted in the milk of lactating animals. It is currently unknown whether fulvestrant passes into human breast milk. Given the potential for serious adverse reactions caused by fulvestrant in breastfed infants, breastfeeding is contraindicated during treatment with this medicinal product (see section "Contraindications").
Fertility.
The effect of fulvestrant on fertility in humans has not been studied.
Ability to influence the speed of reactions when driving or operating machinery.
Fulvestrant-Vista has no effect or a negligible effect on the ability to drive or operate machinery. However, since asthenia has been reported as a very common adverse reaction during treatment with fulvestrant, patients experiencing this side effect while driving or operating machinery should exercise caution.
Method of administration and dosage.
Dosage.
Adult women (including elderly individuals).
The recommended dose is 500 mg administered every 1 month; an additional dose of 500 mg should be given 2 weeks after the first injection.
When using Fulvestrant-Vista in combination with palbociclib, also refer to the summary of product characteristics for palbociclib.
For pre-/perimenopausal women, treatment with gonadotropin-releasing hormone (GnRH) agonists should be initiated prior to and continued during combination therapy with Fulvestrant-Vista and palbociclib, in accordance with local clinical practice guidelines.
Special patient populations.
Renal impairment.
Dose adjustment is not required in patients with mild to moderate renal impairment (creatinine clearance ≥30 mL/min). The efficacy and safety of the medicinal product have not been evaluated in patients with severe renal impairment (creatinine clearance <30 mL/min); therefore, caution should be exercised when administering the medicinal product to these patients (see section "Special precautions for use").
Hepatic impairment.
Dose adjustment is not required in patients with mild to moderate hepatic impairment. However, Fulvestrant-Vista should be administered with caution in these patients due to the potential for increased fulvestrant exposure. Data in patients with severe hepatic impairment are lacking (see sections "Pharmacokinetics" and "Special precautions for use").
Method of administration.
Fulvestrant-Vista must be administered as two consecutive, slow (1–2 minutes per injection) intramuscular injections of 5 mL each, one into each buttock (gluteal region).
Instructions for administration.
The medicinal product should be administered in accordance with local guidelines for administering large-volume intramuscular injections.
NOTE. Due to the close proximity of the sciatic nerve, caution should be exercised when administering Fulvestrant-Vista into the upper outer quadrant of the gluteal region (see section "Special precautions for use").
Warning: Do not autoclave the safety needle (the capped hypodermic needle “BD SafetyGlide™ Safety Hypodermic Needle”) before use.
Hands must remain behind the needle at all times during use and disposal.
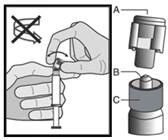
For each of the two syringes:
|
Figure 1
|
|
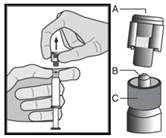
Figure 2
|
|
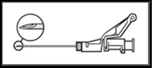
Figure 3
|
(1–2 minutes/injection) into the gluteal region. For user convenience, the needle bevel should be directed toward the lever arm (see Fig. 4). |
Figure 4
|
NOTE. During activation, keep the needle pointed away from yourself and others. Listen for the click and visually confirm that the needle tip is fully enclosed. |
Figure 5
|


Disposal.
Pre-filled syringes are intended for single use only.
This medicinal product may be hazardous to the aquatic environment.
Any unused medical devices or waste material must be disposed of in accordance with local requirements.
Children.
The safety and efficacy of fulvestrant in children from birth to 18 years of age have not been established. Available information is presented in the section "Pharmacological Properties", but no dosage recommendations can be made.
Overdose.
There have been isolated reports of fulvestrant overdose in humans. In case of overdose, symptomatic and supportive treatment is recommended. In animal studies, high doses of fulvestrant did not cause any effects other than those directly or indirectly related to its antiestrogenic activity.
Adverse reactions.
Summary of safety profile.
Monotherapy.
This section provides information based on all reported adverse reactions obtained from clinical trials, post-marketing experience, or spontaneous reports. In the pooled monotherapy dataset with fulvestrant, the most frequently reported adverse reactions were injection site reactions, asthenia, nausea, and increased levels of liver enzymes (ALT (alanine aminotransferase), AST (aspartate aminotransferase), ALP (alkaline phosphatase)).
The frequency data in the table below are summarized based on all reported events, regardless of investigator-assessed causality. The median duration of treatment with fulvestrant 500 mg in the pooled dataset was 6.5 months. List of adverse reactions in tabular form.
The adverse reactions listed below are classified according to frequency of occurrence and by system organ class (SOC). Frequency grouping was performed according to the following conventional criteria: very common (>1/10), common (≥1/100 to <1/10), uncommon (≥1/1,000 to <1/100). Within each frequency group, adverse reactions are listed in order of decreasing severity.
Adverse reactions by system organ class and frequency reported during treatment with fulvestrant in monotherapy
Table 1
| Adverse reactions classified by frequency and system organ class |
||
| Infections and infestations |
Common |
Urinary tract infections |
| Immune system disorders |
Very common |
Hypersensitivity reactions |
| Uncommon |
Anaphylactic reactions |
|
| Metabolism and nutrition disorders |
Common |
Anorexia |
| Nervous system disorders |
Common |
Headache |
| Vascular disorders |
Very common |
Hot flushes |
| Common |
Venous thromboembolisma |
|
| Gastrointestinal disorders |
Very common |
Nausea |
| Common |
Vomiting, diarrhea |
|
| Hepatobiliary disorders |
Very common |
Increased levels of liver enzymes (ALT, AST, ALP)a |
| Common |
Increased bilirubin levelsa |
|
| Uncommon |
Hepatic failurec,f, hepatitisf, increased levels of GGTf |
|
| Skin and subcutaneous tissue disorders |
Very common |
Rash |
| Musculoskeletal and connective tissue disorders |
Very common |
Joint and muscle paind |
| Common |
Back paina |
|
| Reproductive system and breast disorders |
Common |
Vaginal bleedinge |
| Uncommon |
Vaginal candidiasisf, leukorrheaf |
|
| General disorders and administration site conditions |
Very common |
Astheniaa, injection site reactionsb |
| Common |
Peripheral neuropathye, sciaticae |
|
| Uncommon |
Injection site hemorrhagef, injection site hematomaf, neuralgiac,f |
|
| Blood and lymphatic system disorders |
Common |
Decreased platelet counte |
a. Includes adverse drug reactions for which the relationship to fulvestrant could not be precisely assessed due to the underlying disease.
b. The term "injection site reactions" does not include the terms "hemorrhage at injection site" and "hematoma at injection site", "sciatica", "neuralgia", "peripheral neuropathy".
c. The reaction was not observed during large clinical trials.
The frequency was calculated using the upper limit of the 95% confidence interval for point estimation. It was calculated as 3/560 (where 560 is the number of patients in large clinical trials), corresponding to the frequency category "uncommon".
d. Includes arthralgia and, less frequently, musculoskeletal pain, myalgia, and limb pain.
e. There are some differences in the frequency of adverse reactions within the respective organ and system categories between the safety study and the FALCON study.
f. Adverse reactions were not observed during the FALCON study.
Description of selected adverse reactions.
The following description is based on safety analysis of the group of patients who received at least one dose of fulvestrant and the group of patients who received at least one dose of anastrozole in the Phase 3 FALCON study.
Joint pain and musculoskeletal pain.
According to data from the FALCON study, the number of patients reporting joint pain and musculoskeletal pain was 65 (31.2%) and 48 (24.1%) in the fulvestrant and anastrozole groups, respectively. Of the 65 patients receiving fulvestrant, 40% (26/65) reported joint and musculoskeletal pain within the first month of treatment, and 66% (43/65) within the first 3 months of treatment. None of the patients reported events of grade ≥3 according to CTCAE, or events requiring dose reduction, temporary interruption, or discontinuation of the drug due to these adverse reactions.
Combination therapy with palbociclib.
The overall safety profile of fulvestrant when used in combination with palbociclib is based on data from 517 patients with HR-positive, HER2-negative locally advanced or metastatic breast cancer in the randomized PALOMA-3 trial (see section "Pharmacodynamics"). The most commonly reported adverse reactions (≥20%) of any grade in patients receiving fulvestrant in combination with palbociclib were neutropenia, leukopenia, infections, fatigue, nausea, anemia, stomatitis, diarrhea, and thrombocytopenia. The most commonly reported adverse reactions (≥2%) of grade ≥III were neutropenia, leukopenia, anemia, infections, increased AST levels, thrombocytopenia, and fatigue.
The table below presents data on adverse reactions observed in the PALOMA-3 study.
The median duration of treatment with fulvestrant was 11.2 months in the fulvestrant + palbociclib group and 4.9 months in the fulvestrant + placebo group. The median duration of treatment with palbociclib in the fulvestrant + palbociclib group was 10.8 months.
Adverse reactions from the PALOMA-3 study (N=517)
Table 2
| System organ class Frequency Preferred term |
Fulvestrant + palbociclib (N=345) |
Fulvestrant + placebo (N=172) |
||
| All grades n (%) |
≥ Grade 3 n (%) |
All grades n (%) |
≥ Grade 3 n (%) |
|
| Infections and infestations |
||||
| Very common |
||||
| Infectionsb |
163 (47.2) |
11 (3.2) |
54 (31.4) |
5 (2.9) |
| Blood and lymphatic system disorders |
||||
| Very common |
||||
| Neutropeniac |
287 (83.2) |
228 (66.1) |
7 (4.1) |
1 (0.6) |
| Leukopeniad |
183 (53.0) |
105 (30.4) |
9 (5.2) |
2 (1.2) |
| Anemiae |
102 (29.6) |
12 (3.5) |
22 (12.8) |
3 (1.7) |
| Thrombocytopeniaf |
78 (22.6) |
8 (2.3) |
0 (0.0) |
0 |
| Uncommon |
||||
| Febrile neutropenia |
3 (0.9) |
3 (0.9) |
1 (0.6) |
1 (0.6) |
| Metabolism and nutrition disorders |
||||
| Very common |
||||
| Decreased appetite |
55 (15.9) |
3 (0.9) |
14 (8.1) |
1 (0.6) |
| Nervous system disorders |
||||
| Common |
||||
| Dysgeusia |
23 (6.7) |
0 |
5 (2.9) |
0 |
| Eye disorders |
||||
| Common |
||||
| Lacrimation increased |
22 (6.4) |
0 |
2 (1.2) |
0 |
| Blurred vision |
20 (5.8) |
0 |
3 (1.7) |
0 |
| Dry eye |
13 (3.8) |
0 |
3 (1.7) |
0 |
| Respiratory, thoracic and mediastinal disorders |
||||
| Common |
||||
| Nasal haemorrhage |
23 (6.7) |
0 |
3 (1.7) |
0 |
| Gastrointestinal disorders |
||||
| Very common |
||||
| Nausea |
117 (33.9) |
0 |
48 (27.9) |
1 (0.6) |
| Stomatitisg |
97 (28.1) |
2 (0.6) |
22 (12.8) |
0 |
| Diarrhoea |
81 (23.5) |
0 |
33 (19.2) |
2 (1.2) |
| Vomiting |
65 (18.8) |
2 (0.6) |
26 (15.1) |
1 (0.6) |
| Skin and subcutaneous tissue disorders |
||||
| Very common |
||||
| Alopecia |
62 (18.0) |
0 |
11 (6.4) |
0 |
| Rashh |
58 (16.8) |
2 (0.6) |
11 (6.4) |
0 |
| Common |
||||
| Dry skin |
21 (6.1) |
0 |
2 (1.2) |
0 |
| General disorders and administration site conditions |
||||
| Very common |
||||
| Fatigue |
142 (41.2) |
8 (2.3) |
50 (29.1) |
2 (1.2) |
| Pyrexia |
44 (12.8) |
1 (0.3) |
9 (5.2) |
0 |
| Common |
||||
| Asthenia |
26 (7.5) |
0 |
9 (5.2) |
1 (0.6) |
| Investigations |
||||
| Common |
||||
| Increased AST |
26 (7.5) |
10 (2.9) |
9 (5.2) |
3 (1.7) |
| Increased ALT |
20 (5.8) |
6 (1.7) |
6 (3.5) |
0 |
ALT = alanine aminotransferase; AST = aspartate aminotransferase; N/n = number of patients
a Preferred terms (PT) according to MedDRA 17.1 are indicated.
b All PTs belonging to the System Organ Class: infections and infestations.
c Neutropenia includes the following PTs: neutropenia, decreased neutrophil count.
d Leukopenia includes the following PTs: leukopenia, decreased white blood cell count.
e Anaemia includes the following PTs: anaemia, decreased haemoglobin level, decreased haematocrit level.
f Thrombocytopenia includes the following PTs: thrombocytopenia, decreased platelet count.
g Stomatitis includes the following PTs: aphthous stomatitis, cheilitis, glossitis, glossodynia, oral ulceration, mucosal inflammation, oral pain, oropharyngeal discomfort, oropharyngeal pain, stomatitis.
h Rash includes the following PTs: rash, maculopapular rash, rash with pruritus, erythematous rash, papular rash, dermatitis, acneiform dermatitis, toxic skin eruption.
Description of selected adverse reactions.
Neutropenia.
In patients receiving fulvestrant in combination with palbociclib in the PALOMA-3 study, neutropenia of any grade was reported in 287 (83.2%) patients, Grade III neutropenia was reported in 191 (55.4%) patients, and Grade IV neutropenia in 37 (10.7%) patients. In the fulvestrant + placebo group (n=172), neutropenia of any grade was reported in 7 (4.1%) patients and Grade III neutropenia in 1 (0.6%) patient. No cases of Grade IV neutropenia were reported in the fulvestrant + placebo group.
In patients receiving fulvestrant in combination with palbociclib, the median time to first episode of neutropenia was 15 days (range: 13–317), and the median duration of Grade ≥III neutropenia was 7 days. Febrile neutropenia was reported in 0.9% of patients receiving fulvestrant in combination with palbociclib. Reporting of suspected adverse reactions.
Reporting suspected adverse reactions after marketing authorization is important. It allows continued monitoring of the benefit-risk balance of the medicinal product. Healthcare professionals are required to report any suspected adverse reactions through the national reporting system.
Shelf life.
3 years.
Temperature excursions outside the range of 2 to 8 °C should be limited. Exposure to temperatures above 30 °C should be avoided, and the period during which the product is stored at an average temperature below 25 °C (but above 2–8 °C) should not exceed 28 days. After temperature excursions, the product must be returned immediately to the recommended storage conditions (storage and transport at 2 to 8 °C in a refrigerator). Temperature excursions have a cumulative effect on the quality of the medicinal product, and the 28-day period should not be counted beyond the two-year shelf life of Fulvestrant-Vista. Exposure to temperatures below 2 °C does not damage the medicinal product provided it is not stored below –20 °C.
Storage conditions.
Store and transport at 2 to 8 °C.
Keep out of the reach of children.
Keep pre-filled syringes in the original packaging to protect from light.
Incompatibilities.
Since compatibility studies are lacking, this medicinal product should not be mixed with other medicinal products.
Packaging.
One pre-filled syringe with first-opening control in a cardboard box with one safety needle (BD SafetyGlide), or two pre-filled syringes with first-opening control in a cardboard box with two safety needles (BD SafetyGlide).
Prescription category.
Prescription only.
Manufacturer.
LABORATORIOS FARMALAN S.A.
Manufacturer's address and location of its business operations.
Calle La Valiña s/n – Navatejera, Villalcámbre, León, 24193, Spain.